Real-world effects of extended-release buprenorphine
Extended-release buprenorphine is a helpful treatment for many individuals with opioid use disorder. To this point, though, this injection formulation has been studied primarily in clinical trials conducted in controlled settings. To enhance understanding of its benefits in real-world settings, this study examined treatment retention and outcomes for extended-release injectable buprenorphine delivered in community-based outpatient treatment settings.
Extended-release buprenorphine is an effective and convenient treatment option for individuals with opioid use disorder. These injections, delivered monthly or weekly depending on the type of formulation, offer patients more flexibility than daily sublingual buprenorphine doses, since they don’t require daily dosing or frequent clinic and pharmacy visits.
Previous studies have shown that extended-release buprenorphine injections are just as effective as sublingual buprenorphine at reducing illicit opioid use and retaining patients in treatment. Research has also suggested that patients might experience greater treatment satisfaction with extended-release buprenorphine than sublingual buprenorphine. However, the majority of studies examining the benefits of extended-release buprenorphine are clinical trials that administer injections in controlled study environments, which limits appraisal of this medication’s benefits in real-world settings. To evaluate the effects of extended-release buprenorphine treatment in day-to-day practice, this study examined treatment retention and outcomes among treatment-experienced patients receiving 48 weeks of extended-release buprenorphine in a variety of community-based healthcare settings.
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal single-arm, open-label trial of extended-release buprenorphine among patients receiving opioid use disorder treatment across a wide range of healthcare settings. One-hundred participants were recruited from seven specialist public substance use disorder treatment programs, primary care practices, and private practices in three states across Australia.
The researchers investigated treatment retention 24 and 48 weeks after patient’s first extended-release buprenorphine injection, as well as the influence of baseline clinical and demographic factors on retention. The researchers then examined the relationship between treatment duration and changes in past-month clinical characteristics, well-being, and treatment satisfaction.
Participants received monthly extended-release buprenorphine injections from their community treatment providers and completed monthly study sessions for 48 weeks following the first injection. All participants received 300 mg of extended-release buprenorphine for their first and second injections, followed by flexible doses of 100 mg or 300 mg injections in subsequent months, as determined collaboratively by the patients and their doctors. The majority of patients transferred to 100 mg doses by the third injection.
Study sessions occurred prior to treatment initiation (baseline) and every month for 48 weeks following the first extended-release buprenorphine injection. Treatment retention was assessed as the percentage of patients who remained on active extended-release buprenorphine medication 24 weeks and 48 weeks after the first injection, according to clinical records. At baseline and follow-up study sessions, participants completed questionnaires on past-month substance use (Australian Treatment Outcome Profile, confirmed with drug screens), quality of life (Australian Quality of Life 4-Dimension), depression (Patient Health Questionnaire-9, with scores ≥ 10 indicating moderate/severe depression), pain (Pain, Enjoyment, General Activity scale), treatment satisfaction (Treatment Satisfaction Questionnaire for Medication), and other descriptive measures (e.g., past-month employment).
Participants were predominantly men (72%) in their early 40’s, with a primary heroin (55%) or prescription opioid (45%) problem, and a median of 6 years of opioid agonist (i.e., methadone or buprenorphine) treatment across their lifetime. All participants underwent at least 7 days of sublingual buprenorphine treatment prior to starting monthly extended-release buprenorphine injections. At the time of study recruitment, participants had a median duration of 2.2 years on their current opioid agonist treatment, with the majority receiving buprenorphine (94%). Seventeen percent of patients received supplementary doses of sublingual buprenorphine for craving during treatment weeks 4 through 12 of the study.
WHAT DID THIS STUDY FIND?
Most were retained in treatment out to 48 weeks.
