“Not just opioids”: Trends and patient characteristics of Veterans involved in fatal stimulant-related overdoses in the U.S.
The focus on the opioid crisis has overshadowed the rise in stimulant overdose deaths. In 2019 there were more deaths involving stimulants than either prescription opioids or heroin. Greater understanding of the clinical characteristics and patterns of health-care utilization can help inform overdose prevention strategies targeting at-risk populations. This study investigates stimulant-involved overdoses in US veterans between 2012 and 2018.
More than 932,000 people have died since 1999 from a drug overdose in the U.S. There were an estimated 107,622 overdose deaths in 2021 alone, an increase of nearly 15% from 2020. Overdose death increases from 2020 to 2021 included synthetic opioids (primarily fentanyl), psychostimulants such as methamphetamine, and cocaine. From 2012 to 2019, the rate of overdose deaths involving cocaine increased more than 3-fold, and those involving psychostimulants (mostly methamphetamine) increase more than 6-fold. Furthermore, overdose deaths involving multiple substances have been increasing. In fact, most stimulant-involved overdose deaths have also involved other substances. However, national policy and research has centered opioids (i.e., the opioid epidemic). For example, efforts to address opioid overdoses have involved scaling up the availability of the opioid overdose antidote naloxone (“Narcan”). Yet much less has been done to address the overdose deaths involving stimulants.
Some populations, such as Veterans who use Veterans Health Administration (VHA) services, are at heightened risk of overdose and may require tailored prevention approaches. Thus, greater understanding of clinical characteristics and patterns of health care utilization among different stimulant overdose profiles can help inform future overdose prevention strategies among at-risk populations.
HOW WAS THIS STUDY CONDUCTED?
This study was a retrospective cohort study that linked National Death Index data from the National Vital Statistics System mortality files and U.S. Veterans Health Administration data. The National Death Index contains date and cause of death. The Veterans Health Administration is the only national health-care system in the U.S. and includes more than 9 million Veterans seen across 1,298 health care facilities. These two sources of data allowed the researchers to link health-care claims data (e.g., health care utilization, encounter types, and diagnoses) with the cause of death (e.g., overdose).
For the present study, Veterans were included if they were aged 18 or older, died from a stimulant-involved overdose between 2012 and 2018, and had at least one in- or out-patient visit at a VA facility, including emergency department visits, in the year prior to overdose death.
Fatal overdoses were grouped into six mutually exclusive categories based on toxicology reports using the International Classification of Diseases, 10th revision (ICD-10) codes: (1) cocaine only, (2) methamphetamine (hereafter referred to as “meth”) only, (3) cocaine + opioid, (4) meth + opioid, (5) stimulant + other non-opioid substance, and (6) cocaine + meth (with or without opioids). Non-opioid substances included alcohol, cannabis, benzodiazepines, and barbiturates. Meth and other psychostimulant deaths are grouped together under a single toxicology code, which also includes drugs such as caffeine, MDMA, and amphetamine; however, in recent years, 85-90% of death certificates with this code mention meth, and this is thought to be an underestimate. Thus, the researchers refer to the entire ‘psychostimulants with abuse potential’ toxicology code as meth in their study. The researchers then examine demographic, clinical, and treatment history characteristics among the six groups adjusting for VA site to which the participants had the most visits, which accounts for clustering within VA site.
The researchers identified 3,631 Veterans who died from a stimulant-involved overdose between 2012 and 2018 and had a VA health visit in the year prior to death. Of those, 62% were aged 45-64 and 96% identified as male. Just over half (55%) were also White non-Hispanic; however, Black non-Hispanic were overrepresented in overdose deaths and made up 31% of overdose deaths involving stimulants. Almost all (91%) reported living in an urban setting and just over half (56%) had their primary care location at a VA medical center (compared to a community-based outpatient center). There was also a high prevalence of mental health disorders/conditions in the year prior to death among the sample: 28% post-traumatic stress disorder; 42% depressive disorder; 23% opioid use disorder; 38% stimulant use disorder; 44% other substance use disorder; and 13% HIV/HCV. Approximately 85% attended a primary care visit in the last 12 months while 30% attended a substance use disorder clinic.
