Can providing methadone in primary care promote greater use of healthcare services?
Research supports the integration of opioid use disorder medication treatment into primary care for enhancing access to treatment and patient outcomes. Additional research is needed to characterize the effects of integrated healthcare models on patient care and service use. This study examined the impact of integrated methadone treatment, provider incentives, and the duration of medication treatment on patients’ use of healthcare services in Ukraine.
Initiatives to expand access to medication treatments for opioid use disorder (e.g., buprenorphine, methadone) have increased globally. Towards this end, Ukraine recently changed their laws around opioid use disorder medication treatments, allowing for the delivery of methadone in general medical settings like primary care practices. Research supports the integration of opioid use disorder medication treatment into primary care practices for improving patient outcomes. However, additional research is needed to examine whether integrated healthcare models can better help patients obtain the comprehensive care they need, including specialty care like addiction treatment as well as primary care like regular medical exams and hepatitis treatment.
Examining whether patients use the healthcare services that their providers recommend can highlight the impact of integrated treatment on patient care. The impact of integrated healthcare models on patient care and service use in Ukraine is not yet clear. In addition to efforts that expand access to medication treatment, efforts are needed to ensure optimal quality of care. ‘Pay-for-performance’ is a practice in which healthcare providers are paid based on their care delivery and whether optimal patient outcomes are achieved, with the goal of improving the quality and efficiency of care. Pay-for-performance incentives are recommended by the World Health Organization and the Institute of Medicine to improve quality of care, but they are not yet widely used in Ukraine and studies are needed to determine the impact of incentives on healthcare delivery and outcomes.
Studying the impact of integrated healthcare and pay-for-performance models on patients’ healthcare service use can help guide healthcare systems to implement ideal service models that comprehensively support overall patient health in addition to opioid use disorder treatment. To examine the new integrated healthcare model implemented in Ukraine for individuals with opioid use disorder, this randomized trial evaluated the impact of integrated methadone, pay-for-performance incentives, and the duration of medication treatment on patients’ use of healthcare services recommended by their providers.
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal multi-site trial to examine healthcare service use among individuals with opioid use disorder who were randomized to receive methadone treatment at specialty addiction treatment clinics or primary care clinics throughout Ukraine. Nine-hundred and ninety adults seeking or receiving medication treatment were recruited from specialty addiction treatment clinics in nine regions across Ukraine.
Participants were randomly assigned to one of three conditions: (1) methadone treatment at a specialty addiction treatment clinic, the current standard of care in Ukraine; (2) methadone treatment at a primary care clinic with pay-for-performance incentives for physicians; (3) methadone treatment at a primary care clinic without pay-for-performance incentives for physicians.
The researchers randomly assigned primary care clinics to receive pay-for-performance incentives or to not receive these incentives. Participants who were randomized to receive care at a primary care clinic were able to choose their preferred primary care clinic from a list, but were not told (i.e., “blinded”) if the clinic they selected offered pay-for-performance incentives. Clinic type and incentives were balanced across geographic regions.
All clinic staff at primary care practices had completed two three-day training courses (including clinical didactic and case presentations) on opioid agonist treatment, HIV and tuberculosis, ECHO-Integrated Care, and quality improvement strategies. Clinicians at primary care clinics that were randomly assigned to receive pay-for-performance incentives were informed that they could receive a financial monthly bonus depending on the number of healthcare service activities that their patients were referred to and actually completed.
Participants completed self-report questionnaires upon enrolling in the study (baseline), and 6- and 12-months after baseline. Questions were developed using Ukraine Ministry of Health guidelines and national/international experts and concerned healthcare service use in the past 6 months.
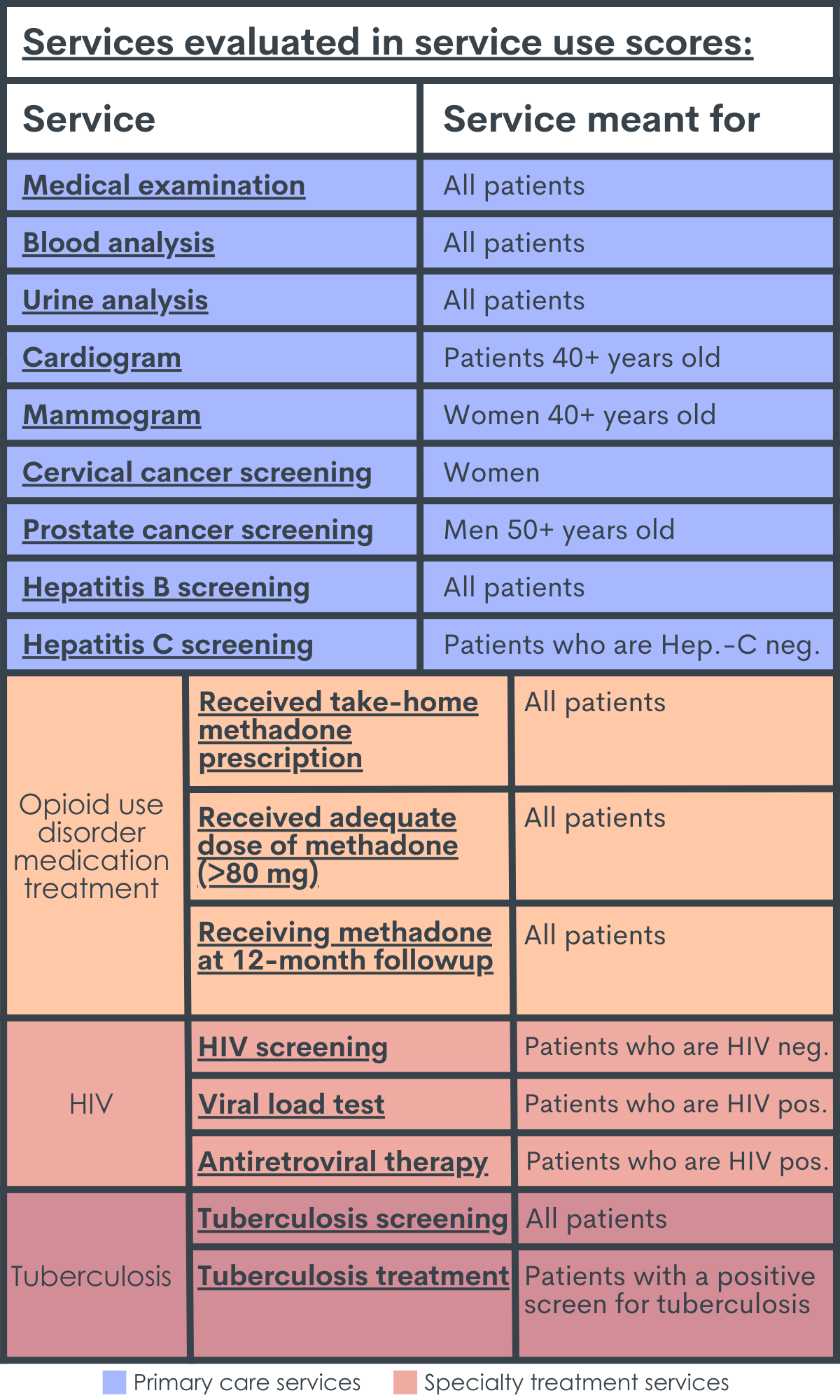
An overall service use score was calculated for each participant by dividing the number of services the patient was recommended and completed/used, by the number of services the patient was recommended, and multiplying by 100 to obtain a percentage of services used.
