Depot buprenorphine: Safe and effective for clients in jails and prisons?
There are barriers to receiving opioid use disorder medications, such as buprenorphine, for individuals in criminal justice settings like jails and prisons. These include limited resources to ensure adequate medical monitoring and the potential for their illegal sharing or selling (i.e., diversion) to other inmates. This study examined safety and opioid use outcomes in a group of incarcerated individuals who received a longer acting, injection formulation of buprenorphine.
Individuals with opioid use disorder in criminal justice settings, like jail or prisons, benefit from opioid agonist medication treatment (i.e., by receiving buprenorphine or methadone) to support theirrecovery. These medications can help with the management of withdrawal symptoms and craving and help to prevent overdose and fatalities. Yet, there are many barriers to receiving opioid agonist medication treatment in these settings. These barriers include stigma towards use of these medications, a lack of knowledge around how to best implement this approach in criminal justice settings, lack of standardization in approaches, and inadequate resources to ensure monitoring for potential medical complications. There is also the potential for illegal sharing or selling (i.e., diversion) of these medications to other individuals in these settings. Some research has even indicated that individuals experience threats or direct violence due to the desirability of these medications.
This study examined the safety and preliminary outcomes of the use of depot buprenorphine in a sample of adults serving a correctional sentence in New South Wales, Australia.
HOW WAS THIS STUDY CONDUCTED?
This study was a 16-week non-randomized, open-label trial of 129 adults in correctional care during 2018-2019. The primary outcomes were the safety of depot buprenorphine and diversion of opioid use disorder medication, while secondary outcomes were substance use and treatment retention. The primary trial group of interest was a group who received depot buprenorphine (formulation provided was CAM2038) while the comparator group was comprised of individuals who were already stable on oral methadone. Eligible participants were adults (18 years or older) in custody who had a full-time sentence of 6 months or more before earliest release date, and who had a diagnosis of moderate to severe opioid use disorder according to the DSM-5 criteria.
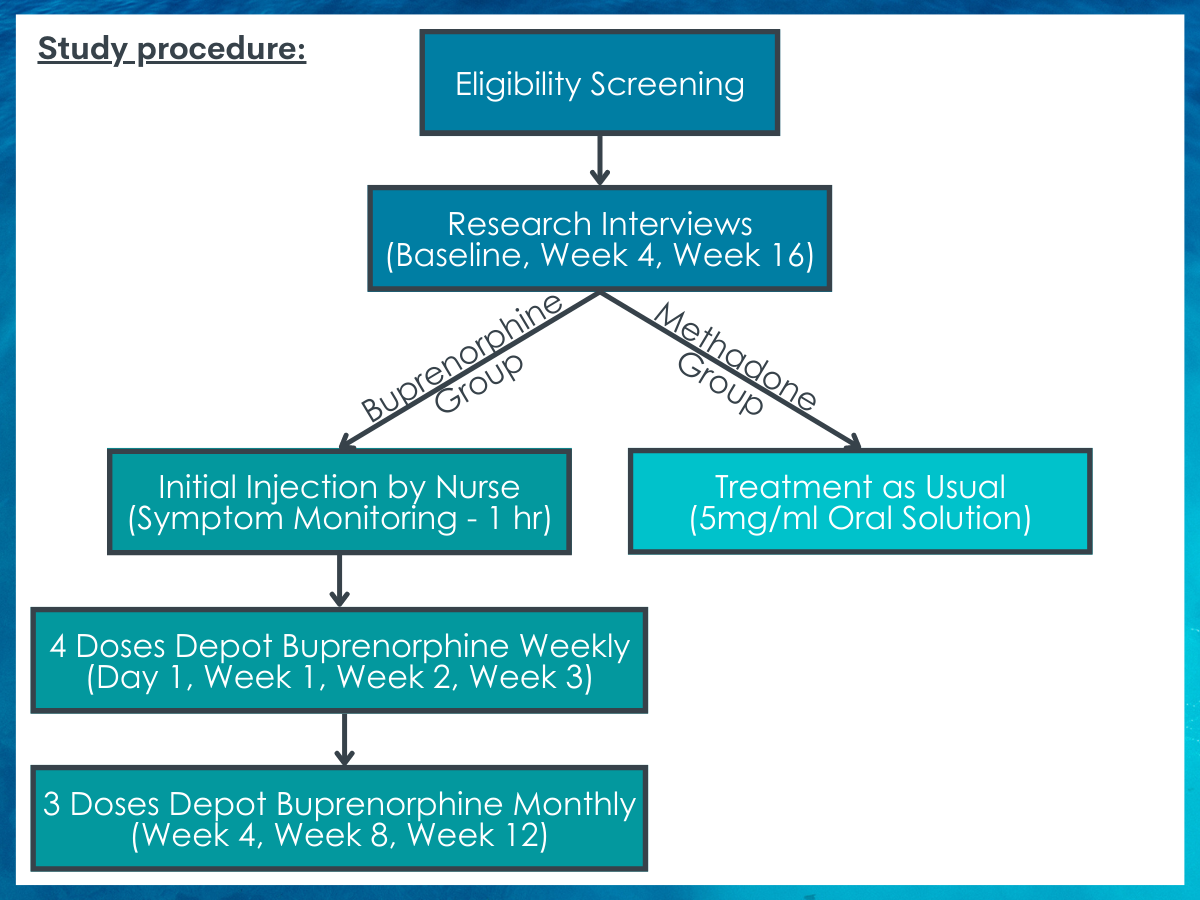
Following screening for eligibility, all eligible individuals completed research interviews at baseline, and weeks 4 and 16. Participants in the depot buprenorphine group received an initial injection by a trained nurse and were monitored for symptoms for the next hour. Following that initiation, these participants received four doses of depot buprenorphine weekly (day 1, week 1, week 2 and week 3) followed by three doses of depot buprenorphine monthly (week 4, week 8 and week 12). These doses could be increased by the nurse as necessary. Individuals in the methadone arm continued with their treatment as usual (5mg/ml oral liquid solution).
