Black patients less likely to get buprenorphine during opioid-related emergency visits
Reduced access to healthcare may explain why Black and Hispanic individuals have increasingly higher rates of opioid overdose than White individuals. As part of a real-world trial that used a clinical decision support tool in the emergency department to initiate buprenorphine in patients with opioid use disorder, this study investigated if racial/ethnic minorities were prescribed buprenorphine at lower rates than White patients.
This previous research, however, has often been unidimensional – focusing on the trends at a single hospital/site. Research examining buprenorphine in the ED across multiple hospitals in different geographical areas can help increase the chances that the research will inform practice and policy across the US (i.e., generalizability). The current study examined differences in ED buprenorphine administration by race and ethnicity across 21 hospitals in various parts of the US. The researchers also examined how hospital affiliation impacted the relationship between race/ethnicity and buprenorphine prescription.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis focused on potential racial/ethnic disparities from a pragmatic cluster randomized controlled trial, where some EDs were intervention sites and others were comparison sites. The original study tested if a user–centered clinical decision support tool helped increase buprenorphine prescription and onsite initiation for ED patients with opioid use disorder.
Patients included in the analyses (N=5047) were 18+ years of age who presented to one of 21 EDs with an opioid use disorder-related issue (e.g., opioid overdose). Patients were not included in the analyses if they were already receiving opioid use disorder medications prior to their first ED visit (e.g., methadone), if they were admitted to the hospital or an inpatient psychiatric unit after the ED visit, pregnant, or if they died while in the ED. Hospitals participating in the trial came from 5 states (Alabama, Colorado, Connecticut, Massachusetts, and North Carolina), with 3-5 emergency departments per health system. All data were collected between November 2019 and May 2021.
Data for the study were collected from the electronic health record databases of each healthcare system and combined for analysis. Variables controlled for in analyses included patients’ age, gender, and opioid-related ED discharge diagnoses (e.g., opioid overdose). How patients’ race/ethnicity was recorded varied across sites – some collected these data at ED intake while others pulled these data from previous hospitalization records. ED clinician variables controlled for in analyses included X-waiver status* of the treating clinician (not waivered, waivered before the start of the study, waivered after the start of the study). Hospital variables controlled for in analyses included the hospital’s affiliation (Community, Academic), urbanicity (rural, suburban, urban), and annual volume of patients with an opioid use disorder.
The primary outcome was the proportion of participants who received buprenorphine at their first ED visit. This was defined as either getting buprenorphine while in the ED or as a discharge prescription. All formulations of buprenorphine and buprenorphine/naloxone were included (e.g., sublingual tablets, transdermal patches, intravenous injections, etc.). The researchers also examined the association between hospital type (academic cs. community) and ED buprenorphine administration across race/ethnicity.
Patients included in the sample consisted mostly of male identified (65.7%) White (71.6%) non-Hispanic (81.2%) people with a median age of 36.0 years. Physicians attending these patients were predominantly male identified (67.0%) people who were between 35-44 years old (39.3%), most of whom had not received X waiver training before the study began (55.3%). No other physician demographic data were presented by the authors.
*An X-Waiver registration was certification physicians were required to attain before they could prescribe buprenorphine for opioid use disorder. As of December 29, 2022, this requirement has been eliminated- physicians can currently prescribe buprenorphine without X-Waiver certification.
WHAT DID THIS STUDY FIND?
Black patients were less likely to receive buprenorphine than White patients.
