Buprenorphine in primary care: What patients think
Primary care offers a highly accessible way to expand access to medication treatment for opioid use disorder, but relatively few patients receive treatment in primary care. To better understand the barriers to, and facilitators of, office-based medication treatment, this study examined the treatment experiences of patients receiving buprenorphine in a comprehensive primary care setting.
There has been an increased effort to expand access to medication treatment for opioid use disorder. Primary care practices are highly accessible outlets that can be leveraged to expand access to these medications. Some offer expertise in both mental and physical healthcare with an ability to follow patients over the long-term, and they are geographically more accessible than the more specialized opioid treatment programs. However, few primary care providers offer medication treatment and those who do typically treat a small number of patients. To further expand availability and use of medication treatment in primary care settings, it is important to understand the perspectives and experiences of patients and providers. Obtaining patients’ views on the barriers and facilitators to treatment in primary care can help improve patients’ experiences and improve treatment uptake and retention. This study sought to better understand the experiences of patients receiving buprenorphine treatment for opioid use disorder in a primary care setting with a comprehensive, integrated healthcare model.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of adult outpatients receiving buprenorphine for opioid use disorder in a primary care setting, in which 14 patients completed interviews about their buprenorphine treatment experience. Individuals were recruited between July and August 2021 from a single urban primary care clinic with a comprehensive treatment model.
All participants were actively receiving buprenorphine treatment for opioid use disorder from a primary care physician within the clinic. In addition to opioid use disorder medication treatment, all patients had on-site access to behavioral health specialists, pharmacists, nurses, and case managers as part of their routine primary care. Primary care providers were trained in addiction medicine. The clinic did not have additional funding dedicated to opioid use disorder medication treatment, and none of the clinic staff had protected time dedicated to providing medication treatment or were explicitly trained to facilitate it.
During the interview, participants answered questions about key aspects of primary care treatment. Interviews asked about: (1) the impact of primary care-based medication treatment on overall health, (2) experiences and interactions with their primary care team. Qualitative interviews were analyzed and barriers and facilitators to medication treatment in primary care were identified.
The researchers identified 7 emergent themes in the interviews and selected 5 of the 7 themes that were most relevant to medication treatment and opioid use disorder for data presentation: (1) overall health improvement, (2) team-based healthcare, (3) comparing primary care to specialty addiction treatment, (4) access to opioid use disorder medications, (5) stigma and discrimination. The researchers also gathered data on demographics and treatment histories from patients’ electronic medical records.
A total of 21 patients were asked to participate in the study, of which, 14 were eligible and agreed to participate. On average, participants had received treatment at the clinic for 22 months. All participants had previous experience participating in specialty addiction treatment programs. The majority of participants were White (79%), and middle-aged (average: 45 years old), and about half were men (57%). About one-third (36%) of patients were engaged in behavioral therapy, 43% had used alcohol or other drugs in the past 90 days, and 57% currently used tobacco. Seventy-nine percent of patients had five or more medical diagnoses, including 36% who had chronic hepatitis C and 21% who had comorbid psychiatric diagnoses. None of the participants had HIV.
WHAT DID THIS STUDY FIND?
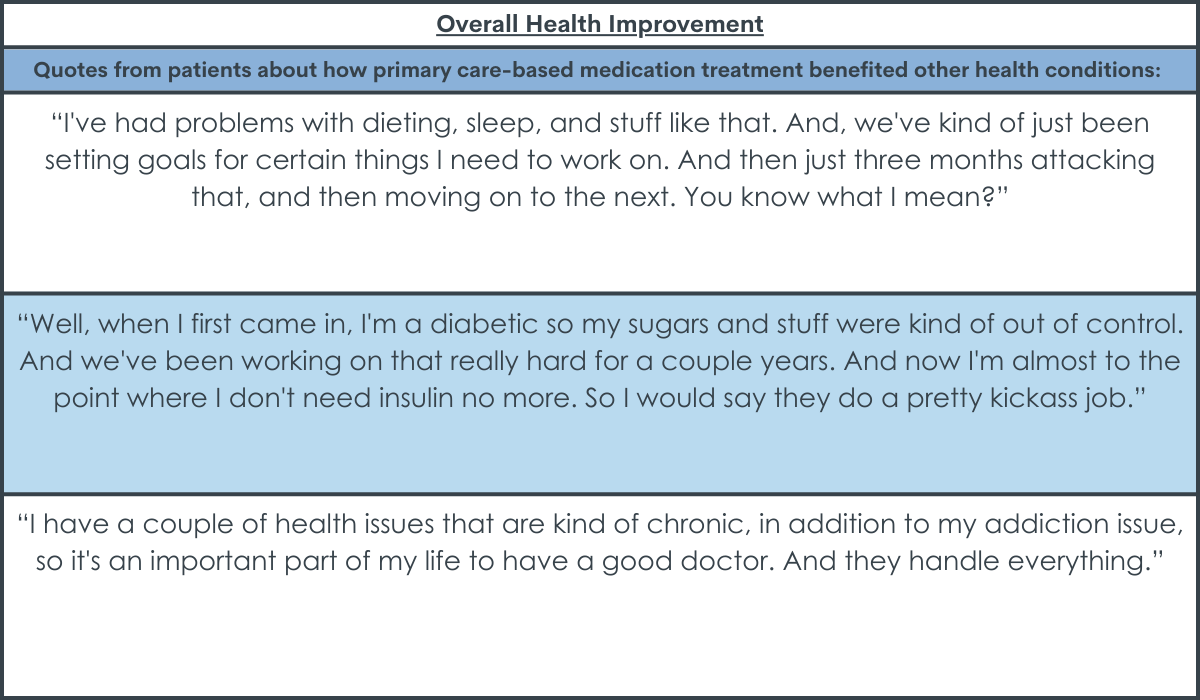
Primary care-based treatment made it easier to get help with other health conditions.
Many patients reported that they didn’t have regular access to a primary care physician before they started receiving buprenorphine treatment in a primary care setting. Once patients started treatment, they were able to address untreated chronic health conditions during regular visits with their primary care provider, including hepatitis C, hypertension, and diabetes. They also liked the convenience of seeing a single doctor for all of their medical needs.
