Can buprenorphine-equipped ambulances help link overdose survivors to addiction treatment?
Many emergency departments now offer to start opioid overdose survivors on a medication, such as buprenorphine. The majority of overdose survivors, however, refuse hospital transport by ambulance or leave the hospital before treatment can be started. This study examined preliminary outcomes of an innovative model where overdose survivors receive ambulance-based buprenorphine and addiction treatment linkage.
Consistent with rising rates of opioid use disorder, the use of emergency medical services for opioid overdose has increased over the past several years. Patients experiencing an opioid overdose are commonly given the drug naloxone, which reverses an opioid overdose. Despite its benefits, naloxone causes opioid withdrawal and subsequent opioid craving. Starting patients on an opioid agonist medication treatment like buprenorphine can help address this withdrawal and craving, and ongoing treatment reduces risk of subsequent overdose and death.
After a person experiences an opioid overdose, it is best practice to initiate that person on a medication for opioid use disorder (e.g., buprenorphine), manage their withdrawal symptoms, and offer them a path to long-term treatment. However, many people who survive an opioid overdose do not start medication treatment. In an effort to increase medication treatment initiation among overdose survivors, many emergency departments now start patients on opioid use disorder medication (e.g., buprenorphine) after an overdose. Patients often refuse transport to the hospital by emergency medical services after an overdose, or leave the hospital before starting medication treatment. Providing buprenorphine through emergency services outside of the hospital setting may help promote the initiation of medication treatment among overdose survivors, but emergency medical technicians and paramedics are not commonly trained to provide such services.
To evaluate buprenorphine administration in emergency medical settings, this study examined differences in addiction treatment attendance and repeat overdoses among patients who received ambulance-based buprenorphine administration and treatment linkage for an opioid overdose, compared to patients who received standard ambulatory care in the field for an opioid overdose.
HOW WAS THIS STUDY CONDUCTED?
This was a retrospective matched cohort study of electronic medical records among 240 patients who experienced an opioid overdose and received emergency medical services from an advanced life support ambulance in an urban community in New Jersey. All patients received the opioid overdose reversal drug, naloxone, during their ambulance encounter and survived their overdose. One hundred and seventeen patients were seen by an ambulance that was equipped with buprenorphine and 123 patients were seen by an ambulance that was not equipped with buprenorphine.
The researchers examined subsequent addiction treatment engagement and opioid overdoses among patients who had an opioid-related overdose encounter with either a buprenorphine-equipped ambulance or a non-buprenorphine equipped ambulance. Thereafter, the researchers focused only on those individuals receiving services from a buprenorphine-equipped ambulance comparing subsequent treatment and overdose among patients who received buprenorphine and treatment linkage relative to those who did not receive buprenorphine or treatment linkage. They also examined changes in opioid withdrawal among those who received buprenorphine.
All buprenorphine-equipped ambulances were participating in Cooper University Health Care’s new protocol for field-based buprenorphine treatment (i.e., “Buprenorphine Field Initiation of Rescue Treatment by EMS”), which allowed for ambulance-based delivery of on-site buprenorphine to patients who received naloxone and regained full decision-making abilities. These buprenorphine-equipped ambulances were staffed by emergency medical technicians or paramedics, all of whom received opioid use disorder education through lectures, literature review, clinic/field observation, counseling training, and scenario testing.
All overdose patients who encountered one of these ambulances were assessed for buprenorphine treatment. Paramedics discussed the patient assessment with an emergency medical services physician who ultimately determined if on-site buprenorphine treatment was appropriate. Patients with clinically significant withdrawal symptoms (as assessed by the clinical opiate withdrawal scale) and those who had not used opioids for 72 hours prior to the current overdose were eligible for buprenorphine treatment. Patients who were pregnant, under age 18, were unwilling to provide their name / date of birth for follow-up, and/or had used methadone within the past 48 hours were not eligible for buprenorphine treatment. If the physician approved, paramedics administered 16 mg of buprenorphine to the patient, monitored their withdrawal symptoms, and provided patients with a same day or next day appointment at an addiction treatment clinic offering addiction, psychiatry, social work, and counseling services. Paramedics could administer another 8 mg of buprenorphine to patients whose withdrawal symptoms did not subside after the first 16 mg dose.
Non-buprenorphine-equipped ambulances provided standard ambulatory care for Cooper University Health Care. These ambulances did not have buprenorphine-trained paramedics and did not offer on-site buprenorphine initiation or addiction treatment clinic appointments. Ambulance paramedics only offered patients a printed list of outpatient resources.
Data were collected from patients’ electronic medical records, obtained from emergency medical services and local hospitals affiliated with Cooper University Health Care. Outcomes included any visit to an addiction clinic within 30 days of the ambulance encounter and opioid-related overdoses within 24 hours and 7 days of the ambulance encounter. The researchers also evaluated whether or not patients were transported to the emergency department during the ambulance encounter, as well as paramedic-reported withdrawal among patients who received buprenorphine before and after ambulance-based buprenorphine administration. Patients with incomplete electronic health records that would prevent complete follow-up were excluded from the study. Patients seen by buprenorphine-equipped and non-buprenorphine equipped ambulances were matched based on age, sex, race/ethnicity, medical comorbidities, and insurance coverage.
Overall, 1,230 patients were seen by a buprenorphine-equipped ambulance (n=94 received buprenorphine) and 611 patients were seen by a non-buprenorphine-equipped ambulance. The researchers studied a subset of 117 patients who saw a buprenorphine-equipped ambulance and a subset of 123 patients seen by a non-buprenorphine equipped ambulance, who were matched on the demographic and clinical characteristics noted above. The researchers also controlled for demographics and clinical characteristics in their analyses. The majority of patients were Non-Hispanic Black (45%) and White (37%) men (74%) in their 40’s with Medicaid-based insurance (82%). About half of the patients had co-occurring physical health and/or mental health conditions. Of the 117 patients seen by a buprenorphine-equipped ambulance, 74 received buprenorphine and were included in analyses. Among patients who received buprenorphine, 21% received 24 mg of buprenorphine and 79% received 16 mg.
WHAT DID THIS STUDY FIND?
Patients seen by buprenorphine-equipped ambulances are more likely to engage with addiction treatment.