The researchers collected data from the criminal justice system on any medical complications documented by study medical officers, diversion incidents documented by the criminal justice system, and injection site and physical examinations. The researchers – who were independent from staff providing the study medication – also collected face-to-face self-report data at baseline and weeks 4 and 16 of the trial. Participants were asked about their experience hearing about diversion-associated violence or their experience diverting medications. They were also asked about non-prescribed use of opioids, injection drugs, and methamphetamines using the Australian Treatment Outcomes Profile, yielding a binary (yes/no) measures of use in the past 28 days.
Of the sample of 129 adult participants who participated in the trial, 67 were enrolled in the depot buprenorphine group and 62 were enrolled in the comparator group – the stable methadone treatment group. While the majority of both groups were Australian-born, less than half of each group were considered Aboriginal or Torres Strait Islander. The majority of the depot buprenorphine group were male (82%), and on average 35 years old. About half (54%) had completed only their junior year of high school (54%). Those in the depot buprenorphine group had a higher opioid craving score (53 versus 18) and were less likely to previously have used opioid agonist medication (70% versus 97%) than those in the methadone group. While the methadone group were also primarily male (85%), they differed in several ways. First, they were slightly older (on average 38 years old), less likely to have completed junior high school (32%), and as noted above, were more likely to have previously used opioid agonist medication (97% versus 70%).
WHAT DID THIS STUDY FIND?
Medical complications (adverse events) were common but mild.
Of the 67 participants in the depot buprenorphine group, 97% experienced at least one adverse medical complication, with 94% of those being directly due to the study drug. Of those who experienced a medical complication, 88% experienced a mild issue, including injection site pain or swelling, constipation, or headache, that was resolved in a day. There were 4 participants in this group who decided to discontinue their participation in the study because of these complications and one was withdrawn due to another comorbid medical condition. In comparison, of the 62 participants in the methadone group, fewer experienced adverse events (73%), but these were individuals who were considered more stable as they had entered the study already on methadone. Neither group experienced any fatalities. The overall probability of staying in treatment was very high (92%).
Diversion or threats related to it was previously common, but rare during the trial.
At the time of the initial study assessment, 78% of all participants had heard of threats, coercion, or intimidation related to diverting medications for opioid use disorder, and 17% of the participants themselves reported actually diverting these medications while incarcerated. During the study follow-up period, less than 10% had heard about recent intimidation or violence related to diverting medications for opioid use disorder and none of the participants reported diverting medications during this time.
The depot buprenorphine group reduced the prevalence and frequency of substance use.