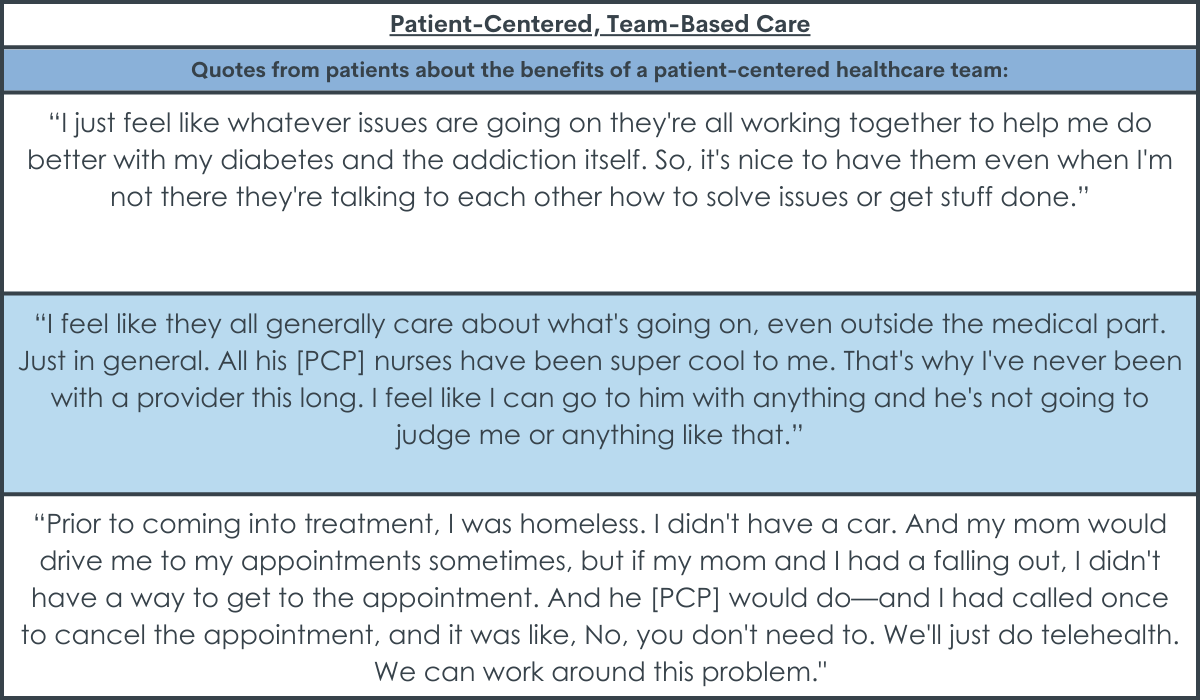
A patient-centered, team-based approach to care made healthcare access more convenient and enjoyable.
Patients mentioned clinic staff in addition to their primary care provider, noting that the team-based approach to their care was convenient and made them feel supported and welcome at the clinic. When patients faced barriers to their care, such as transportation issues or medication-related problems, the care team was easy to reach and willing to work with the patient to help them overcome these barriers. This made it easier to obtain telehealth appointments and avoid interruptions to buprenorphine access.
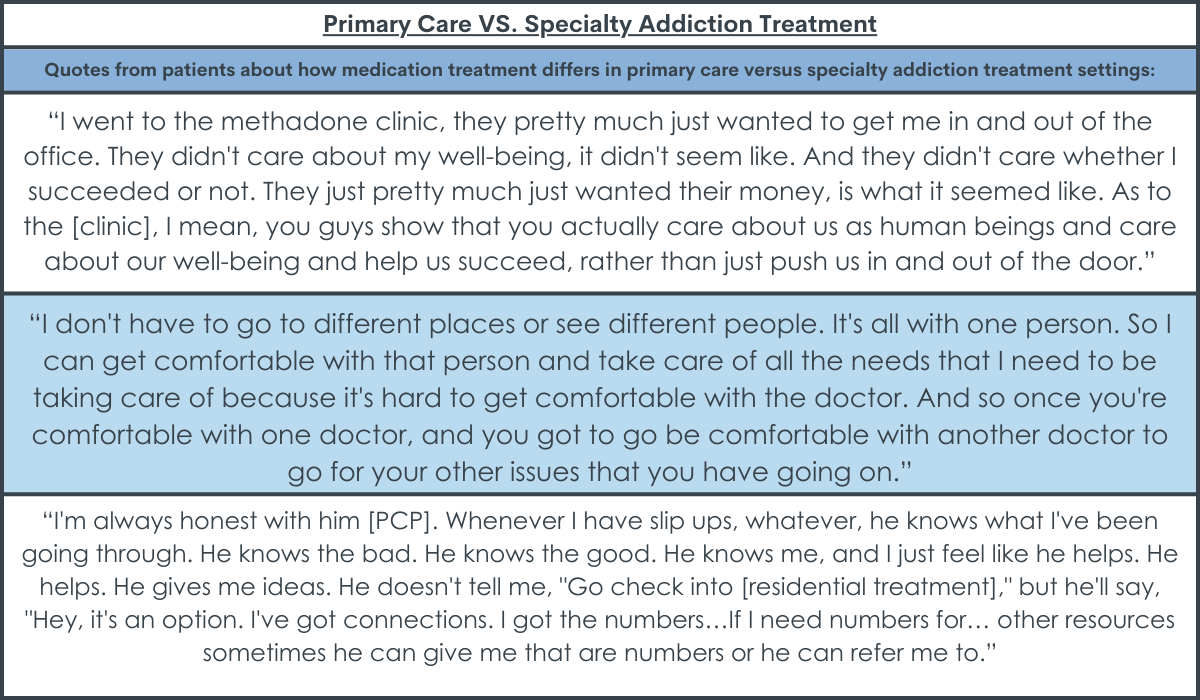
Treatment within primary care was seen as a more personal, private, and trustworthy experience than treatment at a specialty addiction clinic.
Patients felt like the primary care practice valued patients more than specialty addiction programs and made them feel like more than ‘just a number’. They mentioned that the primary care provider explored different treatment options with them instead of pushing medication as the sole ‘cure’ for addiction. Being able to see the same provider at every primary care visit, as opposed to seeing multiple providers at specialty programs, also gave patients a sense of privacy and helped them to build trust with their healthcare team. Primary care teams were also seen as more responsive than specialty clinics, offering quick responses to patient outreach and requests (e.g., requests for refills). Though over one-third of patients used illicit substances at some point over the past three months, none of them felt judged by clinic staff or worried about being dropped from the clinic.
