Can training increase confidence and willingness to prescribe buprenorphine in primary care?
Primary care can help expand access to buprenorphine for opioid use disorder, but relatively few providers offer this medication, which may be due to a lack of skill and confidence in addressing it within their scope of practice. This study examined changes in primary care providers’ knowledge, skills, and attitudes after receiving a novel training for opioid use disorder and medication treatment.
Less than one-third of Americans with a past-year opioid use disorder received addiction treatment at a specialty treatment facility. There has been an increased effort to expand access to treatment, particularly medications for opioid use disorder. Primary care practices are widely available outlets that can be used to expand access to these medications. However, few primary care providers offer medication treatment and those who do typically treat a small number of patients. Primary care providers report several barriers and concerns around providing medication treatment, including worries about taking on a complex patient population. Therefore, merely teaching primary care providers how to prescribe opioid use disorder medication may not be enough to change practice.
Comprehensive medication treatment training programs might help primary care providers overcome misconceptions about opioid use disorder treatment and help encourage providers to integrate medication treatment into their practices. This study developed an opioid use disorder treatment training program specifically designed for primary care providers, and documented changes in providers’ knowledge, skills, and attitudes around opioid use disorder medication treatment, including their willingness to provide medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a muti-site evaluation of a new program that educates primary care providers on opioid use disorder medication treatment and its effect on providers’ perceptions of the importance, their confidence and willingness to implement various aspects of medication treatment in their practices. One hundred and eighty-five primary care providers were recruited from 11 healthcare systems/hospitals, 2 federally qualified health centers, and 2 universities with advanced physician training programs in Northeast Ohio. Primary care providers included physicians, physician assistants, nurse practitioners, and resident physicians.
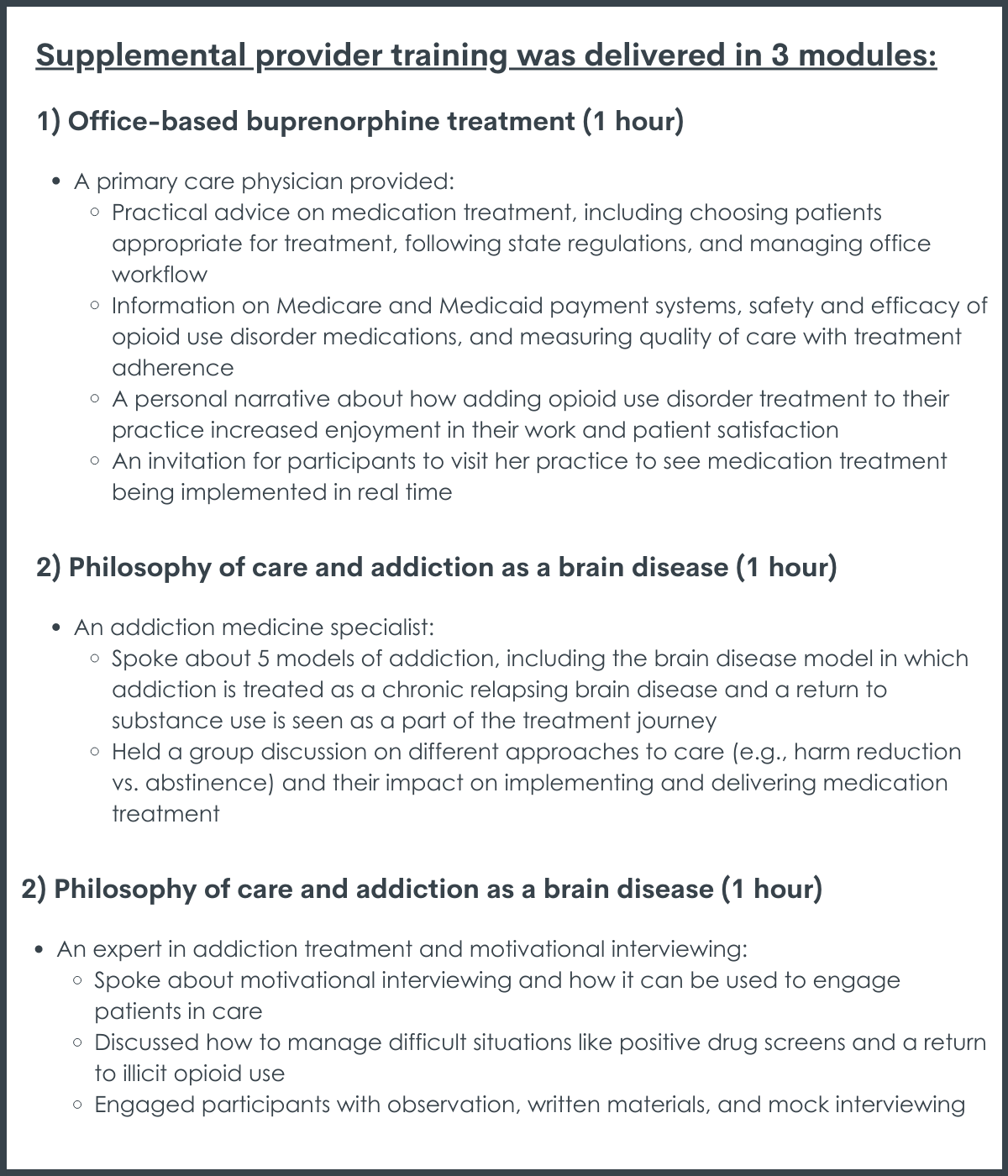
The researchers developed a 4-hour training program that was intended to supplement the 8-hour SAMHSA DATA 2000 waiver training that was previously required for providers to prescribe buprenorphine, but which is no longer required as of June 2023. Training was voluntary and providers were offered $1000 and continuing education credits to participate. The training was intended to address barriers to implementing office-based buprenorphine treatment and to improve primary care providers’ confidence and ability to deliver medication treatment. Supplemental training was delivered in 3 modules:
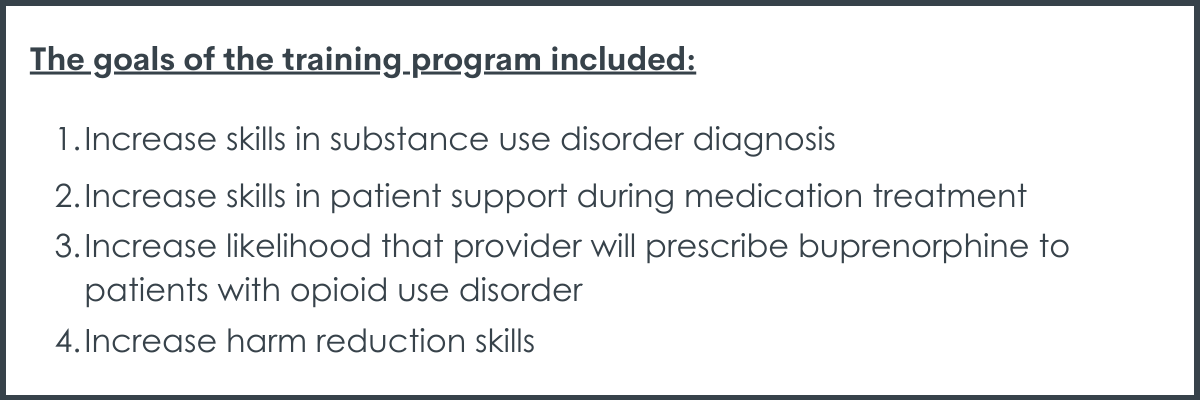
The goals of the training program included: (1) increase skills in substance use disorder diagnosis; (2) increase skills in patient support during medication treatment; (3) increase likelihood that provider will prescribe buprenorphine to patients with opioid use disorder; (4) increase harm reduction skills. A total of 10 training sessions were held between 2018 and 2019.
