Gaps persist in recovery support infrastructure for US inmates with opioid use disorders
Individuals with opioid use disorder have a high risk of overdose after incarceration. The degree to which these criminal justice settings effectively address opioid use disorder may impact how likely such individuals are to initiate and sustain recovery. This study examined the availability of opioid use disorder “best practices” in US jails located in counties heavily impacted by opioid overdose.
This study addressed this public health issue by examining the availability of opioid use disorder “best practices” in jails located in counties heavily impacted by opioid overdose in the U.S.
The opioid use disorder service cascade is one useful way to categorize the different ways that jails and prisons could address substance use disorders, specifically opioid use disorders, to promote recovery and reduce harmful outcomes such as overdoses. This study identified ten opioid use disorder best practices based on current treatment and practice guidelines through the lens of the opioid use disorder service cascade and used these practices to guide their study. These best practices include: (1) screening for opioid use disorder, (2) clinical assessment, (3) medically managed withdrawal, (4) administration of medication for opioid use disorder, (5), medication for opioid use disorder for pregnant individuals, (6) counseling and wrap-around services, (7) collaboration with community providers, (8) assistance with Medicaid or insurance to cover services and treatment, (9) re-entry services after leaving incarceration, and (10) overdose prevention.
The researchers also sought to examine whether the availability of best practices varied across the characteristics of the jails and communities in which they are located. Finally, they asked individuals employed in the criminal justice system what type of training, technical assistance, and resources are needed to expand the availability of best practices for addressing opioid use disorder in jails.
HOW WAS THIS STUDY CONDUCTED?
The researchers identified 244 counties in the US that had the highest concentrations of opioid-overdose mortality from a 2017 dataset. These counties were selected for inclusion in this study using two indicators of opioid use disorder severity: 1) the sample of counties that accounted for half of all opioid-related deaths in the US and 2) counties that had a significantly higher rate of opioid-related deaths per 100,000 people than the national average (20.3 versus 14.7). Once the counties were identified, the study team identified jails in those counties and sought out staff representatives from those jails to engage in the study.
The researchers completed structured interviews from December 2019 to February 2021 with representatives from 76% of the 244 targeted counties and 74% of the 250 targeted jails in these counties. Respondent jails were more likely than non-respondents to be from counties that have larger populations, fewer people living below the federal poverty line, and lower population incarceration rates per 100,000 overall.
Completing the structured interviews with jails often took several attempts as multiple jail representatives were needed to answer some of the interview questions. The structured interviews used questions to assess the availability and accessibility of the following in the previous 12 months: (1) opioid withdrawal management, (2) screening and assessment to identify opioid use problems, (3) provision of medication for opioid use disorder, including eligibility, reasons for use, and restrictions on use, (4) re-entry planning and services, (5) overdose prevention services, and (6) needs for training, technical assistance, and resources to improve their ability to provide opioid use disorder services.
Using results from the survey on these issues, the researchers created a summary score for the percentage of services provided across the 10 best-practice categories (range 0–100%), which was used to categorize jails into 2 groups based on the median of the summary score (i.e., 50% of the data points have a value smaller or equal to the median and 50% of data points have a value higher or equal to the median). In this case, the median was 67%, so they created a low best practices group (0–67% of items endorsed) and a high best practices group (above 67%). The information collected from jails was linked to county-level demographic data including gender, racial, and ethnic demographics, population rate of incarceration, urbanicity, level of poverty in the county in which the jail was located, and availability of providers who could prescribe medication for opioid use disorder in the county.
Among the study sample of jails surveyed, nearly all (95%) are under the auspices of the Sheriff’s office or the county. Most jails house both males and females (96%). Three-fourths indicated that they contract out for healthcare services. The average number of admissions during the 12-month reference period of 2019 was 17,232 (SD = 57,710) for a total of 3,187,920 admissions during that 12-month period.
WHAT DID THIS STUDY FIND?
Most jails offered some of the ten best practices, but some practices were far more common than others.