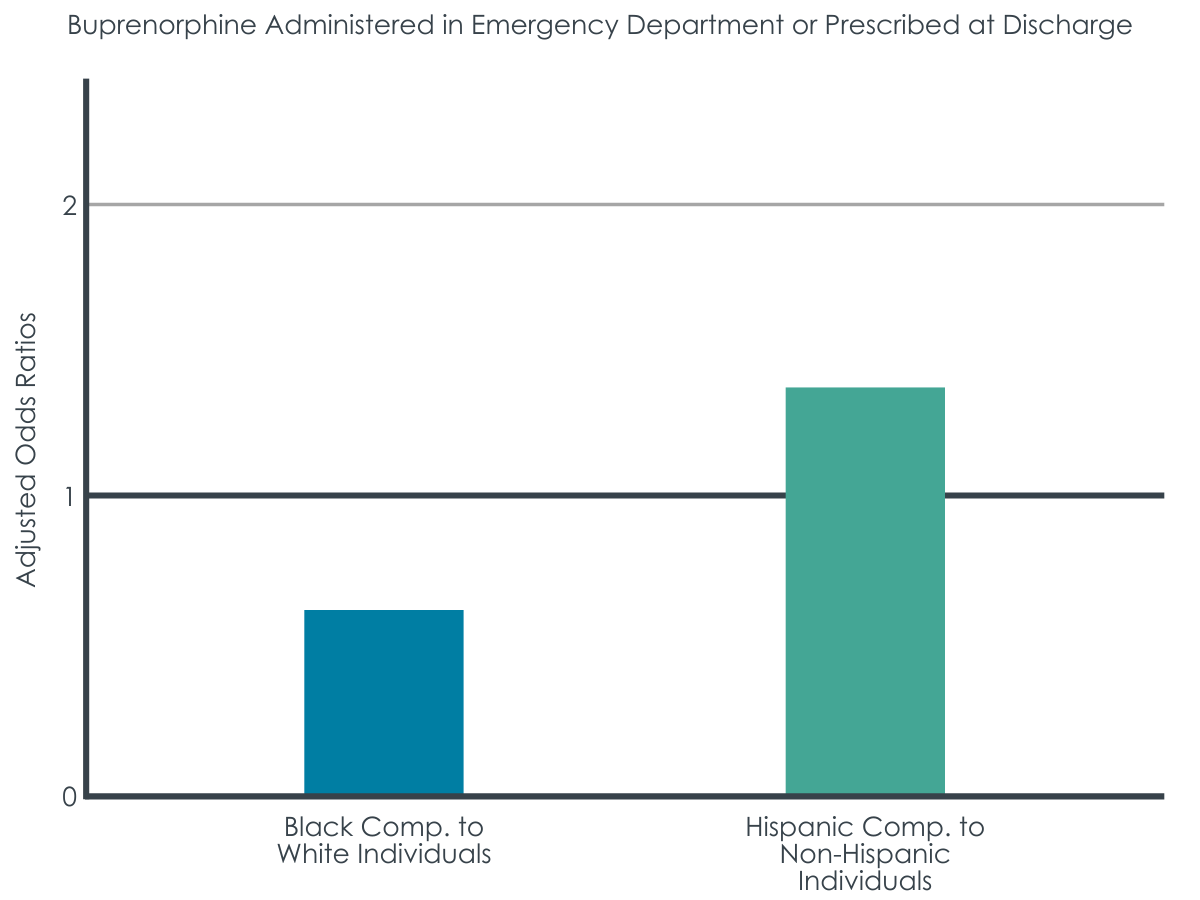
The odds of a Black patient being prescribed buprenorphine were nearly 40% lower than those of a White patient. This association persisted after adjusting for participant level (e.g., age, and gender), clinician level (X-waiver status) and hospital level factors (e.g., hospital type [academic vs. community] and urbanicity [urban vs. rural]).
Figure 1. Odds ratios (ORs) indicate the likelihood (the “odds”) of an outcome, in this case the likelihood to receive buprenorphine in the emergency department or at discharge. ORs less than 1 indicate a negative association, while ORs greater than 1 indicate a positive association, so this figure indicates that Black individuals are less likely to receive buprenorphine than White individuals, while Hispanic individuals are more likely to receive buprenorphine than non-Hispanic individuals.
Hispanic patients were more likely to receive buprenorphine than non-Hispanic patients.
The odds of a Hispanic patient being prescribed buprenorphine were over 30% higher than those of a White patient. This relationship between ethnicity and buprenorphine prescription persisted when adjusting for patient, physician and hospital level factors that may impact buprenorphine prescription (e.g., physician X-waiver status and hospital urbanicity respectively).
Differences by race/ethnicity were no longer present after adjusting for clinical diagnosis.
When statistical models adjusted for diagnoses in each patient’s chart corresponding with the ED service received (e.g., opioid withdrawal), the researchers found that Black and Hispanic patients were prescribed buprenorphine at similar rates to White and non-Hispanic patients, respectively.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Before taking into account discharge diagnoses, the researchers found differences in rates of buprenorphine prescription between Black/Hispanic and White ED patients. Black patients presenting with opioid use disorder related medical consequences (e.g., overdose) were less likely to receive buprenorphine relative to White patients. In contrast, Hispanic patients were more likely to receive buprenorphine compared to non-Hispanic patients. However, the researchers also found that when adjusting for discharge diagnosis of opioid related problems (e.g., opioid withdrawal) these differences disappeared. This suggests that clinical decisions at the diagnosis stage of the ED visit may be responsible for the previously observed prescription discrepancies.
