Greater treatment challenges for those involved in the criminal justice system if living with co-occurring opioid use and mental health disorders
Many individuals in the criminal-legal system with an opioid use disorder also experience mental health disorders. There is a lack of evidence-based treatment for this population within jails and prisons. This study examined how co-occurring opioid use and mental health disorders impact individuals transitioning from the criminal-legal system to community-based treatment, and whether treatment helps address the added burden of a mental health disorder.
It is common for individuals with opioid use disorders in the criminal-legal system also to experience mental health disorders. There is a lack of evidence-based treatment for individuals with opioid use disorders, as well as for co-occurring opioid use and mental health disorders, within jails and prisons. This leaves a major service gap at a critical point in time when individuals may be most likely to engage in services due to the structure of the criminal legal system.
When individuals with these co-occurring disorders transition back to their communities, there is increased risk as they attempt to resume their lives back in the very conditions that led to their incarceration. Engaging in treatment or recovery support is also difficult during this period as individuals released from prison or jail are faced with many barriers to access, including lack of adequate health insurance and active linkages to these services. Even navigating health insurance and referrals can be stressful and burdensome at a time when individuals are trying to reestablish themselves in the community and to identify a source of stable income.
This study sought to improve understanding of how a co-occurring mental health disorder impacts individuals with opioid use disorder and criminal system involvement, and whether community-based treatment may help offset any additional risk. They did this by examining the following four areas: (1) the prevalence of co-occurring opioid use and mental health disorders, (2) the effects of co-occurring mental health disorders on crime recidivism outcomes, (3) the effects of co-occurring mental health disorders on psychiatric recovery outcomes, and (4) whether co-occurring mental health changes how individuals engage in community-based treatment and outcomes.
HOW WAS THIS STUDY CONDUCTED?
This was secondary data analysis of individuals with opioid use disorder enrolled in the Recovery Works program between October 2015 and March 2018. Recovery Works is a voucher-based system to cover behavioral health services. It is only available to adults in Indiana who have an open criminal-legal case with a felony level charge (or prior felony conviction), who have an income lower than 200% of the federal income poverty level, and who are not covered by other forms of health insurance. The researchers used client data from only those individuals who had a baseline assessment and a subsequent episode of care.
The researchers included the following individual demographic characteristics in the analysis: any lifetime history of prior substance use treatment, felony charge one year prior to starting an episode of care, age at time of Recovery Works enrollment, sex, race (White, non-White), completed episode of care, and length of time in treatment. They used client records provided by Recovery Works to the Data Assessment Registry Mental Health and Addiction system to determine whether clients had a co-occurring mental health disorder with their opioid use disorder. The study did not provide information regarding how Recovery Works conducted assessments to determine substance use and mental health diagnoses used in their analyses.
The number of treatment contacts including substance use outpatient (e.g., intensive outpatient treatment for substance use disorder, medications for opioid use disorder, etc.), group therapy for mental health, and individual therapy (“person-centered and interactive psychiatric interviews) at 3-month, 6-month, and 12-months were collected from Recovery Works billing code data.
For outcome variables, the authors used results from the Recovery Works Adult Needs and Strengths Assessment at baseline and completion of treatment including life functioning (for example, employment, social functioning, residential stability), strengths (for example, social connectedness, education, and family strengths), and behavioral health needs (for example, depression, interpersonal problems, and substance use). These domains were analyzed as scale scores where higher scores indicated worse outcomes. That is, higher scores on the life functioning and behavioral health scales indicated a dangerous or disabling need and higher scores on the strengths scale indicated fewer strengths. Recidivism, or return to crime, was defined as any charge at 3-month, 6-month, and 12-months following the start of an episode of care. Recidivism was collected from court records.
The sample in this study was made up of 2039 clients in the Recovery Works program. The majority were white (90%) and male (59%) and were on average 32 years old (SD = 8). They had an average of 6.9 months (SD = 3.8) in the Recovery Works program and approximately 50% of clients fully completed their episode of care. Nearly half (47%) of clients had a co-occurring mental health disorder: the most common diagnoses were depressive disorders (33%), anxiety disorders (24%), and PTSD (21%).
WHAT DID THIS STUDY FIND?
Co-occurring mental health disorder was associated with greater treatment engagement but not crime recidivism.
At all follow-ups, individuals with a co-occurring disorder had higher service utilization than individuals with only an opioid use disorder and no mental health disorder. These individuals attended more substance use outpatient, group psychotherapy, and individual psychotherapy services. Although rates of service use were still very low, more clients with a co-occurring disorder used both substance use outpatient and psychotherapy services at 12-months (13%) compared to clients without a co-occurring disorder (6%). Clients with a co-occurring disorder were also more likely to complete their episode of care. There were no differences between clients with and without a co-occurring disorder for any criminal charge at all follow-ups. Also of note, clients with a co-occurring disorder were more likely to be female compared to clients without a co-occurring disorder.
Using treatment services decreased the likelihood of a criminal charge.