Services included primary care and specialty treatment services (outlined in table below). The same procedure was used to calculate service use scores for: (1) primary care services only (i.e. dividing the number of primary care services the patient was recommended and completed, by the number of primary care services the patient was recommended, and multiplying by 100); (2) specialty care services only (i.e. dividing the number of specialty treatment services the patient was recommended and completed, by the number of specialty treatment services the patient was recommended, and multiplying by 100). All scores ranged from a minimum of 0% to a maximum of 100% and were based on participant questionnaires completed at the 12-month follow-up (i.e., 12 months after beginning the study).
The researchers compared service use scores at month-12 follow up between: (1) patients assigned to primary care clinics vs. patients assigned to specialty care clinics; (2) patients assigned to primary care clinics with vs. without pay-for-performance incentives; (3) patients already established on methadone for 3 or more months at study start vs. patients initiating methadone at study start.
After accounting for participants were unable to be contacted at the follow up timepoints, a total of 818 people were included in analyses concerning healthcare service use (n=291 assigned to specialty treatment clinics; n=527 assigned to primary care clinics). All participants had a history of injection drug use and a diagnosis of opioid use disorder (per the International Classification of Diseases 10 criteria for opioid dependence).
All participants were advised to seek primary care services at their local clinics, regardless of group assignment. Sixty-one percent of participants were already receiving methadone for three or more months at study start, while 39% were newly initiating methadone. Over 90% of participants were still receiving methadone treatment at month-12 follow up. The majority of participants were men (82%) in their early 40’s. About half of the sample was unemployed, had HIV, and hepatitis-C, and about one-third had income below the poverty level. Characteristics did not differ between participants randomized to different groups.
WHAT DID THIS STUDY FIND?
Service use was higher for patients assigned to a primary care practice irrespective of pay-for-performance.
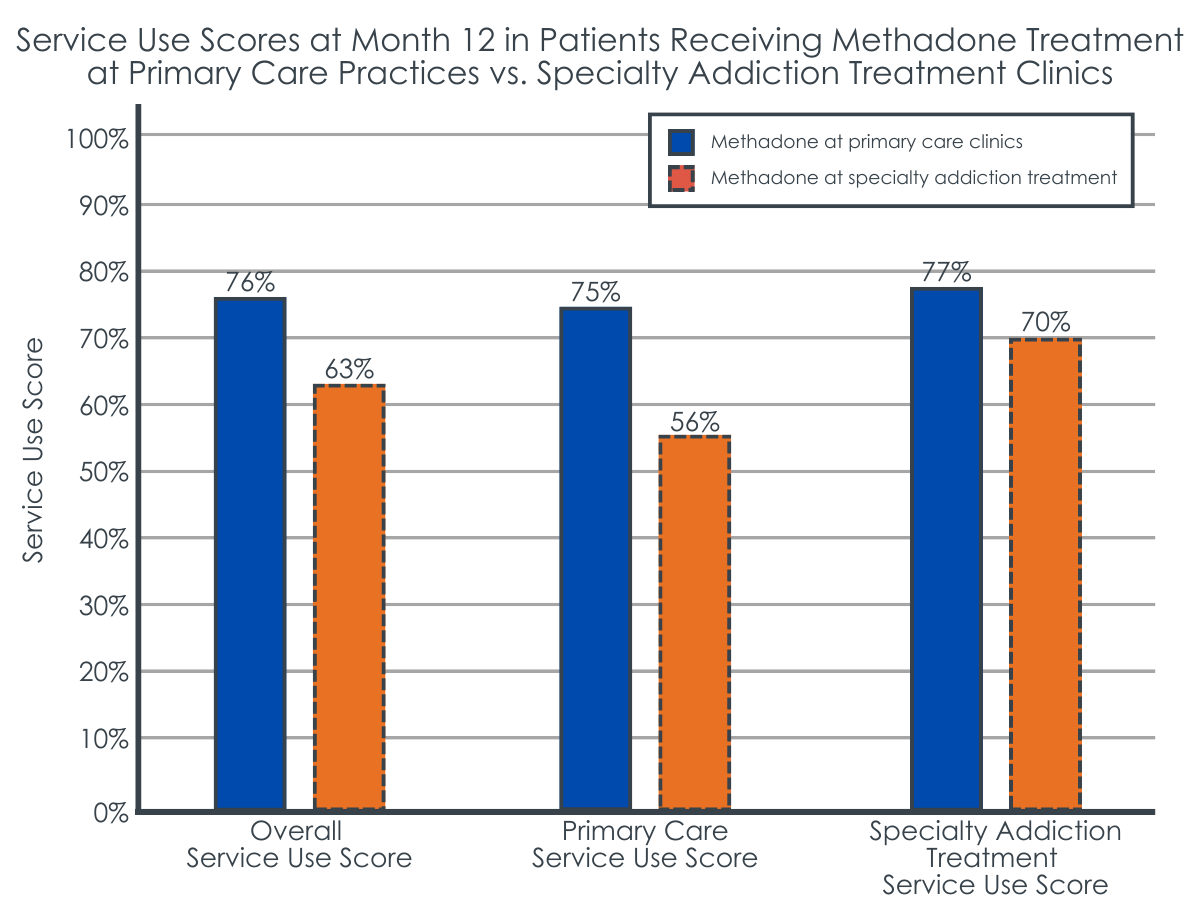
Relative to patients who received methadone from a specialty treatment clinic, patients who received methadone from a primary care clinic had higher overall service use scores at 12 months. When primary care service use scores and specialty treatment service use scores were evaluated independently, both were significantly higher in the group that received treatment at a primary care clinic.
Figure 2 shows the overall service use scores, primary care service use scores, and specialty addiction treatment service use scores of patients receiving methadone at primary care clinics vs. specialty addiction treatment clinics. Scores range from 0% to 100%, with higher scores indicating greater use of healthcare services that patients were referred to.