It is unclear what may be influencing decisions during the diagnostic process. One explanation may be that systemic biases impact the provider-patient relationship and therefore result in different diagnoses. Clinicians’ biases may result in ED providers interacting with Black patients, for example, differently than they would with White patients. Subsequently, clinicians would be less likely to detect, or adequately assess for, opioid use disorder and/or opioid withdrawal resulting in lower buprenorphine prescriptions for Black people. While Black patients were descriptively less likely to be diagnosed with opioid withdrawal than White patients (18 vs. 12%), and analyses suggest this difference accounted, in part, for lower buprenorphine prescription rates, the study cannot explain why this is the case. It is possible clinicians are not appropriately assessing for withdrawal symptoms in Black patients or that Black patients are underreporting withdrawal symptoms (e.g., due to medical mistrust). While future research is needed to understand why Black patients are less likely to receive buprenorphine, to inform practice and policy changes, the researchers’ previously published analyses partially support the explanation that clinical judgment accounts for the disparity at least in part. Specifically, Black patients at study sites randomized to the clinical decision software condition were more likely to receive buprenorphine than in control sites. That is, the software helped providers make treatment recommendations (e.g., buprenorphine prescription) based on patients’ symptoms independent of race/ethnicity.
In contrast, the researchers also found that Hispanic patients were more likely to receive buprenorphine relative to non-Hispanic patients. This is surprising given past research suggesting Hispanic patients are less likely on average to receive buprenorphine. This unexpected finding may be due to one ED in the study with a large number of Hispanic patients. This ED had a buprenorphine administration rate of nearly 40%- well above every other site. Given that this hospital served a large number of Hispanic patients, it is possible the clinicians did not hold anti-Hispanic biases through working frequently with non-majority ethnicity patients and/or because they also identified as Hispanic. While potentially very useful if true, this explanation for higher buprenorphine prescribing rates for Hispanic individuals should be tested in future research before conclusions can be drawn.
The research team does not describe if the experimental condition was included in the statistical models. This may explain why the finding that racial/ethnic minorities were prescribed buprenorphine at similar rates when adjusting for diagnosis. That is, the intervention was designed to remove bias from diagnosis via a computer program which gave a diagnosis based on the patients’ medical records and symptoms. If diagnosis is a proxy of the intervention, it may mean that the intervention was successful- it made buprenorphine prescription more equitable. On the other hand, the already published results of the clinical trial suggests that there was no difference in buprenorphine prescriptions between conditions.These contradictory findings from the same dataset makes it difficult to draw conclusions about what is accounting for the observed differences in opioid use disorder prescriptions.
Most of the study took place during the COVID-19 pandemic (November2019– May 2021). It is very likely that this impacted the findings in some way. For instance, the added stress of the pandemic may have led people with an opioid use disorder to increase their opioid use and subsequently increased rates of ED visits for opioid use disorder related problems. Such an increase may have differentially impacted EDs serving racial/ethnic minorities, since EDs are a critical source of healthcare for these populations.Thismay have led to an influx of more Black/Hispanic patients seeking care at EDs during this time (e.g., for COVID infections). Subsequently, this could have impacted ED clinicians’ triage practices, and potentially resulted in differential treatment of patients with an opioid use disorder across racial/ethnic lines.
BOTTOM LINE
This study found that Black patients who presented with opioid use disorder symptoms at EDs were less likely to be administered or prescribed buprenorphine compared to White patients. Hispanic patients, on the other hand, were more likely to be given buprenorphine relative to non-Hispanic patients, likely explained by one large Hispanic-serving hospital. Given that these differences were no longer present when controlling for diagnosis, it is possible that systemic biases were impacting the provider-patient relationship, ultimately resulting in underdiagnosis of opioid withdrawal, specifically, and lower likelihood of buprenorphine prescription. There remains a pressing need to develop strategies to address buprenorphine access disparities among racial/ethnic minorities in the US.