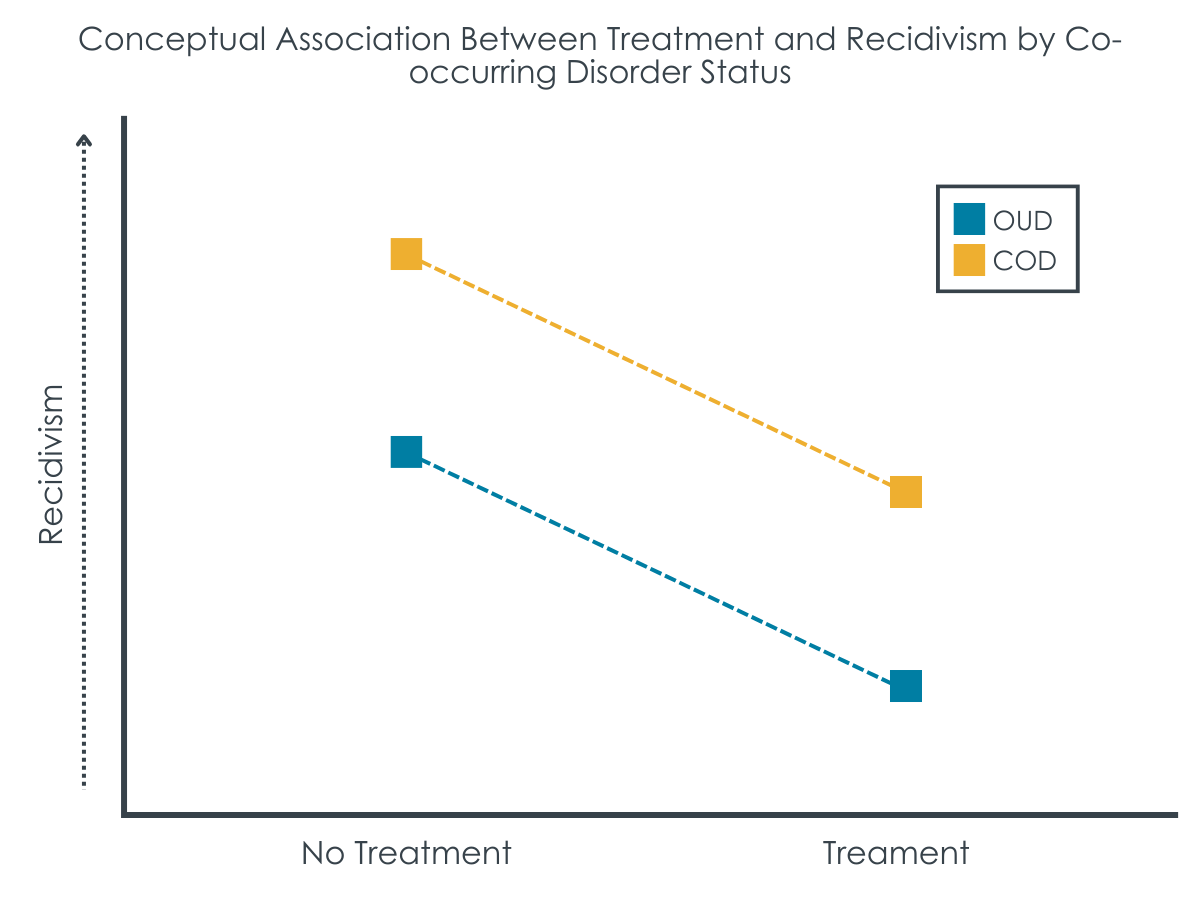
Use of any type of treatment services decreased the likelihood of a criminal charge, but group therapy had the greatest association as it reduced this likelihood at every follow-up. Individual therapy only reduced the likelihood of a criminal charge at 6- and 12-months, while substance use outpatient treatment was not associated with the likelihood of a criminal charge. When examining treatment usage by the presence of a co-occurring disorder, participants with and without a mental health disorder generally had similar, positive effects of treatment on reduced likelihood of another criminal charge over the 1-year follow-up.
Figure. While having a co-occurring disorder was associated with higher likelihood of a criminal charge, both groups experienced associated benefit from treatment.
Co-occurring mental health disorder associated with more behavioral health needs; only group therapy linked to better functioning.
In the group of 516 participants who completed a 12-month follow-up assessment, controlling for functioning when they entered the 12-month program, at completion those with a mental health disorder had more pronounced behavioral health needs. Although individual therapy services predicted worse life functioning at completion of care, the use of substance use outpatient services predicted better life functioning and the use of group therapy predicted better life functioning, behavioral health, and strengths.
Group therapy for mental health, not substance use or individual psychotherapy, associated with more gains for co-occurring disorder group.
