Impact of amphetamine use on treatment with opioid use disorder medications
Amphetamine use is increasing among individuals with opioid use disorder, which may reduce the benefits of opioid use disorder medication while also conferring its own unique harms. This study examined the impact of amphetamine use on medication initiation and outcomes for individuals receiving either buprenorphine or extended-release naltrexone in a randomized control trial.
Rates of amphetamine use have increased over the past several years, with a fourth wave of the overdose epidemic emerging that is characterized by concurrent use of opioids and amphetamines. An increasing number of patients with opioid use disorder are presenting to treatment with recent use of amphetamines.
Mixing opioids and amphetamines comes with various risks and harms, including overdose, with combined amphetamine- and opioid- related overdose deaths increasing in the past several years. Importantly, amphetamine use has the potential to interfere with opioid use disorder medication treatment, including both treatment retention and opioid abstinence. At present, there are no approved medication treatments for amphetamine or other stimulant use disorders (e.g., cocaine) despite rigorous, resource-intensive efforts. Some studies have suggested that medications approved to treat opioid use disorder might also help reduce the use of illicit stimulants in patients with stimulant use disorder. However, findings are mixed, and few studies have evaluated the relationship between medication treatment and amphetamine use in patients with opioid use disorder. Therefore, it is unclear whether patients with co-occurring amphetamine use might have better treatment outcomes with a particular empirically supported medication (e.g., buprenorphine vs. extended-release naltrexone).
Given increased rates of amphetamine use among individuals with opioid use disorder, and absence of empirically supported stimulant use disorder medications, it is essential to evaluate the potential impact of various opioid use disorder medications on amphetamine use. This study examined amphetamine use, its change over time, and its role in successful initiation of opioid use disorder medication treatment, among patients receiving extended-release naltrexone versus buprenorphine treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from the X:BOT trial, an open-label 24-week randomized trial comparing the effectiveness of buprenorphine versus extended-release naltrexone (also known by the brand name Vivitrol) for opioid use disorder, conducted in the United States between 2014 and 2016.
The original trial found that buprenorphine was better than extended-release naltrexone at preventing a return to illicit opioid use. In this secondary analysis, the researchers investigated rates of medication initiation among patients who used amphetamines (methamphetamine and other amphetamines) at baseline, compared to those who didn’t use amphetamines at baseline. They then examined differences in the odds of amphetamine use during the 24-week trial by medication assignment (i.e., patients assigned to buprenorphine vs. extended-release naltrexone), controlling for baseline amphetamine use. The researchers also evaluated the influence of amphetamine use at baseline, and the time of study assessment (week 1 through 24), on amphetamine use over the 24-week trial.
Amphetamine use was assessed at each study visit and was defined as a positive drug test for amphetamines or self-reported use of amphetamines within the past 7 days. All participants in this study were ages 18 or older, had used illicit opioids in the past 30 days, and were enrolled in one of eight specialty addiction treatment sites across the US for a current opioid use disorder, according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Patients started medication in medically supervised inpatient settings, followed by 24 weeks of outpatient medication treatment. Patients completed a baseline assessment prior to starting medication treatment and weekly study assessments for 24 weeks after starting medication.
Five hundred and seventy patients were randomized to receive one of the medication treatments. Among the 18% of patients with baseline amphetamine use, just over half (56%) were assigned to receive buprenorphine and slightly under half (44%) were assigned to receive extended-release naltrexone. Among patients without baseline amphetamine use (72%), 49% were assigned to buprenorphine and 51% were assigned to extended-release naltrexone. The majority of patients in both groups were white (74%) men (70%) in their early thirties who engaged in injection drug use (68%).
WHAT DID THIS STUDY FIND?
Amphetamine use didn’t impact the ability to successfully initiate medication treatment.