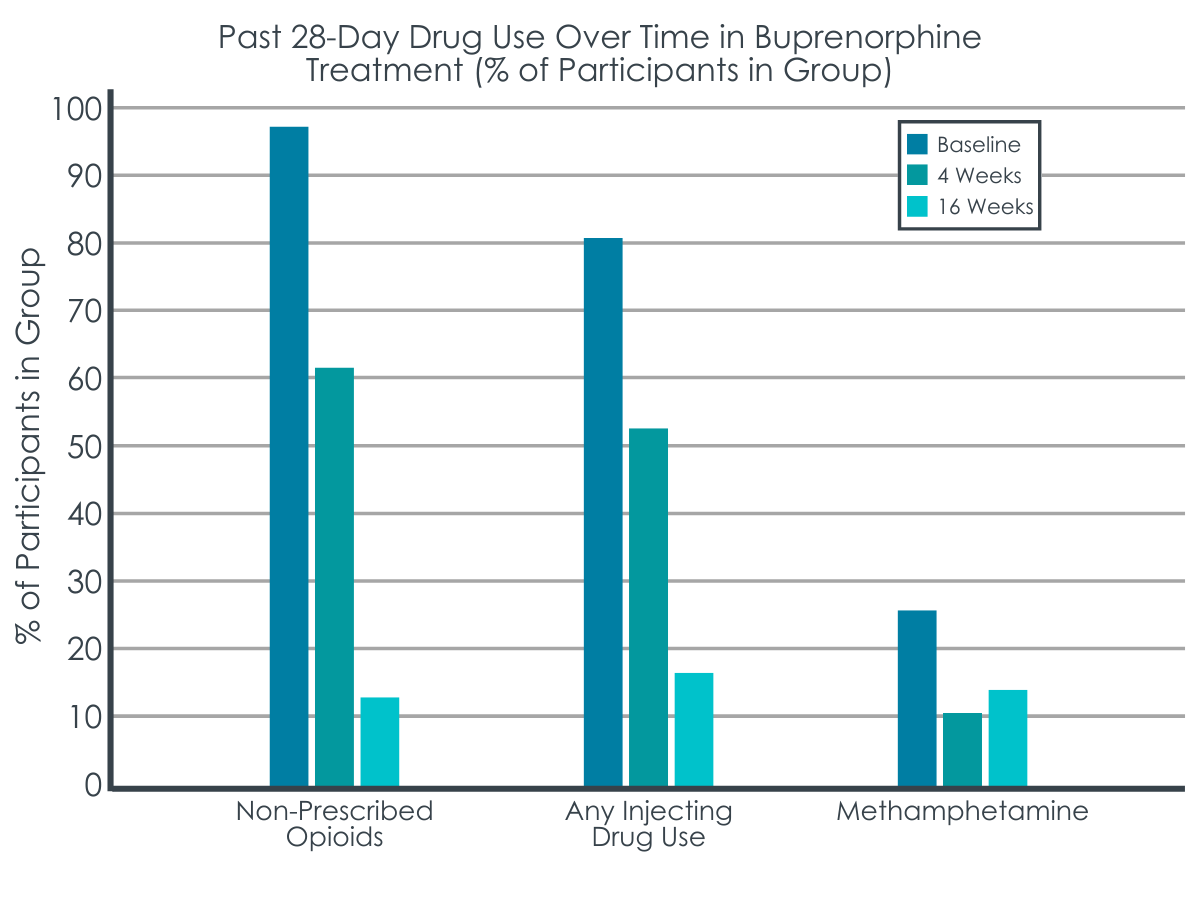
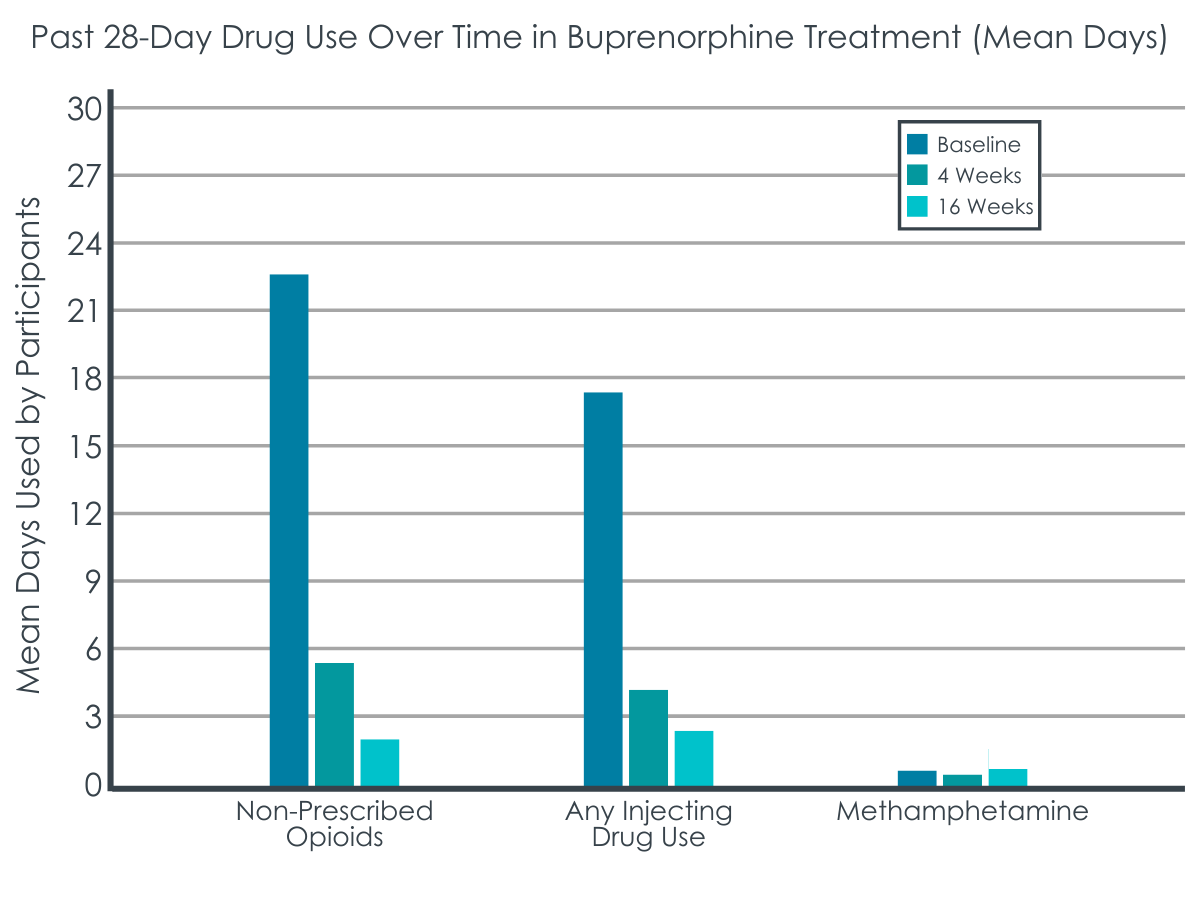
While 97% of individuals in the depot buprenorphine group used non-prescribed opioids at the beginning of the study (baseline), only 12% of individuals in that group used non-prescribed opioids at 16 weeks. This group also decreased their frequency of non-prescribed opioid use from 22.51 days (baseline) to 2.14 days (16 weeks). Similarly, although 81% of individuals in the depot buprenorphine group reported injecting drugs at baseline, only 17% of individuals in that group injected drugs at 16 weeks. This group also decreased their frequency of injecting drugs from 17.55 days (baseline) to 2.51 days (16 weeks). The decreases in days of opioid and injection use during the trial occurred primarily in the first 4 weeks (see Figure below). There was no change – either in frequency or days of use – for methamphetamines, but this is likely due to low baseline use of methamphetamines among this group (i.e., 0.54 days).
Individuals in the methadone group did not reduce their substance use during the study, but unlike the depot buprenorphine group, they were maintained on methadone at study entry and their levels of substance use were already low. For example, 1% or less of the methadone group used non-prescribed opioids or methamphetamine or injected drugs at study entry.
First, depot buprenorphine, a long-acting injectable medication for opioid use disorder, was found to be safe and acceptable among inmates. Individuals were highly likely to be retained in the treatment, reported primarily only minor medical complications (e.g., related to pain at the injection site), reduced non-prescribed opioid and injection drug use, and were unlikely to report trying to divert their medication. Knowing that most individuals did experience an adverse medical complication such as early injection site pain that subsides within a day may be useful for future implementation as it could be included in provider education and setting expectations with clients to assist with treatment retention.
Second, the comparator group, which more closely mirrors standard practice in criminal justice settings, is a group maintained on methadone. This group did not report diverting medications and did not differ on substance use outcomes over time but overall maintained very low substance use. Although not the primary focus of this study, the methadone group provides additional support for the use of oral methadone in these settings given the primarily positive outcomes and behaviors of the group.
The study setting and approach of examining depot buprenorphine did not allow for a rigorous randomized controlled trial. Instead, this is a pre-post study where the closest comparator is a group of individuals on methadone. The methadone group, however, had very different characteristics from the depot buprenorphine group, so it is important not to make direct comparisons between the two groups.
Although the results were promising for the 16 weeks (approximately 4 months) of the trial, it is unclear how individuals in either group did or would do after that time period. Knowing whether they chose to continue and how effective that experience was, would be helpful to ultimately understanding the sustainability of the depot buprenorphine approach in this setting.
BOTTOM LINE
In this study, the researchers found that among individuals with opioid use disorder in correctional facility care in Australia, the use of both depot buprenorphine and methadone medications was safe, helped to substantially reduce non-prescribed opioid use, and did not result in diversion.