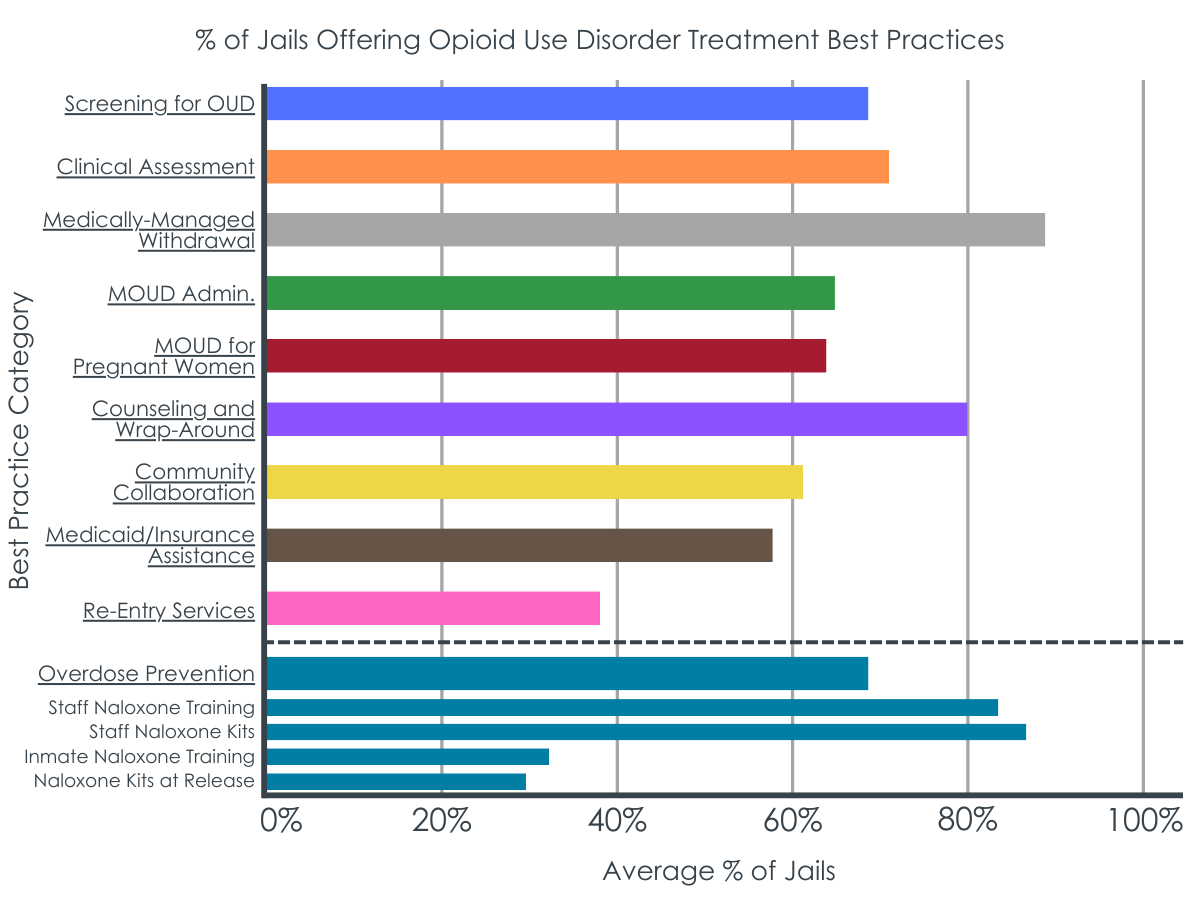
Over 70% of jail respondents indicated that some aspects of each of the ten opioid use disorder best practices were available within their jails, ranging from 71% using clinical assessment to 88% engaging in medically managed withdrawal. As well, of the jails offering overdose prevention, 96% of jails reported doing at least one of the following: provide staff training on how to use Naloxone, provide staff with Naloxone kits to reverse overdose in jail, provide education and training to individuals while incarcerated on how to use Naloxone, and provide individuals with Naloxone kits at release.
Re-entry services were the lowest endorsed category of best practices, with an average of only 38% of jails endorsing options; of these only 18% reported providing written prescriptions for medication for opioid use disorder as part of re-entry. This potentially presents a large barrier to individuals returning to communities where they would need to see a new practitioner for a prescription in addition to other re-entry tasks (finding housing, employment, etc.).
The best-practice groups – high vs. low implementation jails – were different on several key characteristics.
Jails in the high best-practices group had a higher total population mean than the low group (748,391 vs. 434,857), a higher proportion of Hispanic residents (13% vs. 8%), and a slightly lower proportion of residents living in poverty (12% vs. 14%). Jails in the high group had lower average annual jail admissions (3682 vs. 5739) and lower average rates of jail admission per 100,000 population overall (296 vs. 347), as well as specifically for females (86 vs. 108), males (512 vs. 591), and white, non-Hispanics (219 vs. 267).
Jails identified a variety of needs related to funding, education and training, clinical capacity and stigma to improve meeting best practices for opioid use disorders.