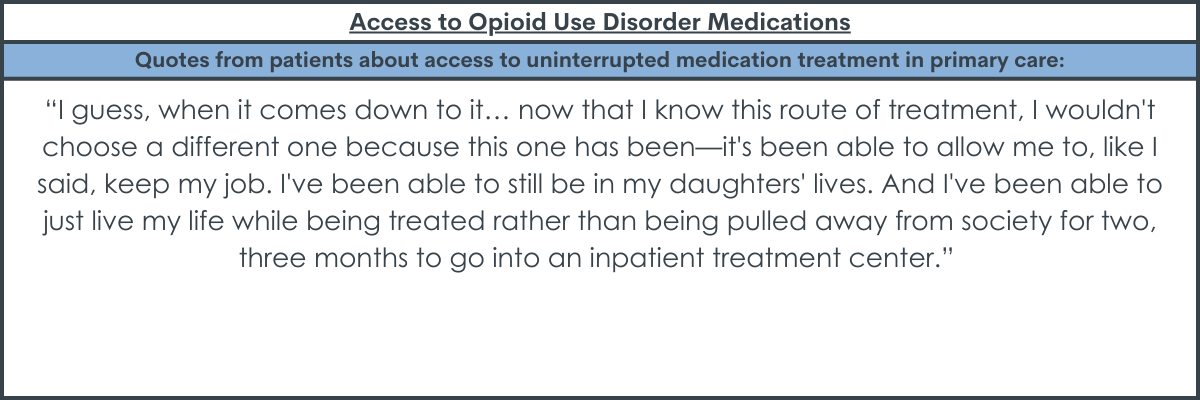
Prioritizing patient access to buprenorphine facilitated uninterrupted treatment and positive medication experiences.
Patients reported that their primary care clinic made buprenorphine access easy by being flexible with treatment and prioritizing access to buprenorphine, even when patients were unable to attend clinic appointments. Medication was seen as a part of patients’ routine care in the primary care setting and patients thought medication treatment was helpful to their recovery. Barriers to uninterrupted buprenorphine access were noted outside of the healthcare setting, including pharmacies that intermittently ran out of buprenorphine.
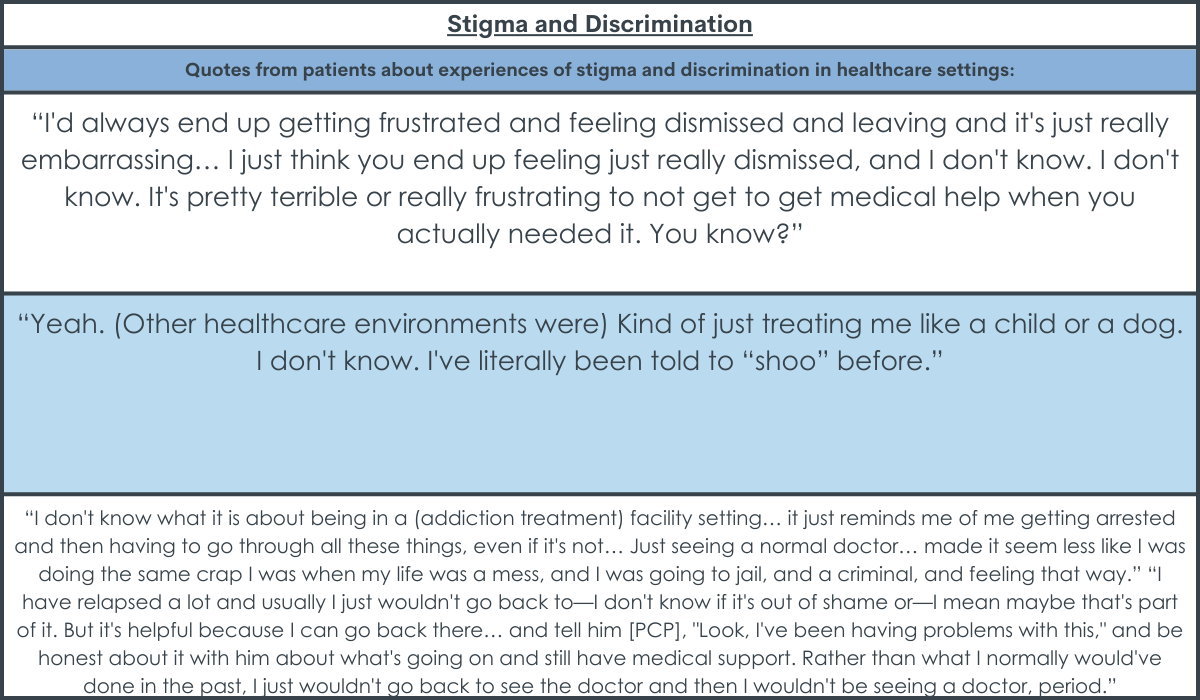
Experiences of stigma and discrimination were common but didn’t occur in the context of their current primary care treatment.
All patients reported prior experiences of stigma and discrimination in other healthcare settings, including being denied routine medical care, being inappropriately questioned about substance use in unrelated healthcare visits, and feeling like they and their health concerns were ignored. Despite these past experiences, none of the patients felt stigmatized or discriminated against by their current primary care team, who made them feel respected and valued.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand some of the experiences of patients receiving buprenorphine treatment in primary care settings and the aspects of healthcare models that may help patients feel supported on their path to recovery. This research is important because it can ultimately help identify various treatment models that help expand access to and engagement in medication treatment for opioid use disorder. Findings suggest that the provision of buprenorphine treatment in comprehensive primary care practices may be a helpful path for expanding access to medication treatment that promotes positive treatment experiences and outcomes among patients with opioid use disorder.
It should be remembered, however, that this study was conducted in a single, academic, primary care practice in an urban setting where primary care providers had addiction medicine training, limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise and to practices in rural settings. The fourteen patients involved in this study were also undergoing treatment for an average of almost 2 years, reflecting a small cohort of more stable patients who have had long-term success with buprenorphine treatment. Additional research is needed to determine if these findings are consistent in other more typical primary care practices and among individuals who have less time in treatment.
Treatment in a primary care setting allowed patients to address their untreated chronic health conditions (e.g., Hepatitis-C, diabetes, hypertension) in addition to their opioid use disorder, resulting in improvements in overall health and wellbeing. Individuals with opioid use disorder often have complex needs, including co-occurring psychiatric and physical health conditions, with many requiring treatment for chronic conditions like HIV, Hepatitis-C, and depression. Receiving treatment from a primary care provider allows for the evaluation and treatment of these conditions alongside opioid medication treatment, which improves the chances of a more holistic recovery that includes physical and mental health. Opioid treatment programs do not typically offer comprehensive care like this, and physical health conditions might go untreated as a result. Providing buprenorphine in primary care settings might help address high rates of chronic, sometimes life threatening, health conditions among this population to improve all aspects of health during treatment.
Many patients felt like the primary care setting allowed for a more personal experience in which healthcare providers and staff made them feel valued as a patient and a person. They liked that they were able to develop a trusting rapport with a single doctor who could conveniently tend to all of their medical needs in one location, both within and outside the confines of their buprenorphine treatment. Though all patients in this study had past experiences of stigma and discrimination at opioid treatment programs, none felt like they had these experiences at their primary care practice. This is important because stigma plays a key role in patient experiences with health services and decisions to engage in these services. Addressing stigma in the healthcare system will ultimately help support patients’ medication treatment and positive recovery outcomes.