During the training session, primary care providers completed the first 4 hours of their SAMHSA DATA 2000 waiver training, followed in the same day by the newly developed 4-hour supplemental training. Providers were told to complete the remaining 4 hours of their DATA waiver training online within 30 days (not required to participate) for a total of 12 hours of training. All participants also received the “SAMHSA Treatment Improvement Protocol 63: Medications for Opiate Use Disorder” document as a resource to help them implement medication treatment. Medication treatment experts were available for program/clinical consultation and training for participants who decided to incorporate what they learned into their practices.
To evaluate the effects of the training program, participants were administered a survey before (i.e., just after the 4-hour DATA waiver training) and after completing the supplemental training program. With the help of an expert panel, the researchers developed a survey to evaluate physicians’ attitudes about delivering specific aspects of buprenorphine treatment.
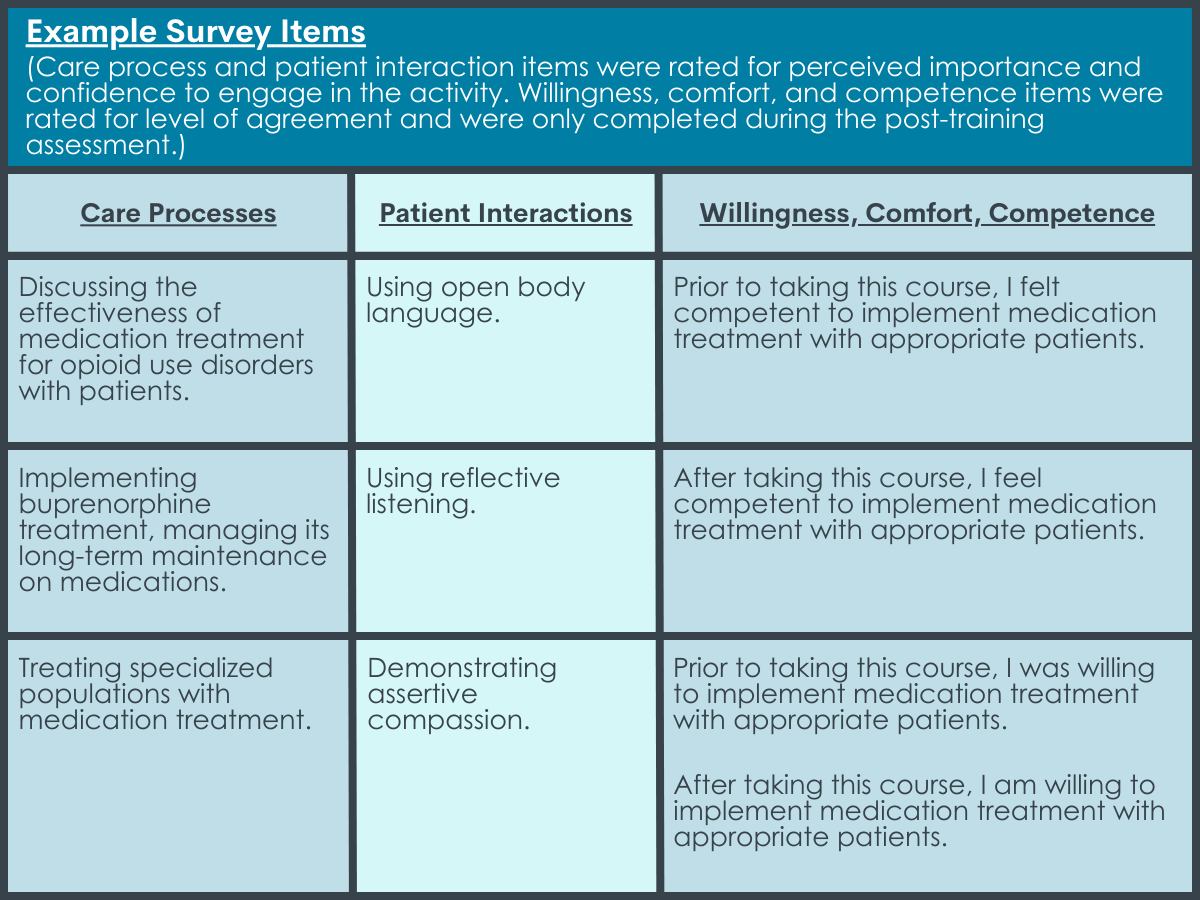
The survey included 12 items that addressed a provider’s perceived importance of engaging in specific treatment practices (i.e., care processes) and patient interactions, as well as their perceived confidence to engage in those practices and interactions. Survey items were rated for importance (9 items) and confidence (3 items) using 4-point Likert scales (1 = ‘Not at all important/confident’ to 4 = ‘Highly important/confident’). An additional eight items were included in the post-training survey only, to evaluate provider’s perceived change in their (1) comfort identifying patients appropriate for medication treatment, (2) competence in implementing medication treatment, (3) willingness to implement medication treatment. These items were intended to assess the training’s impact with pre- and post- training statements rated on a 4-point Likert scale (1 = ‘Strongly disagree’ to 4 = ‘Strongly agree’).
A follow-up survey (80% response rate) was also conducted among providers who completed the supplemental training to identify the percentage of providers who implemented or had plans to implement medication treatment after the training. Those indicating they had plans to implement treatment provided supporting evidence (e.g., colleague training registration, shadowing appointment for hands-on training, etc.).
WHAT DID THIS STUDY FIND?
The supplemental training improved provider’s perceptions of the importance of and confidence in delivering various aspects of medication treatment and patient interactions.