Jails most often indicated that to improve best practices, funding was needed, for medication, clinical staff, tools, and methods to prevent diversion of medication, transportation to services that offer medication for opioid use disorder, and medication for opioid use disorder in the community. The majority of jails reported that education and training needs were necessary across a range of local stakeholders from state/local politicians and to pregnant inmates. Two-thirds also felt that addressing stigma was important to increase access to best practices. Finally, given the low numbers of jails addressing re-entry support, re-entry support needs were also commonly endorsed in the needs assessments.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of jails in the US counties with the highest opioid-overdose mortality highlights positive steps and existing challenges in addressing opioid use disorder in these criminal justice settings.
The findings are encouraging in that a substantial percentage of jails have implemented various best practices, including screening for opioid use disorder, clinical assessment, medication for opioid use disorder that also includes counseling and wrap-around services, and medically managed withdrawal. These practices, especially the use of medication to address opioid use disorder that is maintained by individuals for their entire jail term, are likely to help prevent return to opioid use after re-entry. Additionally, the widespread adoption of measures to prevent overdoses, such as Naloxone training and distribution, highlights the perceived importance of harm reduction practices within these settings. That said, the lower endorsement of re-entry services, particularly the provision of written prescriptions for medication for opioid use disorder, underscores a critical gap at a critical juncture in the continuum of care. The need for written prescriptions for medication for opioid use disorder can be a significant barrier, potentially leading to disruptions in treatment continuity. Indeed, previous research with jail inmates has demonstrated the uncertainty felt in the process of transitioning from the jail’s medication treatment program to a community-based program. Given the many challenges associated with re-entry, including finding housing and employment, and accessing healthcare, it may be helpful to begin the transition process at earlier stages of incarceration. Such work might include providing inmates with resources like peer recovery navigators to support the transition to community care and prevent opioid misuse and related overdose deaths post incarceration. Implementing education and support programs within jails that specifically address the challenges of re-entry, including support for getting prescriptions and medication management, may also better prepare individuals for the transition back into the community.
The study also provides some demographic and operational differences between jails in the high and low best-practices groups for addressing opioid use disorders to explore in future research. These differences can offer insights into potential factors influencing the implementation of best practices in these settings. As jails in the high best-practices group had a larger population and a lower proportion of residents in the county living below the federal poverty line, this suggests that a greater census and more community resources (e.g., via resident taxes) could allow for more resources and infrastructure to support the implementation of best practices. Finally, the best-practice jails had lower average annual jail admissions and lower average rates of jail admission suggesting that these jails may be dealing with a lower influx of individuals, allowing for more focused management and potentially more effective implementation of best practices.
Addressing the challenges highlighted in this study likely requires a multi-faceted approach that involves coordination among jails, healthcare providers, community organizations, and policymakers. By using a recovery-oriented system of care framework to focus on comprehensive and integrated strategies, many of these systemic gaps could be addressed. Establishing strong collaborations between correctional facilities and community healthcare providers is crucial to reducing the clinical and public health harms of opioid and other substance use. This collaboration can facilitate the transfer of medical information, prescriptions, and support services, easing the re-entry process.
These were self-report data from individuals in various positions at the jails who may or may not have had complete knowledge of services offered, or if offered, knowledge of the reality of implementation on a day-to-day basis. In addition, jail staff were first asked about their engagement in the best practices, and then asked about their needs to improve the availability of best practices in the jail, so it is possible that their responses related to perceived needs were influenced by having been potentially “primed” by the initial best practice assessment. This study is a first start to understand what these jails need to implement best practices for opioid use disorder, but addressing these issues will likely need a more in-depth and focused approach for each jail system.
Although these observations suggest that the implementation of best practices for addressing opioid use disorders may be influenced by a combination of demographic factors, population size, and admission rates, the nature of the study design does not allow the direct linkage of highest/lowest practices with county-level data. Yet, understanding these patterns may support future research in examining the effect of tailoring interventions and resource allocation to the specific needs and challenges of different jail settings.
BOTTOM LINE
A significant percentage of jails in counties with high opioid mortality burden have implemented various best practices to address opioid use disorder among inmates. Yet, there are many areas for improvement and the lower endorsement of re-entry services highlights a critical gap in the continuum of care.
For individuals and families seeking recovery: Individuals who are provided with medication for opioid use disorder in the context of jail or prison might benefit from active support across their network, including from healthcare providers, family, and friends. Navigating community systems and resources after release from incarceration may be particularly challenging when transition planning support is not offered in the jail itself as this study suggests happens often.
For treatment professionals and treatment systems: Healthcare systems and the criminal justice system could partner to facilitate inmate transitions to community-based opioid use disorder treatment and ongoing support services. By addressing the intersection of healthcare and criminal justice, these partnerships could create a more holistic and effective approach to opioid use disorder treatment. This would benefit individuals in recovery while also promoting public health and safety and optimizing resource utilization.