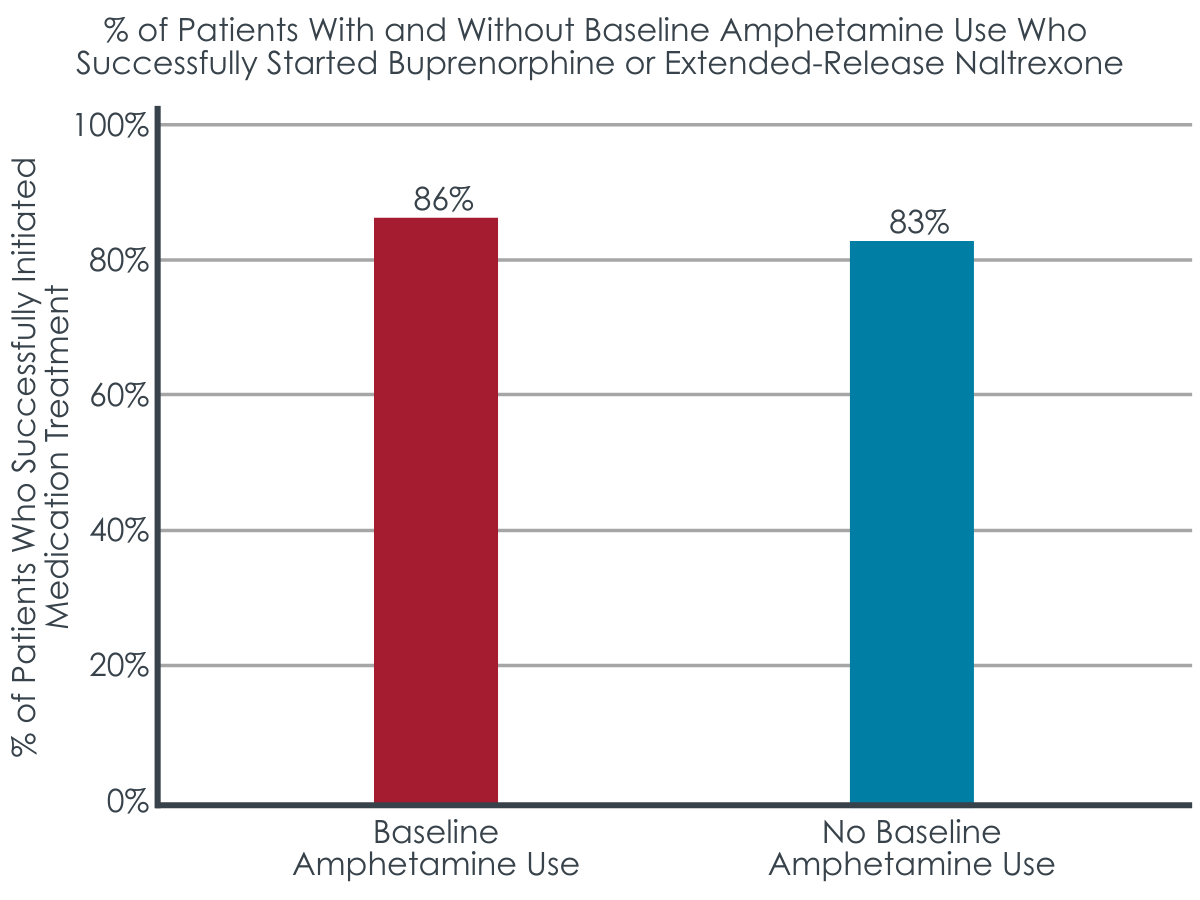
Of the 570 individuals who participated in the clinical trial, the 18% who were using amphetamines at baseline were just as likely as those who didn’t use amphetamines at baseline to successfully start the study medication to which they were assigned: buprenorphine or extended-release naltrexone.
Figure 1. Shows the percentage of patients with and without amphetamine use at baseline who successfully initiated medication treatment.
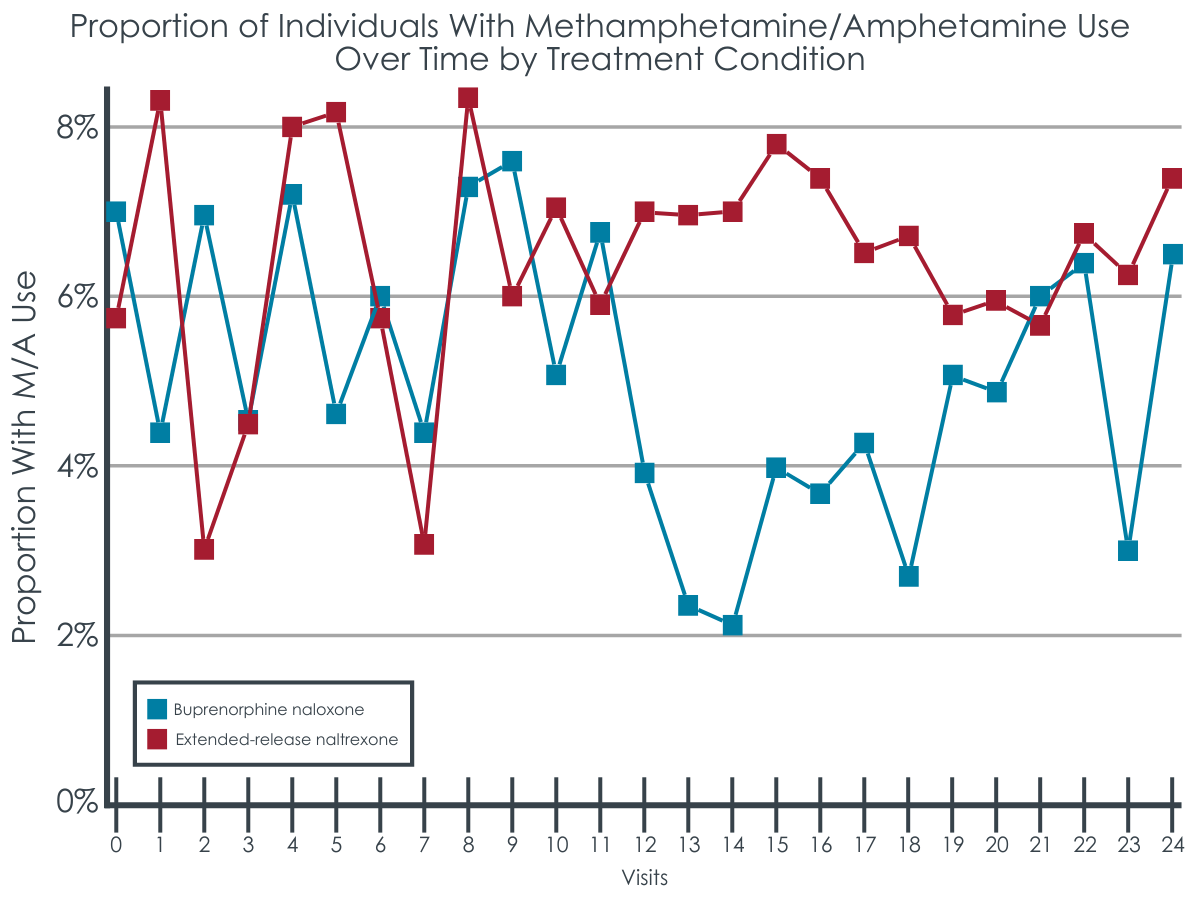
Buprenorphine was associated with a lower likelihood of amphetamine use than extended-release naltrexone.