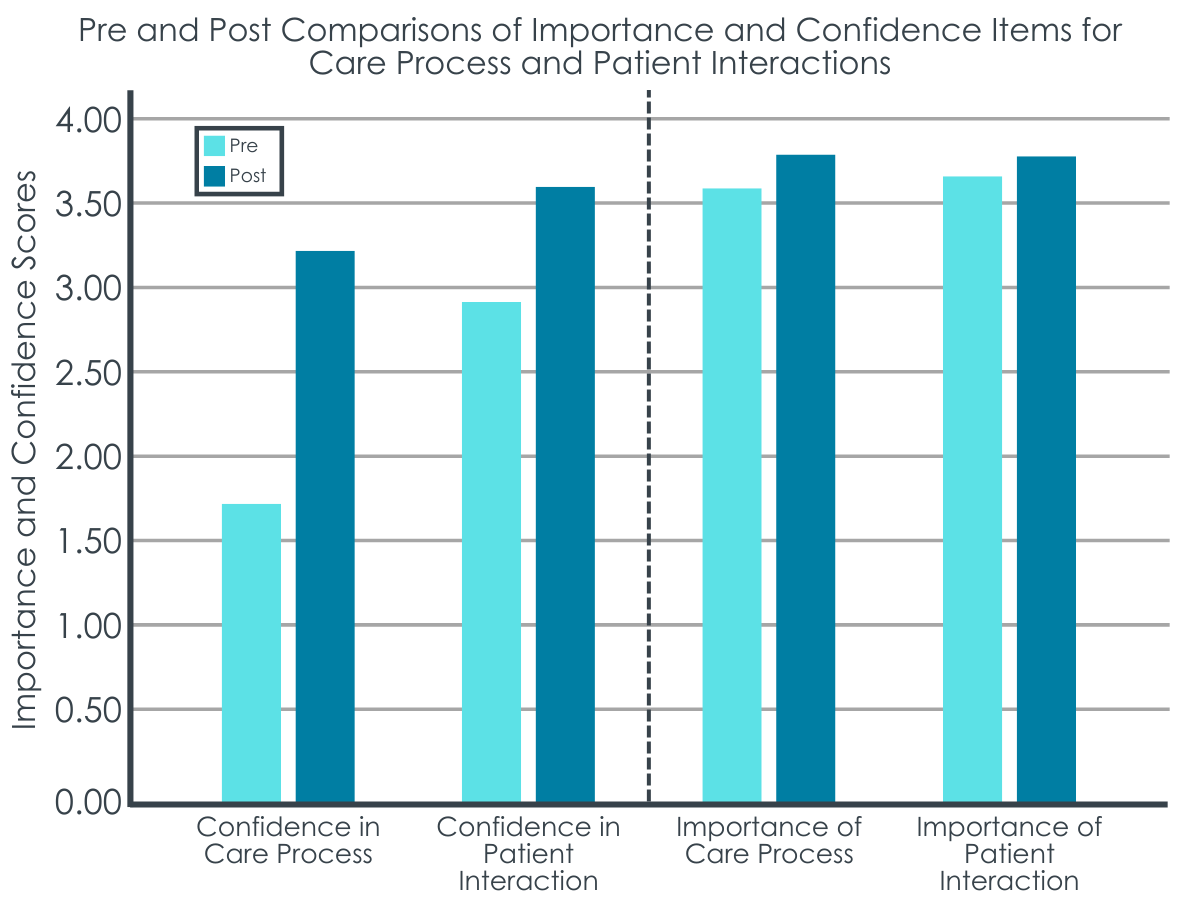
Providers’ confidence in performing medication treatment care processes significantly increased between their pre-training and post-training assessments. A similar, though smaller, increase was also seen for providers’ perceptions of the importance of medication treatment processes and patient interaction skills, as well as their confidence in performing patient interaction skills.
Figure 4 shows changes in confidence and importance for care process and patient interaction both before and after the training was received.
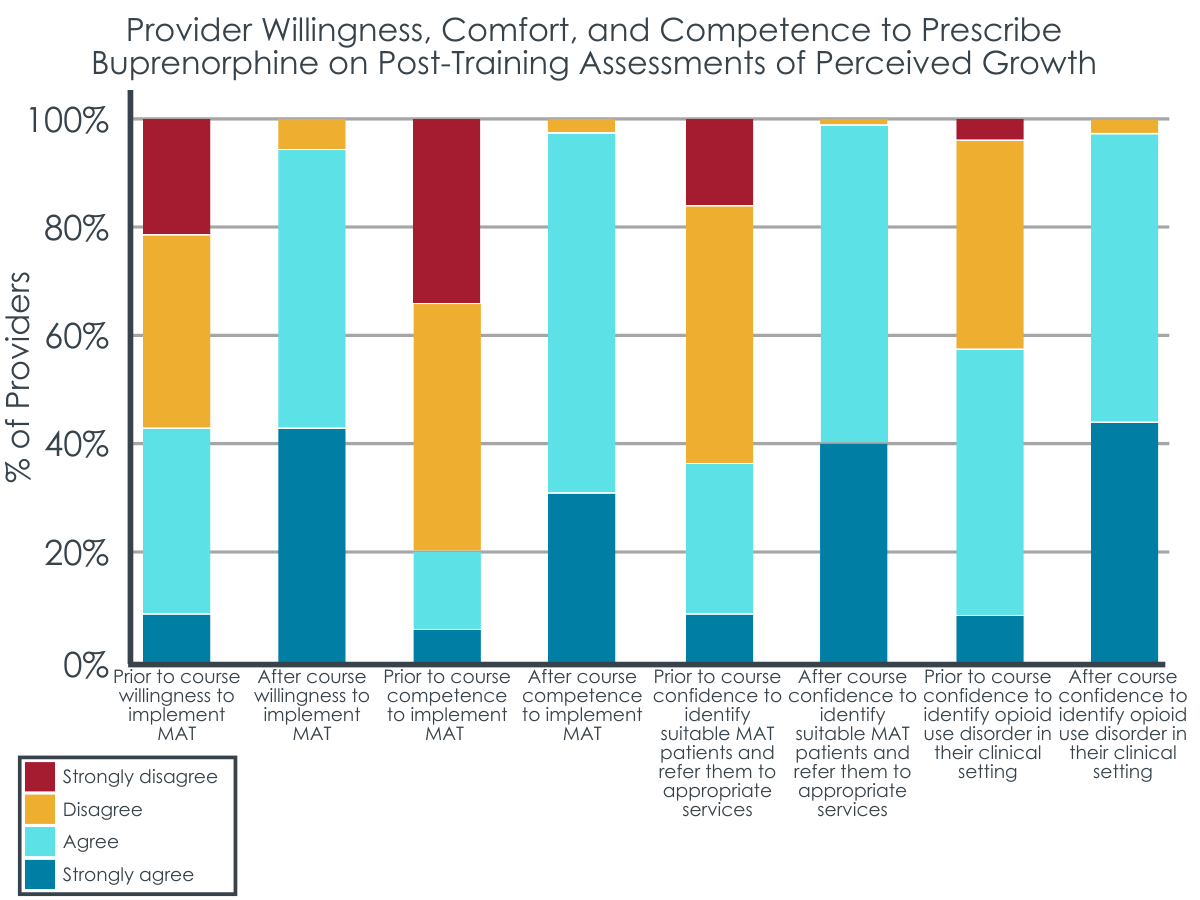
Providers had increased willingness, comfort, and competence to prescribe buprenorphine on post-training assessments of perceived growth.
After the training, providers reflected on their willingness, comfort, and confidence to prescribe before versus after the training. Providers reported being more comfortable and confident with recognizing illicit opioid use, and more comfortable identifying which patients are suitable for medication treatment, after the training. Less than 60% of providers agreed or strongly agreed that they were comfortable with these skills prior to training, whereas nearly all providers agreed or strongly agreed after the training.
Providers also felt that they were more competent and willing to implement medication treatment after the training. Only about 20% of providers agreed or strongly agreed that they were competent in implementing medication treatment before training, but almost 100% agreed or strongly agreed after the training. Similarly, only about 40% of providers agreed or strongly agreed that they were willing to implement medication treatment in their practice prior to training, whereas more than 90% of providers agreed or strongly agreed after training.
Figure 5 shows provider responses to survey items completed after the training.
Most providers implemented or planned to implement medication treatment after supplemental training.