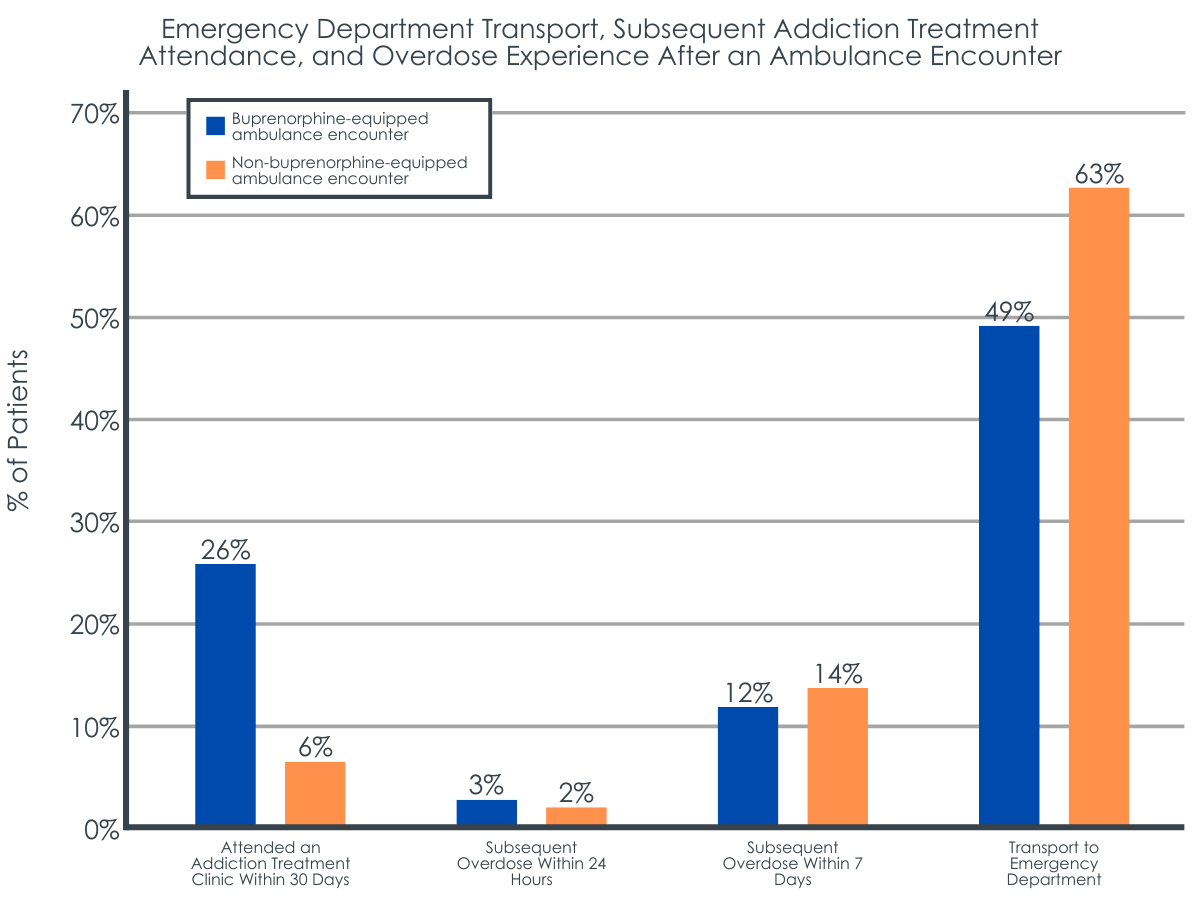
Patients seen by a buprenorphine-equipped ambulance were about 7 times more likely than patients seen by a non-buprenorphine equipped ambulance to visit an addiction treatment clinic at least once within 30 days of their ambulance encounter. Patients seen by a non-buprenorphine equipped ambulance were about 2 times more likely to be transported to the emergency department during their encounter. There were no differences in subsequent overdose rates by ambulance type.
Patients who received buprenorphine are more likely to engage with addiction treatment.
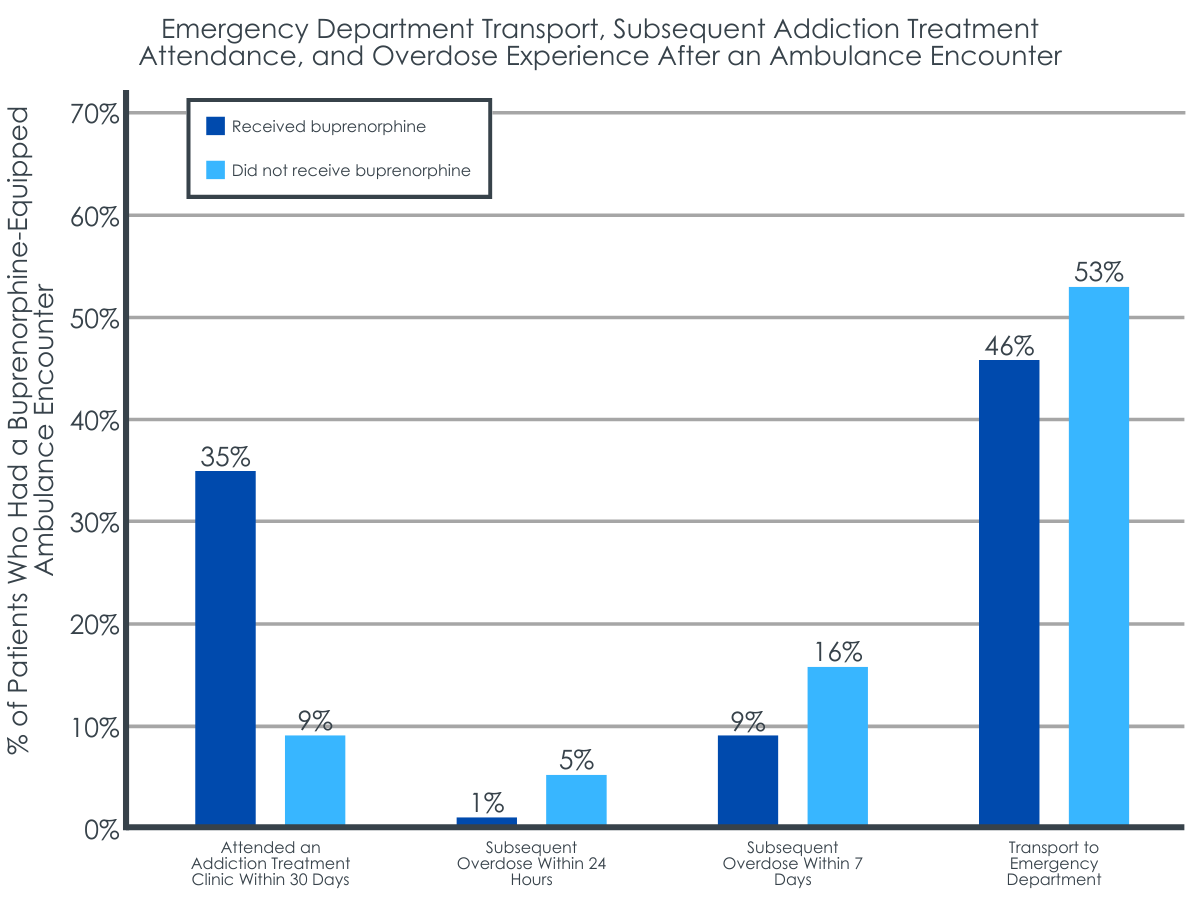
Among only the group of individuals seen by a buprenorphine equipped ambulance, those who received buprenorphine were about 13 times more likely to subsequently attend an addiction treatment clinic compared to those who didn’t receive buprenorphine. There were no differences in the odds of emergency department transport or subsequent overdose by buprenorphine receipt. Among patients who received buprenorphine, withdrawal symptoms decreased 3-fold from pre- to post-buprenorphine administration.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us understand the potential benefits of delivering opioid use disorder medication treatment outside of traditional clinics. This study included a subset of patients seen by a buprenorphine-equipped ambulance. While it is unclear if patients included in this subset had certain demographic and clinical characteristics that may have accounted for the improved outcomes seen here, this study provides a foundation for future research. Additional prospective research among a larger population of patients seen by ambulances across multiple healthcare systems will help to advance our understanding of ambulatory provision of buprenorphine in the field. Despite the relative improvements found here in relation to receiving care from a buprenorphine-equipped ambulance compared to one without buprenorphine on board, approximately 75% of those receiving care from the buprenorphine ambulance still failed to engage with any kind of addiction treatment within 30 days of suffering an opioid overdose. Clearly, there is still a great deal to understand regarding barriers to treatment engagement.
Patients seen by buprenorphine-equipped ambulances for an opioid overdose, as well as patients who received buprenorphine from those ambulances, were more likely to visit an addiction treatment clinic after their ambulance encounter. Prior studies show the benefits of administering and linking patients to opioid use disorder medication treatment (e.g., buprenorphine) when they present to the emergency department with opioid-related problems, including increased engagement in subsequent addiction treatment. However, many patients refuse transport to the hospital after an ambulance encounter for an overdose or leave the hospital before they can be started on a medication. These encounters are missed opportunities to start a patient on medication and link them to longer-term treatment.
This study highlights a model with ambulance-based buprenorphine administration and timely linkage to outpatient addiction treatment to increase patient engagement with treatment after an overdose. Additional research on ambulance-based buprenorphine initiation and linkage to follow-up care will help identify the best model of care for promoting medication treatment initiation and reducing patient risk of subsequent overdose. Importantly, patients included in this study came from a larger group of 1,230 patients seen by a buprenorphine-equipped ambulance, of which, only 94 patients received buprenorphine. It is unclear whether low rates of buprenorphine receipt were due to patient refusal of medication or if buprenorphine was not offered to many patients. Additional research is needed to understand why so few patients received buprenorphine from buprenorphine-equipped ambulances.