Participants randomized to receive buprenorphine were about half as likely as those assigned to extended-release naltrexone to use amphetamines during the 24-week trial, though this difference just missed statistical significance. As would be expected, patients who had used amphetamines at baseline were about 16 times more likely to use amphetamines during treatment. Over the course of the trial, the odds of amphetamine use across all participants increased by 4% with each subsequent study visit. Results were consistent when amphetamine use was examined only among those who successfully started the medication to which they were assigned.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study adds to a limited and mixed literature on the association between amphetamine use and different opioid use disorder medication treatments. Studies like this help us better understand how specific treatments impact co-occurring substance use disorders and reveal important information to determine whether add-on treatments are needed to address common substance use problems that co-occur with opioid use disorder, such as amphetamine.
This study found a trend-level effect suggesting that patients who receive buprenorphine, as opposed to extended-release naltrexone, may be less likely to engage in amphetamine use in a given week while on the medication.
The largest differences in amphetamine use between medication groups began to emerge at around week-12 of medication treatment. It may be that patients who received buprenorphine were less likely to feel the need to use amphetamines as a substitute for illicit opioids given buprenorphine’s stimulation of opioid receptors (i.e., as a partial agonist). In the parent study, a portion of the patients didn’t successfully start extended-release naltrexone, resulting in an advantage in the buprenorphine group, who had about twice as many days of opioid abstinence than the extended-release naltrexone group.
Abstinence from opioids may have also helped patients in the buprenorphine group to engage in other healthy behaviors, like a reduction in the use of non-opioid substances. However, this finding was not statistically significant, and the odds of amphetamine use didn’t decline from the beginning to end of treatment in either medication group. In fact, in the entire sample, the likelihood of amphetamine use increased slightly throughout the trial. These results suggest that medication treatment may not produce significant declines in stimulant use over time and those who are seeking help for co-occurring substance use problems may need additional treatment and recovery resources to address their amphetamine use problems alongside their opioid use disorder.
Still, of the studies that have been conducted to date, some show benefits and others do not. Some research has found that amphetamine use decreases over time among patients receiving buprenorphine treatment for opioid use disorder, while other studies reveal no effect of buprenorphine on stimulant use. Mixed findings are also observed for extended-release naltrexone. For example, one study found that adding bupropion (an antidepressant that is also FDA-approved for smoking cessation) to extended-release naltrexone reduced amphetamine use over time among individuals with methamphetamine use disorder, whereas another study found that amphetamine use remained unchanged among individuals receiving extended-release naltrexone for opioid and amphetamine use.
Additional research will help identify other factors that influence amphetamine use during medication treatment (e.g., motivation for recovery, recovery support resources, etc.) and the patients for whom medication treatment might have beneficial effects on co-occurring stimulant use disorders. Regardless, additional treatment and recovery support that targets amphetamine use problems in addition to opioid use problems is likely warranted for patients with these co-occurring disorders. Research has shown the benefits of contingency management for reducing cocaine use among individuals receiving opioid use disorder medication treatment. Additional studies are needed to determine whether adapting therapies like this can help address amphetamine use.
This study also found that using amphetamines before starting medication was a strong predictor of subsequent amphetamine use during the trial, emphasizing the importance of screening patients for amphetamine use before they start opioid use disorder medication treatment and monitoring stimulant use during treatment. Doing so can help to ensure that co-occurring substance use problems are addressed simultaneously to comprehensively support patients and promote positive recovery outcomes.
This study was a secondary analysis of a randomized trial where amphetamine use wasn’t the focus. In addition, the analyses did not control for medication dose or other clinical factors and missing data on amphetamine use may have impacted the results. The researchers did not report whether those with baseline amphetamine use were more or less likely to start a particular type of medication (i.e., extended-release naltrexone vs. buprenorphine). They also didn’t evaluate the impact of the amount of amphetamine use or an amphetamine use disorder diagnosis at baseline on outcomes. Additional research, including naturalistic studies of real-world patients with co-occurring stimulant and opioid use disorders are needed.
The majority of participants were white men and findings may not apply to other populations. This study also excluded patients who had other psychiatric or substance use disorders that required a higher level of care. Results may not apply to those with greater clinical severity or other co-occurring disorders.
BOTTOM LINE
About one-fifth of patients were using amphetamines before starting treatment. Recent use of amphetamines did not affect patients’ ability to successfully initiate buprenorphine or extended-release naltrexone. Compared to patients who received extended-release naltrexone, those who received buprenorphine were half as likely to use amphetamines each week during treatment. However, this finding did not reach statistical significance and the odds of amphetamine use slightly increased in both medication groups from the beginning of the trial to the end. This study contributes to limited research evaluating the relationship between medication treatments and amphetamine use among patients with opioid use disorder. Enhancing our understanding of the effects of various treatments on co-occurring substance use and related disorders will ultimately help guide treatment approaches for polysubstance use and best practices for enhancing treatment/recovery outcomes.