WHAT DID THIS STUDY FIND?
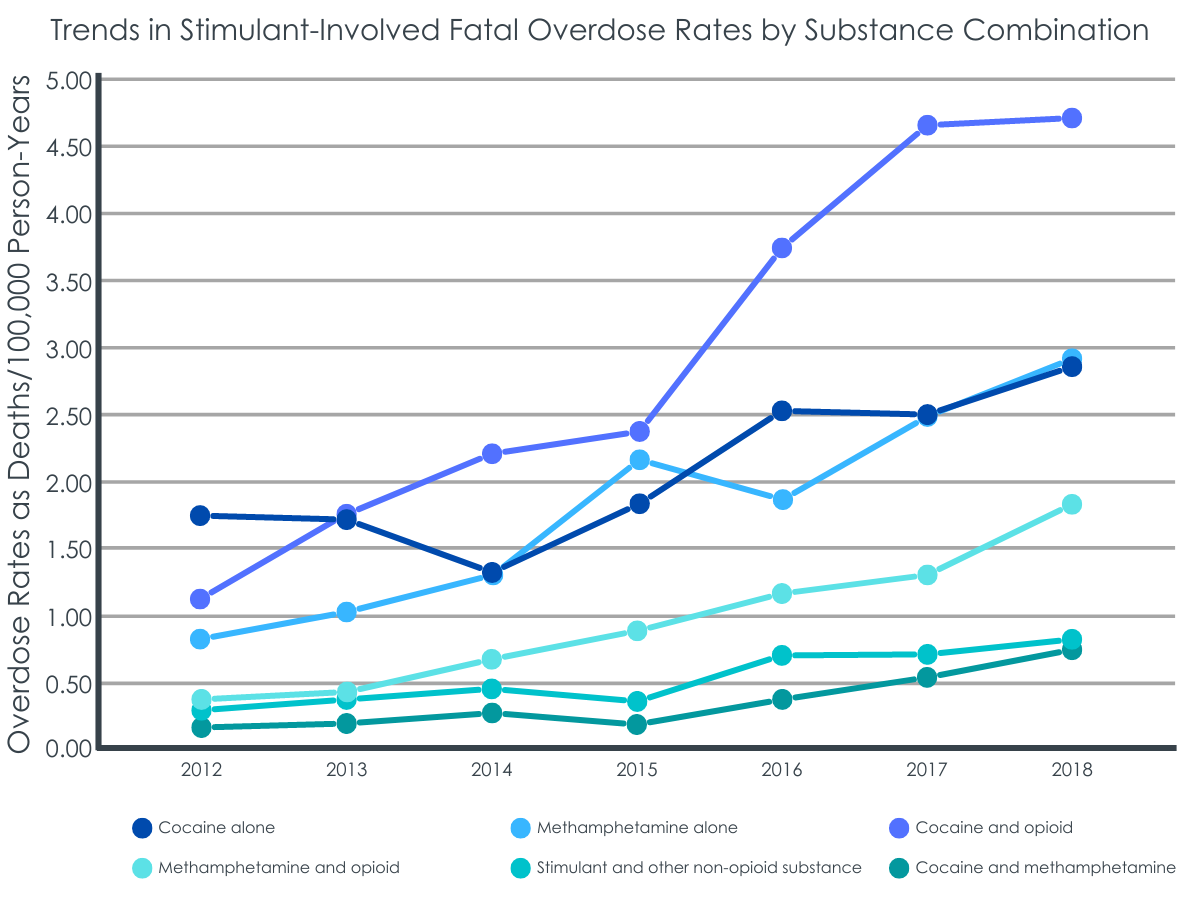
Rates of stimulant-involved overdose deaths tripled over time.