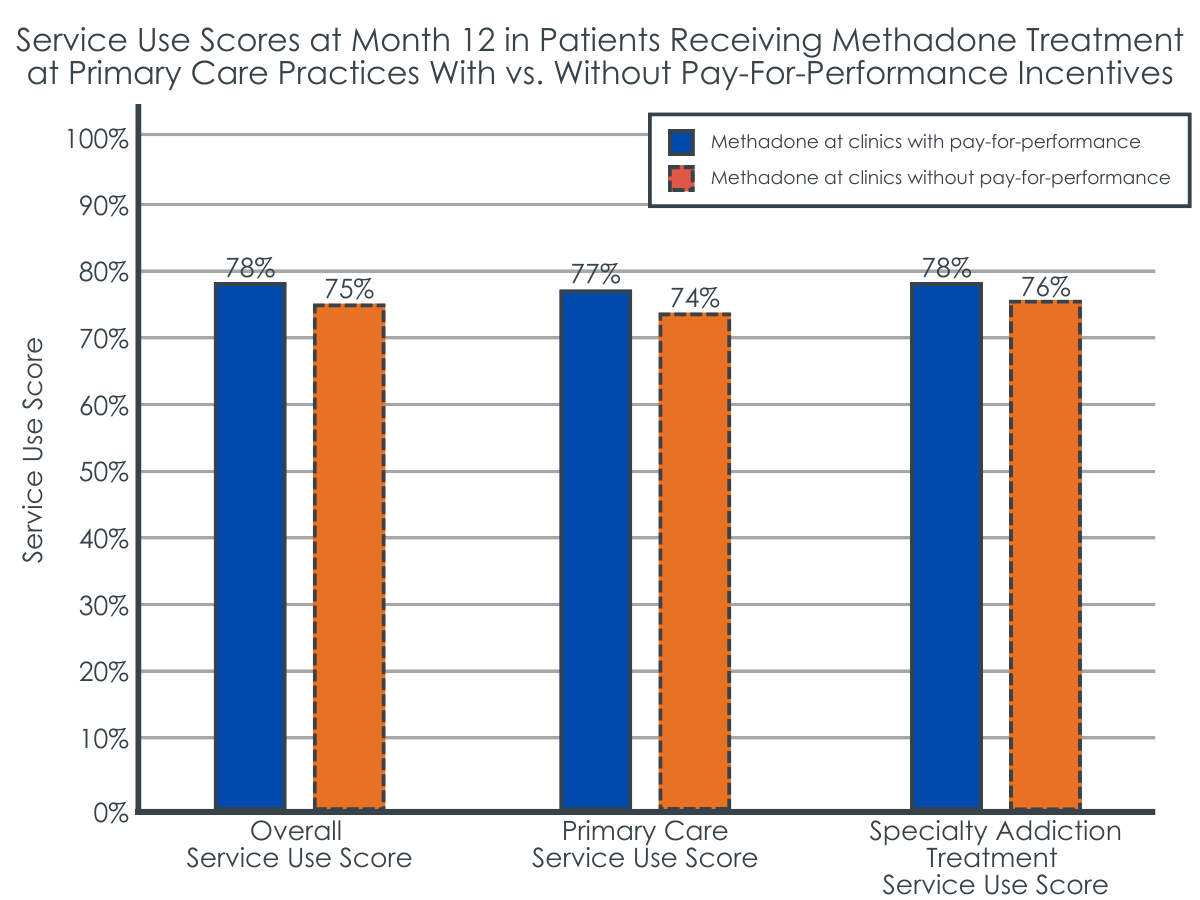
Though patients receiving care at primary care clinics with pay-for-performance incentives had slightly higher service use scores than patients attending primary care clinics without incentives, the difference wasn’t significant.
Figure 3 shows the overall service use scores, primary care service use scores, and specialty addiction treatment service use scores of patients receiving methadone at primary care clinics with vs. without pay-for-performance incentives. Scores range from 0% to 100%, with higher scores indicating greater use of health services that patients were referred to.
Service use was higher for those stable on methadone at the start of the study.
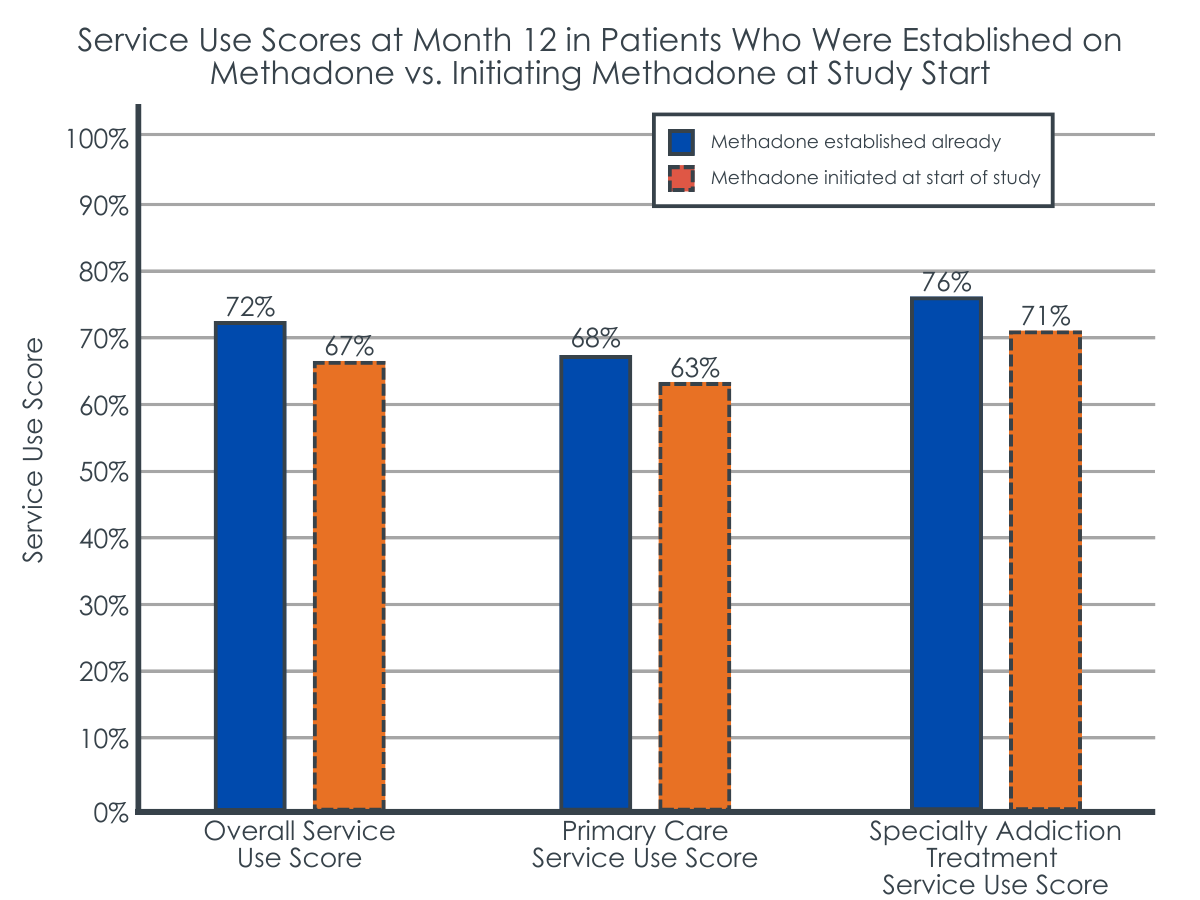
Relative to patients who initiated methadone at the start of the study, patients who were already established on methadone at study start had higher overall service use scores at 12 months. When primary care service use scores and specialty addiction treatment service use scores were evaluated independently, both were significantly higher in the patients who were previously established on methadone.
Figure 4 shows the overall service use scores, primary care service use scores, and specialty treatment service use scores of patients established on methadone compared to those initiating methadone at study start. Scores range from 0% to 100%, with higher scores indicating greater use of health services that patients were referred to.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this randomized trial help us better understand the impact of various healthcare models for opioid use disorder medication treatment on patient care. This research is important because it can ultimately help identify various treatment models that may help expand access to medication treatment for opioid use disorder, while ensuring patients get comprehensive medical care. Findings suggest that the provision of methadone in primary care practices may be a helpful strategy for expanding access to and utilization of care that addresses both opioid use disorder and related health conditions.