For individuals and families seeking recovery: Co-use of opioids and amphetamines may reduce the benefits of opioid use disorder medication treatment while also conferring unique harms in its own right. Though research has yet to determine if a particular medication treatment is best for patients who also use amphetamines, individuals with opioid use disorder are likely to benefit from additional treatment and recovery support, beyond opioid use disorder medication treatment, to address co-occurring substance use problems. For example, contingency management and other psychosocial treatments are shown to help individuals with stimulant use disorders. Individuals seeking treatment should speak with a practitioner about their use of non-opioid substances, in addition to opioids, to determine a treatment and recovery plan that can best support their individual needs.
For treatment professionals and treatment systems: Given the potential negative impact of amphetamine use on opioid use disorder medication treatment, addressing co-occurring amphetamine use is essential to ensure patients’ successful recovery outcomes. Patients receiving buprenorphine treatment for opioid use disorder might be less likely to use amphetamines compared to those receiving extended-release naltrexone but research findings to date are limited and mixed. Patients with co-occurring amphetamine use problems may need additional treatment and recovery supports to address amphetamine use problems during medication treatment. There are currently no FDA approved medications for amphetamine use disorder, but research suggests that some drugs like mirtazapine and methylphenidate show potential promise for some patients. Some behavioral therapies like contingency management are also shown to be helpful treatments for stimulant use. Given that amphetamine use before medication treatment predicts use during treatment, screening, and ongoing monitoring of patients for co-use of amphetamines and other substances before and during treatment can help to ensure that co-occurring substance use problems are addressed simultaneously to promote positive recovery outcomes.
For scientists: It is essential to conduct real-world longitudinal investigations of the relationship between amphetamine use and different medication treatments for opioid use disorder, with purposeful recruitment of patients with co-occurring opioid and amphetamine use disorders. Evaluation of the frequency and amount of amphetamine use over the course of treatment, patient outcomes (e.g., opioid/amphetamine use, treatment retention, well-being, quality of life) with different medications, and moderators of the relationship between medication and amphetamine use are needed to enhance clinical practice and ideal treatment approaches for polysubstance use disorders. Investigations comparing all three FDA-approved medications for opioid use disorder and studies that examine adjunct medications that show promise for stimulant use disorders are also needed.
For policy makers: Studies like this help us better understand how different treatments affect co-occurring substance use disorders, which can help guide clinical approaches for addressing polysubstance use problems, which are the norm amongst substance use disorder populations. Given that the fourth wave of the overdose epidemic is characterized by a rise in co-use of amphetamines and opioids, and that amphetamine use can reduce the benefits of opioid use disorder medication treatment, it is essential to identify optimal treatment approaches for individuals who engage in co-use of these substances. However, there are few studies on the relationship between amphetamine use and opioid use disorder treatments, calling for additional research funding to help identify which medications are ideal for these co-occurring disorders and what additional factors might influence treatment outcomes.
Rates of amphetamine use have increased over the past several years, with a fourth wave of the overdose epidemic emerging that is characterized by concurrent use of opioids and amphetamines. An increasing number of patients with opioid use disorder are presenting to treatment with recent use of amphetamines.
Mixing opioids and amphetamines comes with various risks and harms, including overdose, with combined amphetamine- and opioid- related overdose deaths increasing in the past several years. Importantly, amphetamine use has the potential to interfere with opioid use disorder medication treatment, including both treatment retention and opioid abstinence. At present, there are no approved medication treatments for amphetamine or other stimulant use disorders (e.g., cocaine) despite rigorous, resource-intensive efforts. Some studies have suggested that medications approved to treat opioid use disorder might also help reduce the use of illicit stimulants in patients with stimulant use disorder. However, findings are mixed, and few studies have evaluated the relationship between medication treatment and amphetamine use in patients with opioid use disorder. Therefore, it is unclear whether patients with co-occurring amphetamine use might have better treatment outcomes with a particular empirically supported medication (e.g., buprenorphine vs. extended-release naltrexone).
Given increased rates of amphetamine use among individuals with opioid use disorder, and absence of empirically supported stimulant use disorder medications, it is essential to evaluate the potential impact of various opioid use disorder medications on amphetamine use. This study examined amphetamine use, its change over time, and its role in successful initiation of opioid use disorder medication treatment, among patients receiving extended-release naltrexone versus buprenorphine treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from the X:BOT trial, an open-label 24-week randomized trial comparing the effectiveness of buprenorphine versus extended-release naltrexone (also known by the brand name Vivitrol) for opioid use disorder, conducted in the United States between 2014 and 2016.
The original trial found that buprenorphine was better than extended-release naltrexone at preventing a return to illicit opioid use. In this secondary analysis, the researchers investigated rates of medication initiation among patients who used amphetamines (methamphetamine and other amphetamines) at baseline, compared to those who didn’t use amphetamines at baseline. They then examined differences in the odds of amphetamine use during the 24-week trial by medication assignment (i.e., patients assigned to buprenorphine vs. extended-release naltrexone), controlling for baseline amphetamine use. The researchers also evaluated the influence of amphetamine use at baseline, and the time of study assessment (week 1 through 24), on amphetamine use over the 24-week trial.