Between 2012 and 2018, a total of 3,631 Veterans died from stimulant-involved overdoses, and the rate of stimulant-involved tripled (3.06 times) from 2012 to 2018. Of stimulant-involved overdose deaths, 67% involved cocaine and 38% involved meth. The greatest rate increase from 2012 to 2018 was in cocaine plus opioid-related overdose deaths, which was over four times (4.22 times) higher in 2018 compared to 2012.
Just over half of stimulant-involved overdose deaths included other substances.
Just over half (54%) of stimulant-involved overdose deaths also involved another substance. Most (88%) of polysubstance-involved overdose deaths involved opioids, with 48% of all stimulant-involved overdose deaths co-involving opioids. Of stimulant and opioid co-involved overdose deaths, 46% involved synthetic opioids (e.g., fentanyl), 45% involved heroin, and 26% involved prescription opioids. The most common substance besides opioids was alcohol, with 76% of stimulant-involved overdose deaths that involved another substance beside opioids involving alcohol.
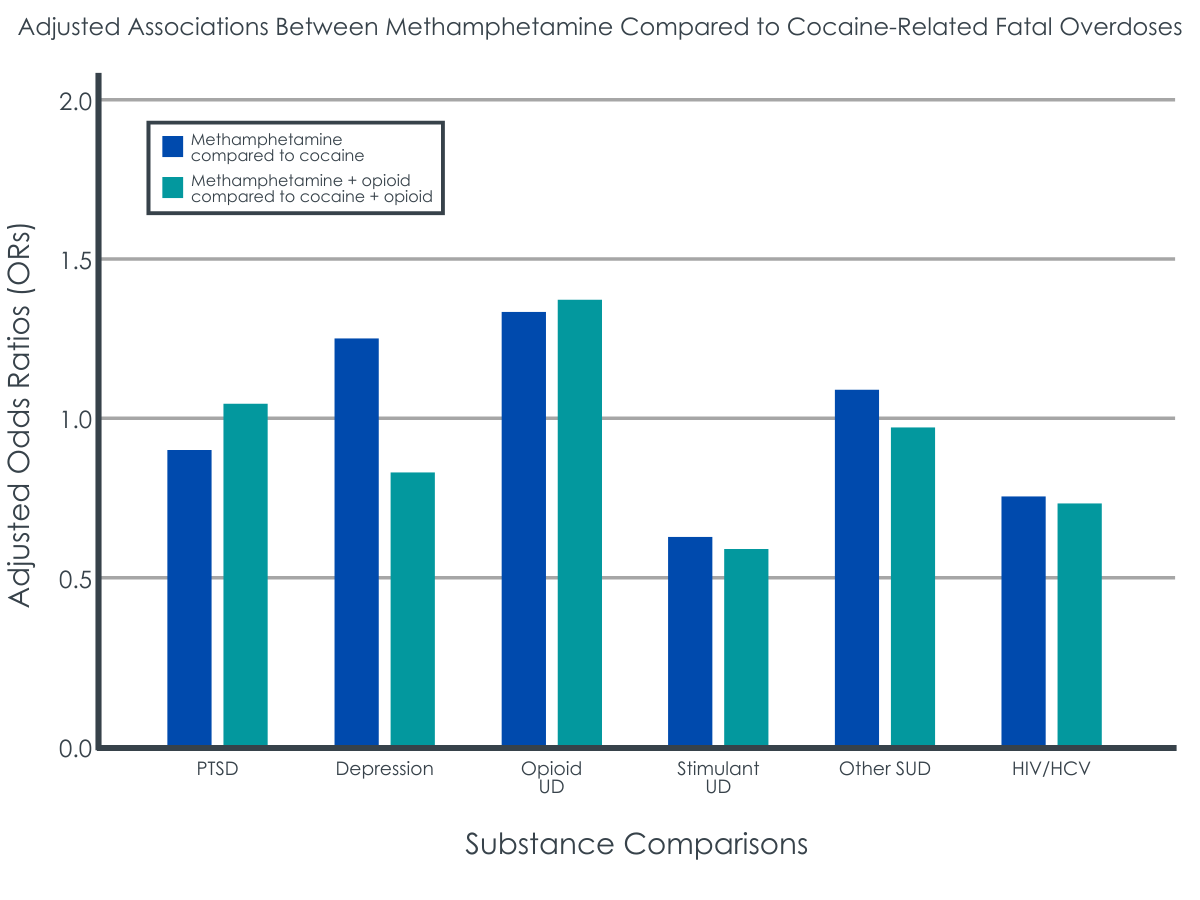
Fatal overdoses involving cocaine differed from those involving meth.