Buprenorphine-equipped ambulances were also associated with a reduced likelihood of patient transport to the emergency department. This may reflect the need for hospital visits to address naloxone-induced withdrawal symptoms with medications like buprenorphine among a subset of patients seen by non-buprenorphine-equipped ambulances, which would require transport to the emergency department by these ambulances. However, on-site buprenorphine receipt did not affect the likelihood of emergency department transport among patients seen by buprenorphine-equipped ambulances. Thus, something other than buprenorphine availability may be driving reduced transport of patients among buprenorphine equipped ambulances. For example, perhaps the increased training of buprenorphine-equipped ambulance paramedics influenced procedures for determining which patients required additional follow-up at the hospital. Nonetheless, transport to the emergency department and observation in the hospital for at least two hours are typically suggested after naloxone use to ensure overdose doesn’t recur in the hours following administration once the naloxone wears off. Additional research is needed to examine the reasons for patient refusal of hospital transport and to determine how ambulance-delivered buprenorphine influences patients’ decisions.
Though the odds of patients experiencing a subsequent overdose did not differ by ambulance type, overdose was only investigated 7 days out from the ambulance encounter. Differences might exist outside of this one-week timeframe, at least for those who continued medication treatment as a result of outpatient linkage. Moreover, overdose events were collected from local medical records which would require an ambulance encounter in the local area. Some individuals are not seen by emergency medical services after an overdose that is reversed with naloxone at home, despite medical advice, and transient patients may have been seen by emergency medical services in the surrounding area that were unaccounted for. Thus, overdose events reported here may be an underestimate of the actual number of experienced overdoses. Importantly, buprenorphine is only effective at reducing overdose risk while the medication is onboard. If patients did not receive ongoing buprenorphine treatment through a follow-up clinic visit, they would remain at risk of subsequent overdose.
This study was a retrospective study of medical records, which might underestimate subsequent overdose and treatment rates among patients. It was also conducted in a single urban area of New Jersey with high overdose rates. Findings may not apply to other states or regions with different opioid use disorder populations. The use of other substances (e.g., alcohol, benzodiazepines, etc.) might also influence outcomes and this was not evaluated in the current study.
Statistical matching procedures were conducted to try to equate groups on variables on which they differed as randomization was not used in this study. While this approach can be helpful, it could mean that the groups differed on other variables which were not measured that could have influenced the measured outcomes.
This study only evaluated subsequent overdose events that occurred within 7 days of the ambulance encounter and did not include overdose date from hospitals or emergency services outside of the local hospitals in the area of interest, which might underestimate the number of subsequent overdoses that occurred. Evaluation of subsequent addiction treatment receipt was also limited to medical records within local hospital systems and did not extend beyond 30 days after an ambulance encounter.