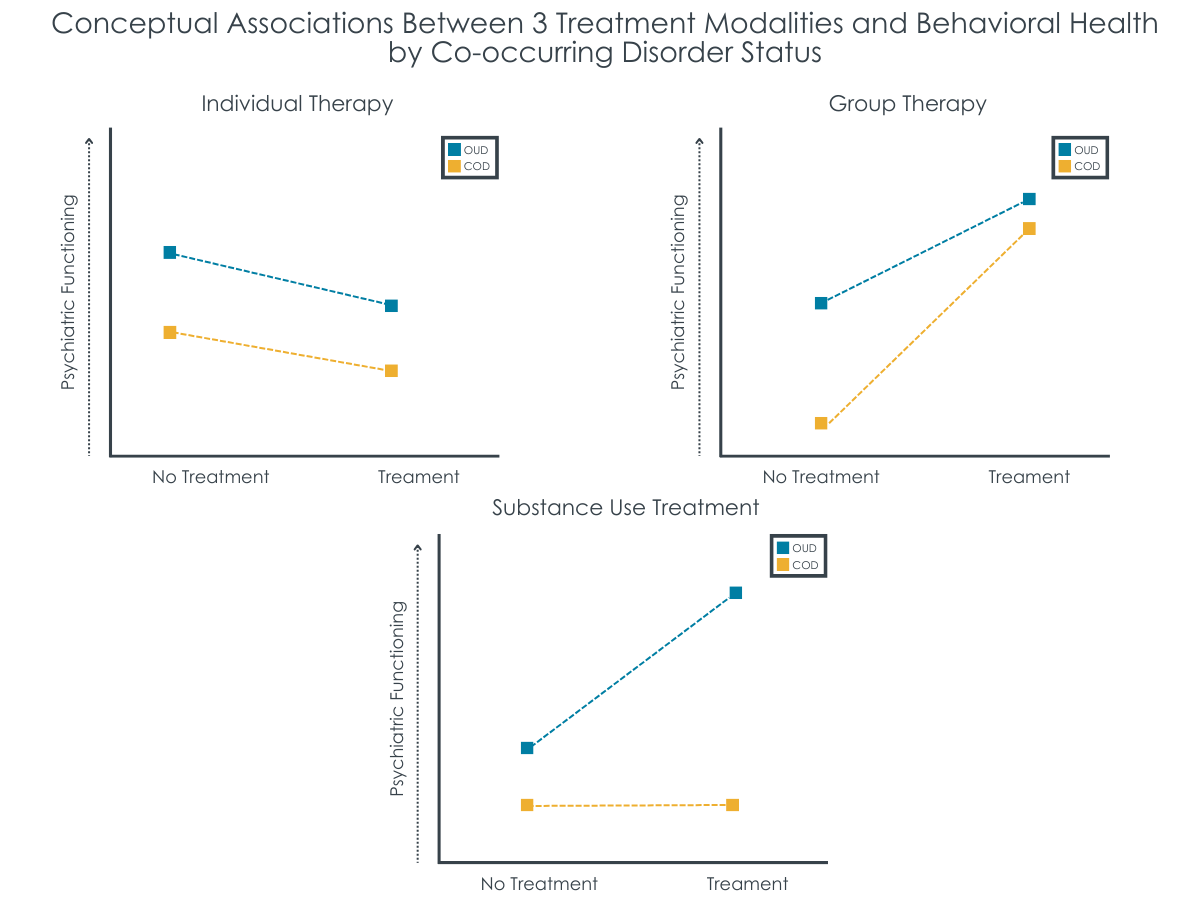
For substance use treatment, more contacts was associated with less severe behavioral health needs (better outcomes) only for those without a co-occurring disorder. Substance use treatment was unrelated to outcomes for those with a co-occurring disorder.
On the other hand, for participants with a co-occurring mental health disorder, more group therapy sessions for mental health was associated with better behavioral health needs scores upon completion of the program. While those with a co-occurring disorder began the program with more behavioral health needs, more group therapy sessions were associated with greater likelihood of “catching up” to the opioid use disorder only group with respect to behavioral health outcomes.
Figure. Co-occurring disorder group (orange bars) had worse psychiatric functioning overall than the opioid use disorder only group (blue bars). While individual therapy was associated with worse functioning contrary to expectations, group therapy was associated with gains for both groups but greater gains for the co-occurring disorder group. Substance use treatment was associated with gains for the opioid use disorder group but not the co-occurring disorder group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 2039 clients in the Indiana Recovery Works program found that almost half of the clients with an opioid use disorder had a co-occurring mental health disorder primarily mood, anxiety, and post-traumatic stress disorders. Compared to those with an opioid use disorder only, co-occurring disorders was associated with higher criminal legal system involvement during early follow-ups (up to 6 months). This is a finding that highlights the instability of early recovery and the potential need for additional system-level supports, resources, and assertive linkage for this more vulnerable population during this time frame. Yet, irrespective of whether or not someone had a co-occurring disorder, individuals who used services had better outcomes in terms of reduced criminal legal system involvement. In other words, treatment might help reduce recidivism for individuals with co-occurring disorders but their risk remains higher than for those with opioid use disorders only.
These results also suggest that while any type of treatment service may contribute to a reduced likelihood of criminal charges and that there is variability in its impact on psychiatric functioning, the exact degree of impact may vary depending on the type of service.