For treatment professionals and treatment systems: The adoption of medication for opioid use disorder treatment programs in jails and prisons depends on the support of leadership and staff in these settings and having a developed infrastructure to sustain these programs. Implementing a long-acting injectable form of medication, that seems to address the contentious issue of diversion may be one way to meet this challenge head-on. Also, the creation of care and transition plans for individuals who initiate medication for opioid use disorder while incarcerated is critical to ensure treatment retention as well as safety after release.
For scientists:Research that more rigorously examines the different medications for opioid use disorder among individuals in correctional or criminal justice settings is needed to replicate and extend these findings. Additional research with more specific populations marginalized in these settings such as females or members of the LGBTQ+ community may also be necessary to understand their experience. In addition to examining the safety and effectiveness of these medications, this research should also focus on system-level issues to identify key barriers and facilitators to adopting and implementing these programs across various legal systems and to ensure availability of these treatments are offered to all inmates.
For policy makers: Although medications such as buprenorphine methadone examined in this study are very helpful life-saving medications for individuals with opioid use disorder, there are many barriers to their implementation in correctional settings throughout the United States. Additional funding to study best ways to implement these treatments and address barriers to implementation will help to expand opioid treatment programs in correctional facilities, which should ultimately help in fighting the opioid overdose epidemic in the United States. Ensuring state and federal policies allow for, and support the dispensing of, these medications in correctional settings, will also be necessary for widespread implementation of these strategies.
Individuals with opioid use disorder in criminal justice settings, like jail or prisons, benefit from opioid agonist medication treatment (i.e., by receiving buprenorphine or methadone) to support theirrecovery. These medications can help with the management of withdrawal symptoms and craving and help to prevent overdose and fatalities. Yet, there are many barriers to receiving opioid agonist medication treatment in these settings. These barriers include stigma towards use of these medications, a lack of knowledge around how to best implement this approach in criminal justice settings, lack of standardization in approaches, and inadequate resources to ensure monitoring for potential medical complications. There is also the potential for illegal sharing or selling (i.e., diversion) of these medications to other individuals in these settings. Some research has even indicated that individuals experience threats or direct violence due to the desirability of these medications.
This study examined the safety and preliminary outcomes of the use of depot buprenorphine in a sample of adults serving a correctional sentence in New South Wales, Australia.
HOW WAS THIS STUDY CONDUCTED?
This study was a 16-week non-randomized, open-label trial of 129 adults in correctional care during 2018-2019. The primary outcomes were the safety of depot buprenorphine and diversion of opioid use disorder medication, while secondary outcomes were substance use and treatment retention. The primary trial group of interest was a group who received depot buprenorphine (formulation provided was CAM2038) while the comparator group was comprised of individuals who were already stable on oral methadone. Eligible participants were adults (18 years or older) in custody who had a full-time sentence of 6 months or more before earliest release date, and who had a diagnosis of moderate to severe opioid use disorder according to the DSM-5 criteria.
Following screening for eligibility, all eligible individuals completed research interviews at baseline, and weeks 4 and 16. Participants in the depot buprenorphine group received an initial injection by a trained nurse and were monitored for symptoms for the next hour. Following that initiation, these participants received four doses of depot buprenorphine weekly (day 1, week 1, week 2 and week 3) followed by three doses of depot buprenorphine monthly (week 4, week 8 and week 12). These doses could be increased by the nurse as necessary. Individuals in the methadone arm continued with their treatment as usual (5mg/ml oral liquid solution).
The researchers collected data from the criminal justice system on any medical complications documented by study medical officers, diversion incidents documented by the criminal justice system, and injection site and physical examinations. The researchers – who were independent from staff providing the study medication – also collected face-to-face self-report data at baseline and weeks 4 and 16 of the trial. Participants were asked about their experience hearing about diversion-associated violence or their experience diverting medications. They were also asked about non-prescribed use of opioids, injection drugs, and methamphetamines using the Australian Treatment Outcomes Profile, yielding a binary (yes/no) measures of use in the past 28 days.
Of the sample of 129 adult participants who participated in the trial, 67 were enrolled in the depot buprenorphine group and 62 were enrolled in the comparator group – the stable methadone treatment group. While the majority of both groups were Australian-born, less than half of each group were considered Aboriginal or Torres Strait Islander. The majority of the depot buprenorphine group were male (82%), and on average 35 years old. About half (54%) had completed only their junior year of high school (54%). Those in the depot buprenorphine group had a higher opioid craving score (53 versus 18) and were less likely to previously have used opioid agonist medication (70% versus 97%) than those in the methadone group. While the methadone group were also primarily male (85%), they differed in several ways. First, they were slightly older (on average 38 years old), less likely to have completed junior high school (32%), and as noted above, were more likely to have previously used opioid agonist medication (97% versus 70%).
WHAT DID THIS STUDY FIND?