Importantly, however, this study was conducted in Ukraine where methadone can be legally dispensed to patients at primary care clinics and all primary care clinic staff received addiction medicine training with ongoing videoconference based clinical care support (i.e., “ECHO“). limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise. The state-of-the-art training and clinical support provided to primary care clinics in this study was also not representative of standard primary care practices in Ukraine (or the United States) and may have put the specialty programs at a disadvantage. Additional research is needed to determine if these findings are consistent in other primary care practices, including standard practices without specialty training and ongoing clinical support, and with different medications (e.g., buprenorphine).
Compared to treatment at a specialty addiction clinic, integrated opioid agonist treatment at primary care clinics (i.e., methadone treatment) resulted in patients using more healthcare services that were recommended by their doctors. Patients receiving treatment at a primary care practice used more specialty care services (e.g., HIV and tuberculosis screening) as well as more primary care services (e.g., medical exams and cardiograms). Thus, patients appear to receive more comprehensive healthcare when they receive medication treatment and primary care in a single primary care location.
Findings are consistent with prior research showing that integrated care at a single site improves treatment completion rates and promotes positive addiction outcomes. Individuals with opioid use disorder often have complex needs, including co-occurring mental and physical health conditions, with many requiring treatments for conditions like HIV, hepatitis, and depression. Receiving treatment in a primary care setting allows for the early detection and treatment of these conditions alongside the treatment of opioid use disorder, which can help improve ease of access and ultimately the overall health of patients.
Specialty addiction treatment programs do not typically provide all of the healthcare services that primary care practices are able to offer and patient referrals to outside services may not be enough to get patients the care they need. Left untreated, some health conditions can prove to be disabling or even life threatening. The convenience of receiving opioid agonist treatment and primary care in a single location might help to facilitate patient engagement in their own healthcare and obtain the services they need. Opioid use disorder treatment outcomes were not reported here, however, and additional research is needed to determine which treatment settings are better at retaining patients on medication treatment and improving rates of remission/recovery.
Patients stable on methadone treatment at study start used more recommended services than patients initiating methadone. Other research suggests that health, well-being, and functioning improve with time on opioid use disorder medications. As patients continue their treatment, the more immediate demands of addressing their addiction might subside, and patients may have more time and energy to focus on addressing other health conditions once they are stabilized on their medication.
Interestingly, pay-for-performance incentives for promoting service use among patients at primary care clinics did not significantly affect healthcare service use. With physicians having particularly low salaries in Ukraine, it is somewhat surprising that financial incentives to engage patients’ healthcare services did not help to increase patient service use. Payment structures may be important to consider in the context of provider incentives. For example, providers may need increased incentives over time, larger, or more frequent payments to motivate their patient care behaviors, and in turn, affect their patient’s behavior. Incentives that align with patients’ treatment goals may also be important to ensure that incentives don’t lead to worse patient outcomes. However, research on the effectiveness of pay-for-performance incentives is mixed, with effects varying by how incentives are designed and the context they are used in.
Given that Ukraine recently created a National Health Service to pay some clinics incentives based on the number of patients and type of care they provide to patients, additional research is needed to determine ideal pay-for-performance models in different treatment settings that promote high quality care and positive patient outcomes.
This study was conducted in Ukraine, where methadone treatment is permitted in primary care practices. Findings may not apply to other countries with different opioid agonist treatment and healthcare models.
This study was an interim analysis, conducted as part of data safety and monitoring to assess self-reported outcomes. Thus, the study may be underpowered to detect group differences (i.e., not having enough study participants to statistically detect differences if they are present).
Over 90% of the study sample was retained on methadone treatment for 12 months. Given higher rates of treatment drop-out observed in other investigations and in other countries, this population may have been particularly motivated to remain in treatment which may have influenced outcomes.
Whereas this study examines utilization of health care services related to patients receiving methadone in either specialty addiction treatment settings or an addiction-trained primary care setting clinic setting, this study does not report on actual opioid use disorder outcomes or remission rates so it is unclear whether one setting is better or worse at helping patients achieve remission or reduce associated harms and consequences from their opioid use disorder. It also did not report on actual health outcomes related to use of the health services to help answer whether patients that used more health services actually had better health related outcomes.
BOTTOM LINE
Relative to patients who received methadone at specialty addiction treatment clinics, patients who received integrated methadone treatment with ongoing, videoconference-based clinical support at primary care clinics in Ukraine used more healthcare services that were recommended by their doctors, including both specialty and primary care services. Pay-for-performance incentives did not significantly affect healthcare service use among patients. Patients established on methadone at the start of the study used more recommended healthcare services than patients initiating methadone. This study helps us better understand the potential benefits of opioid use disorder medication treatment when delivered in real-world healthcare settings with different healthcare delivery models and among patients with different treatment durations. Enhancing our understanding of the effects of various treatment delivery models for opioid use disorder medication will ultimately help guide healthcare system approaches and best practices for improving patients’ care to support their general physical health and addiction-specific outcomes.
For individuals and families seeking recovery: Opioid agonist treatments like buprenorphine and methadone are helpful in addressing opioid use disorder. These medications are delivered in various healthcare settings, including specialty addiction treatment programs and primary care settings. Though methadone treatment is not available in primary care practices in the US, buprenorphine treatment is available. Receiving buprenorphine treatment in a primary care setting may be a good option for patients who have co-occurring medical conditions that need to be addressed, or who want the convenience of receiving healthcare in a single location. Additional research will help identify whether receiving medication treatment in a primary care setting versus a specialty clinic produces better opioid use disorder outcomes.
For treatment professionals and treatment systems: Integrating opioid agonist treatment into primary care practices may be a good way to increase patient use of healthcare services that prevent and treat medical conditions that commonly co-occur with addiction. Patients seeking convenient options for comprehensive healthcare and patients with co-occurring conditions requiring medical attention may benefit from in-office opioid agonist treatment where they can address all aspects of their health in one location.
For scientists: It is essential to conduct additional longitudinal investigations of healthcare system models for opioid agonist treatment delivery and their effect on healthcare quality, patient care, and outcomes. Evaluation of additional services (e.g., mental health, dental) and patient outcomes (e.g., opioid use disorder remission, recovery capital, well-being, quality of life), as well as clinical and demographic moderators, are needed to enhance clinical practice and ensure patients are receiving the comprehensive care they need for the greatest gains in recovery and health outcomes. Studies of integrated buprenorphine and methadone treatment in primary care among patients at different treatment stages with various levels of motivation for treatment and recovery, and in additional countries with different treatment models are also needed.
For policy makers: Compared to opioid use disorder medication treatment at specialty addiction treatment clinics, medication treatment in primary care settings may be a more convenient treatment option for at least some patients with opioid use disorder, which might help to encourage healthcare service use among patients and subsequently promote their mental and physical health alongside their addiction recovery. However, we still have a limited understanding of the best medication treatment delivery models for high quality patient care and positive patient outcomes and opioid use disorder specific outcomes (e.g., remission, reductions in OUD related harms) were not reported so it is unclear from this study which setting is better at effecting most change in these outcomes. Additional research funding will help identify the healthcare models that best support opioid use disorder medication treatment delivery, and for whom different models might work best, to guide clinical recommendations and enhance patient outcomes.