Group therapy for mental health consistently demonstrated the strongest association with better outcomes, individual therapy was effective at only specific time points, and substance use outpatient treatment did not show a significant association with criminal charges. While group therapy may have been especially helpful remedying the greater behavioral health challenges for those with co-occurring disorders, the study did not outline specific aspects of these three treatments and to what degree they included evidence-based elements of best practice for opioid use and mental health disorders. It is difficult to draw conclusions, therefore, about what group therapy may have offered that substance use treatment and individual therapy did not, accounting for the greater observed group therapy effects for the co-occurring disorders participants.
Overall, these findings highlight the complex and nuanced relationships between treatment utilization, treatment modality, and outcomes for individuals with co-occurring opioid use and mental health disorders. It highlights the importance of system-level procedures to identify and link individuals with tailored services to address their needs and the need for future research to examine the impact of specific types and amounts of treatment services provided to individuals with co-occurring opioid use and mental health disorders.
The study is based on a specific sample generated through engagement in a statewide program with stringent inclusion criteria. As a result, the findings may not generalize to other states or geographic areas.
Analyses examining functioning only included the 516 participants who completed the 12-month follow-up. While the study controlled for factors associated with completion vs. non-completion (e.g., higher functioning at baseline), findings may not generalize to all individuals with opioid use disorder.
Billing codes were used to identify the type of treatment a client received, but there is a lack of data on more specific aspects of those treatments and to what degree it included evidence-based elements of best practice for opioid use and mental health disorders. As a result, aside from the broad type of treatment and dose, little information can be gleaned from the treatment category analysis.
Mental health diagnoses represent a broad category of mental health issues and these each have specific symptoms that can affect one’s life, wellbeing, and recovery in different ways. The analysis does not account for different types of mental health diagnoses and the factors associated with outcomes.
BOTTOM LINE
In summary, this study of Recovery Works clients in Indiana highlights the challenges in addressing the complex interplay between co-occurring opioid use and mental health disorders. The findings highlight the importance of a nuanced and tailored approach to treatment, and to studying that treatment, with consideration given to both the type and dose of services provided.
For individuals and families seeking recovery: Community re-entry after reincarceration has many challenges, especially for those experiencing both opioid use and mental health challenges. Without addressing these needs, there is a high likelihood of re-involvement with the criminal legal system and having to start the cycle over. Seeking out treatment – or helping a loved one connect with treatment – especially during this critical period may help improve recovery and wellbeing outcomes and reduce involvement with the criminal legal system.
For treatment professionals and treatment systems: Community re-entry after reincarceration has many challenges, especially for those experiencing both opioid use and mental health disorders. Without addressing these needs, there is a high likelihood of the individual’s return to the criminal legal system, starting the cycle over. There is a significant need for professionals in carceral, health, and community systems to work together to create transition plans that assertively link clients to supports.
For scientists: This study highlights the complexity of examining recovery trajectories and addressing the needs of individuals with co-occurring opioid use and mental health disorders. Further research could examine more specifically the types and duration of treatment for different mental health diagnoses as well as if the findings here replicate to other contexts.
For policy makers: Community re-entry after reincarceration has many challenges, especially for individuals experiencing both opioid use and mental health disorders. Without addressing these needs, there is a high likelihood of the individual’s return to the criminal legal system, starting the cycle over. There is a significant need to develop infrastructure through funding, policies, and programs that support interagency work, including addressing these issues while in the criminal legal system, to reduce the burden on the system and ultimately improve lives.
It is common for individuals with opioid use disorders in the criminal-legal system also to experience mental health disorders. There is a lack of evidence-based treatment for individuals with opioid use disorders, as well as for co-occurring opioid use and mental health disorders, within jails and prisons. This leaves a major service gap at a critical point in time when individuals may be most likely to engage in services due to the structure of the criminal legal system.
When individuals with these co-occurring disorders transition back to their communities, there is increased risk as they attempt to resume their lives back in the very conditions that led to their incarceration. Engaging in treatment or recovery support is also difficult during this period as individuals released from prison or jail are faced with many barriers to access, including lack of adequate health insurance and active linkages to these services. Even navigating health insurance and referrals can be stressful and burdensome at a time when individuals are trying to reestablish themselves in the community and to identify a source of stable income.
This study sought to improve understanding of how a co-occurring mental health disorder impacts individuals with opioid use disorder and criminal system involvement, and whether community-based treatment may help offset any additional risk. They did this by examining the following four areas: (1) the prevalence of co-occurring opioid use and mental health disorders, (2) the effects of co-occurring mental health disorders on crime recidivism outcomes, (3) the effects of co-occurring mental health disorders on psychiatric recovery outcomes, and (4) whether co-occurring mental health changes how individuals engage in community-based treatment and outcomes.
HOW WAS THIS STUDY CONDUCTED?
This was secondary data analysis of individuals with opioid use disorder enrolled in the Recovery Works program between October 2015 and March 2018. Recovery Works is a voucher-based system to cover behavioral health services. It is only available to adults in Indiana who have an open criminal-legal case with a felony level charge (or prior felony conviction), who have an income lower than 200% of the federal income poverty level, and who are not covered by other forms of health insurance. The researchers used client data from only those individuals who had a baseline assessment and a subsequent episode of care.