Overdose deaths involving meth were more common in rural localities compared to those involving cocaine and cocaine plus opioids, 2.7 times higher among meth alone and 1.8 times higher among meth plus opioids respectively. For older adults (65+) compared to young adults (18-29), an overdose involving cocaine alone was 4.5 times more likely as one involving meth alone. An overdose death involving cocaine alone was also 14.3 times as likely among Black non-Hispanic versus White compared to those involving meth alone. Similarly, death involving meth plus opioids was 0.08 times less likely compared to death involving cocaine plus opioids among Black non-Hispanic versus White. Overdose death involving cocaine plus opioids were 3.1 times more likely among Hispanic versus White compared to meth plus opioid deaths.
Those involved in a cocaine alone or cocaine plus opioid death were 1.6 and 1.7 times more likely to also have a stimulant use disorder compared to meth along and meth plus opioid deaths respectively. Treatment utilization, however, was similar between cocaine- or meth-involved overdose deaths.
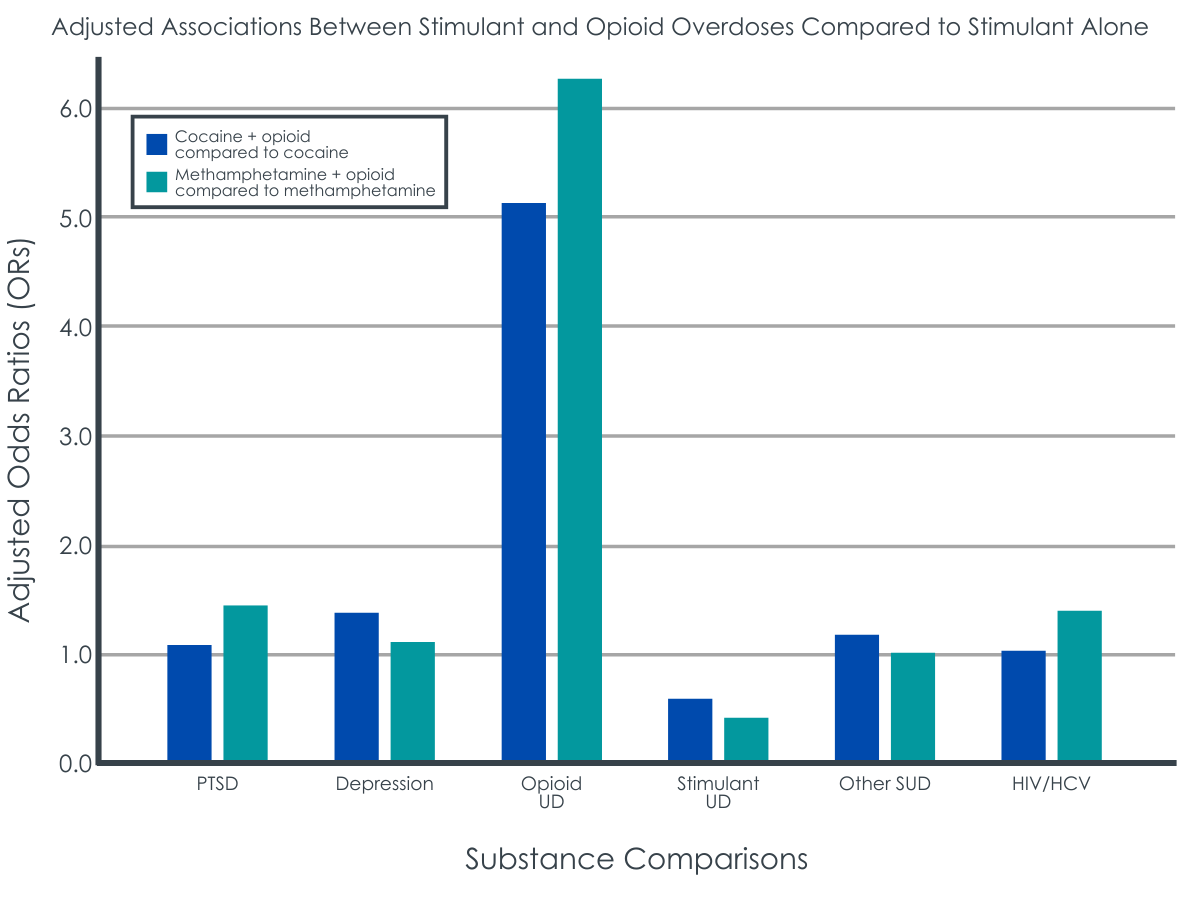
Patient characteristics differed among stimulant deaths that also involved opioids versus stimulants alone.
Overdose deaths that involved a stimulant plus opioids, rather than a stimulant alone, were more likely to occur among people under 30 years old compared to those in middle or later life. Similarly, overdose deaths involving both simulants and opioids, versus a stimulant alone, were more likely among Whites compared to Black non-Hispanics. Cocaine and opioid co-involved overdose deaths were 1.42 times more likely among those with a depressive disorder, 5.11 time more likely among those with an opioid use disorder and 0.55 times less likely among those with a stimulant use disorder compared to cocaine alone overdose deaths. Conversely, meth and opioid co-involved overdose deaths were 1.47 times more likely among those with a post-traumatic stress disorder, 6.29 times more likely among those with an opioid use disorder, and 0.44 times less likely among those with a stimulant use disorder. If opioids were co-involved with a stimulant, the individual was more likely to have an opioid use disorder diagnosis than a stimulant use disorder diagnosis.