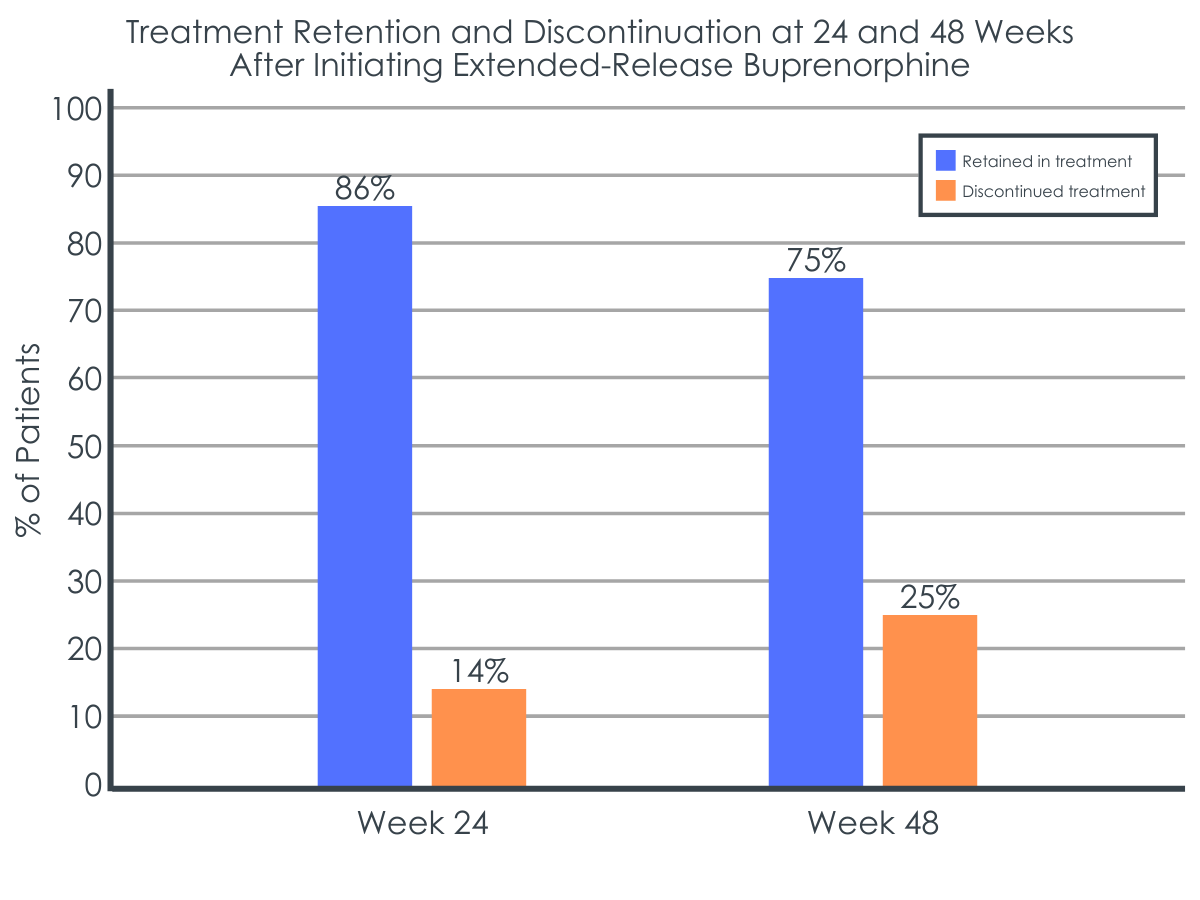
Of the 100 patients enrolled in the study, 86% remained in treatment at week 24 and 75% remained in treatment at week 48, including 73% who received all 12 monthly injections. Among the patients who discontinued treatment by week 48, the majority (64%) were lost to treatment follow-up (i.e., stopped going to their treatment provider at some point during the 48 weeks). The remaining 36% who discontinued did so because they entered prison or residential treatment (12%), transitioned to sublingual buprenorphine (8%), experienced medication side effects (4%), or discontinued for some other reason (12%).
Figure 2. Shows the percentage of patients who remained in treatment or discontinued treatment 24 and 48 weeks after their first extended-release buprenorphine injection.
Individuals with less severe drug use before treatment were more likely to remain in treatment.
Controlling for other relevant demographic and clinical factors, patients who did not engage in past-month injection drug use or heroin use at baseline were about 6 times more likely than patients who did engage in these activities to be retained in treatment after 48 weeks of extended-release buprenorphine.
Past-month clinical characteristics, well-being, and treatment satisfaction improved with treatment duration.
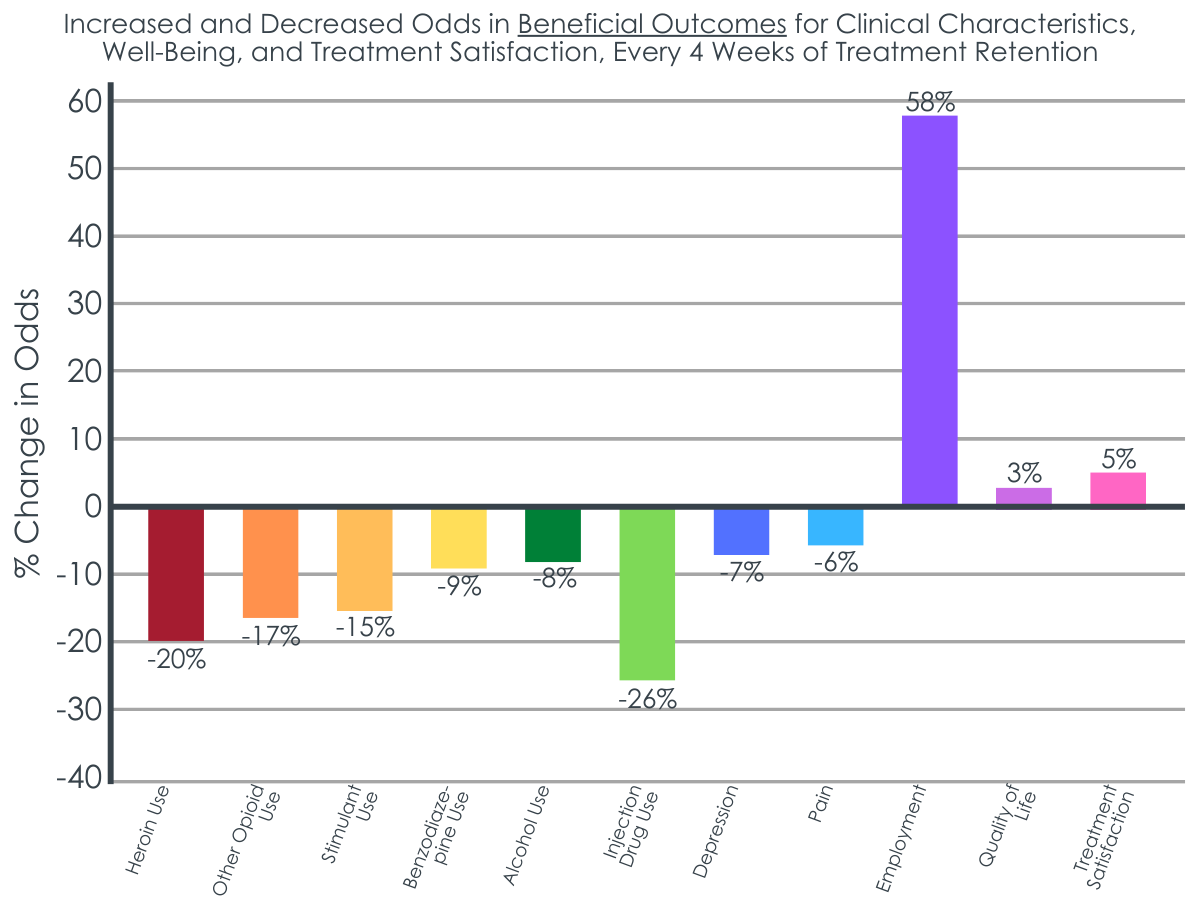
For every four weeks that a patient remained on extended-release buprenorphine, the likelihood of substance use decreased by 8% to 20% across various substances. In addition, the odds of past-month injection drug use, moderate-severe depression, and pain decreased for every four weeks on treatment, whereas the odds of employment, quality of life, and treatment satisfaction increased for every four weeks on treatment.
Figure 3. shows the percent increase and decrease in odds of substance use behaviors, well-being, and treatment satisfaction for every 4 months that a patient was retained in extended-release buprenorphine treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the potential benefits of opioid use disorder medication treatments when delivered in real-world settings and in the context of standard outpatient practices.
Retention in injectable extended-release buprenorphine treatment was relatively high over the course of 48 months. Though retention rates here have been observed in prior research, they are somewhat higher than the rates observed in a number of other clinical trials that have assessed retention at 24 and 48 weeks. Retention rates in this study were also higher than those reported in population-based data for sublingual buprenorphine in Australia, where this research was conducted (~46% retention after 12 months).
The high retention rates seen in this study may be due to the fact that the study’s patient population had extensive experience with opioid use disorder medication treatments, and most were already engaged in medication treatment at the time of study enrollment, with the majority receiving sublingual buprenorphine.