The researchers included the following individual demographic characteristics in the analysis: any lifetime history of prior substance use treatment, felony charge one year prior to starting an episode of care, age at time of Recovery Works enrollment, sex, race (White, non-White), completed episode of care, and length of time in treatment. They used client records provided by Recovery Works to the Data Assessment Registry Mental Health and Addiction system to determine whether clients had a co-occurring mental health disorder with their opioid use disorder. The study did not provide information regarding how Recovery Works conducted assessments to determine substance use and mental health diagnoses used in their analyses.
The number of treatment contacts including substance use outpatient (e.g., intensive outpatient treatment for substance use disorder, medications for opioid use disorder, etc.), group therapy for mental health, and individual therapy (“person-centered and interactive psychiatric interviews) at 3-month, 6-month, and 12-months were collected from Recovery Works billing code data.
For outcome variables, the authors used results from the Recovery Works Adult Needs and Strengths Assessment at baseline and completion of treatment including life functioning (for example, employment, social functioning, residential stability), strengths (for example, social connectedness, education, and family strengths), and behavioral health needs (for example, depression, interpersonal problems, and substance use). These domains were analyzed as scale scores where higher scores indicated worse outcomes. That is, higher scores on the life functioning and behavioral health scales indicated a dangerous or disabling need and higher scores on the strengths scale indicated fewer strengths. Recidivism, or return to crime, was defined as any charge at 3-month, 6-month, and 12-months following the start of an episode of care. Recidivism was collected from court records.
The sample in this study was made up of 2039 clients in the Recovery Works program. The majority were white (90%) and male (59%) and were on average 32 years old (SD = 8). They had an average of 6.9 months (SD = 3.8) in the Recovery Works program and approximately 50% of clients fully completed their episode of care. Nearly half (47%) of clients had a co-occurring mental health disorder: the most common diagnoses were depressive disorders (33%), anxiety disorders (24%), and PTSD (21%).
WHAT DID THIS STUDY FIND?
Co-occurring mental health disorder was associated with greater treatment engagement but not crime recidivism.
At all follow-ups, individuals with a co-occurring disorder had higher service utilization than individuals with only an opioid use disorder and no mental health disorder. These individuals attended more substance use outpatient, group psychotherapy, and individual psychotherapy services. Although rates of service use were still very low, more clients with a co-occurring disorder used both substance use outpatient and psychotherapy services at 12-months (13%) compared to clients without a co-occurring disorder (6%). Clients with a co-occurring disorder were also more likely to complete their episode of care. There were no differences between clients with and without a co-occurring disorder for any criminal charge at all follow-ups. Also of note, clients with a co-occurring disorder were more likely to be female compared to clients without a co-occurring disorder.
Using treatment services decreased the likelihood of a criminal charge.
Use of any type of treatment services decreased the likelihood of a criminal charge, but group therapy had the greatest association as it reduced this likelihood at every follow-up. Individual therapy only reduced the likelihood of a criminal charge at 6- and 12-months, while substance use outpatient treatment was not associated with the likelihood of a criminal charge. When examining treatment usage by the presence of a co-occurring disorder, participants with and without a mental health disorder generally had similar, positive effects of treatment on reduced likelihood of another criminal charge over the 1-year follow-up.
Figure. While having a co-occurring disorder was associated with higher likelihood of a criminal charge, both groups experienced associated benefit from treatment.
Co-occurring mental health disorder associated with more behavioral health needs; only group therapy linked to better functioning.
In the group of 516 participants who completed a 12-month follow-up assessment, controlling for functioning when they entered the 12-month program, at completion those with a mental health disorder had more pronounced behavioral health needs. Although individual therapy services predicted worse life functioning at completion of care, the use of substance use outpatient services predicted better life functioning and the use of group therapy predicted better life functioning, behavioral health, and strengths.
Group therapy for mental health, not substance use or individual psychotherapy, associated with more gains for co-occurring disorder group.
For substance use treatment, more contacts was associated with less severe behavioral health needs (better outcomes) only for those without a co-occurring disorder. Substance use treatment was unrelated to outcomes for those with a co-occurring disorder.
On the other hand, for participants with a co-occurring mental health disorder, more group therapy sessions for mental health was associated with better behavioral health needs scores upon completion of the program. While those with a co-occurring disorder began the program with more behavioral health needs, more group therapy sessions were associated with greater likelihood of “catching up” to the opioid use disorder only group with respect to behavioral health outcomes.