Amphetamine use was assessed at each study visit and was defined as a positive drug test for amphetamines or self-reported use of amphetamines within the past 7 days. All participants in this study were ages 18 or older, had used illicit opioids in the past 30 days, and were enrolled in one of eight specialty addiction treatment sites across the US for a current opioid use disorder, according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Patients started medication in medically supervised inpatient settings, followed by 24 weeks of outpatient medication treatment. Patients completed a baseline assessment prior to starting medication treatment and weekly study assessments for 24 weeks after starting medication.
Five hundred and seventy patients were randomized to receive one of the medication treatments. Among the 18% of patients with baseline amphetamine use, just over half (56%) were assigned to receive buprenorphine and slightly under half (44%) were assigned to receive extended-release naltrexone. Among patients without baseline amphetamine use (72%), 49% were assigned to buprenorphine and 51% were assigned to extended-release naltrexone. The majority of patients in both groups were white (74%) men (70%) in their early thirties who engaged in injection drug use (68%).
WHAT DID THIS STUDY FIND?
Amphetamine use didn’t impact the ability to successfully initiate medication treatment.
Of the 570 individuals who participated in the clinical trial, the 18% who were using amphetamines at baseline were just as likely as those who didn’t use amphetamines at baseline to successfully start the study medication to which they were assigned: buprenorphine or extended-release naltrexone.
Figure 1. Shows the percentage of patients with and without amphetamine use at baseline who successfully initiated medication treatment.
Buprenorphine was associated with a lower likelihood of amphetamine use than extended-release naltrexone.
Participants randomized to receive buprenorphine were about half as likely as those assigned to extended-release naltrexone to use amphetamines during the 24-week trial, though this difference just missed statistical significance. As would be expected, patients who had used amphetamines at baseline were about 16 times more likely to use amphetamines during treatment. Over the course of the trial, the odds of amphetamine use across all participants increased by 4% with each subsequent study visit. Results were consistent when amphetamine use was examined only among those who successfully started the medication to which they were assigned.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study adds to a limited and mixed literature on the association between amphetamine use and different opioid use disorder medication treatments. Studies like this help us better understand how specific treatments impact co-occurring substance use disorders and reveal important information to determine whether add-on treatments are needed to address common substance use problems that co-occur with opioid use disorder, such as amphetamine.
This study found a trend-level effect suggesting that patients who receive buprenorphine, as opposed to extended-release naltrexone, may be less likely to engage in amphetamine use in a given week while on the medication.
The largest differences in amphetamine use between medication groups began to emerge at around week-12 of medication treatment. It may be that patients who received buprenorphine were less likely to feel the need to use amphetamines as a substitute for illicit opioids given buprenorphine’s stimulation of opioid receptors (i.e., as a partial agonist). In the parent study, a portion of the patients didn’t successfully start extended-release naltrexone, resulting in an advantage in the buprenorphine group, who had about twice as many days of opioid abstinence than the extended-release naltrexone group.
Abstinence from opioids may have also helped patients in the buprenorphine group to engage in other healthy behaviors, like a reduction in the use of non-opioid substances. However, this finding was not statistically significant, and the odds of amphetamine use didn’t decline from the beginning to end of treatment in either medication group. In fact, in the entire sample, the likelihood of amphetamine use increased slightly throughout the trial. These results suggest that medication treatment may not produce significant declines in stimulant use over time and those who are seeking help for co-occurring substance use problems may need additional treatment and recovery resources to address their amphetamine use problems alongside their opioid use disorder.
Still, of the studies that have been conducted to date, some show benefits and others do not. Some research has found that amphetamine use decreases over time among patients receiving buprenorphine treatment for opioid use disorder, while other studies reveal no effect of buprenorphine on stimulant use. Mixed findings are also observed for extended-release naltrexone. For example, one study found that adding bupropion (an antidepressant that is also FDA-approved for smoking cessation) to extended-release naltrexone reduced amphetamine use over time among individuals with methamphetamine use disorder, whereas another study found that amphetamine use remained unchanged among individuals receiving extended-release naltrexone for opioid and amphetamine use.
Additional research will help identify other factors that influence amphetamine use during medication treatment (e.g., motivation for recovery, recovery support resources, etc.) and the patients for whom medication treatment might have beneficial effects on co-occurring stimulant use disorders. Regardless, additional treatment and recovery support that targets amphetamine use problems in addition to opioid use problems is likely warranted for patients with these co-occurring disorders. Research has shown the benefits of contingency management for reducing cocaine use among individuals receiving opioid use disorder medication treatment. Additional studies are needed to determine whether adapting therapies like this can help address amphetamine use.
This study also found that using amphetamines before starting medication was a strong predictor of subsequent amphetamine use during the trial, emphasizing the importance of screening patients for amphetamine use before they start opioid use disorder medication treatment and monitoring stimulant use during treatment. Doing so can help to ensure that co-occurring substance use problems are addressed simultaneously to comprehensively support patients and promote positive recovery outcomes.