BOTTOM LINE
Patients seen by a buprenorphine-equipped ambulance were less likely to be transported to the emergency department during their encounter, and more likely to attend an addiction treatment clinic at least once within 30 days of their ambulance encounter. Individuals who received buprenorphine from a buprenorphine-equipped ambulance had even higher odds of visiting an addiction treatment clinic within 30 days. Neither ambulance type nor buprenorphine receipt affected overdose rates within 24 hours and 7 days of a patient’s ambulance encounter. Also, despite the relative improvement in treatment engagement among the overdose patients who were seen by a buprenorphine equipped ambulance, the majority of this group of patients did not engage with any addiction treatment within the 30-day follow up window. Enhancing our understanding of the barriers to medication treatment provision and linkage in emergency-service settings can ultimately help address high rates of opioid overdose and low rates of treatment utilization among patients who experience opioid overdose.
For individuals and families seeking recovery: It is considered best practice for people to start an agonist medication for opioid use disorder (e.g., buprenorphine) after they have experienced an opioid overdose. These medications can help manage withdrawal symptoms and craving caused by the overdose reversal drug, naloxone. They also help reduce the risk of subsequent overdose and death. Patients who experience an overdose are encouraged to immediately seek ambulatory care and ask their local emergency services about their options for starting medication treatment. If local emergency services cannot assist with medication treatment initiation, patients are encouraged to speak to their primary care providers about starting medication treatment to prevent overdose and aid their path to recovery.
For treatment professionals and treatment systems: Providing opioid overdose patients with a single dose of buprenorphine after naloxone administration and overdose reversal, as well as a same day or next day appointment at an addiction treatment clinic might help link more patients to the treatment they need after an overdose. Treatment professionals and systems are encouraged to speak with local emergency services to identify options for collaboration that promote timely linkage to treatment after an encounter with emergency services. Doing so could help prevent subsequent overdose and increase treatment initiation and engagement among patients with opioid use disorder.
For scientists:Given the novelty of this area of study, it is essential to conduct longitudinal studies of buprenorphine initiation and linkage to longer-term treatment in emergency-medical settings that can limit the potential selection biases present in the current study. Additional research is needed to identify who is more likely to receive buprenorphine in these emergency settings, and to identify whether subsequent overdose and treatment use differ between patients that do and do not attend treatment after referral and linkage. Evaluations of longer-term outcomes (e.g., beyond 1 month) and other emergency medical settings across multiple states, as well as clinical and demographic moderators of successful linkage to treatment are needed to enhance treatment receipt post overdose and reduce overdose occurrence. Studies on the cost-effectiveness of such programs in various states and institutions with different emergency-service delivery and linkage models are also needed.
For policy makers: The delivery of buprenorphine and linkage to longer-term treatment within the context of emergency-medical services can ultimately help address high rates of opioid-related overdose and low rates of treatment seeking after an opioid overdose. Research has begun to examine the effects of buprenorphine delivery in emergency medical settings, but there are few studies examining the effects of these linkage services to patients and institutions. Additional research funding will help identify the full potential of emergency-based delivery of and linkage to opioid use disorder medication treatment, to help address the ongoing opioid-overdose epidemic.
Consistent with rising rates of opioid use disorder, the use of emergency medical services for opioid overdose has increased over the past several years. Patients experiencing an opioid overdose are commonly given the drug naloxone, which reverses an opioid overdose. Despite its benefits, naloxone causes opioid withdrawal and subsequent opioid craving. Starting patients on an opioid agonist medication treatment like buprenorphine can help address this withdrawal and craving, and ongoing treatment reduces risk of subsequent overdose and death.
After a person experiences an opioid overdose, it is best practice to initiate that person on a medication for opioid use disorder (e.g., buprenorphine), manage their withdrawal symptoms, and offer them a path to long-term treatment. However, many people who survive an opioid overdose do not start medication treatment. In an effort to increase medication treatment initiation among overdose survivors, many emergency departments now start patients on opioid use disorder medication (e.g., buprenorphine) after an overdose. Patients often refuse transport to the hospital by emergency medical services after an overdose, or leave the hospital before starting medication treatment. Providing buprenorphine through emergency services outside of the hospital setting may help promote the initiation of medication treatment among overdose survivors, but emergency medical technicians and paramedics are not commonly trained to provide such services.
To evaluate buprenorphine administration in emergency medical settings, this study examined differences in addiction treatment attendance and repeat overdoses among patients who received ambulance-based buprenorphine administration and treatment linkage for an opioid overdose, compared to patients who received standard ambulatory care in the field for an opioid overdose.
HOW WAS THIS STUDY CONDUCTED?
This was a retrospective matched cohort study of electronic medical records among 240 patients who experienced an opioid overdose and received emergency medical services from an advanced life support ambulance in an urban community in New Jersey. All patients received the opioid overdose reversal drug, naloxone, during their ambulance encounter and survived their overdose. One hundred and seventeen patients were seen by an ambulance that was equipped with buprenorphine and 123 patients were seen by an ambulance that was not equipped with buprenorphine.
The researchers examined subsequent addiction treatment engagement and opioid overdoses among patients who had an opioid-related overdose encounter with either a buprenorphine-equipped ambulance or a non-buprenorphine equipped ambulance. Thereafter, the researchers focused only on those individuals receiving services from a buprenorphine-equipped ambulance comparing subsequent treatment and overdose among patients who received buprenorphine and treatment linkage relative to those who did not receive buprenorphine or treatment linkage. They also examined changes in opioid withdrawal among those who received buprenorphine.
All buprenorphine-equipped ambulances were participating in Cooper University Health Care’s new protocol for field-based buprenorphine treatment (i.e., “Buprenorphine Field Initiation of Rescue Treatment by EMS”), which allowed for ambulance-based delivery of on-site buprenorphine to patients who received naloxone and regained full decision-making abilities. These buprenorphine-equipped ambulances were staffed by emergency medical technicians or paramedics, all of whom received opioid use disorder education through lectures, literature review, clinic/field observation, counseling training, and scenario testing.
All overdose patients who encountered one of these ambulances were assessed for buprenorphine treatment. Paramedics discussed the patient assessment with an emergency medical services physician who ultimately determined if on-site buprenorphine treatment was appropriate. Patients with clinically significant withdrawal symptoms (as assessed by the clinical opiate withdrawal scale) and those who had not used opioids for 72 hours prior to the current overdose were eligible for buprenorphine treatment. Patients who were pregnant, under age 18, were unwilling to provide their name / date of birth for follow-up, and/or had used methadone within the past 48 hours were not eligible for buprenorphine treatment. If the physician approved, paramedics administered 16 mg of buprenorphine to the patient, monitored their withdrawal symptoms, and provided patients with a same day or next day appointment at an addiction treatment clinic offering addiction, psychiatry, social work, and counseling services. Paramedics could administer another 8 mg of buprenorphine to patients whose withdrawal symptoms did not subside after the first 16 mg dose.