Importantly, this study examined patients in an academic primary care clinic with a comprehensive treatment model that offered on-site access to behavioral health specialists, pharmacists, nurses, and case managers, which is not standard across all primary care practices.
Though few patients used the behavioral health support services offered as part of this treatment model, patients liked the convenience and support of the comprehensive care team and their patient-centered treatment approaches. The integrated care team and their willingness to work with patients to remove barriers to treatment (e.g., transportation issues preventing appointment attendance) helped to ensure that patients’ medication treatment was not interrupted. This patient-centered approach that prioritizes medication treatment, as opposed to rigid models that require abstinence and appointment attendance for medication refills, offers patients flexibility, ensure their ongoing access to medication, and promote treatment retention. The integrated care team also ensured that healthcare providers and staff were easy to reach and quick to respond to patient requests and concerns, which patients liked.
In programs with more rigid rules and requirements, many patients are involuntarily discharged from treatment due to non-compliance with regulations (e.g., lack of abstinence, irregular in-person attendance) or voluntarily leave treatment early because treatment demands are difficult to accommodate with everyday life obligations. Prior research is mixed on the effects of integrated care models on patient outcomes, with some studies revealing similar substance use disorder outcomes in integrated and standard primary care models, and other studies suggesting better patient outcomes with integrated care, such as fewer acute care episodes. Nonetheless, the flexibility offered in this primary care setting appeared to benefit patients’ treatment experiences and may have helped to promote treatment retention.
Expanding access to buprenorphine treatment is important for addressing the opioid epidemic. Until now, providers needed a waiver to prescribe buprenorphine and could only prescribe to a limited number of patients. Recent changes to regulations now mean that providers no longer need this waiver to prescribe buprenorphine, which makes it easier for more primary care doctors to offer opioid use disorder medication treatment. Additional research in this area will help identify ideal buprenorphine treatment models in primary care settings, which can ultimately promote the expansion of buprenorphine provision in primary care.
This study was conducted in a single, academic, primary care practice in an urban setting where primary care providers had addiction medicine training, limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise and to practices in rural settings. Patients in this study were also undergoing treatment for an average of almost 2 years, reflecting a cohort of more stable patients who have had long-term success with buprenorphine treatment. Additional research is needed to determine if these findings are consistent in other primary care practices and among individuals who have less time in treatment.
Only 14 patients were included in this qualitative study and additional qualitative and quantitative research is needed to determine common barriers and facilitators to office-based buprenorphine treatment in the context of different practices, treatment models, and patient characteristics. Because the patients in this study had been on buprenorphine for an average of almost two years, patients who had positive experiences with treatment and clinic staff and decided to remain in treatment might be over-represented in this study and additional research is needed to determine whether experiences in primary care settings differ in the earlier stages of treatment.
BOTTOM LINE
Patients receiving buprenorphine treatment at this comprehensive primary care program liked several aspects of their treatment team and experience. The team’s patient-centered and flexible approach to buprenorphine provision ensured ongoing access to medication, and their comprehensive team made it easy to reach a provider in a timely manner and made patients feel valued. Compared to specialized opioid treatment programs, the primary care clinic was seen as less stigmatizing and treatment experiences were reported as more personal, private, and trustworthy. Having a single provider for all healthcare concerns also allowed patients to address their physical health alongside their opioid use disorder. Though additional research is needed in other primary care settings with different treatment models, individuals seeking flexible medication treatment programs that can concurrently address mental and physical health might benefit from buprenorphine treatment within comprehensive patient-centered primary care practices where those are available.
For individuals and families seeking recovery: Individuals who are seeking a medication treatment program with more flexible regulations that prioritize ongoing access to medication treatment may benefit from buprenorphine treatment in a primary care practice that offers an integrated healthcare team willing to accommodate barriers to treatment (e.g., transportation to appointments, ongoing substance use) with patient-centered solutions. Comprehensive primary care practices may also be a helpful option, if available, for patients looking to conveniently address untreated physical and other mental health conditions in a single setting. Primary care practices have different treatment models and not all provide patient-centered comprehensive care. Individuals are encouraged to speak with their current healthcare providers to identify a primary care practice that offers buprenorphine treatment alongside other healthcare program aspects that they might prefer.
For treatment professionals and treatment systems: This study helps us identify the aspects of buprenorphine treatment in primary care practices that patients like, which can help identify factors that promote treatment satisfaction, retention, and outcomes. Treatment professionals and systems might enhance their patients’ treatment experiences by offering a patient-centered approach to care that prioritizes buprenorphine access and accommodates barriers to treatment (e.g., using telehealth when transportation isn’t available). Trying to create a stigma- and discrimination-free practice wherever possible also appears important for positive treatment experiences among patients. In addition, addressing physical and mental health comorbidities alongside opioid use disorder may be an important part of comprehensive treatment and primary care settings might be an ideal place for patients to get this care in a single convenient location. However, these data concern a small group of patients at a single clinic and additional research will help us better understand which aspects of healthcare programs are most important to treatment and recovery.
For scientists:Additional research is needed to extend these findings in different healthcare settings with different treatment models. Studies are needed to determine whether a comprehensive primary care treatment model results in better treatment engagement, retention, and outcomes than specialized opioid treatment programs. Identification of other factors impacting treatment utilization, provision, and outcomes in primary care practices is also needed. Additional research will help identify patient and provider barriers to medication treatment uptake and provision, and address barriers by developing novel ways to expand access to medication treatment. Research among individuals who are in the initiation and beginning stages of treatment (participants in this study were in treatment for 22 months, on average) is also needed to determine if patient experiences differ by treatment duration.
For policy makers: Studies like this help us better understand the components of buprenorphine treatment programs that patients like that may lead to greater patient engagement and retention – a common challenge in opioid treatment. This study noted several aspects of buprenorphine treatment in an integrated primary care practice that patients liked over and above specialized treatment programs and that they found beneficial to their overall health and wellbeing. Additional funding for this area of research will help identify ideal buprenorphine treatment models and whether these may be based within primary care settings. This can ultimately promote optimal provision of buprenorphine treatment, help expand patients’ access to lifesaving medications, and increase treatment engagement to better address the opioid epidemic.
There has been an increased effort to expand access to medication treatment for opioid use disorder. Primary care practices are highly accessible outlets that can be leveraged to expand access to these medications. Some offer expertise in both mental and physical healthcare with an ability to follow patients over the long-term, and they are geographically more accessible than the more specialized opioid treatment programs. However, few primary care providers offer medication treatment and those who do typically treat a small number of patients. To further expand availability and use of medication treatment in primary care settings, it is important to understand the perspectives and experiences of patients and providers. Obtaining patients’ views on the barriers and facilitators to treatment in primary care can help improve patients’ experiences and improve treatment uptake and retention. This study sought to better understand the experiences of patients receiving buprenorphine treatment for opioid use disorder in a primary care setting with a comprehensive, integrated healthcare model.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of adult outpatients receiving buprenorphine for opioid use disorder in a primary care setting, in which 14 patients completed interviews about their buprenorphine treatment experience. Individuals were recruited between July and August 2021 from a single urban primary care clinic with a comprehensive treatment model.