A similar investigation of patients transitioning from sublingual buprenorphine to extended-release buprenorphine treatment in real-world settings found that individuals who were retained on extended-release buprenorphine for a longer period of time had been on sublingual buprenorphine for longer durations prior to their first injection. This finding emphasizes that stable established patients, like the ones assessed in the current study, may be particularly good candidates for extended-release buprenorphine treatment. At least among patients with prior opioid agonist treatment experience, this study suggests that retention rates in community-based healthcare services may be similar to or better than those observed in controlled trials. Additional research will help identify whether real-world retention rates in treatment-naïve patients are similarly high.
Regarding predictors of retention, prior studies have also found that recent heroin use and injection drug use are associated with discontinuation of extended-release buprenorphine. These substance-use behaviors suggest clinical instability that may require more intensive follow-up care (e.g., more frequent check-ups) to ensure retention in treatment and attainment of its associated benefits. Additional research will help to identify other factors that put patients at risk of treatment dropout and ultimately help inform individualized treatment plans that support patients at various degrees of risk.
The researchers also found that remaining in treatment was associated with ongoing improvements in patient outcomes, including substance use, treatment satisfaction, and various measures of well-being, which is to be expected as someone progresses in their treatment with an evidence-based medication. Previous studies have shown similar benefits of extended-release buprenorphine when delivered under controlled study settings in medication trials, including reduced illicit opioid use and addiction severity, as well as improved quality of life, mental and physical health, employment status, and perceptions of treatment effectiveness over the course of one year. Importantly, the benefits observed in this study increased with every 4 additional weeks retained in treatment, emphasizing the importance of ongoing treatment engagement for positive treatment and recovery outcomes.
Investigating the treatment course and outcomes of extended-release buprenorphine in real-world settings is important because this medication offers a potentially more convenient treatment option for patients with opioid use disorder. Once-monthly injections, as opposed to daily sublingual buprenorphine dosing allows for fewer doctor visits and trips to the pharmacy, and may help to preventexperiences of stigma and reduce potentially harmful medication dosing rituals and habits. More convenient dosing schedules might also be particularly beneficial for individuals who are experiencing greater psychosocial challenges (e.g., homelessness).Additional studies of extended-release buprenorphine in community-based settings will improve our understanding of who in particular is likely to benefit (or not) from this type of medication’s benefits and lead to more precise treatment recommendations.
This study was conducted in Australia among patients with a long history of prior medication treatment (i.e., buprenorphine and methadone). Findings may not apply to other countries with different community-based treatment models or to individuals who are seeking treatment for the first time.