Initiatives to expand access to medication treatments for opioid use disorder (e.g., buprenorphine, methadone) have increased globally. Towards this end, Ukraine recently changed their laws around opioid use disorder medication treatments, allowing for the delivery of methadone in general medical settings like primary care practices. Research supports the integration of opioid use disorder medication treatment into primary care practices for improving patient outcomes. However, additional research is needed to examine whether integrated healthcare models can better help patients obtain the comprehensive care they need, including specialty care like addiction treatment as well as primary care like regular medical exams and hepatitis treatment.
Examining whether patients use the healthcare services that their providers recommend can highlight the impact of integrated treatment on patient care. The impact of integrated healthcare models on patient care and service use in Ukraine is not yet clear. In addition to efforts that expand access to medication treatment, efforts are needed to ensure optimal quality of care. ‘Pay-for-performance’ is a practice in which healthcare providers are paid based on their care delivery and whether optimal patient outcomes are achieved, with the goal of improving the quality and efficiency of care. Pay-for-performance incentives are recommended by the World Health Organization and the Institute of Medicine to improve quality of care, but they are not yet widely used in Ukraine and studies are needed to determine the impact of incentives on healthcare delivery and outcomes.
Studying the impact of integrated healthcare and pay-for-performance models on patients’ healthcare service use can help guide healthcare systems to implement ideal service models that comprehensively support overall patient health in addition to opioid use disorder treatment. To examine the new integrated healthcare model implemented in Ukraine for individuals with opioid use disorder, this randomized trial evaluated the impact of integrated methadone, pay-for-performance incentives, and the duration of medication treatment on patients’ use of healthcare services recommended by their providers.
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal multi-site trial to examine healthcare service use among individuals with opioid use disorder who were randomized to receive methadone treatment at specialty addiction treatment clinics or primary care clinics throughout Ukraine. Nine-hundred and ninety adults seeking or receiving medication treatment were recruited from specialty addiction treatment clinics in nine regions across Ukraine.
Participants were randomly assigned to one of three conditions: (1) methadone treatment at a specialty addiction treatment clinic, the current standard of care in Ukraine; (2) methadone treatment at a primary care clinic with pay-for-performance incentives for physicians; (3) methadone treatment at a primary care clinic without pay-for-performance incentives for physicians.
The researchers randomly assigned primary care clinics to receive pay-for-performance incentives or to not receive these incentives. Participants who were randomized to receive care at a primary care clinic were able to choose their preferred primary care clinic from a list, but were not told (i.e., “blinded”) if the clinic they selected offered pay-for-performance incentives. Clinic type and incentives were balanced across geographic regions.
All clinic staff at primary care practices had completed two three-day training courses (including clinical didactic and case presentations) on opioid agonist treatment, HIV and tuberculosis, ECHO-Integrated Care, and quality improvement strategies. Clinicians at primary care clinics that were randomly assigned to receive pay-for-performance incentives were informed that they could receive a financial monthly bonus depending on the number of healthcare service activities that their patients were referred to and actually completed.
Participants completed self-report questionnaires upon enrolling in the study (baseline), and 6- and 12-months after baseline. Questions were developed using Ukraine Ministry of Health guidelines and national/international experts and concerned healthcare service use in the past 6 months.
An overall service use score was calculated for each participant by dividing the number of services the patient was recommended and completed/used, by the number of services the patient was recommended, and multiplying by 100 to obtain a percentage of services used.
Services included primary care and specialty treatment services (outlined in table below). The same procedure was used to calculate service use scores for: (1) primary care services only (i.e. dividing the number of primary care services the patient was recommended and completed, by the number of primary care services the patient was recommended, and multiplying by 100); (2) specialty care services only (i.e. dividing the number of specialty treatment services the patient was recommended and completed, by the number of specialty treatment services the patient was recommended, and multiplying by 100). All scores ranged from a minimum of 0% to a maximum of 100% and were based on participant questionnaires completed at the 12-month follow-up (i.e., 12 months after beginning the study).
The researchers compared service use scores at month-12 follow up between: (1) patients assigned to primary care clinics vs. patients assigned to specialty care clinics; (2) patients assigned to primary care clinics with vs. without pay-for-performance incentives; (3) patients already established on methadone for 3 or more months at study start vs. patients initiating methadone at study start.
After accounting for participants were unable to be contacted at the follow up timepoints, a total of 818 people were included in analyses concerning healthcare service use (n=291 assigned to specialty treatment clinics; n=527 assigned to primary care clinics). All participants had a history of injection drug use and a diagnosis of opioid use disorder (per the International Classification of Diseases 10 criteria for opioid dependence).
All participants were advised to seek primary care services at their local clinics, regardless of group assignment. Sixty-one percent of participants were already receiving methadone for three or more months at study start, while 39% were newly initiating methadone. Over 90% of participants were still receiving methadone treatment at month-12 follow up. The majority of participants were men (82%) in their early 40’s. About half of the sample was unemployed, had HIV, and hepatitis-C, and about one-third had income below the poverty level. Characteristics did not differ between participants randomized to different groups.
WHAT DID THIS STUDY FIND?
Service use was higher for patients assigned to a primary care practice irrespective of pay-for-performance.
Relative to patients who received methadone from a specialty treatment clinic, patients who received methadone from a primary care clinic had higher overall service use scores at 12 months. When primary care service use scores and specialty treatment service use scores were evaluated independently, both were significantly higher in the group that received treatment at a primary care clinic.
Figure 2 shows the overall service use scores, primary care service use scores, and specialty addiction treatment service use scores of patients receiving methadone at primary care clinics vs. specialty addiction treatment clinics. Scores range from 0% to 100%, with higher scores indicating greater use of healthcare services that patients were referred to.
Though patients receiving care at primary care clinics with pay-for-performance incentives had slightly higher service use scores than patients attending primary care clinics without incentives, the difference wasn’t significant.
Figure 3 shows the overall service use scores, primary care service use scores, and specialty addiction treatment service use scores of patients receiving methadone at primary care clinics with vs. without pay-for-performance incentives. Scores range from 0% to 100%, with higher scores indicating greater use of health services that patients were referred to.
Service use was higher for those stable on methadone at the start of the study.
Relative to patients who initiated methadone at the start of the study, patients who were already established on methadone at study start had higher overall service use scores at 12 months. When primary care service use scores and specialty addiction treatment service use scores were evaluated independently, both were significantly higher in the patients who were previously established on methadone.
Figure 4 shows the overall service use scores, primary care service use scores, and specialty treatment service use scores of patients established on methadone compared to those initiating methadone at study start. Scores range from 0% to 100%, with higher scores indicating greater use of health services that patients were referred to.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this randomized trial help us better understand the impact of various healthcare models for opioid use disorder medication treatment on patient care. This research is important because it can ultimately help identify various treatment models that may help expand access to medication treatment for opioid use disorder, while ensuring patients get comprehensive medical care. Findings suggest that the provision of methadone in primary care practices may be a helpful strategy for expanding access to and utilization of care that addresses both opioid use disorder and related health conditions.