All participants were actively receiving buprenorphine treatment for opioid use disorder from a primary care physician within the clinic. In addition to opioid use disorder medication treatment, all patients had on-site access to behavioral health specialists, pharmacists, nurses, and case managers as part of their routine primary care. Primary care providers were trained in addiction medicine. The clinic did not have additional funding dedicated to opioid use disorder medication treatment, and none of the clinic staff had protected time dedicated to providing medication treatment or were explicitly trained to facilitate it.
During the interview, participants answered questions about key aspects of primary care treatment. Interviews asked about: (1) the impact of primary care-based medication treatment on overall health, (2) experiences and interactions with their primary care team. Qualitative interviews were analyzed and barriers and facilitators to medication treatment in primary care were identified.
The researchers identified 7 emergent themes in the interviews and selected 5 of the 7 themes that were most relevant to medication treatment and opioid use disorder for data presentation: (1) overall health improvement, (2) team-based healthcare, (3) comparing primary care to specialty addiction treatment, (4) access to opioid use disorder medications, (5) stigma and discrimination. The researchers also gathered data on demographics and treatment histories from patients’ electronic medical records.
A total of 21 patients were asked to participate in the study, of which, 14 were eligible and agreed to participate. On average, participants had received treatment at the clinic for 22 months. All participants had previous experience participating in specialty addiction treatment programs. The majority of participants were White (79%), and middle-aged (average: 45 years old), and about half were men (57%). About one-third (36%) of patients were engaged in behavioral therapy, 43% had used alcohol or other drugs in the past 90 days, and 57% currently used tobacco. Seventy-nine percent of patients had five or more medical diagnoses, including 36% who had chronic hepatitis C and 21% who had comorbid psychiatric diagnoses. None of the participants had HIV.
WHAT DID THIS STUDY FIND?
Primary care-based treatment made it easier to get help with other health conditions.
Many patients reported that they didn’t have regular access to a primary care physician before they started receiving buprenorphine treatment in a primary care setting. Once patients started treatment, they were able to address untreated chronic health conditions during regular visits with their primary care provider, including hepatitis C, hypertension, and diabetes. They also liked the convenience of seeing a single doctor for all of their medical needs.
A patient-centered, team-based approach to care made healthcare access more convenient and enjoyable.
Patients mentioned clinic staff in addition to their primary care provider, noting that the team-based approach to their care was convenient and made them feel supported and welcome at the clinic. When patients faced barriers to their care, such as transportation issues or medication-related problems, the care team was easy to reach and willing to work with the patient to help them overcome these barriers. This made it easier to obtain telehealth appointments and avoid interruptions to buprenorphine access.
Treatment within primary care was seen as a more personal, private, and trustworthy experience than treatment at a specialty addiction clinic.
Patients felt like the primary care practice valued patients more than specialty addiction programs and made them feel like more than ‘just a number’. They mentioned that the primary care provider explored different treatment options with them instead of pushing medication as the sole ‘cure’ for addiction. Being able to see the same provider at every primary care visit, as opposed to seeing multiple providers at specialty programs, also gave patients a sense of privacy and helped them to build trust with their healthcare team. Primary care teams were also seen as more responsive than specialty clinics, offering quick responses to patient outreach and requests (e.g., requests for refills). Though over one-third of patients used illicit substances at some point over the past three months, none of them felt judged by clinic staff or worried about being dropped from the clinic.
Prioritizing patient access to buprenorphine facilitated uninterrupted treatment and positive medication experiences.
Patients reported that their primary care clinic made buprenorphine access easy by being flexible with treatment and prioritizing access to buprenorphine, even when patients were unable to attend clinic appointments. Medication was seen as a part of patients’ routine care in the primary care setting and patients thought medication treatment was helpful to their recovery. Barriers to uninterrupted buprenorphine access were noted outside of the healthcare setting, including pharmacies that intermittently ran out of buprenorphine.
Experiences of stigma and discrimination were common but didn’t occur in the context of their current primary care treatment.
All patients reported prior experiences of stigma and discrimination in other healthcare settings, including being denied routine medical care, being inappropriately questioned about substance use in unrelated healthcare visits, and feeling like they and their health concerns were ignored. Despite these past experiences, none of the patients felt stigmatized or discriminated against by their current primary care team, who made them feel respected and valued.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand some of the experiences of patients receiving buprenorphine treatment in primary care settings and the aspects of healthcare models that may help patients feel supported on their path to recovery. This research is important because it can ultimately help identify various treatment models that help expand access to and engagement in medication treatment for opioid use disorder. Findings suggest that the provision of buprenorphine treatment in comprehensive primary care practices may be a helpful path for expanding access to medication treatment that promotes positive treatment experiences and outcomes among patients with opioid use disorder.
It should be remembered, however, that this study was conducted in a single, academic, primary care practice in an urban setting where primary care providers had addiction medicine training, limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise and to practices in rural settings. The fourteen patients involved in this study were also undergoing treatment for an average of almost 2 years, reflecting a small cohort of more stable patients who have had long-term success with buprenorphine treatment. Additional research is needed to determine if these findings are consistent in other more typical primary care practices and among individuals who have less time in treatment.
Treatment in a primary care setting allowed patients to address their untreated chronic health conditions (e.g., Hepatitis-C, diabetes, hypertension) in addition to their opioid use disorder, resulting in improvements in overall health and wellbeing. Individuals with opioid use disorder often have complex needs, including co-occurring psychiatric and physical health conditions, with many requiring treatment for chronic conditions like HIV, Hepatitis-C, and depression. Receiving treatment from a primary care provider allows for the evaluation and treatment of these conditions alongside opioid medication treatment, which improves the chances of a more holistic recovery that includes physical and mental health. Opioid treatment programs do not typically offer comprehensive care like this, and physical health conditions might go untreated as a result. Providing buprenorphine in primary care settings might help address high rates of chronic, sometimes life threatening, health conditions among this population to improve all aspects of health during treatment.
Many patients felt like the primary care setting allowed for a more personal experience in which healthcare providers and staff made them feel valued as a patient and a person. They liked that they were able to develop a trusting rapport with a single doctor who could conveniently tend to all of their medical needs in one location, both within and outside the confines of their buprenorphine treatment. Though all patients in this study had past experiences of stigma and discrimination at opioid treatment programs, none felt like they had these experiences at their primary care practice. This is important because stigma plays a key role in patient experiences with health services and decisions to engage in these services. Addressing stigma in the healthcare system will ultimately help support patients’ medication treatment and positive recovery outcomes.