For scientists: This study highlighted several gaps and areas for improvement to better support individuals with opioid use disorder when they enter jail and throughout their time there until they transition back to the community. As well, this study focused on counties that had the worst opioid-related mortalities in the two years prior to data collection. It is possible that as a result of that, those counties have begun to make changes to address this public health crisis. Research that examines this issue across all counties, e.g., those with both high and low opioid-related mortality, may be necessary to better understand how to make criminal justice system-level changes to address policies and practices nationwide. Additionally, future studies that more closely examine this process in more detail (e.g., via ethnography) within specific types of communities may be necessary to identify unique opportunities and barriers to leverage existing resources and create new ones.
For policy makers: Jail representatives suggested several areas where system-level improvements could be made to better support individuals with opioid use disorder in jail and during the re-entry process. Implementing policies that can promote the integration of substance use disorder treatment into jails and more comprehensive jail healthcare policies may have a lasting impact on improving the continuum of care for these individuals in cost efficient ways.
This study addressed this public health issue by examining the availability of opioid use disorder “best practices” in jails located in counties heavily impacted by opioid overdose in the U.S.
The opioid use disorder service cascade is one useful way to categorize the different ways that jails and prisons could address substance use disorders, specifically opioid use disorders, to promote recovery and reduce harmful outcomes such as overdoses. This study identified ten opioid use disorder best practices based on current treatment and practice guidelines through the lens of the opioid use disorder service cascade and used these practices to guide their study. These best practices include: (1) screening for opioid use disorder, (2) clinical assessment, (3) medically managed withdrawal, (4) administration of medication for opioid use disorder, (5), medication for opioid use disorder for pregnant individuals, (6) counseling and wrap-around services, (7) collaboration with community providers, (8) assistance with Medicaid or insurance to cover services and treatment, (9) re-entry services after leaving incarceration, and (10) overdose prevention.
The researchers also sought to examine whether the availability of best practices varied across the characteristics of the jails and communities in which they are located. Finally, they asked individuals employed in the criminal justice system what type of training, technical assistance, and resources are needed to expand the availability of best practices for addressing opioid use disorder in jails.
HOW WAS THIS STUDY CONDUCTED?
The researchers identified 244 counties in the US that had the highest concentrations of opioid-overdose mortality from a 2017 dataset. These counties were selected for inclusion in this study using two indicators of opioid use disorder severity: 1) the sample of counties that accounted for half of all opioid-related deaths in the US and 2) counties that had a significantly higher rate of opioid-related deaths per 100,000 people than the national average (20.3 versus 14.7). Once the counties were identified, the study team identified jails in those counties and sought out staff representatives from those jails to engage in the study.
The researchers completed structured interviews from December 2019 to February 2021 with representatives from 76% of the 244 targeted counties and 74% of the 250 targeted jails in these counties. Respondent jails were more likely than non-respondents to be from counties that have larger populations, fewer people living below the federal poverty line, and lower population incarceration rates per 100,000 overall.
Completing the structured interviews with jails often took several attempts as multiple jail representatives were needed to answer some of the interview questions. The structured interviews used questions to assess the availability and accessibility of the following in the previous 12 months: (1) opioid withdrawal management, (2) screening and assessment to identify opioid use problems, (3) provision of medication for opioid use disorder, including eligibility, reasons for use, and restrictions on use, (4) re-entry planning and services, (5) overdose prevention services, and (6) needs for training, technical assistance, and resources to improve their ability to provide opioid use disorder services.
Using results from the survey on these issues, the researchers created a summary score for the percentage of services provided across the 10 best-practice categories (range 0–100%), which was used to categorize jails into 2 groups based on the median of the summary score (i.e., 50% of the data points have a value smaller or equal to the median and 50% of data points have a value higher or equal to the median). In this case, the median was 67%, so they created a low best practices group (0–67% of items endorsed) and a high best practices group (above 67%). The information collected from jails was linked to county-level demographic data including gender, racial, and ethnic demographics, population rate of incarceration, urbanicity, level of poverty in the county in which the jail was located, and availability of providers who could prescribe medication for opioid use disorder in the county.
Among the study sample of jails surveyed, nearly all (95%) are under the auspices of the Sheriff’s office or the county. Most jails house both males and females (96%). Three-fourths indicated that they contract out for healthcare services. The average number of admissions during the 12-month reference period of 2019 was 17,232 (SD = 57,710) for a total of 3,187,920 admissions during that 12-month period.
WHAT DID THIS STUDY FIND?