Figure. Co-occurring disorder group (orange bars) had worse psychiatric functioning overall than the opioid use disorder only group (blue bars). While individual therapy was associated with worse functioning contrary to expectations, group therapy was associated with gains for both groups but greater gains for the co-occurring disorder group. Substance use treatment was associated with gains for the opioid use disorder group but not the co-occurring disorder group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 2039 clients in the Indiana Recovery Works program found that almost half of the clients with an opioid use disorder had a co-occurring mental health disorder primarily mood, anxiety, and post-traumatic stress disorders. Compared to those with an opioid use disorder only, co-occurring disorders was associated with higher criminal legal system involvement during early follow-ups (up to 6 months). This is a finding that highlights the instability of early recovery and the potential need for additional system-level supports, resources, and assertive linkage for this more vulnerable population during this time frame. Yet, irrespective of whether or not someone had a co-occurring disorder, individuals who used services had better outcomes in terms of reduced criminal legal system involvement. In other words, treatment might help reduce recidivism for individuals with co-occurring disorders but their risk remains higher than for those with opioid use disorders only.
These results also suggest that while any type of treatment service may contribute to a reduced likelihood of criminal charges and that there is variability in its impact on psychiatric functioning, the exact degree of impact may vary depending on the type of service.
Group therapy for mental health consistently demonstrated the strongest association with better outcomes, individual therapy was effective at only specific time points, and substance use outpatient treatment did not show a significant association with criminal charges. While group therapy may have been especially helpful remedying the greater behavioral health challenges for those with co-occurring disorders, the study did not outline specific aspects of these three treatments and to what degree they included evidence-based elements of best practice for opioid use and mental health disorders. It is difficult to draw conclusions, therefore, about what group therapy may have offered that substance use treatment and individual therapy did not, accounting for the greater observed group therapy effects for the co-occurring disorders participants.
Overall, these findings highlight the complex and nuanced relationships between treatment utilization, treatment modality, and outcomes for individuals with co-occurring opioid use and mental health disorders. It highlights the importance of system-level procedures to identify and link individuals with tailored services to address their needs and the need for future research to examine the impact of specific types and amounts of treatment services provided to individuals with co-occurring opioid use and mental health disorders.
The study is based on a specific sample generated through engagement in a statewide program with stringent inclusion criteria. As a result, the findings may not generalize to other states or geographic areas.
Analyses examining functioning only included the 516 participants who completed the 12-month follow-up. While the study controlled for factors associated with completion vs. non-completion (e.g., higher functioning at baseline), findings may not generalize to all individuals with opioid use disorder.
Billing codes were used to identify the type of treatment a client received, but there is a lack of data on more specific aspects of those treatments and to what degree it included evidence-based elements of best practice for opioid use and mental health disorders. As a result, aside from the broad type of treatment and dose, little information can be gleaned from the treatment category analysis.
Mental health diagnoses represent a broad category of mental health issues and these each have specific symptoms that can affect one’s life, wellbeing, and recovery in different ways. The analysis does not account for different types of mental health diagnoses and the factors associated with outcomes.
BOTTOM LINE
In summary, this study of Recovery Works clients in Indiana highlights the challenges in addressing the complex interplay between co-occurring opioid use and mental health disorders. The findings highlight the importance of a nuanced and tailored approach to treatment, and to studying that treatment, with consideration given to both the type and dose of services provided.
For individuals and families seeking recovery: Community re-entry after reincarceration has many challenges, especially for those experiencing both opioid use and mental health challenges. Without addressing these needs, there is a high likelihood of re-involvement with the criminal legal system and having to start the cycle over. Seeking out treatment – or helping a loved one connect with treatment – especially during this critical period may help improve recovery and wellbeing outcomes and reduce involvement with the criminal legal system.
For treatment professionals and treatment systems: Community re-entry after reincarceration has many challenges, especially for those experiencing both opioid use and mental health disorders. Without addressing these needs, there is a high likelihood of the individual’s return to the criminal legal system, starting the cycle over. There is a significant need for professionals in carceral, health, and community systems to work together to create transition plans that assertively link clients to supports.
For scientists: This study highlights the complexity of examining recovery trajectories and addressing the needs of individuals with co-occurring opioid use and mental health disorders. Further research could examine more specifically the types and duration of treatment for different mental health diagnoses as well as if the findings here replicate to other contexts.
For policy makers: Community re-entry after reincarceration has many challenges, especially for individuals experiencing both opioid use and mental health disorders. Without addressing these needs, there is a high likelihood of the individual’s return to the criminal legal system, starting the cycle over. There is a significant need to develop infrastructure through funding, policies, and programs that support interagency work, including addressing these issues while in the criminal legal system, to reduce the burden on the system and ultimately improve lives.
It is common for individuals with opioid use disorders in the criminal-legal system also to experience mental health disorders. There is a lack of evidence-based treatment for individuals with opioid use disorders, as well as for co-occurring opioid use and mental health disorders, within jails and prisons. This leaves a major service gap at a critical point in time when individuals may be most likely to engage in services due to the structure of the criminal legal system.
When individuals with these co-occurring disorders transition back to their communities, there is increased risk as they attempt to resume their lives back in the very conditions that led to their incarceration. Engaging in treatment or recovery support is also difficult during this period as individuals released from prison or jail are faced with many barriers to access, including lack of adequate health insurance and active linkages to these services. Even navigating health insurance and referrals can be stressful and burdensome at a time when individuals are trying to reestablish themselves in the community and to identify a source of stable income.