This study did not include a comparison group, so it is unclear if extended-release buprenorphine treatment outcomes are better or worse than those seen with other opioid use disorder medication treatments delivered in community-based healthcare settings.
BOTTOM LINE
Retention in extended-release buprenorphine treatment among this treatment-engaged population with opioid use disorder was 86% at week 24 and 75% at week 48. Individuals with past-month heroin use and past-month injection drug use at baseline were more likely to discontinue treatment. Remaining in treatment was associated with ongoing improvements in measures of substance use, well-being, and treatment satisfaction. These included a reduced likelihood of illicit substance use, injection drug use, depression, and pain, as well as increased odds of employment, quality of life, and treatment satisfaction, for every four weeks that a patient remained on extended-release buprenorphine. This study contributes to limited research evaluating patient retention and outcomes for extended-release buprenorphine in real-world treatment settings. Enhancing our understanding of the effects of various medication treatments for opioid use disorder will ultimately help guide individualized treatment approaches and best practices for enhancing patients’ treatment and recovery outcomes in the context of medication treatment.
For individuals and families seeking recovery: Buprenorphine is a helpful treatment for opioid use disorder that saves lives. It comes in various formulations, including sublingual and extended-release injectable versions. Individuals who have a recent history of treatment with sublingual buprenorphine and may be looking to start or transition to a more convenient formulation might consider trying once-monthly injections of extended-release injectable buprenorphine. Interested individuals should speak with a knowledgeable prescriber about the risks and benefits of this medication.
For treatment professionals and treatment systems: Treatment-experienced patients with stable histories of sublingual buprenorphine treatment may be good candidates for extended-release formulations. However, patient preference and risk factors like recent injection drug use or illicit drug use should be evaluated when considering initiation of extended-release buprenorphine treatment, given their relationship to treatment engagement and retention. Discussions and check-ins around convenience, side effects, insurance coverage, recovery goals, and ongoing changes in symptoms and well-being are encouraged to support patients’ treatment retention and success. Treatment providers also should be somewhat cautious with decisions to initiate and transition patients to extended-release injectable buprenorphine, given the variability in patient retention seen across other studies.
For scientists:It is essential to conduct additional real-world longitudinal investigations of medication treatments for opioid use disorder. Evaluations of the treatment’s course (e.g., retention, duration, regimen) and patient’s outcomes (substance use, recovery capital, well-being, interpersonal relationships), as well as clinical and demographic moderators, are needed to enhance clinical practice precision and ensure patients are receiving the treatments that will provide them the greatest gains in recovery outcomes. Investigations of extended-release buprenorphine in treatment-naïve patients and in various countries with different treatment models are also needed.
For policy makers: Compared to daily sublingual buprenorphine dosing, once monthly extended-release buprenorphine injections may be a more convenient treatment option for at least some patients with opioid use disorder, which might help to encourage treatment retention and subsequently promote treatment-related improvements in patients. However, there are few studies on treatment retention and patient outcomes for extended-release buprenorphine, limiting our understanding of the benefits of these medications and for whom they might work best. Additional research funding will help identify the full potential of this medication in real-world settings to guide clinical recommendations and individualized treatments to enhance patient outcomes and promote stable recovery among treatment-experienced and -naïve patients.
Extended-release buprenorphine is an effective and convenient treatment option for individuals with opioid use disorder. These injections, delivered monthly or weekly depending on the type of formulation, offer patients more flexibility than daily sublingual buprenorphine doses, since they don’t require daily dosing or frequent clinic and pharmacy visits.
Previous studies have shown that extended-release buprenorphine injections are just as effective as sublingual buprenorphine at reducing illicit opioid use and retaining patients in treatment. Research has also suggested that patients might experience greater treatment satisfaction with extended-release buprenorphine than sublingual buprenorphine. However, the majority of studies examining the benefits of extended-release buprenorphine are clinical trials that administer injections in controlled study environments, which limits appraisal of this medication’s benefits in real-world settings. To evaluate the effects of extended-release buprenorphine treatment in day-to-day practice, this study examined treatment retention and outcomes among treatment-experienced patients receiving 48 weeks of extended-release buprenorphine in a variety of community-based healthcare settings.
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal single-arm, open-label trial of extended-release buprenorphine among patients receiving opioid use disorder treatment across a wide range of healthcare settings. One-hundred participants were recruited from seven specialist public substance use disorder treatment programs, primary care practices, and private practices in three states across Australia.
The researchers investigated treatment retention 24 and 48 weeks after patient’s first extended-release buprenorphine injection, as well as the influence of baseline clinical and demographic factors on retention. The researchers then examined the relationship between treatment duration and changes in past-month clinical characteristics, well-being, and treatment satisfaction.
Participants received monthly extended-release buprenorphine injections from their community treatment providers and completed monthly study sessions for 48 weeks following the first injection. All participants received 300 mg of extended-release buprenorphine for their first and second injections, followed by flexible doses of 100 mg or 300 mg injections in subsequent months, as determined collaboratively by the patients and their doctors. The majority of patients transferred to 100 mg doses by the third injection.