Most jails offered some of the ten best practices, but some practices were far more common than others.
Over 70% of jail respondents indicated that some aspects of each of the ten opioid use disorder best practices were available within their jails, ranging from 71% using clinical assessment to 88% engaging in medically managed withdrawal. As well, of the jails offering overdose prevention, 96% of jails reported doing at least one of the following: provide staff training on how to use Naloxone, provide staff with Naloxone kits to reverse overdose in jail, provide education and training to individuals while incarcerated on how to use Naloxone, and provide individuals with Naloxone kits at release.
Re-entry services were the lowest endorsed category of best practices, with an average of only 38% of jails endorsing options; of these only 18% reported providing written prescriptions for medication for opioid use disorder as part of re-entry. This potentially presents a large barrier to individuals returning to communities where they would need to see a new practitioner for a prescription in addition to other re-entry tasks (finding housing, employment, etc.).
The best-practice groups – high vs. low implementation jails – were different on several key characteristics.
Jails in the high best-practices group had a higher total population mean than the low group (748,391 vs. 434,857), a higher proportion of Hispanic residents (13% vs. 8%), and a slightly lower proportion of residents living in poverty (12% vs. 14%). Jails in the high group had lower average annual jail admissions (3682 vs. 5739) and lower average rates of jail admission per 100,000 population overall (296 vs. 347), as well as specifically for females (86 vs. 108), males (512 vs. 591), and white, non-Hispanics (219 vs. 267).
Jails identified a variety of needs related to funding, education and training, clinical capacity and stigma to improve meeting best practices for opioid use disorders.
Jails most often indicated that to improve best practices, funding was needed, for medication, clinical staff, tools, and methods to prevent diversion of medication, transportation to services that offer medication for opioid use disorder, and medication for opioid use disorder in the community. The majority of jails reported that education and training needs were necessary across a range of local stakeholders from state/local politicians and to pregnant inmates. Two-thirds also felt that addressing stigma was important to increase access to best practices. Finally, given the low numbers of jails addressing re-entry support, re-entry support needs were also commonly endorsed in the needs assessments.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of jails in the US counties with the highest opioid-overdose mortality highlights positive steps and existing challenges in addressing opioid use disorder in these criminal justice settings.
The findings are encouraging in that a substantial percentage of jails have implemented various best practices, including screening for opioid use disorder, clinical assessment, medication for opioid use disorder that also includes counseling and wrap-around services, and medically managed withdrawal. These practices, especially the use of medication to address opioid use disorder that is maintained by individuals for their entire jail term, are likely to help prevent return to opioid use after re-entry. Additionally, the widespread adoption of measures to prevent overdoses, such as Naloxone training and distribution, highlights the perceived importance of harm reduction practices within these settings. That said, the lower endorsement of re-entry services, particularly the provision of written prescriptions for medication for opioid use disorder, underscores a critical gap at a critical juncture in the continuum of care. The need for written prescriptions for medication for opioid use disorder can be a significant barrier, potentially leading to disruptions in treatment continuity. Indeed, previous research with jail inmates has demonstrated the uncertainty felt in the process of transitioning from the jail’s medication treatment program to a community-based program. Given the many challenges associated with re-entry, including finding housing and employment, and accessing healthcare, it may be helpful to begin the transition process at earlier stages of incarceration. Such work might include providing inmates with resources like peer recovery navigators to support the transition to community care and prevent opioid misuse and related overdose deaths post incarceration. Implementing education and support programs within jails that specifically address the challenges of re-entry, including support for getting prescriptions and medication management, may also better prepare individuals for the transition back into the community.
The study also provides some demographic and operational differences between jails in the high and low best-practices groups for addressing opioid use disorders to explore in future research. These differences can offer insights into potential factors influencing the implementation of best practices in these settings. As jails in the high best-practices group had a larger population and a lower proportion of residents in the county living below the federal poverty line, this suggests that a greater census and more community resources (e.g., via resident taxes) could allow for more resources and infrastructure to support the implementation of best practices. Finally, the best-practice jails had lower average annual jail admissions and lower average rates of jail admission suggesting that these jails may be dealing with a lower influx of individuals, allowing for more focused management and potentially more effective implementation of best practices.
Addressing the challenges highlighted in this study likely requires a multi-faceted approach that involves coordination among jails, healthcare providers, community organizations, and policymakers. By using a recovery-oriented system of care framework to focus on comprehensive and integrated strategies, many of these systemic gaps could be addressed. Establishing strong collaborations between correctional facilities and community healthcare providers is crucial to reducing the clinical and public health harms of opioid and other substance use. This collaboration can facilitate the transfer of medical information, prescriptions, and support services, easing the re-entry process.