For individuals and families seeking recovery: The present research does not provide data on reasons for disparities in buprenorphine prescription, nor does it describe barriers to opioid use disorder treatment faced by racial/ethnic minorities in the US. This makes it difficult to make recommendations for those seeking opioid use disorder treatment. However, the present research does suggest the diagnosis stage of the patient-provider interaction may be a contributor to this treatment disparity. Therefore, those interested in buprenorphine treatment for themselves/others may need to be especially mindful when interacting with clinicians. To ensure they receive necessary opioid use disorder treatment, those seeking care may need to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: It is unknown why sampled Black/Hispanic patients received buprenorphine at differing rates from White/non-Hispanic ED patients, respectively. Nor is it known why these relationships were no longer present when adjusting for patient diagnoses. One possible explanation could be that clinicians’ biases impacted the ways in which they interacted with Black/Hispanic patients. Those providing treatment to and/or work in healthcare system settings serving racial/ethnic minorities may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs. Another option could be for clinicians to utilizeresources to address bias for health professionals.
For policy makers: This study suggests that Black/Hispanic patients who show signs of OUD and related withdrawal and thus could benefit from buprenorphinemaynot be getting it when they present for care at EDs.This may be due in part to these populations having fewer options for where they receive healthcare. One of the farthest-reaching policies would be to increase healthcare access- that is to increase public clinics which serve racial/ethnic minorities. Separate from the critical need of increased healthcare access,it may be helpful for policymakers to create guidelines to increase opioid use disorder screening among all ED patients. That is, this increase in screening may result in more patients with opioid use disorder being identified and referred to treatment who would otherwise not be.
This previous research, however, has often been unidimensional – focusing on the trends at a single hospital/site. Research examining buprenorphine in the ED across multiple hospitals in different geographical areas can help increase the chances that the research will inform practice and policy across the US (i.e., generalizability). The current study examined differences in ED buprenorphine administration by race and ethnicity across 21 hospitals in various parts of the US. The researchers also examined how hospital affiliation impacted the relationship between race/ethnicity and buprenorphine prescription.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis focused on potential racial/ethnic disparities from a pragmatic cluster randomized controlled trial, where some EDs were intervention sites and others were comparison sites. The original study tested if a user–centered clinical decision support tool helped increase buprenorphine prescription and onsite initiation for ED patients with opioid use disorder.
Patients included in the analyses (N=5047) were 18+ years of age who presented to one of 21 EDs with an opioid use disorder-related issue (e.g., opioid overdose). Patients were not included in the analyses if they were already receiving opioid use disorder medications prior to their first ED visit (e.g., methadone), if they were admitted to the hospital or an inpatient psychiatric unit after the ED visit, pregnant, or if they died while in the ED. Hospitals participating in the trial came from 5 states (Alabama, Colorado, Connecticut, Massachusetts, and North Carolina), with 3-5 emergency departments per health system. All data were collected between November 2019 and May 2021.
Data for the study were collected from the electronic health record databases of each healthcare system and combined for analysis. Variables controlled for in analyses included patients’ age, gender, and opioid-related ED discharge diagnoses (e.g., opioid overdose). How patients’ race/ethnicity was recorded varied across sites – some collected these data at ED intake while others pulled these data from previous hospitalization records. ED clinician variables controlled for in analyses included X-waiver status* of the treating clinician (not waivered, waivered before the start of the study, waivered after the start of the study). Hospital variables controlled for in analyses included the hospital’s affiliation (Community, Academic), urbanicity (rural, suburban, urban), and annual volume of patients with an opioid use disorder.
The primary outcome was the proportion of participants who received buprenorphine at their first ED visit. This was defined as either getting buprenorphine while in the ED or as a discharge prescription. All formulations of buprenorphine and buprenorphine/naloxone were included (e.g., sublingual tablets, transdermal patches, intravenous injections, etc.). The researchers also examined the association between hospital type (academic cs. community) and ED buprenorphine administration across race/ethnicity.
Patients included in the sample consisted mostly of male identified (65.7%) White (71.6%) non-Hispanic (81.2%) people with a median age of 36.0 years. Physicians attending these patients were predominantly male identified (67.0%) people who were between 35-44 years old (39.3%), most of whom had not received X waiver training before the study began (55.3%). No other physician demographic data were presented by the authors.
*An X-Waiver registration was certification physicians were required to attain before they could prescribe buprenorphine for opioid use disorder. As of December 29, 2022, this requirement has been eliminated- physicians can currently prescribe buprenorphine without X-Waiver certification.
WHAT DID THIS STUDY FIND?
Black patients were less likely to receive buprenorphine than White patients.
The odds of a Black patient being prescribed buprenorphine were nearly 40% lower than those of a White patient. This association persisted after adjusting for participant level (e.g., age, and gender), clinician level (X-waiver status) and hospital level factors (e.g., hospital type [academic vs. community] and urbanicity [urban vs. rural]).