After completing training, over half of providers implemented opioid use disorder medication treatment in their practices and almost 20% had plans to implement medication treatment into their practice.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study described a novel training to help primary care providers to prescribe opioid use disorder medication treatment within their practices. This research is important because it can ultimately help expand access to medication treatment for opioid use disorder. Findings suggest that a new training intended to further educate primary care providers on opioid use disorder medication treatment – supplementing the formerly mandatory DATA waiver training that is no longer required – can improve providers’ perceived importance of and confidence in implementing various medication treatment care processes and patient interaction skills, as well as increase providers’ willingness, comfort, and competence in assessing and providing patients office-based medication treatment.
Evaluating perceived importance of and confidence in engaging in specific medication treatment practices is important because these factors are thought to be associated with motivation to change a behavior. Thus, if providers aren’t confident in prescribing medication treatment to patients and/or don’t see it as important, they may be unlikely to start offering medication treatment in their practices.
In this study, confidence in implementing medication treatment care processes (e.g., discussing treatment options and goals with patients; providing medication treatment and long-term management) increased after training, with providers reporting that on average they were not at all confident before training and were moderately confident after training. Given additional room to grow in confidence post training, programs with additional guidance and consultation as providers start up buprenorphine treatment programs in their practices may be needed. Importance of care processes and patient interactions, as well as confidence in patient interactions also increased, though to a lesser degree. This may be due to the high ratings on these items before providers completed the supplemental training, which left less room for providers to improve in the post-training evaluation (i.e., “ceiling” measurement effects). Additional research is needed to determine if this training is beneficial for improving importance and confidence in performing various aspects medication treatment among providers who have more negative views on medication treatment or less baseline education prior to training.
Nonetheless, the improvement in provider perceptions seen here suggests provider education programs that support systems with practical advice and information on screening for opioid use disorder, implementing medication treatment in primary care, and managing patients with an emphasis on the brain disease model of addiction can help promote positive perceptions about treating patients with opioid use disorder and increase willingness to provide medication treatment, which can ultimately help expand access to treatment to better address the opioid epidemic. Providers here increased their willingness to implement medication treatment in their practices by about 50% and increased their perceived competence to implement medication treatment by about 75%. In the author’s follow-up survey, they also found that the majority of providers who completed the training subsequently implemented or had plans to implement medication treatment into their practices. That said, it remains unclear whether any potential adoption of this new change in practice would be maintained over time without further support. More research is needed in this regard.
Also, providers were recruited from several hospital systems, and it is unclear if providers in this study already had plans to obtain a DATA waiver and implement medication treatment into their practices prior to the supplemental training. This would have increased their motivation to actually implement medication treatment thereafter and may have accounted for the high percentage of providers who reported implementing medication treatment at the time of follow up, rather than the novel training itself. Given the demand for opioid use disorder treatment outpaces supply, additional research on training programs like this is essential for adequately equipping providers with the skills, practical knowledge, and confidence they need to offer office-based medication treatment to their patients.
It should be noted, however, that this 4-hour training was intended to supplement the 8-hour SAMHSA training that was previously required to prescribe buprenorphine for opioid use disorder, and all providers in this study received at least 4 hours of the SAMHSA training prior to receiving the new supplement. Given that this 8-hour training is no longer required to prescribe buprenorphine, it is important to determine the independent effects of the SAMHSA DATA waiver training vs. the training developed in this study. It is also essential to identify who might benefit from training and how training programs like the one developed in this study impact provider perspectives and provision of buprenorphine sans buprenorphine waiver training requirements. Allotting dedicated training time for providers and offering free trainings with continuing education credits may also be warranted to encourage providers to engage in such trainings, particularly for those reluctant to learn more about medication treatment. Additional research is needed to determine best training practices and how to promote training within healthcare systems to increase willingness to prescribe opioid use disorder medication treatment.
This study was conducted when the DATA waiver was required for primary care providers to prescribe buprenorphine treatment and all participants completed at least 4 hours of waiver training prior to engaging in this study’s supplemental training. Given that the waiver and its associated training is no longer required, additional research is needed to determine the effects of this study’s educational program as a stand-alone training, relative to no training and other training models. This study was also conducted in a single state, limiting conclusions about the applicability of results to primary care practices and providers in other states.
Primary care providers in this study had time built into their schedule to accommodate training, which is not common across all healthcare systems. Training was also voluntary, and providers were offered $1000 and continuing education credits to participate. This makes it unclear if providers would be motivated to engage in such training without training-dedicated work hours or financial compensation. Alternatively, these providers may have been particularly motivated to complete the training and because they already had plans to obtain a DATA waiver and implement medication treatment in their practices.
Training was delivered by experts in addiction medicine and medication treatment experts were available to providers for program/clinical consultation to help them incorporate opioid use disorder treatment into their practices. Identifying experts with a high level of expertise in addiction and medication treatment to train and advise providers in medication treatment program development may not be feasible across all healthcare systems, though mainstreaming of video conferencing platforms during the COVID-19 pandemic encourage new scalable approaches to access buprenorphine trainings like these.
BOTTOM LINE
Providers who completed this supplementary educational program showed several improvements in their perceptions of opioid use disorder medication treatment. These included higher perceived importance of medication treatment care processes and patient interaction skills, greater confidence in implementing medication treatment and patient interaction skills, as well as increased willingness, comfort, and competence to assess patients and provide them with office-based medication treatment. Improvements were accompanied by a relatively high percentage of providers who implemented or had plans to implement medication treatment into their practice after the training.
Though additional research is needed now that training requirements for prescribing medication treatment have changed, provider education programs that support medical professionals with practical training on opioid use disorder screening, implementing and maintaining medication treatment in primary care, and managing patients with an emphasis on the brain disease model of addiction might help promote positive perceptions about medication treatment and increase providers’ willingness to provide it in their primary care practices, which can ultimately help expand access to opioid use disorder treatment. Given that this study did not include a control condition, other factors might explain the increase in perceived competence and willingness to prescribe, and future studies that control for potentially influential factors will help clarify the effect of provider training on willingness to prescribe opioid use disorder medication treatment.
For individuals and families seeking recovery: Individuals seeking medication treatment should know that training and education around medication treatment can vary among different primary care providers. Engaging more providers in training might ultimately encourage more doctors to offer medication treatment programs, which could help meet the high demand for opioid use disorder treatment. Individuals are encouraged to speak with their current healthcare providers to identify a primary care practice with a treatment model and provider that works with them to support their treatment and recovery.
For treatment professionals and treatment systems: This study helps us examine new ways to motivate the primary care workforce to provide office-based medication treatment for opioid use disorder, which can help increase patient access to medication treatment. Engaging in ongoing supplemental education that supports practical training on opioid use disorder screening and implementation of medication treatment in primary care might help promote providers’ positive perceptions about opioid use disorder medication treatment and increase their willingness to provide it in their practices. Treatment professionals and systems are encouraged to find training programs that help support startup of medication treatment programs and maintenance of those programs over time, in the context of primary care, to increase providers’ confidence and willingness to prescribe medication treatment. Additional research will help us better identify the best training elements and ideal educational programing to encourage providers to start implementing medication treatment and support their confidence in maintaining such programs within their practices.