This study sought to improve understanding of how a co-occurring mental health disorder impacts individuals with opioid use disorder and criminal system involvement, and whether community-based treatment may help offset any additional risk. They did this by examining the following four areas: (1) the prevalence of co-occurring opioid use and mental health disorders, (2) the effects of co-occurring mental health disorders on crime recidivism outcomes, (3) the effects of co-occurring mental health disorders on psychiatric recovery outcomes, and (4) whether co-occurring mental health changes how individuals engage in community-based treatment and outcomes.
HOW WAS THIS STUDY CONDUCTED?
This was secondary data analysis of individuals with opioid use disorder enrolled in the Recovery Works program between October 2015 and March 2018. Recovery Works is a voucher-based system to cover behavioral health services. It is only available to adults in Indiana who have an open criminal-legal case with a felony level charge (or prior felony conviction), who have an income lower than 200% of the federal income poverty level, and who are not covered by other forms of health insurance. The researchers used client data from only those individuals who had a baseline assessment and a subsequent episode of care.
The researchers included the following individual demographic characteristics in the analysis: any lifetime history of prior substance use treatment, felony charge one year prior to starting an episode of care, age at time of Recovery Works enrollment, sex, race (White, non-White), completed episode of care, and length of time in treatment. They used client records provided by Recovery Works to the Data Assessment Registry Mental Health and Addiction system to determine whether clients had a co-occurring mental health disorder with their opioid use disorder. The study did not provide information regarding how Recovery Works conducted assessments to determine substance use and mental health diagnoses used in their analyses.
The number of treatment contacts including substance use outpatient (e.g., intensive outpatient treatment for substance use disorder, medications for opioid use disorder, etc.), group therapy for mental health, and individual therapy (“person-centered and interactive psychiatric interviews) at 3-month, 6-month, and 12-months were collected from Recovery Works billing code data.
For outcome variables, the authors used results from the Recovery Works Adult Needs and Strengths Assessment at baseline and completion of treatment including life functioning (for example, employment, social functioning, residential stability), strengths (for example, social connectedness, education, and family strengths), and behavioral health needs (for example, depression, interpersonal problems, and substance use). These domains were analyzed as scale scores where higher scores indicated worse outcomes. That is, higher scores on the life functioning and behavioral health scales indicated a dangerous or disabling need and higher scores on the strengths scale indicated fewer strengths. Recidivism, or return to crime, was defined as any charge at 3-month, 6-month, and 12-months following the start of an episode of care. Recidivism was collected from court records.
The sample in this study was made up of 2039 clients in the Recovery Works program. The majority were white (90%) and male (59%) and were on average 32 years old (SD = 8). They had an average of 6.9 months (SD = 3.8) in the Recovery Works program and approximately 50% of clients fully completed their episode of care. Nearly half (47%) of clients had a co-occurring mental health disorder: the most common diagnoses were depressive disorders (33%), anxiety disorders (24%), and PTSD (21%).
WHAT DID THIS STUDY FIND?
Co-occurring mental health disorder was associated with greater treatment engagement but not crime recidivism.
At all follow-ups, individuals with a co-occurring disorder had higher service utilization than individuals with only an opioid use disorder and no mental health disorder. These individuals attended more substance use outpatient, group psychotherapy, and individual psychotherapy services. Although rates of service use were still very low, more clients with a co-occurring disorder used both substance use outpatient and psychotherapy services at 12-months (13%) compared to clients without a co-occurring disorder (6%). Clients with a co-occurring disorder were also more likely to complete their episode of care. There were no differences between clients with and without a co-occurring disorder for any criminal charge at all follow-ups. Also of note, clients with a co-occurring disorder were more likely to be female compared to clients without a co-occurring disorder.
Using treatment services decreased the likelihood of a criminal charge.
Use of any type of treatment services decreased the likelihood of a criminal charge, but group therapy had the greatest association as it reduced this likelihood at every follow-up. Individual therapy only reduced the likelihood of a criminal charge at 6- and 12-months, while substance use outpatient treatment was not associated with the likelihood of a criminal charge. When examining treatment usage by the presence of a co-occurring disorder, participants with and without a mental health disorder generally had similar, positive effects of treatment on reduced likelihood of another criminal charge over the 1-year follow-up.
Figure. While having a co-occurring disorder was associated with higher likelihood of a criminal charge, both groups experienced associated benefit from treatment.
Co-occurring mental health disorder associated with more behavioral health needs; only group therapy linked to better functioning.
In the group of 516 participants who completed a 12-month follow-up assessment, controlling for functioning when they entered the 12-month program, at completion those with a mental health disorder had more pronounced behavioral health needs. Although individual therapy services predicted worse life functioning at completion of care, the use of substance use outpatient services predicted better life functioning and the use of group therapy predicted better life functioning, behavioral health, and strengths.
Group therapy for mental health, not substance use or individual psychotherapy, associated with more gains for co-occurring disorder group.
For substance use treatment, more contacts was associated with less severe behavioral health needs (better outcomes) only for those without a co-occurring disorder. Substance use treatment was unrelated to outcomes for those with a co-occurring disorder.