Figure 1. Odds ratios (ORs) indicate the likelihood (the “odds”) of an outcome, in this case the likelihood to receive buprenorphine in the emergency department or at discharge. ORs less than 1 indicate a negative association, while ORs greater than 1 indicate a positive association, so this figure indicates that Black individuals are less likely to receive buprenorphine than White individuals, while Hispanic individuals are more likely to receive buprenorphine than non-Hispanic individuals.
Hispanic patients were more likely to receive buprenorphine than non-Hispanic patients.
The odds of a Hispanic patient being prescribed buprenorphine were over 30% higher than those of a White patient. This relationship between ethnicity and buprenorphine prescription persisted when adjusting for patient, physician and hospital level factors that may impact buprenorphine prescription (e.g., physician X-waiver status and hospital urbanicity respectively).
Differences by race/ethnicity were no longer present after adjusting for clinical diagnosis.
When statistical models adjusted for diagnoses in each patient’s chart corresponding with the ED service received (e.g., opioid withdrawal), the researchers found that Black and Hispanic patients were prescribed buprenorphine at similar rates to White and non-Hispanic patients, respectively.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Before taking into account discharge diagnoses, the researchers found differences in rates of buprenorphine prescription between Black/Hispanic and White ED patients. Black patients presenting with opioid use disorder related medical consequences (e.g., overdose) were less likely to receive buprenorphine relative to White patients. In contrast, Hispanic patients were more likely to receive buprenorphine compared to non-Hispanic patients. However, the researchers also found that when adjusting for discharge diagnosis of opioid related problems (e.g., opioid withdrawal) these differences disappeared. This suggests that clinical decisions at the diagnosis stage of the ED visit may be responsible for the previously observed prescription discrepancies.
It is unclear what may be influencing decisions during the diagnostic process. One explanation may be that systemic biases impact the provider-patient relationship and therefore result in different diagnoses. Clinicians’ biases may result in ED providers interacting with Black patients, for example, differently than they would with White patients. Subsequently, clinicians would be less likely to detect, or adequately assess for, opioid use disorder and/or opioid withdrawal resulting in lower buprenorphine prescriptions for Black people. While Black patients were descriptively less likely to be diagnosed with opioid withdrawal than White patients (18 vs. 12%), and analyses suggest this difference accounted, in part, for lower buprenorphine prescription rates, the study cannot explain why this is the case. It is possible clinicians are not appropriately assessing for withdrawal symptoms in Black patients or that Black patients are underreporting withdrawal symptoms (e.g., due to medical mistrust). While future research is needed to understand why Black patients are less likely to receive buprenorphine, to inform practice and policy changes, the researchers’ previously published analyses partially support the explanation that clinical judgment accounts for the disparity at least in part. Specifically, Black patients at study sites randomized to the clinical decision software condition were more likely to receive buprenorphine than in control sites. That is, the software helped providers make treatment recommendations (e.g., buprenorphine prescription) based on patients’ symptoms independent of race/ethnicity.
In contrast, the researchers also found that Hispanic patients were more likely to receive buprenorphine relative to non-Hispanic patients. This is surprising given past research suggesting Hispanic patients are less likely on average to receive buprenorphine. This unexpected finding may be due to one ED in the study with a large number of Hispanic patients. This ED had a buprenorphine administration rate of nearly 40%- well above every other site. Given that this hospital served a large number of Hispanic patients, it is possible the clinicians did not hold anti-Hispanic biases through working frequently with non-majority ethnicity patients and/or because they also identified as Hispanic. While potentially very useful if true, this explanation for higher buprenorphine prescribing rates for Hispanic individuals should be tested in future research before conclusions can be drawn.
The research team does not describe if the experimental condition was included in the statistical models. This may explain why the finding that racial/ethnic minorities were prescribed buprenorphine at similar rates when adjusting for diagnosis. That is, the intervention was designed to remove bias from diagnosis via a computer program which gave a diagnosis based on the patients’ medical records and symptoms. If diagnosis is a proxy of the intervention, it may mean that the intervention was successful- it made buprenorphine prescription more equitable. On the other hand, the already published results of the clinical trial suggests that there was no difference in buprenorphine prescriptions between conditions.These contradictory findings from the same dataset makes it difficult to draw conclusions about what is accounting for the observed differences in opioid use disorder prescriptions.