Importantly, however, this study was conducted in Ukraine where methadone can be legally dispensed to patients at primary care clinics and all primary care clinic staff received addiction medicine training with ongoing videoconference based clinical care support (i.e., “ECHO“). limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise. The state-of-the-art training and clinical support provided to primary care clinics in this study was also not representative of standard primary care practices in Ukraine (or the United States) and may have put the specialty programs at a disadvantage. Additional research is needed to determine if these findings are consistent in other primary care practices, including standard practices without specialty training and ongoing clinical support, and with different medications (e.g., buprenorphine).
Compared to treatment at a specialty addiction clinic, integrated opioid agonist treatment at primary care clinics (i.e., methadone treatment) resulted in patients using more healthcare services that were recommended by their doctors. Patients receiving treatment at a primary care practice used more specialty care services (e.g., HIV and tuberculosis screening) as well as more primary care services (e.g., medical exams and cardiograms). Thus, patients appear to receive more comprehensive healthcare when they receive medication treatment and primary care in a single primary care location.
Findings are consistent with prior research showing that integrated care at a single site improves treatment completion rates and promotes positive addiction outcomes. Individuals with opioid use disorder often have complex needs, including co-occurring mental and physical health conditions, with many requiring treatments for conditions like HIV, hepatitis, and depression. Receiving treatment in a primary care setting allows for the early detection and treatment of these conditions alongside the treatment of opioid use disorder, which can help improve ease of access and ultimately the overall health of patients.
Specialty addiction treatment programs do not typically provide all of the healthcare services that primary care practices are able to offer and patient referrals to outside services may not be enough to get patients the care they need. Left untreated, some health conditions can prove to be disabling or even life threatening. The convenience of receiving opioid agonist treatment and primary care in a single location might help to facilitate patient engagement in their own healthcare and obtain the services they need. Opioid use disorder treatment outcomes were not reported here, however, and additional research is needed to determine which treatment settings are better at retaining patients on medication treatment and improving rates of remission/recovery.
Patients stable on methadone treatment at study start used more recommended services than patients initiating methadone. Other research suggests that health, well-being, and functioning improve with time on opioid use disorder medications. As patients continue their treatment, the more immediate demands of addressing their addiction might subside, and patients may have more time and energy to focus on addressing other health conditions once they are stabilized on their medication.
Interestingly, pay-for-performance incentives for promoting service use among patients at primary care clinics did not significantly affect healthcare service use. With physicians having particularly low salaries in Ukraine, it is somewhat surprising that financial incentives to engage patients’ healthcare services did not help to increase patient service use. Payment structures may be important to consider in the context of provider incentives. For example, providers may need increased incentives over time, larger, or more frequent payments to motivate their patient care behaviors, and in turn, affect their patient’s behavior. Incentives that align with patients’ treatment goals may also be important to ensure that incentives don’t lead to worse patient outcomes. However, research on the effectiveness of pay-for-performance incentives is mixed, with effects varying by how incentives are designed and the context they are used in.
Given that Ukraine recently created a National Health Service to pay some clinics incentives based on the number of patients and type of care they provide to patients, additional research is needed to determine ideal pay-for-performance models in different treatment settings that promote high quality care and positive patient outcomes.
This study was conducted in Ukraine, where methadone treatment is permitted in primary care practices. Findings may not apply to other countries with different opioid agonist treatment and healthcare models.
This study was an interim analysis, conducted as part of data safety and monitoring to assess self-reported outcomes. Thus, the study may be underpowered to detect group differences (i.e., not having enough study participants to statistically detect differences if they are present).
Over 90% of the study sample was retained on methadone treatment for 12 months. Given higher rates of treatment drop-out observed in other investigations and in other countries, this population may have been particularly motivated to remain in treatment which may have influenced outcomes.
Whereas this study examines utilization of health care services related to patients receiving methadone in either specialty addiction treatment settings or an addiction-trained primary care setting clinic setting, this study does not report on actual opioid use disorder outcomes or remission rates so it is unclear whether one setting is better or worse at helping patients achieve remission or reduce associated harms and consequences from their opioid use disorder. It also did not report on actual health outcomes related to use of the health services to help answer whether patients that used more health services actually had better health related outcomes.
BOTTOM LINE
Relative to patients who received methadone at specialty addiction treatment clinics, patients who received integrated methadone treatment with ongoing, videoconference-based clinical support at primary care clinics in Ukraine used more healthcare services that were recommended by their doctors, including both specialty and primary care services. Pay-for-performance incentives did not significantly affect healthcare service use among patients. Patients established on methadone at the start of the study used more recommended healthcare services than patients initiating methadone. This study helps us better understand the potential benefits of opioid use disorder medication treatment when delivered in real-world healthcare settings with different healthcare delivery models and among patients with different treatment durations. Enhancing our understanding of the effects of various treatment delivery models for opioid use disorder medication will ultimately help guide healthcare system approaches and best practices for improving patients’ care to support their general physical health and addiction-specific outcomes.
For individuals and families seeking recovery: Opioid agonist treatments like buprenorphine and methadone are helpful in addressing opioid use disorder. These medications are delivered in various healthcare settings, including specialty addiction treatment programs and primary care settings. Though methadone treatment is not available in primary care practices in the US, buprenorphine treatment is available. Receiving buprenorphine treatment in a primary care setting may be a good option for patients who have co-occurring medical conditions that need to be addressed, or who want the convenience of receiving healthcare in a single location. Additional research will help identify whether receiving medication treatment in a primary care setting versus a specialty clinic produces better opioid use disorder outcomes.
For treatment professionals and treatment systems: Integrating opioid agonist treatment into primary care practices may be a good way to increase patient use of healthcare services that prevent and treat medical conditions that commonly co-occur with addiction. Patients seeking convenient options for comprehensive healthcare and patients with co-occurring conditions requiring medical attention may benefit from in-office opioid agonist treatment where they can address all aspects of their health in one location.
For scientists: It is essential to conduct additional longitudinal investigations of healthcare system models for opioid agonist treatment delivery and their effect on healthcare quality, patient care, and outcomes. Evaluation of additional services (e.g., mental health, dental) and patient outcomes (e.g., opioid use disorder remission, recovery capital, well-being, quality of life), as well as clinical and demographic moderators, are needed to enhance clinical practice and ensure patients are receiving the comprehensive care they need for the greatest gains in recovery and health outcomes. Studies of integrated buprenorphine and methadone treatment in primary care among patients at different treatment stages with various levels of motivation for treatment and recovery, and in additional countries with different treatment models are also needed.
For policy makers: Compared to opioid use disorder medication treatment at specialty addiction treatment clinics, medication treatment in primary care settings may be a more convenient treatment option for at least some patients with opioid use disorder, which might help to encourage healthcare service use among patients and subsequently promote their mental and physical health alongside their addiction recovery. However, we still have a limited understanding of the best medication treatment delivery models for high quality patient care and positive patient outcomes and opioid use disorder specific outcomes (e.g., remission, reductions in OUD related harms) were not reported so it is unclear from this study which setting is better at effecting most change in these outcomes. Additional research funding will help identify the healthcare models that best support opioid use disorder medication treatment delivery, and for whom different models might work best, to guide clinical recommendations and enhance patient outcomes.