These were self-report data from individuals in various positions at the jails who may or may not have had complete knowledge of services offered, or if offered, knowledge of the reality of implementation on a day-to-day basis. In addition, jail staff were first asked about their engagement in the best practices, and then asked about their needs to improve the availability of best practices in the jail, so it is possible that their responses related to perceived needs were influenced by having been potentially “primed” by the initial best practice assessment. This study is a first start to understand what these jails need to implement best practices for opioid use disorder, but addressing these issues will likely need a more in-depth and focused approach for each jail system.
Although these observations suggest that the implementation of best practices for addressing opioid use disorders may be influenced by a combination of demographic factors, population size, and admission rates, the nature of the study design does not allow the direct linkage of highest/lowest practices with county-level data. Yet, understanding these patterns may support future research in examining the effect of tailoring interventions and resource allocation to the specific needs and challenges of different jail settings.
BOTTOM LINE
A significant percentage of jails in counties with high opioid mortality burden have implemented various best practices to address opioid use disorder among inmates. Yet, there are many areas for improvement and the lower endorsement of re-entry services highlights a critical gap in the continuum of care.
For individuals and families seeking recovery: Individuals who are provided with medication for opioid use disorder in the context of jail or prison might benefit from active support across their network, including from healthcare providers, family, and friends. Navigating community systems and resources after release from incarceration may be particularly challenging when transition planning support is not offered in the jail itself as this study suggests happens often.
For treatment professionals and treatment systems: Healthcare systems and the criminal justice system could partner to facilitate inmate transitions to community-based opioid use disorder treatment and ongoing support services. By addressing the intersection of healthcare and criminal justice, these partnerships could create a more holistic and effective approach to opioid use disorder treatment. This would benefit individuals in recovery while also promoting public health and safety and optimizing resource utilization.
For scientists: This study highlighted several gaps and areas for improvement to better support individuals with opioid use disorder when they enter jail and throughout their time there until they transition back to the community. As well, this study focused on counties that had the worst opioid-related mortalities in the two years prior to data collection. It is possible that as a result of that, those counties have begun to make changes to address this public health crisis. Research that examines this issue across all counties, e.g., those with both high and low opioid-related mortality, may be necessary to better understand how to make criminal justice system-level changes to address policies and practices nationwide. Additionally, future studies that more closely examine this process in more detail (e.g., via ethnography) within specific types of communities may be necessary to identify unique opportunities and barriers to leverage existing resources and create new ones.
For policy makers: Jail representatives suggested several areas where system-level improvements could be made to better support individuals with opioid use disorder in jail and during the re-entry process. Implementing policies that can promote the integration of substance use disorder treatment into jails and more comprehensive jail healthcare policies may have a lasting impact on improving the continuum of care for these individuals in cost efficient ways.
This study addressed this public health issue by examining the availability of opioid use disorder “best practices” in jails located in counties heavily impacted by opioid overdose in the U.S.
The opioid use disorder service cascade is one useful way to categorize the different ways that jails and prisons could address substance use disorders, specifically opioid use disorders, to promote recovery and reduce harmful outcomes such as overdoses. This study identified ten opioid use disorder best practices based on current treatment and practice guidelines through the lens of the opioid use disorder service cascade and used these practices to guide their study. These best practices include: (1) screening for opioid use disorder, (2) clinical assessment, (3) medically managed withdrawal, (4) administration of medication for opioid use disorder, (5), medication for opioid use disorder for pregnant individuals, (6) counseling and wrap-around services, (7) collaboration with community providers, (8) assistance with Medicaid or insurance to cover services and treatment, (9) re-entry services after leaving incarceration, and (10) overdose prevention.
The researchers also sought to examine whether the availability of best practices varied across the characteristics of the jails and communities in which they are located. Finally, they asked individuals employed in the criminal justice system what type of training, technical assistance, and resources are needed to expand the availability of best practices for addressing opioid use disorder in jails.
HOW WAS THIS STUDY CONDUCTED?
The researchers identified 244 counties in the US that had the highest concentrations of opioid-overdose mortality from a 2017 dataset. These counties were selected for inclusion in this study using two indicators of opioid use disorder severity: 1) the sample of counties that accounted for half of all opioid-related deaths in the US and 2) counties that had a significantly higher rate of opioid-related deaths per 100,000 people than the national average (20.3 versus 14.7). Once the counties were identified, the study team identified jails in those counties and sought out staff representatives from those jails to engage in the study.