Most of the study took place during the COVID-19 pandemic (November2019– May 2021). It is very likely that this impacted the findings in some way. For instance, the added stress of the pandemic may have led people with an opioid use disorder to increase their opioid use and subsequently increased rates of ED visits for opioid use disorder related problems. Such an increase may have differentially impacted EDs serving racial/ethnic minorities, since EDs are a critical source of healthcare for these populations.Thismay have led to an influx of more Black/Hispanic patients seeking care at EDs during this time (e.g., for COVID infections). Subsequently, this could have impacted ED clinicians’ triage practices, and potentially resulted in differential treatment of patients with an opioid use disorder across racial/ethnic lines.
BOTTOM LINE
This study found that Black patients who presented with opioid use disorder symptoms at EDs were less likely to be administered or prescribed buprenorphine compared to White patients. Hispanic patients, on the other hand, were more likely to be given buprenorphine relative to non-Hispanic patients, likely explained by one large Hispanic-serving hospital. Given that these differences were no longer present when controlling for diagnosis, it is possible that systemic biases were impacting the provider-patient relationship, ultimately resulting in underdiagnosis of opioid withdrawal, specifically, and lower likelihood of buprenorphine prescription. There remains a pressing need to develop strategies to address buprenorphine access disparities among racial/ethnic minorities in the US.
For individuals and families seeking recovery: The present research does not provide data on reasons for disparities in buprenorphine prescription, nor does it describe barriers to opioid use disorder treatment faced by racial/ethnic minorities in the US. This makes it difficult to make recommendations for those seeking opioid use disorder treatment. However, the present research does suggest the diagnosis stage of the patient-provider interaction may be a contributor to this treatment disparity. Therefore, those interested in buprenorphine treatment for themselves/others may need to be especially mindful when interacting with clinicians. To ensure they receive necessary opioid use disorder treatment, those seeking care may need to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: It is unknown why sampled Black/Hispanic patients received buprenorphine at differing rates from White/non-Hispanic ED patients, respectively. Nor is it known why these relationships were no longer present when adjusting for patient diagnoses. One possible explanation could be that clinicians’ biases impacted the ways in which they interacted with Black/Hispanic patients. Those providing treatment to and/or work in healthcare system settings serving racial/ethnic minorities may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs. Another option could be for clinicians to utilizeresources to address bias for health professionals.
For policy makers: This study suggests that Black/Hispanic patients who show signs of OUD and related withdrawal and thus could benefit from buprenorphinemaynot be getting it when they present for care at EDs.This may be due in part to these populations having fewer options for where they receive healthcare. One of the farthest-reaching policies would be to increase healthcare access- that is to increase public clinics which serve racial/ethnic minorities. Separate from the critical need of increased healthcare access,it may be helpful for policymakers to create guidelines to increase opioid use disorder screening among all ED patients. That is, this increase in screening may result in more patients with opioid use disorder being identified and referred to treatment who would otherwise not be.
This previous research, however, has often been unidimensional – focusing on the trends at a single hospital/site. Research examining buprenorphine in the ED across multiple hospitals in different geographical areas can help increase the chances that the research will inform practice and policy across the US (i.e., generalizability). The current study examined differences in ED buprenorphine administration by race and ethnicity across 21 hospitals in various parts of the US. The researchers also examined how hospital affiliation impacted the relationship between race/ethnicity and buprenorphine prescription.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis focused on potential racial/ethnic disparities from a pragmatic cluster randomized controlled trial, where some EDs were intervention sites and others were comparison sites. The original study tested if a user–centered clinical decision support tool helped increase buprenorphine prescription and onsite initiation for ED patients with opioid use disorder.
Patients included in the analyses (N=5047) were 18+ years of age who presented to one of 21 EDs with an opioid use disorder-related issue (e.g., opioid overdose). Patients were not included in the analyses if they were already receiving opioid use disorder medications prior to their first ED visit (e.g., methadone), if they were admitted to the hospital or an inpatient psychiatric unit after the ED visit, pregnant, or if they died while in the ED. Hospitals participating in the trial came from 5 states (Alabama, Colorado, Connecticut, Massachusetts, and North Carolina), with 3-5 emergency departments per health system. All data were collected between November 2019 and May 2021.
Data for the study were collected from the electronic health record databases of each healthcare system and combined for analysis. Variables controlled for in analyses included patients’ age, gender, and opioid-related ED discharge diagnoses (e.g., opioid overdose). How patients’ race/ethnicity was recorded varied across sites – some collected these data at ED intake while others pulled these data from previous hospitalization records. ED clinician variables controlled for in analyses included X-waiver status* of the treating clinician (not waivered, waivered before the start of the study, waivered after the start of the study). Hospital variables controlled for in analyses included the hospital’s affiliation (Community, Academic), urbanicity (rural, suburban, urban), and annual volume of patients with an opioid use disorder.