Initiatives to expand access to medication treatments for opioid use disorder (e.g., buprenorphine, methadone) have increased globally. Towards this end, Ukraine recently changed their laws around opioid use disorder medication treatments, allowing for the delivery of methadone in general medical settings like primary care practices. Research supports the integration of opioid use disorder medication treatment into primary care practices for improving patient outcomes. However, additional research is needed to examine whether integrated healthcare models can better help patients obtain the comprehensive care they need, including specialty care like addiction treatment as well as primary care like regular medical exams and hepatitis treatment.
Examining whether patients use the healthcare services that their providers recommend can highlight the impact of integrated treatment on patient care. The impact of integrated healthcare models on patient care and service use in Ukraine is not yet clear. In addition to efforts that expand access to medication treatment, efforts are needed to ensure optimal quality of care. ‘Pay-for-performance’ is a practice in which healthcare providers are paid based on their care delivery and whether optimal patient outcomes are achieved, with the goal of improving the quality and efficiency of care. Pay-for-performance incentives are recommended by the World Health Organization and the Institute of Medicine to improve quality of care, but they are not yet widely used in Ukraine and studies are needed to determine the impact of incentives on healthcare delivery and outcomes.
Studying the impact of integrated healthcare and pay-for-performance models on patients’ healthcare service use can help guide healthcare systems to implement ideal service models that comprehensively support overall patient health in addition to opioid use disorder treatment. To examine the new integrated healthcare model implemented in Ukraine for individuals with opioid use disorder, this randomized trial evaluated the impact of integrated methadone, pay-for-performance incentives, and the duration of medication treatment on patients’ use of healthcare services recommended by their providers.
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal multi-site trial to examine healthcare service use among individuals with opioid use disorder who were randomized to receive methadone treatment at specialty addiction treatment clinics or primary care clinics throughout Ukraine. Nine-hundred and ninety adults seeking or receiving medication treatment were recruited from specialty addiction treatment clinics in nine regions across Ukraine.
Participants were randomly assigned to one of three conditions: (1) methadone treatment at a specialty addiction treatment clinic, the current standard of care in Ukraine; (2) methadone treatment at a primary care clinic with pay-for-performance incentives for physicians; (3) methadone treatment at a primary care clinic without pay-for-performance incentives for physicians.
The researchers randomly assigned primary care clinics to receive pay-for-performance incentives or to not receive these incentives. Participants who were randomized to receive care at a primary care clinic were able to choose their preferred primary care clinic from a list, but were not told (i.e., “blinded”) if the clinic they selected offered pay-for-performance incentives. Clinic type and incentives were balanced across geographic regions.
All clinic staff at primary care practices had completed two three-day training courses (including clinical didactic and case presentations) on opioid agonist treatment, HIV and tuberculosis, ECHO-Integrated Care, and quality improvement strategies. Clinicians at primary care clinics that were randomly assigned to receive pay-for-performance incentives were informed that they could receive a financial monthly bonus depending on the number of healthcare service activities that their patients were referred to and actually completed.
Participants completed self-report questionnaires upon enrolling in the study (baseline), and 6- and 12-months after baseline. Questions were developed using Ukraine Ministry of Health guidelines and national/international experts and concerned healthcare service use in the past 6 months.
An overall service use score was calculated for each participant by dividing the number of services the patient was recommended and completed/used, by the number of services the patient was recommended, and multiplying by 100 to obtain a percentage of services used.
Services included primary care and specialty treatment services (outlined in table below). The same procedure was used to calculate service use scores for: (1) primary care services only (i.e. dividing the number of primary care services the patient was recommended and completed, by the number of primary care services the patient was recommended, and multiplying by 100); (2) specialty care services only (i.e. dividing the number of specialty treatment services the patient was recommended and completed, by the number of specialty treatment services the patient was recommended, and multiplying by 100). All scores ranged from a minimum of 0% to a maximum of 100% and were based on participant questionnaires completed at the 12-month follow-up (i.e., 12 months after beginning the study).
The researchers compared service use scores at month-12 follow up between: (1) patients assigned to primary care clinics vs. patients assigned to specialty care clinics; (2) patients assigned to primary care clinics with vs. without pay-for-performance incentives; (3) patients already established on methadone for 3 or more months at study start vs. patients initiating methadone at study start.
After accounting for participants were unable to be contacted at the follow up timepoints, a total of 818 people were included in analyses concerning healthcare service use (n=291 assigned to specialty treatment clinics; n=527 assigned to primary care clinics). All participants had a history of injection drug use and a diagnosis of opioid use disorder (per the International Classification of Diseases 10 criteria for opioid dependence).
All participants were advised to seek primary care services at their local clinics, regardless of group assignment. Sixty-one percent of participants were already receiving methadone for three or more months at study start, while 39% were newly initiating methadone. Over 90% of participants were still receiving methadone treatment at month-12 follow up. The majority of participants were men (82%) in their early 40’s. About half of the sample was unemployed, had HIV, and hepatitis-C, and about one-third had income below the poverty level. Characteristics did not differ between participants randomized to different groups.
WHAT DID THIS STUDY FIND?
Service use was higher for patients assigned to a primary care practice irrespective of pay-for-performance.
Relative to patients who received methadone from a specialty treatment clinic, patients who received methadone from a primary care clinic had higher overall service use scores at 12 months. When primary care service use scores and specialty treatment service use scores were evaluated independently, both were significantly higher in the group that received treatment at a primary care clinic.
Figure 2 shows the overall service use scores, primary care service use scores, and specialty addiction treatment service use scores of patients receiving methadone at primary care clinics vs. specialty addiction treatment clinics. Scores range from 0% to 100%, with higher scores indicating greater use of healthcare services that patients were referred to.
Though patients receiving care at primary care clinics with pay-for-performance incentives had slightly higher service use scores than patients attending primary care clinics without incentives, the difference wasn’t significant.
Figure 3 shows the overall service use scores, primary care service use scores, and specialty addiction treatment service use scores of patients receiving methadone at primary care clinics with vs. without pay-for-performance incentives. Scores range from 0% to 100%, with higher scores indicating greater use of health services that patients were referred to.
Service use was higher for those stable on methadone at the start of the study.
Relative to patients who initiated methadone at the start of the study, patients who were already established on methadone at study start had higher overall service use scores at 12 months. When primary care service use scores and specialty addiction treatment service use scores were evaluated independently, both were significantly higher in the patients who were previously established on methadone.
Figure 4 shows the overall service use scores, primary care service use scores, and specialty treatment service use scores of patients established on methadone compared to those initiating methadone at study start. Scores range from 0% to 100%, with higher scores indicating greater use of health services that patients were referred to.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this randomized trial help us better understand the impact of various healthcare models for opioid use disorder medication treatment on patient care. This research is important because it can ultimately help identify various treatment models that may help expand access to medication treatment for opioid use disorder, while ensuring patients get comprehensive medical care. Findings suggest that the provision of methadone in primary care practices may be a helpful strategy for expanding access to and utilization of care that addresses both opioid use disorder and related health conditions.