The researchers completed structured interviews from December 2019 to February 2021 with representatives from 76% of the 244 targeted counties and 74% of the 250 targeted jails in these counties. Respondent jails were more likely than non-respondents to be from counties that have larger populations, fewer people living below the federal poverty line, and lower population incarceration rates per 100,000 overall.
Completing the structured interviews with jails often took several attempts as multiple jail representatives were needed to answer some of the interview questions. The structured interviews used questions to assess the availability and accessibility of the following in the previous 12 months: (1) opioid withdrawal management, (2) screening and assessment to identify opioid use problems, (3) provision of medication for opioid use disorder, including eligibility, reasons for use, and restrictions on use, (4) re-entry planning and services, (5) overdose prevention services, and (6) needs for training, technical assistance, and resources to improve their ability to provide opioid use disorder services.
Using results from the survey on these issues, the researchers created a summary score for the percentage of services provided across the 10 best-practice categories (range 0–100%), which was used to categorize jails into 2 groups based on the median of the summary score (i.e., 50% of the data points have a value smaller or equal to the median and 50% of data points have a value higher or equal to the median). In this case, the median was 67%, so they created a low best practices group (0–67% of items endorsed) and a high best practices group (above 67%). The information collected from jails was linked to county-level demographic data including gender, racial, and ethnic demographics, population rate of incarceration, urbanicity, level of poverty in the county in which the jail was located, and availability of providers who could prescribe medication for opioid use disorder in the county.
Among the study sample of jails surveyed, nearly all (95%) are under the auspices of the Sheriff’s office or the county. Most jails house both males and females (96%). Three-fourths indicated that they contract out for healthcare services. The average number of admissions during the 12-month reference period of 2019 was 17,232 (SD = 57,710) for a total of 3,187,920 admissions during that 12-month period.
WHAT DID THIS STUDY FIND?
Most jails offered some of the ten best practices, but some practices were far more common than others.
Over 70% of jail respondents indicated that some aspects of each of the ten opioid use disorder best practices were available within their jails, ranging from 71% using clinical assessment to 88% engaging in medically managed withdrawal. As well, of the jails offering overdose prevention, 96% of jails reported doing at least one of the following: provide staff training on how to use Naloxone, provide staff with Naloxone kits to reverse overdose in jail, provide education and training to individuals while incarcerated on how to use Naloxone, and provide individuals with Naloxone kits at release.
Re-entry services were the lowest endorsed category of best practices, with an average of only 38% of jails endorsing options; of these only 18% reported providing written prescriptions for medication for opioid use disorder as part of re-entry. This potentially presents a large barrier to individuals returning to communities where they would need to see a new practitioner for a prescription in addition to other re-entry tasks (finding housing, employment, etc.).
The best-practice groups – high vs. low implementation jails – were different on several key characteristics.
Jails in the high best-practices group had a higher total population mean than the low group (748,391 vs. 434,857), a higher proportion of Hispanic residents (13% vs. 8%), and a slightly lower proportion of residents living in poverty (12% vs. 14%). Jails in the high group had lower average annual jail admissions (3682 vs. 5739) and lower average rates of jail admission per 100,000 population overall (296 vs. 347), as well as specifically for females (86 vs. 108), males (512 vs. 591), and white, non-Hispanics (219 vs. 267).
Jails identified a variety of needs related to funding, education and training, clinical capacity and stigma to improve meeting best practices for opioid use disorders.
Jails most often indicated that to improve best practices, funding was needed, for medication, clinical staff, tools, and methods to prevent diversion of medication, transportation to services that offer medication for opioid use disorder, and medication for opioid use disorder in the community. The majority of jails reported that education and training needs were necessary across a range of local stakeholders from state/local politicians and to pregnant inmates. Two-thirds also felt that addressing stigma was important to increase access to best practices. Finally, given the low numbers of jails addressing re-entry support, re-entry support needs were also commonly endorsed in the needs assessments.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of jails in the US counties with the highest opioid-overdose mortality highlights positive steps and existing challenges in addressing opioid use disorder in these criminal justice settings.