The primary outcome was the proportion of participants who received buprenorphine at their first ED visit. This was defined as either getting buprenorphine while in the ED or as a discharge prescription. All formulations of buprenorphine and buprenorphine/naloxone were included (e.g., sublingual tablets, transdermal patches, intravenous injections, etc.). The researchers also examined the association between hospital type (academic cs. community) and ED buprenorphine administration across race/ethnicity.
Patients included in the sample consisted mostly of male identified (65.7%) White (71.6%) non-Hispanic (81.2%) people with a median age of 36.0 years. Physicians attending these patients were predominantly male identified (67.0%) people who were between 35-44 years old (39.3%), most of whom had not received X waiver training before the study began (55.3%). No other physician demographic data were presented by the authors.
*An X-Waiver registration was certification physicians were required to attain before they could prescribe buprenorphine for opioid use disorder. As of December 29, 2022, this requirement has been eliminated- physicians can currently prescribe buprenorphine without X-Waiver certification.
WHAT DID THIS STUDY FIND?
Black patients were less likely to receive buprenorphine than White patients.
The odds of a Black patient being prescribed buprenorphine were nearly 40% lower than those of a White patient. This association persisted after adjusting for participant level (e.g., age, and gender), clinician level (X-waiver status) and hospital level factors (e.g., hospital type [academic vs. community] and urbanicity [urban vs. rural]).
Figure 1. Odds ratios (ORs) indicate the likelihood (the “odds”) of an outcome, in this case the likelihood to receive buprenorphine in the emergency department or at discharge. ORs less than 1 indicate a negative association, while ORs greater than 1 indicate a positive association, so this figure indicates that Black individuals are less likely to receive buprenorphine than White individuals, while Hispanic individuals are more likely to receive buprenorphine than non-Hispanic individuals.
Hispanic patients were more likely to receive buprenorphine than non-Hispanic patients.
The odds of a Hispanic patient being prescribed buprenorphine were over 30% higher than those of a White patient. This relationship between ethnicity and buprenorphine prescription persisted when adjusting for patient, physician and hospital level factors that may impact buprenorphine prescription (e.g., physician X-waiver status and hospital urbanicity respectively).
Differences by race/ethnicity were no longer present after adjusting for clinical diagnosis.
When statistical models adjusted for diagnoses in each patient’s chart corresponding with the ED service received (e.g., opioid withdrawal), the researchers found that Black and Hispanic patients were prescribed buprenorphine at similar rates to White and non-Hispanic patients, respectively.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Before taking into account discharge diagnoses, the researchers found differences in rates of buprenorphine prescription between Black/Hispanic and White ED patients. Black patients presenting with opioid use disorder related medical consequences (e.g., overdose) were less likely to receive buprenorphine relative to White patients. In contrast, Hispanic patients were more likely to receive buprenorphine compared to non-Hispanic patients. However, the researchers also found that when adjusting for discharge diagnosis of opioid related problems (e.g., opioid withdrawal) these differences disappeared. This suggests that clinical decisions at the diagnosis stage of the ED visit may be responsible for the previously observed prescription discrepancies.
It is unclear what may be influencing decisions during the diagnostic process. One explanation may be that systemic biases impact the provider-patient relationship and therefore result in different diagnoses. Clinicians’ biases may result in ED providers interacting with Black patients, for example, differently than they would with White patients. Subsequently, clinicians would be less likely to detect, or adequately assess for, opioid use disorder and/or opioid withdrawal resulting in lower buprenorphine prescriptions for Black people. While Black patients were descriptively less likely to be diagnosed with opioid withdrawal than White patients (18 vs. 12%), and analyses suggest this difference accounted, in part, for lower buprenorphine prescription rates, the study cannot explain why this is the case. It is possible clinicians are not appropriately assessing for withdrawal symptoms in Black patients or that Black patients are underreporting withdrawal symptoms (e.g., due to medical mistrust). While future research is needed to understand why Black patients are less likely to receive buprenorphine, to inform practice and policy changes, the researchers’ previously published analyses partially support the explanation that clinical judgment accounts for the disparity at least in part. Specifically, Black patients at study sites randomized to the clinical decision software condition were more likely to receive buprenorphine than in control sites. That is, the software helped providers make treatment recommendations (e.g., buprenorphine prescription) based on patients’ symptoms independent of race/ethnicity.