For scientists: Additional research, including randomized controlled trials, is needed to extend these findings in different healthcare settings and other states while controlling for potentially confounding factors. Studies are needed to evaluate and reassess this training program’s content, and programs like it, now that DATA waiver training is no longer required. Identification of other factors impacting provider perceptions of medication treatment provision, as well as confidence and willingness to implement medication as well as maintain treatment in primary care practices is also needed. Additional research will help identify provider barriers to medication treatment provision in various healthcare settings, and address barriers by expanding existing training program content and developing novel programs and methods to expand access to medication treatment. Research among providers who are particularly reluctant to prescribe opioid use disorder medication treatment is also needed to determine if training programs like this can be effective in this subset of providers.
For policy makers: Studies like this highlight potential ways to expand access to opioid use disorder medication treatment. This study found that a new 4-hour educational program with practical training that gives providers information on how to implement opioid use disorder medication treatment in their primary care practices may be a useful way to enhance provider confidence, willingness, and actual implementation of medication treatment into their practices. Given that this study was conducted before federal regulations changed around training and buprenorphine prescribing, more research is needed. Additional funding will help identify the best training programs and methods encourage primary care providers to offer medication treatment and support those who ultimately prescribe them. This can ultimately expand access to medication treatment, which is currently needed to better address the opioid epidemic.
Less than one-third of Americans with a past-year opioid use disorder received addiction treatment at a specialty treatment facility. There has been an increased effort to expand access to treatment, particularly medications for opioid use disorder. Primary care practices are widely available outlets that can be used to expand access to these medications. However, few primary care providers offer medication treatment and those who do typically treat a small number of patients. Primary care providers report several barriers and concerns around providing medication treatment, including worries about taking on a complex patient population. Therefore, merely teaching primary care providers how to prescribe opioid use disorder medication may not be enough to change practice.
Comprehensive medication treatment training programs might help primary care providers overcome misconceptions about opioid use disorder treatment and help encourage providers to integrate medication treatment into their practices. This study developed an opioid use disorder treatment training program specifically designed for primary care providers, and documented changes in providers’ knowledge, skills, and attitudes around opioid use disorder medication treatment, including their willingness to provide medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a muti-site evaluation of a new program that educates primary care providers on opioid use disorder medication treatment and its effect on providers’ perceptions of the importance, their confidence and willingness to implement various aspects of medication treatment in their practices. One hundred and eighty-five primary care providers were recruited from 11 healthcare systems/hospitals, 2 federally qualified health centers, and 2 universities with advanced physician training programs in Northeast Ohio. Primary care providers included physicians, physician assistants, nurse practitioners, and resident physicians.
The researchers developed a 4-hour training program that was intended to supplement the 8-hour SAMHSA DATA 2000 waiver training that was previously required for providers to prescribe buprenorphine, but which is no longer required as of June 2023. Training was voluntary and providers were offered $1000 and continuing education credits to participate. The training was intended to address barriers to implementing office-based buprenorphine treatment and to improve primary care providers’ confidence and ability to deliver medication treatment. Supplemental training was delivered in 3 modules:
The goals of the training program included: (1) increase skills in substance use disorder diagnosis; (2) increase skills in patient support during medication treatment; (3) increase likelihood that provider will prescribe buprenorphine to patients with opioid use disorder; (4) increase harm reduction skills. A total of 10 training sessions were held between 2018 and 2019.
During the training session, primary care providers completed the first 4 hours of their SAMHSA DATA 2000 waiver training, followed in the same day by the newly developed 4-hour supplemental training. Providers were told to complete the remaining 4 hours of their DATA waiver training online within 30 days (not required to participate) for a total of 12 hours of training. All participants also received the “SAMHSA Treatment Improvement Protocol 63: Medications for Opiate Use Disorder” document as a resource to help them implement medication treatment. Medication treatment experts were available for program/clinical consultation and training for participants who decided to incorporate what they learned into their practices.
To evaluate the effects of the training program, participants were administered a survey before (i.e., just after the 4-hour DATA waiver training) and after completing the supplemental training program. With the help of an expert panel, the researchers developed a survey to evaluate physicians’ attitudes about delivering specific aspects of buprenorphine treatment.
The survey included 12 items that addressed a provider’s perceived importance of engaging in specific treatment practices (i.e., care processes) and patient interactions, as well as their perceived confidence to engage in those practices and interactions. Survey items were rated for importance (9 items) and confidence (3 items) using 4-point Likert scales (1 = ‘Not at all important/confident’ to 4 = ‘Highly important/confident’). An additional eight items were included in the post-training survey only, to evaluate provider’s perceived change in their (1) comfort identifying patients appropriate for medication treatment, (2) competence in implementing medication treatment, (3) willingness to implement medication treatment. These items were intended to assess the training’s impact with pre- and post- training statements rated on a 4-point Likert scale (1 = ‘Strongly disagree’ to 4 = ‘Strongly agree’).
A follow-up survey (80% response rate) was also conducted among providers who completed the supplemental training to identify the percentage of providers who implemented or had plans to implement medication treatment after the training. Those indicating they had plans to implement treatment provided supporting evidence (e.g., colleague training registration, shadowing appointment for hands-on training, etc.).
WHAT DID THIS STUDY FIND?
The supplemental training improved provider’s perceptions of the importance of and confidence in delivering various aspects of medication treatment and patient interactions.
Providers’ confidence in performing medication treatment care processes significantly increased between their pre-training and post-training assessments. A similar, though smaller, increase was also seen for providers’ perceptions of the importance of medication treatment processes and patient interaction skills, as well as their confidence in performing patient interaction skills.
Figure 4 shows changes in confidence and importance for care process and patient interaction both before and after the training was received.
Providers had increased willingness, comfort, and competence to prescribe buprenorphine on post-training assessments of perceived growth.
After the training, providers reflected on their willingness, comfort, and confidence to prescribe before versus after the training. Providers reported being more comfortable and confident with recognizing illicit opioid use, and more comfortable identifying which patients are suitable for medication treatment, after the training. Less than 60% of providers agreed or strongly agreed that they were comfortable with these skills prior to training, whereas nearly all providers agreed or strongly agreed after the training.
Providers also felt that they were more competent and willing to implement medication treatment after the training. Only about 20% of providers agreed or strongly agreed that they were competent in implementing medication treatment before training, but almost 100% agreed or strongly agreed after the training. Similarly, only about 40% of providers agreed or strongly agreed that they were willing to implement medication treatment in their practice prior to training, whereas more than 90% of providers agreed or strongly agreed after training.
Figure 5 shows provider responses to survey items completed after the training.
Most providers implemented or planned to implement medication treatment after supplemental training.
After completing training, over half of providers implemented opioid use disorder medication treatment in their practices and almost 20% had plans to implement medication treatment into their practice.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study described a novel training to help primary care providers to prescribe opioid use disorder medication treatment within their practices. This research is important because it can ultimately help expand access to medication treatment for opioid use disorder. Findings suggest that a new training intended to further educate primary care providers on opioid use disorder medication treatment – supplementing the formerly mandatory DATA waiver training that is no longer required – can improve providers’ perceived importance of and confidence in implementing various medication treatment care processes and patient interaction skills, as well as increase providers’ willingness, comfort, and competence in assessing and providing patients office-based medication treatment.