Non-buprenorphine-equipped ambulances provided standard ambulatory care for Cooper University Health Care. These ambulances did not have buprenorphine-trained paramedics and did not offer on-site buprenorphine initiation or addiction treatment clinic appointments. Ambulance paramedics only offered patients a printed list of outpatient resources.
Data were collected from patients’ electronic medical records, obtained from emergency medical services and local hospitals affiliated with Cooper University Health Care. Outcomes included any visit to an addiction clinic within 30 days of the ambulance encounter and opioid-related overdoses within 24 hours and 7 days of the ambulance encounter. The researchers also evaluated whether or not patients were transported to the emergency department during the ambulance encounter, as well as paramedic-reported withdrawal among patients who received buprenorphine before and after ambulance-based buprenorphine administration. Patients with incomplete electronic health records that would prevent complete follow-up were excluded from the study. Patients seen by buprenorphine-equipped and non-buprenorphine equipped ambulances were matched based on age, sex, race/ethnicity, medical comorbidities, and insurance coverage.
Overall, 1,230 patients were seen by a buprenorphine-equipped ambulance (n=94 received buprenorphine) and 611 patients were seen by a non-buprenorphine-equipped ambulance. The researchers studied a subset of 117 patients who saw a buprenorphine-equipped ambulance and a subset of 123 patients seen by a non-buprenorphine equipped ambulance, who were matched on the demographic and clinical characteristics noted above. The researchers also controlled for demographics and clinical characteristics in their analyses. The majority of patients were Non-Hispanic Black (45%) and White (37%) men (74%) in their 40’s with Medicaid-based insurance (82%). About half of the patients had co-occurring physical health and/or mental health conditions. Of the 117 patients seen by a buprenorphine-equipped ambulance, 74 received buprenorphine and were included in analyses. Among patients who received buprenorphine, 21% received 24 mg of buprenorphine and 79% received 16 mg.
WHAT DID THIS STUDY FIND?
Patients seen by buprenorphine-equipped ambulances are more likely to engage with addiction treatment.
Patients seen by a buprenorphine-equipped ambulance were about 7 times more likely than patients seen by a non-buprenorphine equipped ambulance to visit an addiction treatment clinic at least once within 30 days of their ambulance encounter. Patients seen by a non-buprenorphine equipped ambulance were about 2 times more likely to be transported to the emergency department during their encounter. There were no differences in subsequent overdose rates by ambulance type.
Patients who received buprenorphine are more likely to engage with addiction treatment.
Among only the group of individuals seen by a buprenorphine equipped ambulance, those who received buprenorphine were about 13 times more likely to subsequently attend an addiction treatment clinic compared to those who didn’t receive buprenorphine. There were no differences in the odds of emergency department transport or subsequent overdose by buprenorphine receipt. Among patients who received buprenorphine, withdrawal symptoms decreased 3-fold from pre- to post-buprenorphine administration.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us understand the potential benefits of delivering opioid use disorder medication treatment outside of traditional clinics. This study included a subset of patients seen by a buprenorphine-equipped ambulance. While it is unclear if patients included in this subset had certain demographic and clinical characteristics that may have accounted for the improved outcomes seen here, this study provides a foundation for future research. Additional prospective research among a larger population of patients seen by ambulances across multiple healthcare systems will help to advance our understanding of ambulatory provision of buprenorphine in the field. Despite the relative improvements found here in relation to receiving care from a buprenorphine-equipped ambulance compared to one without buprenorphine on board, approximately 75% of those receiving care from the buprenorphine ambulance still failed to engage with any kind of addiction treatment within 30 days of suffering an opioid overdose. Clearly, there is still a great deal to understand regarding barriers to treatment engagement.
Patients seen by buprenorphine-equipped ambulances for an opioid overdose, as well as patients who received buprenorphine from those ambulances, were more likely to visit an addiction treatment clinic after their ambulance encounter. Prior studies show the benefits of administering and linking patients to opioid use disorder medication treatment (e.g., buprenorphine) when they present to the emergency department with opioid-related problems, including increased engagement in subsequent addiction treatment. However, many patients refuse transport to the hospital after an ambulance encounter for an overdose or leave the hospital before they can be started on a medication. These encounters are missed opportunities to start a patient on medication and link them to longer-term treatment.
This study highlights a model with ambulance-based buprenorphine administration and timely linkage to outpatient addiction treatment to increase patient engagement with treatment after an overdose. Additional research on ambulance-based buprenorphine initiation and linkage to follow-up care will help identify the best model of care for promoting medication treatment initiation and reducing patient risk of subsequent overdose. Importantly, patients included in this study came from a larger group of 1,230 patients seen by a buprenorphine-equipped ambulance, of which, only 94 patients received buprenorphine. It is unclear whether low rates of buprenorphine receipt were due to patient refusal of medication or if buprenorphine was not offered to many patients. Additional research is needed to understand why so few patients received buprenorphine from buprenorphine-equipped ambulances.
Buprenorphine-equipped ambulances were also associated with a reduced likelihood of patient transport to the emergency department. This may reflect the need for hospital visits to address naloxone-induced withdrawal symptoms with medications like buprenorphine among a subset of patients seen by non-buprenorphine-equipped ambulances, which would require transport to the emergency department by these ambulances. However, on-site buprenorphine receipt did not affect the likelihood of emergency department transport among patients seen by buprenorphine-equipped ambulances. Thus, something other than buprenorphine availability may be driving reduced transport of patients among buprenorphine equipped ambulances. For example, perhaps the increased training of buprenorphine-equipped ambulance paramedics influenced procedures for determining which patients required additional follow-up at the hospital. Nonetheless, transport to the emergency department and observation in the hospital for at least two hours are typically suggested after naloxone use to ensure overdose doesn’t recur in the hours following administration once the naloxone wears off. Additional research is needed to examine the reasons for patient refusal of hospital transport and to determine how ambulance-delivered buprenorphine influences patients’ decisions.