The findings are encouraging in that a substantial percentage of jails have implemented various best practices, including screening for opioid use disorder, clinical assessment, medication for opioid use disorder that also includes counseling and wrap-around services, and medically managed withdrawal. These practices, especially the use of medication to address opioid use disorder that is maintained by individuals for their entire jail term, are likely to help prevent return to opioid use after re-entry. Additionally, the widespread adoption of measures to prevent overdoses, such as Naloxone training and distribution, highlights the perceived importance of harm reduction practices within these settings. That said, the lower endorsement of re-entry services, particularly the provision of written prescriptions for medication for opioid use disorder, underscores a critical gap at a critical juncture in the continuum of care. The need for written prescriptions for medication for opioid use disorder can be a significant barrier, potentially leading to disruptions in treatment continuity. Indeed, previous research with jail inmates has demonstrated the uncertainty felt in the process of transitioning from the jail’s medication treatment program to a community-based program. Given the many challenges associated with re-entry, including finding housing and employment, and accessing healthcare, it may be helpful to begin the transition process at earlier stages of incarceration. Such work might include providing inmates with resources like peer recovery navigators to support the transition to community care and prevent opioid misuse and related overdose deaths post incarceration. Implementing education and support programs within jails that specifically address the challenges of re-entry, including support for getting prescriptions and medication management, may also better prepare individuals for the transition back into the community.
The study also provides some demographic and operational differences between jails in the high and low best-practices groups for addressing opioid use disorders to explore in future research. These differences can offer insights into potential factors influencing the implementation of best practices in these settings. As jails in the high best-practices group had a larger population and a lower proportion of residents in the county living below the federal poverty line, this suggests that a greater census and more community resources (e.g., via resident taxes) could allow for more resources and infrastructure to support the implementation of best practices. Finally, the best-practice jails had lower average annual jail admissions and lower average rates of jail admission suggesting that these jails may be dealing with a lower influx of individuals, allowing for more focused management and potentially more effective implementation of best practices.
Addressing the challenges highlighted in this study likely requires a multi-faceted approach that involves coordination among jails, healthcare providers, community organizations, and policymakers. By using a recovery-oriented system of care framework to focus on comprehensive and integrated strategies, many of these systemic gaps could be addressed. Establishing strong collaborations between correctional facilities and community healthcare providers is crucial to reducing the clinical and public health harms of opioid and other substance use. This collaboration can facilitate the transfer of medical information, prescriptions, and support services, easing the re-entry process.
These were self-report data from individuals in various positions at the jails who may or may not have had complete knowledge of services offered, or if offered, knowledge of the reality of implementation on a day-to-day basis. In addition, jail staff were first asked about their engagement in the best practices, and then asked about their needs to improve the availability of best practices in the jail, so it is possible that their responses related to perceived needs were influenced by having been potentially “primed” by the initial best practice assessment. This study is a first start to understand what these jails need to implement best practices for opioid use disorder, but addressing these issues will likely need a more in-depth and focused approach for each jail system.
Although these observations suggest that the implementation of best practices for addressing opioid use disorders may be influenced by a combination of demographic factors, population size, and admission rates, the nature of the study design does not allow the direct linkage of highest/lowest practices with county-level data. Yet, understanding these patterns may support future research in examining the effect of tailoring interventions and resource allocation to the specific needs and challenges of different jail settings.
BOTTOM LINE
A significant percentage of jails in counties with high opioid mortality burden have implemented various best practices to address opioid use disorder among inmates. Yet, there are many areas for improvement and the lower endorsement of re-entry services highlights a critical gap in the continuum of care.
For individuals and families seeking recovery: Individuals who are provided with medication for opioid use disorder in the context of jail or prison might benefit from active support across their network, including from healthcare providers, family, and friends. Navigating community systems and resources after release from incarceration may be particularly challenging when transition planning support is not offered in the jail itself as this study suggests happens often.
For treatment professionals and treatment systems: Healthcare systems and the criminal justice system could partner to facilitate inmate transitions to community-based opioid use disorder treatment and ongoing support services. By addressing the intersection of healthcare and criminal justice, these partnerships could create a more holistic and effective approach to opioid use disorder treatment. This would benefit individuals in recovery while also promoting public health and safety and optimizing resource utilization.
For scientists: This study highlighted several gaps and areas for improvement to better support individuals with opioid use disorder when they enter jail and throughout their time there until they transition back to the community. As well, this study focused on counties that had the worst opioid-related mortalities in the two years prior to data collection. It is possible that as a result of that, those counties have begun to make changes to address this public health crisis. Research that examines this issue across all counties, e.g., those with both high and low opioid-related mortality, may be necessary to better understand how to make criminal justice system-level changes to address policies and practices nationwide. Additionally, future studies that more closely examine this process in more detail (e.g., via ethnography) within specific types of communities may be necessary to identify unique opportunities and barriers to leverage existing resources and create new ones.
For policy makers: Jail representatives suggested several areas where system-level improvements could be made to better support individuals with opioid use disorder in jail and during the re-entry process. Implementing policies that can promote the integration of substance use disorder treatment into jails and more comprehensive jail healthcare policies may have a lasting impact on improving the continuum of care for these individuals in cost efficient ways.