Study sessions occurred prior to treatment initiation (baseline) and every month for 48 weeks following the first extended-release buprenorphine injection. Treatment retention was assessed as the percentage of patients who remained on active extended-release buprenorphine medication 24 weeks and 48 weeks after the first injection, according to clinical records. At baseline and follow-up study sessions, participants completed questionnaires on past-month substance use (Australian Treatment Outcome Profile, confirmed with drug screens), quality of life (Australian Quality of Life 4-Dimension), depression (Patient Health Questionnaire-9, with scores ≥ 10 indicating moderate/severe depression), pain (Pain, Enjoyment, General Activity scale), treatment satisfaction (Treatment Satisfaction Questionnaire for Medication), and other descriptive measures (e.g., past-month employment).
Participants were predominantly men (72%) in their early 40’s, with a primary heroin (55%) or prescription opioid (45%) problem, and a median of 6 years of opioid agonist (i.e., methadone or buprenorphine) treatment across their lifetime. All participants underwent at least 7 days of sublingual buprenorphine treatment prior to starting monthly extended-release buprenorphine injections. At the time of study recruitment, participants had a median duration of 2.2 years on their current opioid agonist treatment, with the majority receiving buprenorphine (94%). Seventeen percent of patients received supplementary doses of sublingual buprenorphine for craving during treatment weeks 4 through 12 of the study.
WHAT DID THIS STUDY FIND?
Most were retained in treatment out to 48 weeks.
Of the 100 patients enrolled in the study, 86% remained in treatment at week 24 and 75% remained in treatment at week 48, including 73% who received all 12 monthly injections. Among the patients who discontinued treatment by week 48, the majority (64%) were lost to treatment follow-up (i.e., stopped going to their treatment provider at some point during the 48 weeks). The remaining 36% who discontinued did so because they entered prison or residential treatment (12%), transitioned to sublingual buprenorphine (8%), experienced medication side effects (4%), or discontinued for some other reason (12%).
Figure 2. Shows the percentage of patients who remained in treatment or discontinued treatment 24 and 48 weeks after their first extended-release buprenorphine injection.
Individuals with less severe drug use before treatment were more likely to remain in treatment.
Controlling for other relevant demographic and clinical factors, patients who did not engage in past-month injection drug use or heroin use at baseline were about 6 times more likely than patients who did engage in these activities to be retained in treatment after 48 weeks of extended-release buprenorphine.
Past-month clinical characteristics, well-being, and treatment satisfaction improved with treatment duration.
For every four weeks that a patient remained on extended-release buprenorphine, the likelihood of substance use decreased by 8% to 20% across various substances. In addition, the odds of past-month injection drug use, moderate-severe depression, and pain decreased for every four weeks on treatment, whereas the odds of employment, quality of life, and treatment satisfaction increased for every four weeks on treatment.
Figure 3. shows the percent increase and decrease in odds of substance use behaviors, well-being, and treatment satisfaction for every 4 months that a patient was retained in extended-release buprenorphine treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the potential benefits of opioid use disorder medication treatments when delivered in real-world settings and in the context of standard outpatient practices.
Retention in injectable extended-release buprenorphine treatment was relatively high over the course of 48 months. Though retention rates here have been observed in prior research, they are somewhat higher than the rates observed in a number of other clinical trials that have assessed retention at 24 and 48 weeks. Retention rates in this study were also higher than those reported in population-based data for sublingual buprenorphine in Australia, where this research was conducted (~46% retention after 12 months).
The high retention rates seen in this study may be due to the fact that the study’s patient population had extensive experience with opioid use disorder medication treatments, and most were already engaged in medication treatment at the time of study enrollment, with the majority receiving sublingual buprenorphine.
A similar investigation of patients transitioning from sublingual buprenorphine to extended-release buprenorphine treatment in real-world settings found that individuals who were retained on extended-release buprenorphine for a longer period of time had been on sublingual buprenorphine for longer durations prior to their first injection. This finding emphasizes that stable established patients, like the ones assessed in the current study, may be particularly good candidates for extended-release buprenorphine treatment. At least among patients with prior opioid agonist treatment experience, this study suggests that retention rates in community-based healthcare services may be similar to or better than those observed in controlled trials. Additional research will help identify whether real-world retention rates in treatment-naïve patients are similarly high.
Regarding predictors of retention, prior studies have also found that recent heroin use and injection drug use are associated with discontinuation of extended-release buprenorphine. These substance-use behaviors suggest clinical instability that may require more intensive follow-up care (e.g., more frequent check-ups) to ensure retention in treatment and attainment of its associated benefits. Additional research will help to identify other factors that put patients at risk of treatment dropout and ultimately help inform individualized treatment plans that support patients at various degrees of risk.
The researchers also found that remaining in treatment was associated with ongoing improvements in patient outcomes, including substance use, treatment satisfaction, and various measures of well-being, which is to be expected as someone progresses in their treatment with an evidence-based medication. Previous studies have shown similar benefits of extended-release buprenorphine when delivered under controlled study settings in medication trials, including reduced illicit opioid use and addiction severity, as well as improved quality of life, mental and physical health, employment status, and perceptions of treatment effectiveness over the course of one year. Importantly, the benefits observed in this study increased with every 4 additional weeks retained in treatment, emphasizing the importance of ongoing treatment engagement for positive treatment and recovery outcomes.