Evaluating perceived importance of and confidence in engaging in specific medication treatment practices is important because these factors are thought to be associated with motivation to change a behavior. Thus, if providers aren’t confident in prescribing medication treatment to patients and/or don’t see it as important, they may be unlikely to start offering medication treatment in their practices.
In this study, confidence in implementing medication treatment care processes (e.g., discussing treatment options and goals with patients; providing medication treatment and long-term management) increased after training, with providers reporting that on average they were not at all confident before training and were moderately confident after training. Given additional room to grow in confidence post training, programs with additional guidance and consultation as providers start up buprenorphine treatment programs in their practices may be needed. Importance of care processes and patient interactions, as well as confidence in patient interactions also increased, though to a lesser degree. This may be due to the high ratings on these items before providers completed the supplemental training, which left less room for providers to improve in the post-training evaluation (i.e., “ceiling” measurement effects). Additional research is needed to determine if this training is beneficial for improving importance and confidence in performing various aspects medication treatment among providers who have more negative views on medication treatment or less baseline education prior to training.
Nonetheless, the improvement in provider perceptions seen here suggests provider education programs that support systems with practical advice and information on screening for opioid use disorder, implementing medication treatment in primary care, and managing patients with an emphasis on the brain disease model of addiction can help promote positive perceptions about treating patients with opioid use disorder and increase willingness to provide medication treatment, which can ultimately help expand access to treatment to better address the opioid epidemic. Providers here increased their willingness to implement medication treatment in their practices by about 50% and increased their perceived competence to implement medication treatment by about 75%. In the author’s follow-up survey, they also found that the majority of providers who completed the training subsequently implemented or had plans to implement medication treatment into their practices. That said, it remains unclear whether any potential adoption of this new change in practice would be maintained over time without further support. More research is needed in this regard.
Also, providers were recruited from several hospital systems, and it is unclear if providers in this study already had plans to obtain a DATA waiver and implement medication treatment into their practices prior to the supplemental training. This would have increased their motivation to actually implement medication treatment thereafter and may have accounted for the high percentage of providers who reported implementing medication treatment at the time of follow up, rather than the novel training itself. Given the demand for opioid use disorder treatment outpaces supply, additional research on training programs like this is essential for adequately equipping providers with the skills, practical knowledge, and confidence they need to offer office-based medication treatment to their patients.
It should be noted, however, that this 4-hour training was intended to supplement the 8-hour SAMHSA training that was previously required to prescribe buprenorphine for opioid use disorder, and all providers in this study received at least 4 hours of the SAMHSA training prior to receiving the new supplement. Given that this 8-hour training is no longer required to prescribe buprenorphine, it is important to determine the independent effects of the SAMHSA DATA waiver training vs. the training developed in this study. It is also essential to identify who might benefit from training and how training programs like the one developed in this study impact provider perspectives and provision of buprenorphine sans buprenorphine waiver training requirements. Allotting dedicated training time for providers and offering free trainings with continuing education credits may also be warranted to encourage providers to engage in such trainings, particularly for those reluctant to learn more about medication treatment. Additional research is needed to determine best training practices and how to promote training within healthcare systems to increase willingness to prescribe opioid use disorder medication treatment.
This study was conducted when the DATA waiver was required for primary care providers to prescribe buprenorphine treatment and all participants completed at least 4 hours of waiver training prior to engaging in this study’s supplemental training. Given that the waiver and its associated training is no longer required, additional research is needed to determine the effects of this study’s educational program as a stand-alone training, relative to no training and other training models. This study was also conducted in a single state, limiting conclusions about the applicability of results to primary care practices and providers in other states.
Primary care providers in this study had time built into their schedule to accommodate training, which is not common across all healthcare systems. Training was also voluntary, and providers were offered $1000 and continuing education credits to participate. This makes it unclear if providers would be motivated to engage in such training without training-dedicated work hours or financial compensation. Alternatively, these providers may have been particularly motivated to complete the training and because they already had plans to obtain a DATA waiver and implement medication treatment in their practices.
Training was delivered by experts in addiction medicine and medication treatment experts were available to providers for program/clinical consultation to help them incorporate opioid use disorder treatment into their practices. Identifying experts with a high level of expertise in addiction and medication treatment to train and advise providers in medication treatment program development may not be feasible across all healthcare systems, though mainstreaming of video conferencing platforms during the COVID-19 pandemic encourage new scalable approaches to access buprenorphine trainings like these.
BOTTOM LINE
Providers who completed this supplementary educational program showed several improvements in their perceptions of opioid use disorder medication treatment. These included higher perceived importance of medication treatment care processes and patient interaction skills, greater confidence in implementing medication treatment and patient interaction skills, as well as increased willingness, comfort, and competence to assess patients and provide them with office-based medication treatment. Improvements were accompanied by a relatively high percentage of providers who implemented or had plans to implement medication treatment into their practice after the training.
Though additional research is needed now that training requirements for prescribing medication treatment have changed, provider education programs that support medical professionals with practical training on opioid use disorder screening, implementing and maintaining medication treatment in primary care, and managing patients with an emphasis on the brain disease model of addiction might help promote positive perceptions about medication treatment and increase providers’ willingness to provide it in their primary care practices, which can ultimately help expand access to opioid use disorder treatment. Given that this study did not include a control condition, other factors might explain the increase in perceived competence and willingness to prescribe, and future studies that control for potentially influential factors will help clarify the effect of provider training on willingness to prescribe opioid use disorder medication treatment.
For individuals and families seeking recovery: Individuals seeking medication treatment should know that training and education around medication treatment can vary among different primary care providers. Engaging more providers in training might ultimately encourage more doctors to offer medication treatment programs, which could help meet the high demand for opioid use disorder treatment. Individuals are encouraged to speak with their current healthcare providers to identify a primary care practice with a treatment model and provider that works with them to support their treatment and recovery.
For treatment professionals and treatment systems: This study helps us examine new ways to motivate the primary care workforce to provide office-based medication treatment for opioid use disorder, which can help increase patient access to medication treatment. Engaging in ongoing supplemental education that supports practical training on opioid use disorder screening and implementation of medication treatment in primary care might help promote providers’ positive perceptions about opioid use disorder medication treatment and increase their willingness to provide it in their practices. Treatment professionals and systems are encouraged to find training programs that help support startup of medication treatment programs and maintenance of those programs over time, in the context of primary care, to increase providers’ confidence and willingness to prescribe medication treatment. Additional research will help us better identify the best training elements and ideal educational programing to encourage providers to start implementing medication treatment and support their confidence in maintaining such programs within their practices.
For scientists: Additional research, including randomized controlled trials, is needed to extend these findings in different healthcare settings and other states while controlling for potentially confounding factors. Studies are needed to evaluate and reassess this training program’s content, and programs like it, now that DATA waiver training is no longer required. Identification of other factors impacting provider perceptions of medication treatment provision, as well as confidence and willingness to implement medication as well as maintain treatment in primary care practices is also needed. Additional research will help identify provider barriers to medication treatment provision in various healthcare settings, and address barriers by expanding existing training program content and developing novel programs and methods to expand access to medication treatment. Research among providers who are particularly reluctant to prescribe opioid use disorder medication treatment is also needed to determine if training programs like this can be effective in this subset of providers.