Importantly, however, this study was conducted in Ukraine where methadone can be legally dispensed to patients at primary care clinics and all primary care clinic staff received addiction medicine training with ongoing videoconference based clinical care support (i.e., “ECHO“). limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise. The state-of-the-art training and clinical support provided to primary care clinics in this study was also not representative of standard primary care practices in Ukraine (or the United States) and may have put the specialty programs at a disadvantage. Additional research is needed to determine if these findings are consistent in other primary care practices, including standard practices without specialty training and ongoing clinical support, and with different medications (e.g., buprenorphine).
Compared to treatment at a specialty addiction clinic, integrated opioid agonist treatment at primary care clinics (i.e., methadone treatment) resulted in patients using more healthcare services that were recommended by their doctors. Patients receiving treatment at a primary care practice used more specialty care services (e.g., HIV and tuberculosis screening) as well as more primary care services (e.g., medical exams and cardiograms). Thus, patients appear to receive more comprehensive healthcare when they receive medication treatment and primary care in a single primary care location.
Findings are consistent with prior research showing that integrated care at a single site improves treatment completion rates and promotes positive addiction outcomes. Individuals with opioid use disorder often have complex needs, including co-occurring mental and physical health conditions, with many requiring treatments for conditions like HIV, hepatitis, and depression. Receiving treatment in a primary care setting allows for the early detection and treatment of these conditions alongside the treatment of opioid use disorder, which can help improve ease of access and ultimately the overall health of patients.
Specialty addiction treatment programs do not typically provide all of the healthcare services that primary care practices are able to offer and patient referrals to outside services may not be enough to get patients the care they need. Left untreated, some health conditions can prove to be disabling or even life threatening. The convenience of receiving opioid agonist treatment and primary care in a single location might help to facilitate patient engagement in their own healthcare and obtain the services they need. Opioid use disorder treatment outcomes were not reported here, however, and additional research is needed to determine which treatment settings are better at retaining patients on medication treatment and improving rates of remission/recovery.
Patients stable on methadone treatment at study start used more recommended services than patients initiating methadone. Other research suggests that health, well-being, and functioning improve with time on opioid use disorder medications. As patients continue their treatment, the more immediate demands of addressing their addiction might subside, and patients may have more time and energy to focus on addressing other health conditions once they are stabilized on their medication.
Interestingly, pay-for-performance incentives for promoting service use among patients at primary care clinics did not significantly affect healthcare service use. With physicians having particularly low salaries in Ukraine, it is somewhat surprising that financial incentives to engage patients’ healthcare services did not help to increase patient service use. Payment structures may be important to consider in the context of provider incentives. For example, providers may need increased incentives over time, larger, or more frequent payments to motivate their patient care behaviors, and in turn, affect their patient’s behavior. Incentives that align with patients’ treatment goals may also be important to ensure that incentives don’t lead to worse patient outcomes. However, research on the effectiveness of pay-for-performance incentives is mixed, with effects varying by how incentives are designed and the context they are used in.
Given that Ukraine recently created a National Health Service to pay some clinics incentives based on the number of patients and type of care they provide to patients, additional research is needed to determine ideal pay-for-performance models in different treatment settings that promote high quality care and positive patient outcomes.
This study was conducted in Ukraine, where methadone treatment is permitted in primary care practices. Findings may not apply to other countries with different opioid agonist treatment and healthcare models.
This study was an interim analysis, conducted as part of data safety and monitoring to assess self-reported outcomes. Thus, the study may be underpowered to detect group differences (i.e., not having enough study participants to statistically detect differences if they are present).
Over 90% of the study sample was retained on methadone treatment for 12 months. Given higher rates of treatment drop-out observed in other investigations and in other countries, this population may have been particularly motivated to remain in treatment which may have influenced outcomes.
Whereas this study examines utilization of health care services related to patients receiving methadone in either specialty addiction treatment settings or an addiction-trained primary care setting clinic setting, this study does not report on actual opioid use disorder outcomes or remission rates so it is unclear whether one setting is better or worse at helping patients achieve remission or reduce associated harms and consequences from their opioid use disorder. It also did not report on actual health outcomes related to use of the health services to help answer whether patients that used more health services actually had better health related outcomes.
BOTTOM LINE
Relative to patients who received methadone at specialty addiction treatment clinics, patients who received integrated methadone treatment with ongoing, videoconference-based clinical support at primary care clinics in Ukraine used more healthcare services that were recommended by their doctors, including both specialty and primary care services. Pay-for-performance incentives did not significantly affect healthcare service use among patients. Patients established on methadone at the start of the study used more recommended healthcare services than patients initiating methadone. This study helps us better understand the potential benefits of opioid use disorder medication treatment when delivered in real-world healthcare settings with different healthcare delivery models and among patients with different treatment durations. Enhancing our understanding of the effects of various treatment delivery models for opioid use disorder medication will ultimately help guide healthcare system approaches and best practices for improving patients’ care to support their general physical health and addiction-specific outcomes.
For individuals and families seeking recovery: Opioid agonist treatments like buprenorphine and methadone are helpful in addressing opioid use disorder. These medications are delivered in various healthcare settings, including specialty addiction treatment programs and primary care settings. Though methadone treatment is not available in primary care practices in the US, buprenorphine treatment is available. Receiving buprenorphine treatment in a primary care setting may be a good option for patients who have co-occurring medical conditions that need to be addressed, or who want the convenience of receiving healthcare in a single location. Additional research will help identify whether receiving medication treatment in a primary care setting versus a specialty clinic produces better opioid use disorder outcomes.
For treatment professionals and treatment systems: Integrating opioid agonist treatment into primary care practices may be a good way to increase patient use of healthcare services that prevent and treat medical conditions that commonly co-occur with addiction. Patients seeking convenient options for comprehensive healthcare and patients with co-occurring conditions requiring medical attention may benefit from in-office opioid agonist treatment where they can address all aspects of their health in one location.
For scientists: It is essential to conduct additional longitudinal investigations of healthcare system models for opioid agonist treatment delivery and their effect on healthcare quality, patient care, and outcomes. Evaluation of additional services (e.g., mental health, dental) and patient outcomes (e.g., opioid use disorder remission, recovery capital, well-being, quality of life), as well as clinical and demographic moderators, are needed to enhance clinical practice and ensure patients are receiving the comprehensive care they need for the greatest gains in recovery and health outcomes. Studies of integrated buprenorphine and methadone treatment in primary care among patients at different treatment stages with various levels of motivation for treatment and recovery, and in additional countries with different treatment models are also needed.
For policy makers: Compared to opioid use disorder medication treatment at specialty addiction treatment clinics, medication treatment in primary care settings may be a more convenient treatment option for at least some patients with opioid use disorder, which might help to encourage healthcare service use among patients and subsequently promote their mental and physical health alongside their addiction recovery. However, we still have a limited understanding of the best medication treatment delivery models for high quality patient care and positive patient outcomes and opioid use disorder specific outcomes (e.g., remission, reductions in OUD related harms) were not reported so it is unclear from this study which setting is better at effecting most change in these outcomes. Additional research funding will help identify the healthcare models that best support opioid use disorder medication treatment delivery, and for whom different models might work best, to guide clinical recommendations and enhance patient outcomes.