On the other hand, for participants with a co-occurring mental health disorder, more group therapy sessions for mental health was associated with better behavioral health needs scores upon completion of the program. While those with a co-occurring disorder began the program with more behavioral health needs, more group therapy sessions were associated with greater likelihood of “catching up” to the opioid use disorder only group with respect to behavioral health outcomes.
Figure. Co-occurring disorder group (orange bars) had worse psychiatric functioning overall than the opioid use disorder only group (blue bars). While individual therapy was associated with worse functioning contrary to expectations, group therapy was associated with gains for both groups but greater gains for the co-occurring disorder group. Substance use treatment was associated with gains for the opioid use disorder group but not the co-occurring disorder group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 2039 clients in the Indiana Recovery Works program found that almost half of the clients with an opioid use disorder had a co-occurring mental health disorder primarily mood, anxiety, and post-traumatic stress disorders. Compared to those with an opioid use disorder only, co-occurring disorders was associated with higher criminal legal system involvement during early follow-ups (up to 6 months). This is a finding that highlights the instability of early recovery and the potential need for additional system-level supports, resources, and assertive linkage for this more vulnerable population during this time frame. Yet, irrespective of whether or not someone had a co-occurring disorder, individuals who used services had better outcomes in terms of reduced criminal legal system involvement. In other words, treatment might help reduce recidivism for individuals with co-occurring disorders but their risk remains higher than for those with opioid use disorders only.
These results also suggest that while any type of treatment service may contribute to a reduced likelihood of criminal charges and that there is variability in its impact on psychiatric functioning, the exact degree of impact may vary depending on the type of service.
Group therapy for mental health consistently demonstrated the strongest association with better outcomes, individual therapy was effective at only specific time points, and substance use outpatient treatment did not show a significant association with criminal charges. While group therapy may have been especially helpful remedying the greater behavioral health challenges for those with co-occurring disorders, the study did not outline specific aspects of these three treatments and to what degree they included evidence-based elements of best practice for opioid use and mental health disorders. It is difficult to draw conclusions, therefore, about what group therapy may have offered that substance use treatment and individual therapy did not, accounting for the greater observed group therapy effects for the co-occurring disorders participants.
Overall, these findings highlight the complex and nuanced relationships between treatment utilization, treatment modality, and outcomes for individuals with co-occurring opioid use and mental health disorders. It highlights the importance of system-level procedures to identify and link individuals with tailored services to address their needs and the need for future research to examine the impact of specific types and amounts of treatment services provided to individuals with co-occurring opioid use and mental health disorders.
The study is based on a specific sample generated through engagement in a statewide program with stringent inclusion criteria. As a result, the findings may not generalize to other states or geographic areas.
Analyses examining functioning only included the 516 participants who completed the 12-month follow-up. While the study controlled for factors associated with completion vs. non-completion (e.g., higher functioning at baseline), findings may not generalize to all individuals with opioid use disorder.
Billing codes were used to identify the type of treatment a client received, but there is a lack of data on more specific aspects of those treatments and to what degree it included evidence-based elements of best practice for opioid use and mental health disorders. As a result, aside from the broad type of treatment and dose, little information can be gleaned from the treatment category analysis.
Mental health diagnoses represent a broad category of mental health issues and these each have specific symptoms that can affect one’s life, wellbeing, and recovery in different ways. The analysis does not account for different types of mental health diagnoses and the factors associated with outcomes.
BOTTOM LINE
In summary, this study of Recovery Works clients in Indiana highlights the challenges in addressing the complex interplay between co-occurring opioid use and mental health disorders. The findings highlight the importance of a nuanced and tailored approach to treatment, and to studying that treatment, with consideration given to both the type and dose of services provided.
For individuals and families seeking recovery: Community re-entry after reincarceration has many challenges, especially for those experiencing both opioid use and mental health challenges. Without addressing these needs, there is a high likelihood of re-involvement with the criminal legal system and having to start the cycle over. Seeking out treatment – or helping a loved one connect with treatment – especially during this critical period may help improve recovery and wellbeing outcomes and reduce involvement with the criminal legal system.
For treatment professionals and treatment systems: Community re-entry after reincarceration has many challenges, especially for those experiencing both opioid use and mental health disorders. Without addressing these needs, there is a high likelihood of the individual’s return to the criminal legal system, starting the cycle over. There is a significant need for professionals in carceral, health, and community systems to work together to create transition plans that assertively link clients to supports.
For scientists: This study highlights the complexity of examining recovery trajectories and addressing the needs of individuals with co-occurring opioid use and mental health disorders. Further research could examine more specifically the types and duration of treatment for different mental health diagnoses as well as if the findings here replicate to other contexts.
For policy makers: Community re-entry after reincarceration has many challenges, especially for individuals experiencing both opioid use and mental health disorders. Without addressing these needs, there is a high likelihood of the individual’s return to the criminal legal system, starting the cycle over. There is a significant need to develop infrastructure through funding, policies, and programs that support interagency work, including addressing these issues while in the criminal legal system, to reduce the burden on the system and ultimately improve lives.