In contrast, the researchers also found that Hispanic patients were more likely to receive buprenorphine relative to non-Hispanic patients. This is surprising given past research suggesting Hispanic patients are less likely on average to receive buprenorphine. This unexpected finding may be due to one ED in the study with a large number of Hispanic patients. This ED had a buprenorphine administration rate of nearly 40%- well above every other site. Given that this hospital served a large number of Hispanic patients, it is possible the clinicians did not hold anti-Hispanic biases through working frequently with non-majority ethnicity patients and/or because they also identified as Hispanic. While potentially very useful if true, this explanation for higher buprenorphine prescribing rates for Hispanic individuals should be tested in future research before conclusions can be drawn.
The research team does not describe if the experimental condition was included in the statistical models. This may explain why the finding that racial/ethnic minorities were prescribed buprenorphine at similar rates when adjusting for diagnosis. That is, the intervention was designed to remove bias from diagnosis via a computer program which gave a diagnosis based on the patients’ medical records and symptoms. If diagnosis is a proxy of the intervention, it may mean that the intervention was successful- it made buprenorphine prescription more equitable. On the other hand, the already published results of the clinical trial suggests that there was no difference in buprenorphine prescriptions between conditions.These contradictory findings from the same dataset makes it difficult to draw conclusions about what is accounting for the observed differences in opioid use disorder prescriptions.
Most of the study took place during the COVID-19 pandemic (November2019– May 2021). It is very likely that this impacted the findings in some way. For instance, the added stress of the pandemic may have led people with an opioid use disorder to increase their opioid use and subsequently increased rates of ED visits for opioid use disorder related problems. Such an increase may have differentially impacted EDs serving racial/ethnic minorities, since EDs are a critical source of healthcare for these populations.Thismay have led to an influx of more Black/Hispanic patients seeking care at EDs during this time (e.g., for COVID infections). Subsequently, this could have impacted ED clinicians’ triage practices, and potentially resulted in differential treatment of patients with an opioid use disorder across racial/ethnic lines.
BOTTOM LINE
This study found that Black patients who presented with opioid use disorder symptoms at EDs were less likely to be administered or prescribed buprenorphine compared to White patients. Hispanic patients, on the other hand, were more likely to be given buprenorphine relative to non-Hispanic patients, likely explained by one large Hispanic-serving hospital. Given that these differences were no longer present when controlling for diagnosis, it is possible that systemic biases were impacting the provider-patient relationship, ultimately resulting in underdiagnosis of opioid withdrawal, specifically, and lower likelihood of buprenorphine prescription. There remains a pressing need to develop strategies to address buprenorphine access disparities among racial/ethnic minorities in the US.
For individuals and families seeking recovery: The present research does not provide data on reasons for disparities in buprenorphine prescription, nor does it describe barriers to opioid use disorder treatment faced by racial/ethnic minorities in the US. This makes it difficult to make recommendations for those seeking opioid use disorder treatment. However, the present research does suggest the diagnosis stage of the patient-provider interaction may be a contributor to this treatment disparity. Therefore, those interested in buprenorphine treatment for themselves/others may need to be especially mindful when interacting with clinicians. To ensure they receive necessary opioid use disorder treatment, those seeking care may need to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: It is unknown why sampled Black/Hispanic patients received buprenorphine at differing rates from White/non-Hispanic ED patients, respectively. Nor is it known why these relationships were no longer present when adjusting for patient diagnoses. One possible explanation could be that clinicians’ biases impacted the ways in which they interacted with Black/Hispanic patients. Those providing treatment to and/or work in healthcare system settings serving racial/ethnic minorities may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs. Another option could be for clinicians to utilizeresources to address bias for health professionals.
For policy makers: This study suggests that Black/Hispanic patients who show signs of OUD and related withdrawal and thus could benefit from buprenorphinemaynot be getting it when they present for care at EDs.This may be due in part to these populations having fewer options for where they receive healthcare. One of the farthest-reaching policies would be to increase healthcare access- that is to increase public clinics which serve racial/ethnic minorities. Separate from the critical need of increased healthcare access,it may be helpful for policymakers to create guidelines to increase opioid use disorder screening among all ED patients. That is, this increase in screening may result in more patients with opioid use disorder being identified and referred to treatment who would otherwise not be.