For policy makers: Studies like this highlight potential ways to expand access to opioid use disorder medication treatment. This study found that a new 4-hour educational program with practical training that gives providers information on how to implement opioid use disorder medication treatment in their primary care practices may be a useful way to enhance provider confidence, willingness, and actual implementation of medication treatment into their practices. Given that this study was conducted before federal regulations changed around training and buprenorphine prescribing, more research is needed. Additional funding will help identify the best training programs and methods encourage primary care providers to offer medication treatment and support those who ultimately prescribe them. This can ultimately expand access to medication treatment, which is currently needed to better address the opioid epidemic.
Less than one-third of Americans with a past-year opioid use disorder received addiction treatment at a specialty treatment facility. There has been an increased effort to expand access to treatment, particularly medications for opioid use disorder. Primary care practices are widely available outlets that can be used to expand access to these medications. However, few primary care providers offer medication treatment and those who do typically treat a small number of patients. Primary care providers report several barriers and concerns around providing medication treatment, including worries about taking on a complex patient population. Therefore, merely teaching primary care providers how to prescribe opioid use disorder medication may not be enough to change practice.
Comprehensive medication treatment training programs might help primary care providers overcome misconceptions about opioid use disorder treatment and help encourage providers to integrate medication treatment into their practices. This study developed an opioid use disorder treatment training program specifically designed for primary care providers, and documented changes in providers’ knowledge, skills, and attitudes around opioid use disorder medication treatment, including their willingness to provide medication treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a muti-site evaluation of a new program that educates primary care providers on opioid use disorder medication treatment and its effect on providers’ perceptions of the importance, their confidence and willingness to implement various aspects of medication treatment in their practices. One hundred and eighty-five primary care providers were recruited from 11 healthcare systems/hospitals, 2 federally qualified health centers, and 2 universities with advanced physician training programs in Northeast Ohio. Primary care providers included physicians, physician assistants, nurse practitioners, and resident physicians.
The researchers developed a 4-hour training program that was intended to supplement the 8-hour SAMHSA DATA 2000 waiver training that was previously required for providers to prescribe buprenorphine, but which is no longer required as of June 2023. Training was voluntary and providers were offered $1000 and continuing education credits to participate. The training was intended to address barriers to implementing office-based buprenorphine treatment and to improve primary care providers’ confidence and ability to deliver medication treatment. Supplemental training was delivered in 3 modules:
The goals of the training program included: (1) increase skills in substance use disorder diagnosis; (2) increase skills in patient support during medication treatment; (3) increase likelihood that provider will prescribe buprenorphine to patients with opioid use disorder; (4) increase harm reduction skills. A total of 10 training sessions were held between 2018 and 2019.
During the training session, primary care providers completed the first 4 hours of their SAMHSA DATA 2000 waiver training, followed in the same day by the newly developed 4-hour supplemental training. Providers were told to complete the remaining 4 hours of their DATA waiver training online within 30 days (not required to participate) for a total of 12 hours of training. All participants also received the “SAMHSA Treatment Improvement Protocol 63: Medications for Opiate Use Disorder” document as a resource to help them implement medication treatment. Medication treatment experts were available for program/clinical consultation and training for participants who decided to incorporate what they learned into their practices.
To evaluate the effects of the training program, participants were administered a survey before (i.e., just after the 4-hour DATA waiver training) and after completing the supplemental training program. With the help of an expert panel, the researchers developed a survey to evaluate physicians’ attitudes about delivering specific aspects of buprenorphine treatment.
The survey included 12 items that addressed a provider’s perceived importance of engaging in specific treatment practices (i.e., care processes) and patient interactions, as well as their perceived confidence to engage in those practices and interactions. Survey items were rated for importance (9 items) and confidence (3 items) using 4-point Likert scales (1 = ‘Not at all important/confident’ to 4 = ‘Highly important/confident’). An additional eight items were included in the post-training survey only, to evaluate provider’s perceived change in their (1) comfort identifying patients appropriate for medication treatment, (2) competence in implementing medication treatment, (3) willingness to implement medication treatment. These items were intended to assess the training’s impact with pre- and post- training statements rated on a 4-point Likert scale (1 = ‘Strongly disagree’ to 4 = ‘Strongly agree’).
A follow-up survey (80% response rate) was also conducted among providers who completed the supplemental training to identify the percentage of providers who implemented or had plans to implement medication treatment after the training. Those indicating they had plans to implement treatment provided supporting evidence (e.g., colleague training registration, shadowing appointment for hands-on training, etc.).
WHAT DID THIS STUDY FIND?
The supplemental training improved provider’s perceptions of the importance of and confidence in delivering various aspects of medication treatment and patient interactions.
Providers’ confidence in performing medication treatment care processes significantly increased between their pre-training and post-training assessments. A similar, though smaller, increase was also seen for providers’ perceptions of the importance of medication treatment processes and patient interaction skills, as well as their confidence in performing patient interaction skills.
Figure 4 shows changes in confidence and importance for care process and patient interaction both before and after the training was received.
Providers had increased willingness, comfort, and competence to prescribe buprenorphine on post-training assessments of perceived growth.
After the training, providers reflected on their willingness, comfort, and confidence to prescribe before versus after the training. Providers reported being more comfortable and confident with recognizing illicit opioid use, and more comfortable identifying which patients are suitable for medication treatment, after the training. Less than 60% of providers agreed or strongly agreed that they were comfortable with these skills prior to training, whereas nearly all providers agreed or strongly agreed after the training.
Providers also felt that they were more competent and willing to implement medication treatment after the training. Only about 20% of providers agreed or strongly agreed that they were competent in implementing medication treatment before training, but almost 100% agreed or strongly agreed after the training. Similarly, only about 40% of providers agreed or strongly agreed that they were willing to implement medication treatment in their practice prior to training, whereas more than 90% of providers agreed or strongly agreed after training.
Figure 5 shows provider responses to survey items completed after the training.
Most providers implemented or planned to implement medication treatment after supplemental training.
After completing training, over half of providers implemented opioid use disorder medication treatment in their practices and almost 20% had plans to implement medication treatment into their practice.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study described a novel training to help primary care providers to prescribe opioid use disorder medication treatment within their practices. This research is important because it can ultimately help expand access to medication treatment for opioid use disorder. Findings suggest that a new training intended to further educate primary care providers on opioid use disorder medication treatment – supplementing the formerly mandatory DATA waiver training that is no longer required – can improve providers’ perceived importance of and confidence in implementing various medication treatment care processes and patient interaction skills, as well as increase providers’ willingness, comfort, and competence in assessing and providing patients office-based medication treatment.
Evaluating perceived importance of and confidence in engaging in specific medication treatment practices is important because these factors are thought to be associated with motivation to change a behavior. Thus, if providers aren’t confident in prescribing medication treatment to patients and/or don’t see it as important, they may be unlikely to start offering medication treatment in their practices.