Medical complications (adverse events) were common but mild.
Of the 67 participants in the depot buprenorphine group, 97% experienced at least one adverse medical complication, with 94% of those being directly due to the study drug. Of those who experienced a medical complication, 88% experienced a mild issue, including injection site pain or swelling, constipation, or headache, that was resolved in a day. There were 4 participants in this group who decided to discontinue their participation in the study because of these complications and one was withdrawn due to another comorbid medical condition. In comparison, of the 62 participants in the methadone group, fewer experienced adverse events (73%), but these were individuals who were considered more stable as they had entered the study already on methadone. Neither group experienced any fatalities. The overall probability of staying in treatment was very high (92%).
Diversion or threats related to it was previously common, but rare during the trial.
At the time of the initial study assessment, 78% of all participants had heard of threats, coercion, or intimidation related to diverting medications for opioid use disorder, and 17% of the participants themselves reported actually diverting these medications while incarcerated. During the study follow-up period, less than 10% had heard about recent intimidation or violence related to diverting medications for opioid use disorder and none of the participants reported diverting medications during this time.
The depot buprenorphine group reduced the prevalence and frequency of substance use.
While 97% of individuals in the depot buprenorphine group used non-prescribed opioids at the beginning of the study (baseline), only 12% of individuals in that group used non-prescribed opioids at 16 weeks. This group also decreased their frequency of non-prescribed opioid use from 22.51 days (baseline) to 2.14 days (16 weeks). Similarly, although 81% of individuals in the depot buprenorphine group reported injecting drugs at baseline, only 17% of individuals in that group injected drugs at 16 weeks. This group also decreased their frequency of injecting drugs from 17.55 days (baseline) to 2.51 days (16 weeks). The decreases in days of opioid and injection use during the trial occurred primarily in the first 4 weeks (see Figure below). There was no change – either in frequency or days of use – for methamphetamines, but this is likely due to low baseline use of methamphetamines among this group (i.e., 0.54 days).
Individuals in the methadone group did not reduce their substance use during the study, but unlike the depot buprenorphine group, they were maintained on methadone at study entry and their levels of substance use were already low. For example, 1% or less of the methadone group used non-prescribed opioids or methamphetamine or injected drugs at study entry.
First, depot buprenorphine, a long-acting injectable medication for opioid use disorder, was found to be safe and acceptable among inmates. Individuals were highly likely to be retained in the treatment, reported primarily only minor medical complications (e.g., related to pain at the injection site), reduced non-prescribed opioid and injection drug use, and were unlikely to report trying to divert their medication. Knowing that most individuals did experience an adverse medical complication such as early injection site pain that subsides within a day may be useful for future implementation as it could be included in provider education and setting expectations with clients to assist with treatment retention.
Second, the comparator group, which more closely mirrors standard practice in criminal justice settings, is a group maintained on methadone. This group did not report diverting medications and did not differ on substance use outcomes over time but overall maintained very low substance use. Although not the primary focus of this study, the methadone group provides additional support for the use of oral methadone in these settings given the primarily positive outcomes and behaviors of the group.
The study setting and approach of examining depot buprenorphine did not allow for a rigorous randomized controlled trial. Instead, this is a pre-post study where the closest comparator is a group of individuals on methadone. The methadone group, however, had very different characteristics from the depot buprenorphine group, so it is important not to make direct comparisons between the two groups.
Although the results were promising for the 16 weeks (approximately 4 months) of the trial, it is unclear how individuals in either group did or would do after that time period. Knowing whether they chose to continue and how effective that experience was, would be helpful to ultimately understanding the sustainability of the depot buprenorphine approach in this setting.
BOTTOM LINE
In this study, the researchers found that among individuals with opioid use disorder in correctional facility care in Australia, the use of both depot buprenorphine and methadone medications was safe, helped to substantially reduce non-prescribed opioid use, and did not result in diversion.
For treatment professionals and treatment systems: The adoption of medication for opioid use disorder treatment programs in jails and prisons depends on the support of leadership and staff in these settings and having a developed infrastructure to sustain these programs. Implementing a long-acting injectable form of medication, that seems to address the contentious issue of diversion may be one way to meet this challenge head-on. Also, the creation of care and transition plans for individuals who initiate medication for opioid use disorder while incarcerated is critical to ensure treatment retention as well as safety after release.
For scientists:Research that more rigorously examines the different medications for opioid use disorder among individuals in correctional or criminal justice settings is needed to replicate and extend these findings. Additional research with more specific populations marginalized in these settings such as females or members of the LGBTQ+ community may also be necessary to understand their experience. In addition to examining the safety and effectiveness of these medications, this research should also focus on system-level issues to identify key barriers and facilitators to adopting and implementing these programs across various legal systems and to ensure availability of these treatments are offered to all inmates.