Investigating the treatment course and outcomes of extended-release buprenorphine in real-world settings is important because this medication offers a potentially more convenient treatment option for patients with opioid use disorder. Once-monthly injections, as opposed to daily sublingual buprenorphine dosing allows for fewer doctor visits and trips to the pharmacy, and may help to preventexperiences of stigma and reduce potentially harmful medication dosing rituals and habits. More convenient dosing schedules might also be particularly beneficial for individuals who are experiencing greater psychosocial challenges (e.g., homelessness).Additional studies of extended-release buprenorphine in community-based settings will improve our understanding of who in particular is likely to benefit (or not) from this type of medication’s benefits and lead to more precise treatment recommendations.
This study was conducted in Australia among patients with a long history of prior medication treatment (i.e., buprenorphine and methadone). Findings may not apply to other countries with different community-based treatment models or to individuals who are seeking treatment for the first time.
This study did not include a comparison group, so it is unclear if extended-release buprenorphine treatment outcomes are better or worse than those seen with other opioid use disorder medication treatments delivered in community-based healthcare settings.
BOTTOM LINE
Retention in extended-release buprenorphine treatment among this treatment-engaged population with opioid use disorder was 86% at week 24 and 75% at week 48. Individuals with past-month heroin use and past-month injection drug use at baseline were more likely to discontinue treatment. Remaining in treatment was associated with ongoing improvements in measures of substance use, well-being, and treatment satisfaction. These included a reduced likelihood of illicit substance use, injection drug use, depression, and pain, as well as increased odds of employment, quality of life, and treatment satisfaction, for every four weeks that a patient remained on extended-release buprenorphine. This study contributes to limited research evaluating patient retention and outcomes for extended-release buprenorphine in real-world treatment settings. Enhancing our understanding of the effects of various medication treatments for opioid use disorder will ultimately help guide individualized treatment approaches and best practices for enhancing patients’ treatment and recovery outcomes in the context of medication treatment.
For individuals and families seeking recovery: Buprenorphine is a helpful treatment for opioid use disorder that saves lives. It comes in various formulations, including sublingual and extended-release injectable versions. Individuals who have a recent history of treatment with sublingual buprenorphine and may be looking to start or transition to a more convenient formulation might consider trying once-monthly injections of extended-release injectable buprenorphine. Interested individuals should speak with a knowledgeable prescriber about the risks and benefits of this medication.
For treatment professionals and treatment systems: Treatment-experienced patients with stable histories of sublingual buprenorphine treatment may be good candidates for extended-release formulations. However, patient preference and risk factors like recent injection drug use or illicit drug use should be evaluated when considering initiation of extended-release buprenorphine treatment, given their relationship to treatment engagement and retention. Discussions and check-ins around convenience, side effects, insurance coverage, recovery goals, and ongoing changes in symptoms and well-being are encouraged to support patients’ treatment retention and success. Treatment providers also should be somewhat cautious with decisions to initiate and transition patients to extended-release injectable buprenorphine, given the variability in patient retention seen across other studies.
For scientists:It is essential to conduct additional real-world longitudinal investigations of medication treatments for opioid use disorder. Evaluations of the treatment’s course (e.g., retention, duration, regimen) and patient’s outcomes (substance use, recovery capital, well-being, interpersonal relationships), as well as clinical and demographic moderators, are needed to enhance clinical practice precision and ensure patients are receiving the treatments that will provide them the greatest gains in recovery outcomes. Investigations of extended-release buprenorphine in treatment-naïve patients and in various countries with different treatment models are also needed.
For policy makers: Compared to daily sublingual buprenorphine dosing, once monthly extended-release buprenorphine injections may be a more convenient treatment option for at least some patients with opioid use disorder, which might help to encourage treatment retention and subsequently promote treatment-related improvements in patients. However, there are few studies on treatment retention and patient outcomes for extended-release buprenorphine, limiting our understanding of the benefits of these medications and for whom they might work best. Additional research funding will help identify the full potential of this medication in real-world settings to guide clinical recommendations and individualized treatments to enhance patient outcomes and promote stable recovery among treatment-experienced and -naïve patients.
Extended-release buprenorphine is an effective and convenient treatment option for individuals with opioid use disorder. These injections, delivered monthly or weekly depending on the type of formulation, offer patients more flexibility than daily sublingual buprenorphine doses, since they don’t require daily dosing or frequent clinic and pharmacy visits.
Previous studies have shown that extended-release buprenorphine injections are just as effective as sublingual buprenorphine at reducing illicit opioid use and retaining patients in treatment. Research has also suggested that patients might experience greater treatment satisfaction with extended-release buprenorphine than sublingual buprenorphine. However, the majority of studies examining the benefits of extended-release buprenorphine are clinical trials that administer injections in controlled study environments, which limits appraisal of this medication’s benefits in real-world settings. To evaluate the effects of extended-release buprenorphine treatment in day-to-day practice, this study examined treatment retention and outcomes among treatment-experienced patients receiving 48 weeks of extended-release buprenorphine in a variety of community-based healthcare settings.