Though the odds of patients experiencing a subsequent overdose did not differ by ambulance type, overdose was only investigated 7 days out from the ambulance encounter. Differences might exist outside of this one-week timeframe, at least for those who continued medication treatment as a result of outpatient linkage. Moreover, overdose events were collected from local medical records which would require an ambulance encounter in the local area. Some individuals are not seen by emergency medical services after an overdose that is reversed with naloxone at home, despite medical advice, and transient patients may have been seen by emergency medical services in the surrounding area that were unaccounted for. Thus, overdose events reported here may be an underestimate of the actual number of experienced overdoses. Importantly, buprenorphine is only effective at reducing overdose risk while the medication is onboard. If patients did not receive ongoing buprenorphine treatment through a follow-up clinic visit, they would remain at risk of subsequent overdose.
This study was a retrospective study of medical records, which might underestimate subsequent overdose and treatment rates among patients. It was also conducted in a single urban area of New Jersey with high overdose rates. Findings may not apply to other states or regions with different opioid use disorder populations. The use of other substances (e.g., alcohol, benzodiazepines, etc.) might also influence outcomes and this was not evaluated in the current study.
Statistical matching procedures were conducted to try to equate groups on variables on which they differed as randomization was not used in this study. While this approach can be helpful, it could mean that the groups differed on other variables which were not measured that could have influenced the measured outcomes.
This study only evaluated subsequent overdose events that occurred within 7 days of the ambulance encounter and did not include overdose date from hospitals or emergency services outside of the local hospitals in the area of interest, which might underestimate the number of subsequent overdoses that occurred. Evaluation of subsequent addiction treatment receipt was also limited to medical records within local hospital systems and did not extend beyond 30 days after an ambulance encounter.
BOTTOM LINE
Patients seen by a buprenorphine-equipped ambulance were less likely to be transported to the emergency department during their encounter, and more likely to attend an addiction treatment clinic at least once within 30 days of their ambulance encounter. Individuals who received buprenorphine from a buprenorphine-equipped ambulance had even higher odds of visiting an addiction treatment clinic within 30 days. Neither ambulance type nor buprenorphine receipt affected overdose rates within 24 hours and 7 days of a patient’s ambulance encounter. Also, despite the relative improvement in treatment engagement among the overdose patients who were seen by a buprenorphine equipped ambulance, the majority of this group of patients did not engage with any addiction treatment within the 30-day follow up window. Enhancing our understanding of the barriers to medication treatment provision and linkage in emergency-service settings can ultimately help address high rates of opioid overdose and low rates of treatment utilization among patients who experience opioid overdose.
For individuals and families seeking recovery: It is considered best practice for people to start an agonist medication for opioid use disorder (e.g., buprenorphine) after they have experienced an opioid overdose. These medications can help manage withdrawal symptoms and craving caused by the overdose reversal drug, naloxone. They also help reduce the risk of subsequent overdose and death. Patients who experience an overdose are encouraged to immediately seek ambulatory care and ask their local emergency services about their options for starting medication treatment. If local emergency services cannot assist with medication treatment initiation, patients are encouraged to speak to their primary care providers about starting medication treatment to prevent overdose and aid their path to recovery.
For treatment professionals and treatment systems: Providing opioid overdose patients with a single dose of buprenorphine after naloxone administration and overdose reversal, as well as a same day or next day appointment at an addiction treatment clinic might help link more patients to the treatment they need after an overdose. Treatment professionals and systems are encouraged to speak with local emergency services to identify options for collaboration that promote timely linkage to treatment after an encounter with emergency services. Doing so could help prevent subsequent overdose and increase treatment initiation and engagement among patients with opioid use disorder.
For scientists:Given the novelty of this area of study, it is essential to conduct longitudinal studies of buprenorphine initiation and linkage to longer-term treatment in emergency-medical settings that can limit the potential selection biases present in the current study. Additional research is needed to identify who is more likely to receive buprenorphine in these emergency settings, and to identify whether subsequent overdose and treatment use differ between patients that do and do not attend treatment after referral and linkage. Evaluations of longer-term outcomes (e.g., beyond 1 month) and other emergency medical settings across multiple states, as well as clinical and demographic moderators of successful linkage to treatment are needed to enhance treatment receipt post overdose and reduce overdose occurrence. Studies on the cost-effectiveness of such programs in various states and institutions with different emergency-service delivery and linkage models are also needed.
For policy makers: The delivery of buprenorphine and linkage to longer-term treatment within the context of emergency-medical services can ultimately help address high rates of opioid-related overdose and low rates of treatment seeking after an opioid overdose. Research has begun to examine the effects of buprenorphine delivery in emergency medical settings, but there are few studies examining the effects of these linkage services to patients and institutions. Additional research funding will help identify the full potential of emergency-based delivery of and linkage to opioid use disorder medication treatment, to help address the ongoing opioid-overdose epidemic.
Consistent with rising rates of opioid use disorder, the use of emergency medical services for opioid overdose has increased over the past several years. Patients experiencing an opioid overdose are commonly given the drug naloxone, which reverses an opioid overdose. Despite its benefits, naloxone causes opioid withdrawal and subsequent opioid craving. Starting patients on an opioid agonist medication treatment like buprenorphine can help address this withdrawal and craving, and ongoing treatment reduces risk of subsequent overdose and death.
After a person experiences an opioid overdose, it is best practice to initiate that person on a medication for opioid use disorder (e.g., buprenorphine), manage their withdrawal symptoms, and offer them a path to long-term treatment. However, many people who survive an opioid overdose do not start medication treatment. In an effort to increase medication treatment initiation among overdose survivors, many emergency departments now start patients on opioid use disorder medication (e.g., buprenorphine) after an overdose. Patients often refuse transport to the hospital by emergency medical services after an overdose, or leave the hospital before starting medication treatment. Providing buprenorphine through emergency services outside of the hospital setting may help promote the initiation of medication treatment among overdose survivors, but emergency medical technicians and paramedics are not commonly trained to provide such services.
To evaluate buprenorphine administration in emergency medical settings, this study examined differences in addiction treatment attendance and repeat overdoses among patients who received ambulance-based buprenorphine administration and treatment linkage for an opioid overdose, compared to patients who received standard ambulatory care in the field for an opioid overdose.
HOW WAS THIS STUDY CONDUCTED?
This was a retrospective matched cohort study of electronic medical records among 240 patients who experienced an opioid overdose and received emergency medical services from an advanced life support ambulance in an urban community in New Jersey. All patients received the opioid overdose reversal drug, naloxone, during their ambulance encounter and survived their overdose. One hundred and seventeen patients were seen by an ambulance that was equipped with buprenorphine and 123 patients were seen by an ambulance that was not equipped with buprenorphine.