Importantly, this study examined patients in an academic primary care clinic with a comprehensive treatment model that offered on-site access to behavioral health specialists, pharmacists, nurses, and case managers, which is not standard across all primary care practices.
Though few patients used the behavioral health support services offered as part of this treatment model, patients liked the convenience and support of the comprehensive care team and their patient-centered treatment approaches. The integrated care team and their willingness to work with patients to remove barriers to treatment (e.g., transportation issues preventing appointment attendance) helped to ensure that patients’ medication treatment was not interrupted. This patient-centered approach that prioritizes medication treatment, as opposed to rigid models that require abstinence and appointment attendance for medication refills, offers patients flexibility, ensure their ongoing access to medication, and promote treatment retention. The integrated care team also ensured that healthcare providers and staff were easy to reach and quick to respond to patient requests and concerns, which patients liked.
In programs with more rigid rules and requirements, many patients are involuntarily discharged from treatment due to non-compliance with regulations (e.g., lack of abstinence, irregular in-person attendance) or voluntarily leave treatment early because treatment demands are difficult to accommodate with everyday life obligations. Prior research is mixed on the effects of integrated care models on patient outcomes, with some studies revealing similar substance use disorder outcomes in integrated and standard primary care models, and other studies suggesting better patient outcomes with integrated care, such as fewer acute care episodes. Nonetheless, the flexibility offered in this primary care setting appeared to benefit patients’ treatment experiences and may have helped to promote treatment retention.
Expanding access to buprenorphine treatment is important for addressing the opioid epidemic. Until now, providers needed a waiver to prescribe buprenorphine and could only prescribe to a limited number of patients. Recent changes to regulations now mean that providers no longer need this waiver to prescribe buprenorphine, which makes it easier for more primary care doctors to offer opioid use disorder medication treatment. Additional research in this area will help identify ideal buprenorphine treatment models in primary care settings, which can ultimately promote the expansion of buprenorphine provision in primary care.
This study was conducted in a single, academic, primary care practice in an urban setting where primary care providers had addiction medicine training, limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise and to practices in rural settings. Patients in this study were also undergoing treatment for an average of almost 2 years, reflecting a cohort of more stable patients who have had long-term success with buprenorphine treatment. Additional research is needed to determine if these findings are consistent in other primary care practices and among individuals who have less time in treatment.
Only 14 patients were included in this qualitative study and additional qualitative and quantitative research is needed to determine common barriers and facilitators to office-based buprenorphine treatment in the context of different practices, treatment models, and patient characteristics. Because the patients in this study had been on buprenorphine for an average of almost two years, patients who had positive experiences with treatment and clinic staff and decided to remain in treatment might be over-represented in this study and additional research is needed to determine whether experiences in primary care settings differ in the earlier stages of treatment.
BOTTOM LINE
Patients receiving buprenorphine treatment at this comprehensive primary care program liked several aspects of their treatment team and experience. The team’s patient-centered and flexible approach to buprenorphine provision ensured ongoing access to medication, and their comprehensive team made it easy to reach a provider in a timely manner and made patients feel valued. Compared to specialized opioid treatment programs, the primary care clinic was seen as less stigmatizing and treatment experiences were reported as more personal, private, and trustworthy. Having a single provider for all healthcare concerns also allowed patients to address their physical health alongside their opioid use disorder. Though additional research is needed in other primary care settings with different treatment models, individuals seeking flexible medication treatment programs that can concurrently address mental and physical health might benefit from buprenorphine treatment within comprehensive patient-centered primary care practices where those are available.
For individuals and families seeking recovery: Individuals who are seeking a medication treatment program with more flexible regulations that prioritize ongoing access to medication treatment may benefit from buprenorphine treatment in a primary care practice that offers an integrated healthcare team willing to accommodate barriers to treatment (e.g., transportation to appointments, ongoing substance use) with patient-centered solutions. Comprehensive primary care practices may also be a helpful option, if available, for patients looking to conveniently address untreated physical and other mental health conditions in a single setting. Primary care practices have different treatment models and not all provide patient-centered comprehensive care. Individuals are encouraged to speak with their current healthcare providers to identify a primary care practice that offers buprenorphine treatment alongside other healthcare program aspects that they might prefer.
For treatment professionals and treatment systems: This study helps us identify the aspects of buprenorphine treatment in primary care practices that patients like, which can help identify factors that promote treatment satisfaction, retention, and outcomes. Treatment professionals and systems might enhance their patients’ treatment experiences by offering a patient-centered approach to care that prioritizes buprenorphine access and accommodates barriers to treatment (e.g., using telehealth when transportation isn’t available). Trying to create a stigma- and discrimination-free practice wherever possible also appears important for positive treatment experiences among patients. In addition, addressing physical and mental health comorbidities alongside opioid use disorder may be an important part of comprehensive treatment and primary care settings might be an ideal place for patients to get this care in a single convenient location. However, these data concern a small group of patients at a single clinic and additional research will help us better understand which aspects of healthcare programs are most important to treatment and recovery.
For scientists:Additional research is needed to extend these findings in different healthcare settings with different treatment models. Studies are needed to determine whether a comprehensive primary care treatment model results in better treatment engagement, retention, and outcomes than specialized opioid treatment programs. Identification of other factors impacting treatment utilization, provision, and outcomes in primary care practices is also needed. Additional research will help identify patient and provider barriers to medication treatment uptake and provision, and address barriers by developing novel ways to expand access to medication treatment. Research among individuals who are in the initiation and beginning stages of treatment (participants in this study were in treatment for 22 months, on average) is also needed to determine if patient experiences differ by treatment duration.
For policy makers: Studies like this help us better understand the components of buprenorphine treatment programs that patients like that may lead to greater patient engagement and retention – a common challenge in opioid treatment. This study noted several aspects of buprenorphine treatment in an integrated primary care practice that patients liked over and above specialized treatment programs and that they found beneficial to their overall health and wellbeing. Additional funding for this area of research will help identify ideal buprenorphine treatment models and whether these may be based within primary care settings. This can ultimately promote optimal provision of buprenorphine treatment, help expand patients’ access to lifesaving medications, and increase treatment engagement to better address the opioid epidemic.