This study was a secondary analysis of a randomized trial where amphetamine use wasn’t the focus. In addition, the analyses did not control for medication dose or other clinical factors and missing data on amphetamine use may have impacted the results. The researchers did not report whether those with baseline amphetamine use were more or less likely to start a particular type of medication (i.e., extended-release naltrexone vs. buprenorphine). They also didn’t evaluate the impact of the amount of amphetamine use or an amphetamine use disorder diagnosis at baseline on outcomes. Additional research, including naturalistic studies of real-world patients with co-occurring stimulant and opioid use disorders are needed.
The majority of participants were white men and findings may not apply to other populations. This study also excluded patients who had other psychiatric or substance use disorders that required a higher level of care. Results may not apply to those with greater clinical severity or other co-occurring disorders.
BOTTOM LINE
About one-fifth of patients were using amphetamines before starting treatment. Recent use of amphetamines did not affect patients’ ability to successfully initiate buprenorphine or extended-release naltrexone. Compared to patients who received extended-release naltrexone, those who received buprenorphine were half as likely to use amphetamines each week during treatment. However, this finding did not reach statistical significance and the odds of amphetamine use slightly increased in both medication groups from the beginning of the trial to the end. This study contributes to limited research evaluating the relationship between medication treatments and amphetamine use among patients with opioid use disorder. Enhancing our understanding of the effects of various treatments on co-occurring substance use and related disorders will ultimately help guide treatment approaches for polysubstance use and best practices for enhancing treatment/recovery outcomes.
For individuals and families seeking recovery: Co-use of opioids and amphetamines may reduce the benefits of opioid use disorder medication treatment while also conferring unique harms in its own right. Though research has yet to determine if a particular medication treatment is best for patients who also use amphetamines, individuals with opioid use disorder are likely to benefit from additional treatment and recovery support, beyond opioid use disorder medication treatment, to address co-occurring substance use problems. For example, contingency management and other psychosocial treatments are shown to help individuals with stimulant use disorders. Individuals seeking treatment should speak with a practitioner about their use of non-opioid substances, in addition to opioids, to determine a treatment and recovery plan that can best support their individual needs.
For treatment professionals and treatment systems: Given the potential negative impact of amphetamine use on opioid use disorder medication treatment, addressing co-occurring amphetamine use is essential to ensure patients’ successful recovery outcomes. Patients receiving buprenorphine treatment for opioid use disorder might be less likely to use amphetamines compared to those receiving extended-release naltrexone but research findings to date are limited and mixed. Patients with co-occurring amphetamine use problems may need additional treatment and recovery supports to address amphetamine use problems during medication treatment. There are currently no FDA approved medications for amphetamine use disorder, but research suggests that some drugs like mirtazapine and methylphenidate show potential promise for some patients. Some behavioral therapies like contingency management are also shown to be helpful treatments for stimulant use. Given that amphetamine use before medication treatment predicts use during treatment, screening, and ongoing monitoring of patients for co-use of amphetamines and other substances before and during treatment can help to ensure that co-occurring substance use problems are addressed simultaneously to promote positive recovery outcomes.
For scientists: It is essential to conduct real-world longitudinal investigations of the relationship between amphetamine use and different medication treatments for opioid use disorder, with purposeful recruitment of patients with co-occurring opioid and amphetamine use disorders. Evaluation of the frequency and amount of amphetamine use over the course of treatment, patient outcomes (e.g., opioid/amphetamine use, treatment retention, well-being, quality of life) with different medications, and moderators of the relationship between medication and amphetamine use are needed to enhance clinical practice and ideal treatment approaches for polysubstance use disorders. Investigations comparing all three FDA-approved medications for opioid use disorder and studies that examine adjunct medications that show promise for stimulant use disorders are also needed.
For policy makers: Studies like this help us better understand how different treatments affect co-occurring substance use disorders, which can help guide clinical approaches for addressing polysubstance use problems, which are the norm amongst substance use disorder populations. Given that the fourth wave of the overdose epidemic is characterized by a rise in co-use of amphetamines and opioids, and that amphetamine use can reduce the benefits of opioid use disorder medication treatment, it is essential to identify optimal treatment approaches for individuals who engage in co-use of these substances. However, there are few studies on the relationship between amphetamine use and opioid use disorder treatments, calling for additional research funding to help identify which medications are ideal for these co-occurring disorders and what additional factors might influence treatment outcomes.
Rates of amphetamine use have increased over the past several years, with a fourth wave of the overdose epidemic emerging that is characterized by concurrent use of opioids and amphetamines. An increasing number of patients with opioid use disorder are presenting to treatment with recent use of amphetamines.
Mixing opioids and amphetamines comes with various risks and harms, including overdose, with combined amphetamine- and opioid- related overdose deaths increasing in the past several years. Importantly, amphetamine use has the potential to interfere with opioid use disorder medication treatment, including both treatment retention and opioid abstinence. At present, there are no approved medication treatments for amphetamine or other stimulant use disorders (e.g., cocaine) despite rigorous, resource-intensive efforts. Some studies have suggested that medications approved to treat opioid use disorder might also help reduce the use of illicit stimulants in patients with stimulant use disorder. However, findings are mixed, and few studies have evaluated the relationship between medication treatment and amphetamine use in patients with opioid use disorder. Therefore, it is unclear whether patients with co-occurring amphetamine use might have better treatment outcomes with a particular empirically supported medication (e.g., buprenorphine vs. extended-release naltrexone).