The researchers examined subsequent addiction treatment engagement and opioid overdoses among patients who had an opioid-related overdose encounter with either a buprenorphine-equipped ambulance or a non-buprenorphine equipped ambulance. Thereafter, the researchers focused only on those individuals receiving services from a buprenorphine-equipped ambulance comparing subsequent treatment and overdose among patients who received buprenorphine and treatment linkage relative to those who did not receive buprenorphine or treatment linkage. They also examined changes in opioid withdrawal among those who received buprenorphine.
All buprenorphine-equipped ambulances were participating in Cooper University Health Care’s new protocol for field-based buprenorphine treatment (i.e., “Buprenorphine Field Initiation of Rescue Treatment by EMS”), which allowed for ambulance-based delivery of on-site buprenorphine to patients who received naloxone and regained full decision-making abilities. These buprenorphine-equipped ambulances were staffed by emergency medical technicians or paramedics, all of whom received opioid use disorder education through lectures, literature review, clinic/field observation, counseling training, and scenario testing.
All overdose patients who encountered one of these ambulances were assessed for buprenorphine treatment. Paramedics discussed the patient assessment with an emergency medical services physician who ultimately determined if on-site buprenorphine treatment was appropriate. Patients with clinically significant withdrawal symptoms (as assessed by the clinical opiate withdrawal scale) and those who had not used opioids for 72 hours prior to the current overdose were eligible for buprenorphine treatment. Patients who were pregnant, under age 18, were unwilling to provide their name / date of birth for follow-up, and/or had used methadone within the past 48 hours were not eligible for buprenorphine treatment. If the physician approved, paramedics administered 16 mg of buprenorphine to the patient, monitored their withdrawal symptoms, and provided patients with a same day or next day appointment at an addiction treatment clinic offering addiction, psychiatry, social work, and counseling services. Paramedics could administer another 8 mg of buprenorphine to patients whose withdrawal symptoms did not subside after the first 16 mg dose.
Non-buprenorphine-equipped ambulances provided standard ambulatory care for Cooper University Health Care. These ambulances did not have buprenorphine-trained paramedics and did not offer on-site buprenorphine initiation or addiction treatment clinic appointments. Ambulance paramedics only offered patients a printed list of outpatient resources.
Data were collected from patients’ electronic medical records, obtained from emergency medical services and local hospitals affiliated with Cooper University Health Care. Outcomes included any visit to an addiction clinic within 30 days of the ambulance encounter and opioid-related overdoses within 24 hours and 7 days of the ambulance encounter. The researchers also evaluated whether or not patients were transported to the emergency department during the ambulance encounter, as well as paramedic-reported withdrawal among patients who received buprenorphine before and after ambulance-based buprenorphine administration. Patients with incomplete electronic health records that would prevent complete follow-up were excluded from the study. Patients seen by buprenorphine-equipped and non-buprenorphine equipped ambulances were matched based on age, sex, race/ethnicity, medical comorbidities, and insurance coverage.
Overall, 1,230 patients were seen by a buprenorphine-equipped ambulance (n=94 received buprenorphine) and 611 patients were seen by a non-buprenorphine-equipped ambulance. The researchers studied a subset of 117 patients who saw a buprenorphine-equipped ambulance and a subset of 123 patients seen by a non-buprenorphine equipped ambulance, who were matched on the demographic and clinical characteristics noted above. The researchers also controlled for demographics and clinical characteristics in their analyses. The majority of patients were Non-Hispanic Black (45%) and White (37%) men (74%) in their 40’s with Medicaid-based insurance (82%). About half of the patients had co-occurring physical health and/or mental health conditions. Of the 117 patients seen by a buprenorphine-equipped ambulance, 74 received buprenorphine and were included in analyses. Among patients who received buprenorphine, 21% received 24 mg of buprenorphine and 79% received 16 mg.
WHAT DID THIS STUDY FIND?
Patients seen by buprenorphine-equipped ambulances are more likely to engage with addiction treatment.
Patients seen by a buprenorphine-equipped ambulance were about 7 times more likely than patients seen by a non-buprenorphine equipped ambulance to visit an addiction treatment clinic at least once within 30 days of their ambulance encounter. Patients seen by a non-buprenorphine equipped ambulance were about 2 times more likely to be transported to the emergency department during their encounter. There were no differences in subsequent overdose rates by ambulance type.
Patients who received buprenorphine are more likely to engage with addiction treatment.
Among only the group of individuals seen by a buprenorphine equipped ambulance, those who received buprenorphine were about 13 times more likely to subsequently attend an addiction treatment clinic compared to those who didn’t receive buprenorphine. There were no differences in the odds of emergency department transport or subsequent overdose by buprenorphine receipt. Among patients who received buprenorphine, withdrawal symptoms decreased 3-fold from pre- to post-buprenorphine administration.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us understand the potential benefits of delivering opioid use disorder medication treatment outside of traditional clinics. This study included a subset of patients seen by a buprenorphine-equipped ambulance. While it is unclear if patients included in this subset had certain demographic and clinical characteristics that may have accounted for the improved outcomes seen here, this study provides a foundation for future research. Additional prospective research among a larger population of patients seen by ambulances across multiple healthcare systems will help to advance our understanding of ambulatory provision of buprenorphine in the field. Despite the relative improvements found here in relation to receiving care from a buprenorphine-equipped ambulance compared to one without buprenorphine on board, approximately 75% of those receiving care from the buprenorphine ambulance still failed to engage with any kind of addiction treatment within 30 days of suffering an opioid overdose. Clearly, there is still a great deal to understand regarding barriers to treatment engagement.
Patients seen by buprenorphine-equipped ambulances for an opioid overdose, as well as patients who received buprenorphine from those ambulances, were more likely to visit an addiction treatment clinic after their ambulance encounter. Prior studies show the benefits of administering and linking patients to opioid use disorder medication treatment (e.g., buprenorphine) when they present to the emergency department with opioid-related problems, including increased engagement in subsequent addiction treatment. However, many patients refuse transport to the hospital after an ambulance encounter for an overdose or leave the hospital before they can be started on a medication. These encounters are missed opportunities to start a patient on medication and link them to longer-term treatment.