There has been an increased effort to expand access to medication treatment for opioid use disorder. Primary care practices are highly accessible outlets that can be leveraged to expand access to these medications. Some offer expertise in both mental and physical healthcare with an ability to follow patients over the long-term, and they are geographically more accessible than the more specialized opioid treatment programs. However, few primary care providers offer medication treatment and those who do typically treat a small number of patients. To further expand availability and use of medication treatment in primary care settings, it is important to understand the perspectives and experiences of patients and providers. Obtaining patients’ views on the barriers and facilitators to treatment in primary care can help improve patients’ experiences and improve treatment uptake and retention. This study sought to better understand the experiences of patients receiving buprenorphine treatment for opioid use disorder in a primary care setting with a comprehensive, integrated healthcare model.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of adult outpatients receiving buprenorphine for opioid use disorder in a primary care setting, in which 14 patients completed interviews about their buprenorphine treatment experience. Individuals were recruited between July and August 2021 from a single urban primary care clinic with a comprehensive treatment model.
All participants were actively receiving buprenorphine treatment for opioid use disorder from a primary care physician within the clinic. In addition to opioid use disorder medication treatment, all patients had on-site access to behavioral health specialists, pharmacists, nurses, and case managers as part of their routine primary care. Primary care providers were trained in addiction medicine. The clinic did not have additional funding dedicated to opioid use disorder medication treatment, and none of the clinic staff had protected time dedicated to providing medication treatment or were explicitly trained to facilitate it.
During the interview, participants answered questions about key aspects of primary care treatment. Interviews asked about: (1) the impact of primary care-based medication treatment on overall health, (2) experiences and interactions with their primary care team. Qualitative interviews were analyzed and barriers and facilitators to medication treatment in primary care were identified.
The researchers identified 7 emergent themes in the interviews and selected 5 of the 7 themes that were most relevant to medication treatment and opioid use disorder for data presentation: (1) overall health improvement, (2) team-based healthcare, (3) comparing primary care to specialty addiction treatment, (4) access to opioid use disorder medications, (5) stigma and discrimination. The researchers also gathered data on demographics and treatment histories from patients’ electronic medical records.
A total of 21 patients were asked to participate in the study, of which, 14 were eligible and agreed to participate. On average, participants had received treatment at the clinic for 22 months. All participants had previous experience participating in specialty addiction treatment programs. The majority of participants were White (79%), and middle-aged (average: 45 years old), and about half were men (57%). About one-third (36%) of patients were engaged in behavioral therapy, 43% had used alcohol or other drugs in the past 90 days, and 57% currently used tobacco. Seventy-nine percent of patients had five or more medical diagnoses, including 36% who had chronic hepatitis C and 21% who had comorbid psychiatric diagnoses. None of the participants had HIV.
WHAT DID THIS STUDY FIND?
Primary care-based treatment made it easier to get help with other health conditions.
Many patients reported that they didn’t have regular access to a primary care physician before they started receiving buprenorphine treatment in a primary care setting. Once patients started treatment, they were able to address untreated chronic health conditions during regular visits with their primary care provider, including hepatitis C, hypertension, and diabetes. They also liked the convenience of seeing a single doctor for all of their medical needs.
A patient-centered, team-based approach to care made healthcare access more convenient and enjoyable.
Patients mentioned clinic staff in addition to their primary care provider, noting that the team-based approach to their care was convenient and made them feel supported and welcome at the clinic. When patients faced barriers to their care, such as transportation issues or medication-related problems, the care team was easy to reach and willing to work with the patient to help them overcome these barriers. This made it easier to obtain telehealth appointments and avoid interruptions to buprenorphine access.
Treatment within primary care was seen as a more personal, private, and trustworthy experience than treatment at a specialty addiction clinic.
Patients felt like the primary care practice valued patients more than specialty addiction programs and made them feel like more than ‘just a number’. They mentioned that the primary care provider explored different treatment options with them instead of pushing medication as the sole ‘cure’ for addiction. Being able to see the same provider at every primary care visit, as opposed to seeing multiple providers at specialty programs, also gave patients a sense of privacy and helped them to build trust with their healthcare team. Primary care teams were also seen as more responsive than specialty clinics, offering quick responses to patient outreach and requests (e.g., requests for refills). Though over one-third of patients used illicit substances at some point over the past three months, none of them felt judged by clinic staff or worried about being dropped from the clinic.
Prioritizing patient access to buprenorphine facilitated uninterrupted treatment and positive medication experiences.
Patients reported that their primary care clinic made buprenorphine access easy by being flexible with treatment and prioritizing access to buprenorphine, even when patients were unable to attend clinic appointments. Medication was seen as a part of patients’ routine care in the primary care setting and patients thought medication treatment was helpful to their recovery. Barriers to uninterrupted buprenorphine access were noted outside of the healthcare setting, including pharmacies that intermittently ran out of buprenorphine.
Experiences of stigma and discrimination were common but didn’t occur in the context of their current primary care treatment.
All patients reported prior experiences of stigma and discrimination in other healthcare settings, including being denied routine medical care, being inappropriately questioned about substance use in unrelated healthcare visits, and feeling like they and their health concerns were ignored. Despite these past experiences, none of the patients felt stigmatized or discriminated against by their current primary care team, who made them feel respected and valued.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand some of the experiences of patients receiving buprenorphine treatment in primary care settings and the aspects of healthcare models that may help patients feel supported on their path to recovery. This research is important because it can ultimately help identify various treatment models that help expand access to and engagement in medication treatment for opioid use disorder. Findings suggest that the provision of buprenorphine treatment in comprehensive primary care practices may be a helpful path for expanding access to medication treatment that promotes positive treatment experiences and outcomes among patients with opioid use disorder.
It should be remembered, however, that this study was conducted in a single, academic, primary care practice in an urban setting where primary care providers had addiction medicine training, limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise and to practices in rural settings. The fourteen patients involved in this study were also undergoing treatment for an average of almost 2 years, reflecting a small cohort of more stable patients who have had long-term success with buprenorphine treatment. Additional research is needed to determine if these findings are consistent in other more typical primary care practices and among individuals who have less time in treatment.
Treatment in a primary care setting allowed patients to address their untreated chronic health conditions (e.g., Hepatitis-C, diabetes, hypertension) in addition to their opioid use disorder, resulting in improvements in overall health and wellbeing. Individuals with opioid use disorder often have complex needs, including co-occurring psychiatric and physical health conditions, with many requiring treatment for chronic conditions like HIV, Hepatitis-C, and depression. Receiving treatment from a primary care provider allows for the evaluation and treatment of these conditions alongside opioid medication treatment, which improves the chances of a more holistic recovery that includes physical and mental health. Opioid treatment programs do not typically offer comprehensive care like this, and physical health conditions might go untreated as a result. Providing buprenorphine in primary care settings might help address high rates of chronic, sometimes life threatening, health conditions among this population to improve all aspects of health during treatment.