For policy makers: Although medications such as buprenorphine methadone examined in this study are very helpful life-saving medications for individuals with opioid use disorder, there are many barriers to their implementation in correctional settings throughout the United States. Additional funding to study best ways to implement these treatments and address barriers to implementation will help to expand opioid treatment programs in correctional facilities, which should ultimately help in fighting the opioid overdose epidemic in the United States. Ensuring state and federal policies allow for, and support the dispensing of, these medications in correctional settings, will also be necessary for widespread implementation of these strategies.
Individuals with opioid use disorder in criminal justice settings, like jail or prisons, benefit from opioid agonist medication treatment (i.e., by receiving buprenorphine or methadone) to support theirrecovery. These medications can help with the management of withdrawal symptoms and craving and help to prevent overdose and fatalities. Yet, there are many barriers to receiving opioid agonist medication treatment in these settings. These barriers include stigma towards use of these medications, a lack of knowledge around how to best implement this approach in criminal justice settings, lack of standardization in approaches, and inadequate resources to ensure monitoring for potential medical complications. There is also the potential for illegal sharing or selling (i.e., diversion) of these medications to other individuals in these settings. Some research has even indicated that individuals experience threats or direct violence due to the desirability of these medications.
This study examined the safety and preliminary outcomes of the use of depot buprenorphine in a sample of adults serving a correctional sentence in New South Wales, Australia.
HOW WAS THIS STUDY CONDUCTED?
This study was a 16-week non-randomized, open-label trial of 129 adults in correctional care during 2018-2019. The primary outcomes were the safety of depot buprenorphine and diversion of opioid use disorder medication, while secondary outcomes were substance use and treatment retention. The primary trial group of interest was a group who received depot buprenorphine (formulation provided was CAM2038) while the comparator group was comprised of individuals who were already stable on oral methadone. Eligible participants were adults (18 years or older) in custody who had a full-time sentence of 6 months or more before earliest release date, and who had a diagnosis of moderate to severe opioid use disorder according to the DSM-5 criteria.
Following screening for eligibility, all eligible individuals completed research interviews at baseline, and weeks 4 and 16. Participants in the depot buprenorphine group received an initial injection by a trained nurse and were monitored for symptoms for the next hour. Following that initiation, these participants received four doses of depot buprenorphine weekly (day 1, week 1, week 2 and week 3) followed by three doses of depot buprenorphine monthly (week 4, week 8 and week 12). These doses could be increased by the nurse as necessary. Individuals in the methadone arm continued with their treatment as usual (5mg/ml oral liquid solution).
The researchers collected data from the criminal justice system on any medical complications documented by study medical officers, diversion incidents documented by the criminal justice system, and injection site and physical examinations. The researchers – who were independent from staff providing the study medication – also collected face-to-face self-report data at baseline and weeks 4 and 16 of the trial. Participants were asked about their experience hearing about diversion-associated violence or their experience diverting medications. They were also asked about non-prescribed use of opioids, injection drugs, and methamphetamines using the Australian Treatment Outcomes Profile, yielding a binary (yes/no) measures of use in the past 28 days.
Of the sample of 129 adult participants who participated in the trial, 67 were enrolled in the depot buprenorphine group and 62 were enrolled in the comparator group – the stable methadone treatment group. While the majority of both groups were Australian-born, less than half of each group were considered Aboriginal or Torres Strait Islander. The majority of the depot buprenorphine group were male (82%), and on average 35 years old. About half (54%) had completed only their junior year of high school (54%). Those in the depot buprenorphine group had a higher opioid craving score (53 versus 18) and were less likely to previously have used opioid agonist medication (70% versus 97%) than those in the methadone group. While the methadone group were also primarily male (85%), they differed in several ways. First, they were slightly older (on average 38 years old), less likely to have completed junior high school (32%), and as noted above, were more likely to have previously used opioid agonist medication (97% versus 70%).
WHAT DID THIS STUDY FIND?
Medical complications (adverse events) were common but mild.
Of the 67 participants in the depot buprenorphine group, 97% experienced at least one adverse medical complication, with 94% of those being directly due to the study drug. Of those who experienced a medical complication, 88% experienced a mild issue, including injection site pain or swelling, constipation, or headache, that was resolved in a day. There were 4 participants in this group who decided to discontinue their participation in the study because of these complications and one was withdrawn due to another comorbid medical condition. In comparison, of the 62 participants in the methadone group, fewer experienced adverse events (73%), but these were individuals who were considered more stable as they had entered the study already on methadone. Neither group experienced any fatalities. The overall probability of staying in treatment was very high (92%).