This study highlights a model with ambulance-based buprenorphine administration and timely linkage to outpatient addiction treatment to increase patient engagement with treatment after an overdose. Additional research on ambulance-based buprenorphine initiation and linkage to follow-up care will help identify the best model of care for promoting medication treatment initiation and reducing patient risk of subsequent overdose. Importantly, patients included in this study came from a larger group of 1,230 patients seen by a buprenorphine-equipped ambulance, of which, only 94 patients received buprenorphine. It is unclear whether low rates of buprenorphine receipt were due to patient refusal of medication or if buprenorphine was not offered to many patients. Additional research is needed to understand why so few patients received buprenorphine from buprenorphine-equipped ambulances.
Buprenorphine-equipped ambulances were also associated with a reduced likelihood of patient transport to the emergency department. This may reflect the need for hospital visits to address naloxone-induced withdrawal symptoms with medications like buprenorphine among a subset of patients seen by non-buprenorphine-equipped ambulances, which would require transport to the emergency department by these ambulances. However, on-site buprenorphine receipt did not affect the likelihood of emergency department transport among patients seen by buprenorphine-equipped ambulances. Thus, something other than buprenorphine availability may be driving reduced transport of patients among buprenorphine equipped ambulances. For example, perhaps the increased training of buprenorphine-equipped ambulance paramedics influenced procedures for determining which patients required additional follow-up at the hospital. Nonetheless, transport to the emergency department and observation in the hospital for at least two hours are typically suggested after naloxone use to ensure overdose doesn’t recur in the hours following administration once the naloxone wears off. Additional research is needed to examine the reasons for patient refusal of hospital transport and to determine how ambulance-delivered buprenorphine influences patients’ decisions.
Though the odds of patients experiencing a subsequent overdose did not differ by ambulance type, overdose was only investigated 7 days out from the ambulance encounter. Differences might exist outside of this one-week timeframe, at least for those who continued medication treatment as a result of outpatient linkage. Moreover, overdose events were collected from local medical records which would require an ambulance encounter in the local area. Some individuals are not seen by emergency medical services after an overdose that is reversed with naloxone at home, despite medical advice, and transient patients may have been seen by emergency medical services in the surrounding area that were unaccounted for. Thus, overdose events reported here may be an underestimate of the actual number of experienced overdoses. Importantly, buprenorphine is only effective at reducing overdose risk while the medication is onboard. If patients did not receive ongoing buprenorphine treatment through a follow-up clinic visit, they would remain at risk of subsequent overdose.
This study was a retrospective study of medical records, which might underestimate subsequent overdose and treatment rates among patients. It was also conducted in a single urban area of New Jersey with high overdose rates. Findings may not apply to other states or regions with different opioid use disorder populations. The use of other substances (e.g., alcohol, benzodiazepines, etc.) might also influence outcomes and this was not evaluated in the current study.
Statistical matching procedures were conducted to try to equate groups on variables on which they differed as randomization was not used in this study. While this approach can be helpful, it could mean that the groups differed on other variables which were not measured that could have influenced the measured outcomes.
This study only evaluated subsequent overdose events that occurred within 7 days of the ambulance encounter and did not include overdose date from hospitals or emergency services outside of the local hospitals in the area of interest, which might underestimate the number of subsequent overdoses that occurred. Evaluation of subsequent addiction treatment receipt was also limited to medical records within local hospital systems and did not extend beyond 30 days after an ambulance encounter.
BOTTOM LINE
Patients seen by a buprenorphine-equipped ambulance were less likely to be transported to the emergency department during their encounter, and more likely to attend an addiction treatment clinic at least once within 30 days of their ambulance encounter. Individuals who received buprenorphine from a buprenorphine-equipped ambulance had even higher odds of visiting an addiction treatment clinic within 30 days. Neither ambulance type nor buprenorphine receipt affected overdose rates within 24 hours and 7 days of a patient’s ambulance encounter. Also, despite the relative improvement in treatment engagement among the overdose patients who were seen by a buprenorphine equipped ambulance, the majority of this group of patients did not engage with any addiction treatment within the 30-day follow up window. Enhancing our understanding of the barriers to medication treatment provision and linkage in emergency-service settings can ultimately help address high rates of opioid overdose and low rates of treatment utilization among patients who experience opioid overdose.
For individuals and families seeking recovery: It is considered best practice for people to start an agonist medication for opioid use disorder (e.g., buprenorphine) after they have experienced an opioid overdose. These medications can help manage withdrawal symptoms and craving caused by the overdose reversal drug, naloxone. They also help reduce the risk of subsequent overdose and death. Patients who experience an overdose are encouraged to immediately seek ambulatory care and ask their local emergency services about their options for starting medication treatment. If local emergency services cannot assist with medication treatment initiation, patients are encouraged to speak to their primary care providers about starting medication treatment to prevent overdose and aid their path to recovery.
For treatment professionals and treatment systems: Providing opioid overdose patients with a single dose of buprenorphine after naloxone administration and overdose reversal, as well as a same day or next day appointment at an addiction treatment clinic might help link more patients to the treatment they need after an overdose. Treatment professionals and systems are encouraged to speak with local emergency services to identify options for collaboration that promote timely linkage to treatment after an encounter with emergency services. Doing so could help prevent subsequent overdose and increase treatment initiation and engagement among patients with opioid use disorder.
For scientists:Given the novelty of this area of study, it is essential to conduct longitudinal studies of buprenorphine initiation and linkage to longer-term treatment in emergency-medical settings that can limit the potential selection biases present in the current study. Additional research is needed to identify who is more likely to receive buprenorphine in these emergency settings, and to identify whether subsequent overdose and treatment use differ between patients that do and do not attend treatment after referral and linkage. Evaluations of longer-term outcomes (e.g., beyond 1 month) and other emergency medical settings across multiple states, as well as clinical and demographic moderators of successful linkage to treatment are needed to enhance treatment receipt post overdose and reduce overdose occurrence. Studies on the cost-effectiveness of such programs in various states and institutions with different emergency-service delivery and linkage models are also needed.
For policy makers: The delivery of buprenorphine and linkage to longer-term treatment within the context of emergency-medical services can ultimately help address high rates of opioid-related overdose and low rates of treatment seeking after an opioid overdose. Research has begun to examine the effects of buprenorphine delivery in emergency medical settings, but there are few studies examining the effects of these linkage services to patients and institutions. Additional research funding will help identify the full potential of emergency-based delivery of and linkage to opioid use disorder medication treatment, to help address the ongoing opioid-overdose epidemic.