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal single-arm, open-label trial of extended-release buprenorphine among patients receiving opioid use disorder treatment across a wide range of healthcare settings. One-hundred participants were recruited from seven specialist public substance use disorder treatment programs, primary care practices, and private practices in three states across Australia.
The researchers investigated treatment retention 24 and 48 weeks after patient’s first extended-release buprenorphine injection, as well as the influence of baseline clinical and demographic factors on retention. The researchers then examined the relationship between treatment duration and changes in past-month clinical characteristics, well-being, and treatment satisfaction.
Participants received monthly extended-release buprenorphine injections from their community treatment providers and completed monthly study sessions for 48 weeks following the first injection. All participants received 300 mg of extended-release buprenorphine for their first and second injections, followed by flexible doses of 100 mg or 300 mg injections in subsequent months, as determined collaboratively by the patients and their doctors. The majority of patients transferred to 100 mg doses by the third injection.
Study sessions occurred prior to treatment initiation (baseline) and every month for 48 weeks following the first extended-release buprenorphine injection. Treatment retention was assessed as the percentage of patients who remained on active extended-release buprenorphine medication 24 weeks and 48 weeks after the first injection, according to clinical records. At baseline and follow-up study sessions, participants completed questionnaires on past-month substance use (Australian Treatment Outcome Profile, confirmed with drug screens), quality of life (Australian Quality of Life 4-Dimension), depression (Patient Health Questionnaire-9, with scores ≥ 10 indicating moderate/severe depression), pain (Pain, Enjoyment, General Activity scale), treatment satisfaction (Treatment Satisfaction Questionnaire for Medication), and other descriptive measures (e.g., past-month employment).
Participants were predominantly men (72%) in their early 40’s, with a primary heroin (55%) or prescription opioid (45%) problem, and a median of 6 years of opioid agonist (i.e., methadone or buprenorphine) treatment across their lifetime. All participants underwent at least 7 days of sublingual buprenorphine treatment prior to starting monthly extended-release buprenorphine injections. At the time of study recruitment, participants had a median duration of 2.2 years on their current opioid agonist treatment, with the majority receiving buprenorphine (94%). Seventeen percent of patients received supplementary doses of sublingual buprenorphine for craving during treatment weeks 4 through 12 of the study.
WHAT DID THIS STUDY FIND?
Most were retained in treatment out to 48 weeks.
Of the 100 patients enrolled in the study, 86% remained in treatment at week 24 and 75% remained in treatment at week 48, including 73% who received all 12 monthly injections. Among the patients who discontinued treatment by week 48, the majority (64%) were lost to treatment follow-up (i.e., stopped going to their treatment provider at some point during the 48 weeks). The remaining 36% who discontinued did so because they entered prison or residential treatment (12%), transitioned to sublingual buprenorphine (8%), experienced medication side effects (4%), or discontinued for some other reason (12%).
Figure 2. Shows the percentage of patients who remained in treatment or discontinued treatment 24 and 48 weeks after their first extended-release buprenorphine injection.
Individuals with less severe drug use before treatment were more likely to remain in treatment.
Controlling for other relevant demographic and clinical factors, patients who did not engage in past-month injection drug use or heroin use at baseline were about 6 times more likely than patients who did engage in these activities to be retained in treatment after 48 weeks of extended-release buprenorphine.
Past-month clinical characteristics, well-being, and treatment satisfaction improved with treatment duration.
For every four weeks that a patient remained on extended-release buprenorphine, the likelihood of substance use decreased by 8% to 20% across various substances. In addition, the odds of past-month injection drug use, moderate-severe depression, and pain decreased for every four weeks on treatment, whereas the odds of employment, quality of life, and treatment satisfaction increased for every four weeks on treatment.
Figure 3. shows the percent increase and decrease in odds of substance use behaviors, well-being, and treatment satisfaction for every 4 months that a patient was retained in extended-release buprenorphine treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the potential benefits of opioid use disorder medication treatments when delivered in real-world settings and in the context of standard outpatient practices.
Retention in injectable extended-release buprenorphine treatment was relatively high over the course of 48 months. Though retention rates here have been observed in prior research, they are somewhat higher than the rates observed in a number of other clinical trials that have assessed retention at 24 and 48 weeks. Retention rates in this study were also higher than those reported in population-based data for sublingual buprenorphine in Australia, where this research was conducted (~46% retention after 12 months).
The high retention rates seen in this study may be due to the fact that the study’s patient population had extensive experience with opioid use disorder medication treatments, and most were already engaged in medication treatment at the time of study enrollment, with the majority receiving sublingual buprenorphine.
A similar investigation of patients transitioning from sublingual buprenorphine to extended-release buprenorphine treatment in real-world settings found that individuals who were retained on extended-release buprenorphine for a longer period of time had been on sublingual buprenorphine for longer durations prior to their first injection. This finding emphasizes that stable established patients, like the ones assessed in the current study, may be particularly good candidates for extended-release buprenorphine treatment. At least among patients with prior opioid agonist treatment experience, this study suggests that retention rates in community-based healthcare services may be similar to or better than those observed in controlled trials. Additional research will help identify whether real-world retention rates in treatment-naïve patients are similarly high.