Diversion or threats related to it was previously common, but rare during the trial.
At the time of the initial study assessment, 78% of all participants had heard of threats, coercion, or intimidation related to diverting medications for opioid use disorder, and 17% of the participants themselves reported actually diverting these medications while incarcerated. During the study follow-up period, less than 10% had heard about recent intimidation or violence related to diverting medications for opioid use disorder and none of the participants reported diverting medications during this time.
The depot buprenorphine group reduced the prevalence and frequency of substance use.
While 97% of individuals in the depot buprenorphine group used non-prescribed opioids at the beginning of the study (baseline), only 12% of individuals in that group used non-prescribed opioids at 16 weeks. This group also decreased their frequency of non-prescribed opioid use from 22.51 days (baseline) to 2.14 days (16 weeks). Similarly, although 81% of individuals in the depot buprenorphine group reported injecting drugs at baseline, only 17% of individuals in that group injected drugs at 16 weeks. This group also decreased their frequency of injecting drugs from 17.55 days (baseline) to 2.51 days (16 weeks). The decreases in days of opioid and injection use during the trial occurred primarily in the first 4 weeks (see Figure below). There was no change – either in frequency or days of use – for methamphetamines, but this is likely due to low baseline use of methamphetamines among this group (i.e., 0.54 days).
Individuals in the methadone group did not reduce their substance use during the study, but unlike the depot buprenorphine group, they were maintained on methadone at study entry and their levels of substance use were already low. For example, 1% or less of the methadone group used non-prescribed opioids or methamphetamine or injected drugs at study entry.
First, depot buprenorphine, a long-acting injectable medication for opioid use disorder, was found to be safe and acceptable among inmates. Individuals were highly likely to be retained in the treatment, reported primarily only minor medical complications (e.g., related to pain at the injection site), reduced non-prescribed opioid and injection drug use, and were unlikely to report trying to divert their medication. Knowing that most individuals did experience an adverse medical complication such as early injection site pain that subsides within a day may be useful for future implementation as it could be included in provider education and setting expectations with clients to assist with treatment retention.
Second, the comparator group, which more closely mirrors standard practice in criminal justice settings, is a group maintained on methadone. This group did not report diverting medications and did not differ on substance use outcomes over time but overall maintained very low substance use. Although not the primary focus of this study, the methadone group provides additional support for the use of oral methadone in these settings given the primarily positive outcomes and behaviors of the group.
The study setting and approach of examining depot buprenorphine did not allow for a rigorous randomized controlled trial. Instead, this is a pre-post study where the closest comparator is a group of individuals on methadone. The methadone group, however, had very different characteristics from the depot buprenorphine group, so it is important not to make direct comparisons between the two groups.
Although the results were promising for the 16 weeks (approximately 4 months) of the trial, it is unclear how individuals in either group did or would do after that time period. Knowing whether they chose to continue and how effective that experience was, would be helpful to ultimately understanding the sustainability of the depot buprenorphine approach in this setting.
BOTTOM LINE
In this study, the researchers found that among individuals with opioid use disorder in correctional facility care in Australia, the use of both depot buprenorphine and methadone medications was safe, helped to substantially reduce non-prescribed opioid use, and did not result in diversion.
For treatment professionals and treatment systems: The adoption of medication for opioid use disorder treatment programs in jails and prisons depends on the support of leadership and staff in these settings and having a developed infrastructure to sustain these programs. Implementing a long-acting injectable form of medication, that seems to address the contentious issue of diversion may be one way to meet this challenge head-on. Also, the creation of care and transition plans for individuals who initiate medication for opioid use disorder while incarcerated is critical to ensure treatment retention as well as safety after release.
For scientists:Research that more rigorously examines the different medications for opioid use disorder among individuals in correctional or criminal justice settings is needed to replicate and extend these findings. Additional research with more specific populations marginalized in these settings such as females or members of the LGBTQ+ community may also be necessary to understand their experience. In addition to examining the safety and effectiveness of these medications, this research should also focus on system-level issues to identify key barriers and facilitators to adopting and implementing these programs across various legal systems and to ensure availability of these treatments are offered to all inmates.
For policy makers: Although medications such as buprenorphine methadone examined in this study are very helpful life-saving medications for individuals with opioid use disorder, there are many barriers to their implementation in correctional settings throughout the United States. Additional funding to study best ways to implement these treatments and address barriers to implementation will help to expand opioid treatment programs in correctional facilities, which should ultimately help in fighting the opioid overdose epidemic in the United States. Ensuring state and federal policies allow for, and support the dispensing of, these medications in correctional settings, will also be necessary for widespread implementation of these strategies.