Given increased rates of amphetamine use among individuals with opioid use disorder, and absence of empirically supported stimulant use disorder medications, it is essential to evaluate the potential impact of various opioid use disorder medications on amphetamine use. This study examined amphetamine use, its change over time, and its role in successful initiation of opioid use disorder medication treatment, among patients receiving extended-release naltrexone versus buprenorphine treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from the X:BOT trial, an open-label 24-week randomized trial comparing the effectiveness of buprenorphine versus extended-release naltrexone (also known by the brand name Vivitrol) for opioid use disorder, conducted in the United States between 2014 and 2016.
The original trial found that buprenorphine was better than extended-release naltrexone at preventing a return to illicit opioid use. In this secondary analysis, the researchers investigated rates of medication initiation among patients who used amphetamines (methamphetamine and other amphetamines) at baseline, compared to those who didn’t use amphetamines at baseline. They then examined differences in the odds of amphetamine use during the 24-week trial by medication assignment (i.e., patients assigned to buprenorphine vs. extended-release naltrexone), controlling for baseline amphetamine use. The researchers also evaluated the influence of amphetamine use at baseline, and the time of study assessment (week 1 through 24), on amphetamine use over the 24-week trial.
Amphetamine use was assessed at each study visit and was defined as a positive drug test for amphetamines or self-reported use of amphetamines within the past 7 days. All participants in this study were ages 18 or older, had used illicit opioids in the past 30 days, and were enrolled in one of eight specialty addiction treatment sites across the US for a current opioid use disorder, according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Patients started medication in medically supervised inpatient settings, followed by 24 weeks of outpatient medication treatment. Patients completed a baseline assessment prior to starting medication treatment and weekly study assessments for 24 weeks after starting medication.
Five hundred and seventy patients were randomized to receive one of the medication treatments. Among the 18% of patients with baseline amphetamine use, just over half (56%) were assigned to receive buprenorphine and slightly under half (44%) were assigned to receive extended-release naltrexone. Among patients without baseline amphetamine use (72%), 49% were assigned to buprenorphine and 51% were assigned to extended-release naltrexone. The majority of patients in both groups were white (74%) men (70%) in their early thirties who engaged in injection drug use (68%).
WHAT DID THIS STUDY FIND?
Amphetamine use didn’t impact the ability to successfully initiate medication treatment.
Of the 570 individuals who participated in the clinical trial, the 18% who were using amphetamines at baseline were just as likely as those who didn’t use amphetamines at baseline to successfully start the study medication to which they were assigned: buprenorphine or extended-release naltrexone.
Figure 1. Shows the percentage of patients with and without amphetamine use at baseline who successfully initiated medication treatment.
Buprenorphine was associated with a lower likelihood of amphetamine use than extended-release naltrexone.
Participants randomized to receive buprenorphine were about half as likely as those assigned to extended-release naltrexone to use amphetamines during the 24-week trial, though this difference just missed statistical significance. As would be expected, patients who had used amphetamines at baseline were about 16 times more likely to use amphetamines during treatment. Over the course of the trial, the odds of amphetamine use across all participants increased by 4% with each subsequent study visit. Results were consistent when amphetamine use was examined only among those who successfully started the medication to which they were assigned.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study adds to a limited and mixed literature on the association between amphetamine use and different opioid use disorder medication treatments. Studies like this help us better understand how specific treatments impact co-occurring substance use disorders and reveal important information to determine whether add-on treatments are needed to address common substance use problems that co-occur with opioid use disorder, such as amphetamine.
This study found a trend-level effect suggesting that patients who receive buprenorphine, as opposed to extended-release naltrexone, may be less likely to engage in amphetamine use in a given week while on the medication.
The largest differences in amphetamine use between medication groups began to emerge at around week-12 of medication treatment. It may be that patients who received buprenorphine were less likely to feel the need to use amphetamines as a substitute for illicit opioids given buprenorphine’s stimulation of opioid receptors (i.e., as a partial agonist). In the parent study, a portion of the patients didn’t successfully start extended-release naltrexone, resulting in an advantage in the buprenorphine group, who had about twice as many days of opioid abstinence than the extended-release naltrexone group.
Abstinence from opioids may have also helped patients in the buprenorphine group to engage in other healthy behaviors, like a reduction in the use of non-opioid substances. However, this finding was not statistically significant, and the odds of amphetamine use didn’t decline from the beginning to end of treatment in either medication group. In fact, in the entire sample, the likelihood of amphetamine use increased slightly throughout the trial. These results suggest that medication treatment may not produce significant declines in stimulant use over time and those who are seeking help for co-occurring substance use problems may need additional treatment and recovery resources to address their amphetamine use problems alongside their opioid use disorder.
Still, of the studies that have been conducted to date, some show benefits and others do not. Some research has found that amphetamine use decreases over time among patients receiving buprenorphine treatment for opioid use disorder, while other studies reveal no effect of buprenorphine on stimulant use. Mixed findings are also observed for extended-release naltrexone. For example, one study found that adding bupropion (an antidepressant that is also FDA-approved for smoking cessation) to extended-release naltrexone reduced amphetamine use over time among individuals with methamphetamine use disorder, whereas another study found that amphetamine use remained unchanged among individuals receiving extended-release naltrexone for opioid and amphetamine use.