Regarding predictors of retention, prior studies have also found that recent heroin use and injection drug use are associated with discontinuation of extended-release buprenorphine. These substance-use behaviors suggest clinical instability that may require more intensive follow-up care (e.g., more frequent check-ups) to ensure retention in treatment and attainment of its associated benefits. Additional research will help to identify other factors that put patients at risk of treatment dropout and ultimately help inform individualized treatment plans that support patients at various degrees of risk.
The researchers also found that remaining in treatment was associated with ongoing improvements in patient outcomes, including substance use, treatment satisfaction, and various measures of well-being, which is to be expected as someone progresses in their treatment with an evidence-based medication. Previous studies have shown similar benefits of extended-release buprenorphine when delivered under controlled study settings in medication trials, including reduced illicit opioid use and addiction severity, as well as improved quality of life, mental and physical health, employment status, and perceptions of treatment effectiveness over the course of one year. Importantly, the benefits observed in this study increased with every 4 additional weeks retained in treatment, emphasizing the importance of ongoing treatment engagement for positive treatment and recovery outcomes.
Investigating the treatment course and outcomes of extended-release buprenorphine in real-world settings is important because this medication offers a potentially more convenient treatment option for patients with opioid use disorder. Once-monthly injections, as opposed to daily sublingual buprenorphine dosing allows for fewer doctor visits and trips to the pharmacy, and may help to preventexperiences of stigma and reduce potentially harmful medication dosing rituals and habits. More convenient dosing schedules might also be particularly beneficial for individuals who are experiencing greater psychosocial challenges (e.g., homelessness).Additional studies of extended-release buprenorphine in community-based settings will improve our understanding of who in particular is likely to benefit (or not) from this type of medication’s benefits and lead to more precise treatment recommendations.
This study was conducted in Australia among patients with a long history of prior medication treatment (i.e., buprenorphine and methadone). Findings may not apply to other countries with different community-based treatment models or to individuals who are seeking treatment for the first time.
This study did not include a comparison group, so it is unclear if extended-release buprenorphine treatment outcomes are better or worse than those seen with other opioid use disorder medication treatments delivered in community-based healthcare settings.
BOTTOM LINE
Retention in extended-release buprenorphine treatment among this treatment-engaged population with opioid use disorder was 86% at week 24 and 75% at week 48. Individuals with past-month heroin use and past-month injection drug use at baseline were more likely to discontinue treatment. Remaining in treatment was associated with ongoing improvements in measures of substance use, well-being, and treatment satisfaction. These included a reduced likelihood of illicit substance use, injection drug use, depression, and pain, as well as increased odds of employment, quality of life, and treatment satisfaction, for every four weeks that a patient remained on extended-release buprenorphine. This study contributes to limited research evaluating patient retention and outcomes for extended-release buprenorphine in real-world treatment settings. Enhancing our understanding of the effects of various medication treatments for opioid use disorder will ultimately help guide individualized treatment approaches and best practices for enhancing patients’ treatment and recovery outcomes in the context of medication treatment.
For individuals and families seeking recovery: Buprenorphine is a helpful treatment for opioid use disorder that saves lives. It comes in various formulations, including sublingual and extended-release injectable versions. Individuals who have a recent history of treatment with sublingual buprenorphine and may be looking to start or transition to a more convenient formulation might consider trying once-monthly injections of extended-release injectable buprenorphine. Interested individuals should speak with a knowledgeable prescriber about the risks and benefits of this medication.
For treatment professionals and treatment systems: Treatment-experienced patients with stable histories of sublingual buprenorphine treatment may be good candidates for extended-release formulations. However, patient preference and risk factors like recent injection drug use or illicit drug use should be evaluated when considering initiation of extended-release buprenorphine treatment, given their relationship to treatment engagement and retention. Discussions and check-ins around convenience, side effects, insurance coverage, recovery goals, and ongoing changes in symptoms and well-being are encouraged to support patients’ treatment retention and success. Treatment providers also should be somewhat cautious with decisions to initiate and transition patients to extended-release injectable buprenorphine, given the variability in patient retention seen across other studies.
For scientists:It is essential to conduct additional real-world longitudinal investigations of medication treatments for opioid use disorder. Evaluations of the treatment’s course (e.g., retention, duration, regimen) and patient’s outcomes (substance use, recovery capital, well-being, interpersonal relationships), as well as clinical and demographic moderators, are needed to enhance clinical practice precision and ensure patients are receiving the treatments that will provide them the greatest gains in recovery outcomes. Investigations of extended-release buprenorphine in treatment-naïve patients and in various countries with different treatment models are also needed.
For policy makers: Compared to daily sublingual buprenorphine dosing, once monthly extended-release buprenorphine injections may be a more convenient treatment option for at least some patients with opioid use disorder, which might help to encourage treatment retention and subsequently promote treatment-related improvements in patients. However, there are few studies on treatment retention and patient outcomes for extended-release buprenorphine, limiting our understanding of the benefits of these medications and for whom they might work best. Additional research funding will help identify the full potential of this medication in real-world settings to guide clinical recommendations and individualized treatments to enhance patient outcomes and promote stable recovery among treatment-experienced and -naïve patients.