Many patients felt like the primary care setting allowed for a more personal experience in which healthcare providers and staff made them feel valued as a patient and a person. They liked that they were able to develop a trusting rapport with a single doctor who could conveniently tend to all of their medical needs in one location, both within and outside the confines of their buprenorphine treatment. Though all patients in this study had past experiences of stigma and discrimination at opioid treatment programs, none felt like they had these experiences at their primary care practice. This is important because stigma plays a key role in patient experiences with health services and decisions to engage in these services. Addressing stigma in the healthcare system will ultimately help support patients’ medication treatment and positive recovery outcomes.
Importantly, this study examined patients in an academic primary care clinic with a comprehensive treatment model that offered on-site access to behavioral health specialists, pharmacists, nurses, and case managers, which is not standard across all primary care practices.
Though few patients used the behavioral health support services offered as part of this treatment model, patients liked the convenience and support of the comprehensive care team and their patient-centered treatment approaches. The integrated care team and their willingness to work with patients to remove barriers to treatment (e.g., transportation issues preventing appointment attendance) helped to ensure that patients’ medication treatment was not interrupted. This patient-centered approach that prioritizes medication treatment, as opposed to rigid models that require abstinence and appointment attendance for medication refills, offers patients flexibility, ensure their ongoing access to medication, and promote treatment retention. The integrated care team also ensured that healthcare providers and staff were easy to reach and quick to respond to patient requests and concerns, which patients liked.
In programs with more rigid rules and requirements, many patients are involuntarily discharged from treatment due to non-compliance with regulations (e.g., lack of abstinence, irregular in-person attendance) or voluntarily leave treatment early because treatment demands are difficult to accommodate with everyday life obligations. Prior research is mixed on the effects of integrated care models on patient outcomes, with some studies revealing similar substance use disorder outcomes in integrated and standard primary care models, and other studies suggesting better patient outcomes with integrated care, such as fewer acute care episodes. Nonetheless, the flexibility offered in this primary care setting appeared to benefit patients’ treatment experiences and may have helped to promote treatment retention.
Expanding access to buprenorphine treatment is important for addressing the opioid epidemic. Until now, providers needed a waiver to prescribe buprenorphine and could only prescribe to a limited number of patients. Recent changes to regulations now mean that providers no longer need this waiver to prescribe buprenorphine, which makes it easier for more primary care doctors to offer opioid use disorder medication treatment. Additional research in this area will help identify ideal buprenorphine treatment models in primary care settings, which can ultimately promote the expansion of buprenorphine provision in primary care.
This study was conducted in a single, academic, primary care practice in an urban setting where primary care providers had addiction medicine training, limiting conclusions about the applicability of these results to other primary care practices with differing healthcare models/expertise and to practices in rural settings. Patients in this study were also undergoing treatment for an average of almost 2 years, reflecting a cohort of more stable patients who have had long-term success with buprenorphine treatment. Additional research is needed to determine if these findings are consistent in other primary care practices and among individuals who have less time in treatment.
Only 14 patients were included in this qualitative study and additional qualitative and quantitative research is needed to determine common barriers and facilitators to office-based buprenorphine treatment in the context of different practices, treatment models, and patient characteristics. Because the patients in this study had been on buprenorphine for an average of almost two years, patients who had positive experiences with treatment and clinic staff and decided to remain in treatment might be over-represented in this study and additional research is needed to determine whether experiences in primary care settings differ in the earlier stages of treatment.
BOTTOM LINE
Patients receiving buprenorphine treatment at this comprehensive primary care program liked several aspects of their treatment team and experience. The team’s patient-centered and flexible approach to buprenorphine provision ensured ongoing access to medication, and their comprehensive team made it easy to reach a provider in a timely manner and made patients feel valued. Compared to specialized opioid treatment programs, the primary care clinic was seen as less stigmatizing and treatment experiences were reported as more personal, private, and trustworthy. Having a single provider for all healthcare concerns also allowed patients to address their physical health alongside their opioid use disorder. Though additional research is needed in other primary care settings with different treatment models, individuals seeking flexible medication treatment programs that can concurrently address mental and physical health might benefit from buprenorphine treatment within comprehensive patient-centered primary care practices where those are available.
For individuals and families seeking recovery: Individuals who are seeking a medication treatment program with more flexible regulations that prioritize ongoing access to medication treatment may benefit from buprenorphine treatment in a primary care practice that offers an integrated healthcare team willing to accommodate barriers to treatment (e.g., transportation to appointments, ongoing substance use) with patient-centered solutions. Comprehensive primary care practices may also be a helpful option, if available, for patients looking to conveniently address untreated physical and other mental health conditions in a single setting. Primary care practices have different treatment models and not all provide patient-centered comprehensive care. Individuals are encouraged to speak with their current healthcare providers to identify a primary care practice that offers buprenorphine treatment alongside other healthcare program aspects that they might prefer.
For treatment professionals and treatment systems: This study helps us identify the aspects of buprenorphine treatment in primary care practices that patients like, which can help identify factors that promote treatment satisfaction, retention, and outcomes. Treatment professionals and systems might enhance their patients’ treatment experiences by offering a patient-centered approach to care that prioritizes buprenorphine access and accommodates barriers to treatment (e.g., using telehealth when transportation isn’t available). Trying to create a stigma- and discrimination-free practice wherever possible also appears important for positive treatment experiences among patients. In addition, addressing physical and mental health comorbidities alongside opioid use disorder may be an important part of comprehensive treatment and primary care settings might be an ideal place for patients to get this care in a single convenient location. However, these data concern a small group of patients at a single clinic and additional research will help us better understand which aspects of healthcare programs are most important to treatment and recovery.
For scientists:Additional research is needed to extend these findings in different healthcare settings with different treatment models. Studies are needed to determine whether a comprehensive primary care treatment model results in better treatment engagement, retention, and outcomes than specialized opioid treatment programs. Identification of other factors impacting treatment utilization, provision, and outcomes in primary care practices is also needed. Additional research will help identify patient and provider barriers to medication treatment uptake and provision, and address barriers by developing novel ways to expand access to medication treatment. Research among individuals who are in the initiation and beginning stages of treatment (participants in this study were in treatment for 22 months, on average) is also needed to determine if patient experiences differ by treatment duration.
For policy makers: Studies like this help us better understand the components of buprenorphine treatment programs that patients like that may lead to greater patient engagement and retention – a common challenge in opioid treatment. This study noted several aspects of buprenorphine treatment in an integrated primary care practice that patients liked over and above specialized treatment programs and that they found beneficial to their overall health and wellbeing. Additional funding for this area of research will help identify ideal buprenorphine treatment models and whether these may be based within primary care settings. This can ultimately promote optimal provision of buprenorphine treatment, help expand patients’ access to lifesaving medications, and increase treatment engagement to better address the opioid epidemic.