Additional research will help identify other factors that influence amphetamine use during medication treatment (e.g., motivation for recovery, recovery support resources, etc.) and the patients for whom medication treatment might have beneficial effects on co-occurring stimulant use disorders. Regardless, additional treatment and recovery support that targets amphetamine use problems in addition to opioid use problems is likely warranted for patients with these co-occurring disorders. Research has shown the benefits of contingency management for reducing cocaine use among individuals receiving opioid use disorder medication treatment. Additional studies are needed to determine whether adapting therapies like this can help address amphetamine use.
This study also found that using amphetamines before starting medication was a strong predictor of subsequent amphetamine use during the trial, emphasizing the importance of screening patients for amphetamine use before they start opioid use disorder medication treatment and monitoring stimulant use during treatment. Doing so can help to ensure that co-occurring substance use problems are addressed simultaneously to comprehensively support patients and promote positive recovery outcomes.
This study was a secondary analysis of a randomized trial where amphetamine use wasn’t the focus. In addition, the analyses did not control for medication dose or other clinical factors and missing data on amphetamine use may have impacted the results. The researchers did not report whether those with baseline amphetamine use were more or less likely to start a particular type of medication (i.e., extended-release naltrexone vs. buprenorphine). They also didn’t evaluate the impact of the amount of amphetamine use or an amphetamine use disorder diagnosis at baseline on outcomes. Additional research, including naturalistic studies of real-world patients with co-occurring stimulant and opioid use disorders are needed.
The majority of participants were white men and findings may not apply to other populations. This study also excluded patients who had other psychiatric or substance use disorders that required a higher level of care. Results may not apply to those with greater clinical severity or other co-occurring disorders.
BOTTOM LINE
About one-fifth of patients were using amphetamines before starting treatment. Recent use of amphetamines did not affect patients’ ability to successfully initiate buprenorphine or extended-release naltrexone. Compared to patients who received extended-release naltrexone, those who received buprenorphine were half as likely to use amphetamines each week during treatment. However, this finding did not reach statistical significance and the odds of amphetamine use slightly increased in both medication groups from the beginning of the trial to the end. This study contributes to limited research evaluating the relationship between medication treatments and amphetamine use among patients with opioid use disorder. Enhancing our understanding of the effects of various treatments on co-occurring substance use and related disorders will ultimately help guide treatment approaches for polysubstance use and best practices for enhancing treatment/recovery outcomes.
For individuals and families seeking recovery: Co-use of opioids and amphetamines may reduce the benefits of opioid use disorder medication treatment while also conferring unique harms in its own right. Though research has yet to determine if a particular medication treatment is best for patients who also use amphetamines, individuals with opioid use disorder are likely to benefit from additional treatment and recovery support, beyond opioid use disorder medication treatment, to address co-occurring substance use problems. For example, contingency management and other psychosocial treatments are shown to help individuals with stimulant use disorders. Individuals seeking treatment should speak with a practitioner about their use of non-opioid substances, in addition to opioids, to determine a treatment and recovery plan that can best support their individual needs.
For treatment professionals and treatment systems: Given the potential negative impact of amphetamine use on opioid use disorder medication treatment, addressing co-occurring amphetamine use is essential to ensure patients’ successful recovery outcomes. Patients receiving buprenorphine treatment for opioid use disorder might be less likely to use amphetamines compared to those receiving extended-release naltrexone but research findings to date are limited and mixed. Patients with co-occurring amphetamine use problems may need additional treatment and recovery supports to address amphetamine use problems during medication treatment. There are currently no FDA approved medications for amphetamine use disorder, but research suggests that some drugs like mirtazapine and methylphenidate show potential promise for some patients. Some behavioral therapies like contingency management are also shown to be helpful treatments for stimulant use. Given that amphetamine use before medication treatment predicts use during treatment, screening, and ongoing monitoring of patients for co-use of amphetamines and other substances before and during treatment can help to ensure that co-occurring substance use problems are addressed simultaneously to promote positive recovery outcomes.
For scientists: It is essential to conduct real-world longitudinal investigations of the relationship between amphetamine use and different medication treatments for opioid use disorder, with purposeful recruitment of patients with co-occurring opioid and amphetamine use disorders. Evaluation of the frequency and amount of amphetamine use over the course of treatment, patient outcomes (e.g., opioid/amphetamine use, treatment retention, well-being, quality of life) with different medications, and moderators of the relationship between medication and amphetamine use are needed to enhance clinical practice and ideal treatment approaches for polysubstance use disorders. Investigations comparing all three FDA-approved medications for opioid use disorder and studies that examine adjunct medications that show promise for stimulant use disorders are also needed.
For policy makers: Studies like this help us better understand how different treatments affect co-occurring substance use disorders, which can help guide clinical approaches for addressing polysubstance use problems, which are the norm amongst substance use disorder populations. Given that the fourth wave of the overdose epidemic is characterized by a rise in co-use of amphetamines and opioids, and that amphetamine use can reduce the benefits of opioid use disorder medication treatment, it is essential to identify optimal treatment approaches for individuals who engage in co-use of these substances. However, there are few studies on the relationship between amphetamine use and opioid use disorder treatments, calling for additional research funding to help identify which medications are ideal for these co-occurring disorders and what additional factors might influence treatment outcomes.