In this study, confidence in implementing medication treatment care processes (e.g., discussing treatment options and goals with patients; providing medication treatment and long-term management) increased after training, with providers reporting that on average they were not at all confident before training and were moderately confident after training. Given additional room to grow in confidence post training, programs with additional guidance and consultation as providers start up buprenorphine treatment programs in their practices may be needed. Importance of care processes and patient interactions, as well as confidence in patient interactions also increased, though to a lesser degree. This may be due to the high ratings on these items before providers completed the supplemental training, which left less room for providers to improve in the post-training evaluation (i.e., “ceiling” measurement effects). Additional research is needed to determine if this training is beneficial for improving importance and confidence in performing various aspects medication treatment among providers who have more negative views on medication treatment or less baseline education prior to training.
Nonetheless, the improvement in provider perceptions seen here suggests provider education programs that support systems with practical advice and information on screening for opioid use disorder, implementing medication treatment in primary care, and managing patients with an emphasis on the brain disease model of addiction can help promote positive perceptions about treating patients with opioid use disorder and increase willingness to provide medication treatment, which can ultimately help expand access to treatment to better address the opioid epidemic. Providers here increased their willingness to implement medication treatment in their practices by about 50% and increased their perceived competence to implement medication treatment by about 75%. In the author’s follow-up survey, they also found that the majority of providers who completed the training subsequently implemented or had plans to implement medication treatment into their practices. That said, it remains unclear whether any potential adoption of this new change in practice would be maintained over time without further support. More research is needed in this regard.
Also, providers were recruited from several hospital systems, and it is unclear if providers in this study already had plans to obtain a DATA waiver and implement medication treatment into their practices prior to the supplemental training. This would have increased their motivation to actually implement medication treatment thereafter and may have accounted for the high percentage of providers who reported implementing medication treatment at the time of follow up, rather than the novel training itself. Given the demand for opioid use disorder treatment outpaces supply, additional research on training programs like this is essential for adequately equipping providers with the skills, practical knowledge, and confidence they need to offer office-based medication treatment to their patients.
It should be noted, however, that this 4-hour training was intended to supplement the 8-hour SAMHSA training that was previously required to prescribe buprenorphine for opioid use disorder, and all providers in this study received at least 4 hours of the SAMHSA training prior to receiving the new supplement. Given that this 8-hour training is no longer required to prescribe buprenorphine, it is important to determine the independent effects of the SAMHSA DATA waiver training vs. the training developed in this study. It is also essential to identify who might benefit from training and how training programs like the one developed in this study impact provider perspectives and provision of buprenorphine sans buprenorphine waiver training requirements. Allotting dedicated training time for providers and offering free trainings with continuing education credits may also be warranted to encourage providers to engage in such trainings, particularly for those reluctant to learn more about medication treatment. Additional research is needed to determine best training practices and how to promote training within healthcare systems to increase willingness to prescribe opioid use disorder medication treatment.
This study was conducted when the DATA waiver was required for primary care providers to prescribe buprenorphine treatment and all participants completed at least 4 hours of waiver training prior to engaging in this study’s supplemental training. Given that the waiver and its associated training is no longer required, additional research is needed to determine the effects of this study’s educational program as a stand-alone training, relative to no training and other training models. This study was also conducted in a single state, limiting conclusions about the applicability of results to primary care practices and providers in other states.
Primary care providers in this study had time built into their schedule to accommodate training, which is not common across all healthcare systems. Training was also voluntary, and providers were offered $1000 and continuing education credits to participate. This makes it unclear if providers would be motivated to engage in such training without training-dedicated work hours or financial compensation. Alternatively, these providers may have been particularly motivated to complete the training and because they already had plans to obtain a DATA waiver and implement medication treatment in their practices.
Training was delivered by experts in addiction medicine and medication treatment experts were available to providers for program/clinical consultation to help them incorporate opioid use disorder treatment into their practices. Identifying experts with a high level of expertise in addiction and medication treatment to train and advise providers in medication treatment program development may not be feasible across all healthcare systems, though mainstreaming of video conferencing platforms during the COVID-19 pandemic encourage new scalable approaches to access buprenorphine trainings like these.
BOTTOM LINE
Providers who completed this supplementary educational program showed several improvements in their perceptions of opioid use disorder medication treatment. These included higher perceived importance of medication treatment care processes and patient interaction skills, greater confidence in implementing medication treatment and patient interaction skills, as well as increased willingness, comfort, and competence to assess patients and provide them with office-based medication treatment. Improvements were accompanied by a relatively high percentage of providers who implemented or had plans to implement medication treatment into their practice after the training.
Though additional research is needed now that training requirements for prescribing medication treatment have changed, provider education programs that support medical professionals with practical training on opioid use disorder screening, implementing and maintaining medication treatment in primary care, and managing patients with an emphasis on the brain disease model of addiction might help promote positive perceptions about medication treatment and increase providers’ willingness to provide it in their primary care practices, which can ultimately help expand access to opioid use disorder treatment. Given that this study did not include a control condition, other factors might explain the increase in perceived competence and willingness to prescribe, and future studies that control for potentially influential factors will help clarify the effect of provider training on willingness to prescribe opioid use disorder medication treatment.
For individuals and families seeking recovery: Individuals seeking medication treatment should know that training and education around medication treatment can vary among different primary care providers. Engaging more providers in training might ultimately encourage more doctors to offer medication treatment programs, which could help meet the high demand for opioid use disorder treatment. Individuals are encouraged to speak with their current healthcare providers to identify a primary care practice with a treatment model and provider that works with them to support their treatment and recovery.
For treatment professionals and treatment systems: This study helps us examine new ways to motivate the primary care workforce to provide office-based medication treatment for opioid use disorder, which can help increase patient access to medication treatment. Engaging in ongoing supplemental education that supports practical training on opioid use disorder screening and implementation of medication treatment in primary care might help promote providers’ positive perceptions about opioid use disorder medication treatment and increase their willingness to provide it in their practices. Treatment professionals and systems are encouraged to find training programs that help support startup of medication treatment programs and maintenance of those programs over time, in the context of primary care, to increase providers’ confidence and willingness to prescribe medication treatment. Additional research will help us better identify the best training elements and ideal educational programing to encourage providers to start implementing medication treatment and support their confidence in maintaining such programs within their practices.
For scientists: Additional research, including randomized controlled trials, is needed to extend these findings in different healthcare settings and other states while controlling for potentially confounding factors. Studies are needed to evaluate and reassess this training program’s content, and programs like it, now that DATA waiver training is no longer required. Identification of other factors impacting provider perceptions of medication treatment provision, as well as confidence and willingness to implement medication as well as maintain treatment in primary care practices is also needed. Additional research will help identify provider barriers to medication treatment provision in various healthcare settings, and address barriers by expanding existing training program content and developing novel programs and methods to expand access to medication treatment. Research among providers who are particularly reluctant to prescribe opioid use disorder medication treatment is also needed to determine if training programs like this can be effective in this subset of providers.
For policy makers: Studies like this highlight potential ways to expand access to opioid use disorder medication treatment. This study found that a new 4-hour educational program with practical training that gives providers information on how to implement opioid use disorder medication treatment in their primary care practices may be a useful way to enhance provider confidence, willingness, and actual implementation of medication treatment into their practices. Given that this study was conducted before federal regulations changed around training and buprenorphine prescribing, more research is needed. Additional funding will help identify the best training programs and methods encourage primary care providers to offer medication treatment and support those who ultimately prescribe them. This can ultimately expand access to medication treatment, which is currently needed to better address the opioid epidemic.