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The overdose crisis has been conceptualized as a triple wave phenomenon. The first wave was from 1999 to 2010 and was primarily due to prescription opioids. The second wave began in 2010 with sharp rises in heroin-related overdose deaths. The third wave began in 2014 when synthetic opioids-related (mainly fentanyl and fentanyl analogs) overdose rose dramatically. However, we may now be in a fourth wave of high mortality involving both opioids and stimulants. Perhaps overshadowed by the focus on opioids, stimulant-related overdose deaths have been on the rise, with a 3-fold and 6-fold increase in cocaine and meth involved overdoes dose deaths from 2012-2019.
This study highlights the rising trend of stimulant-involved overdose deaths among Veterans in the U.S. from 2012 to 2018 and explores clinical and health-care utilization characteristics of patients across stimulant-related overdose deaths. The study found that stimulant-involved overdose deaths was 3.06 times higher in 2018 than 2012. The sharpest increase in overdose deaths was cocaine plus opioids (4.22 times higher in 2018 than 2012).
This study also found that Black non-Hispanic patients were overrepresented across stimulant-involved overdose deaths, particularly cocaine-involved, relative to the racial and ethnic composition of the Veterans Health Administration. This mirrors findings from the general U.S. population on the racial disparities in opioid involved death rates – the rate of opioid involved death rates has increased more among African Americans than Whites (199% vs 77% from 2013-2018). Racial disparities in overdose deaths, among the general population and the VA, highlight the need for equity in overdose prevention, intervention, and treatment resources.
Polysubstance involved overdose deaths made up over half (54%) of overdose deaths related to stimulants, with most (88%) comprising of a stimulant and an opioid. Similarly, in Massachusetts from 2014 to 2015, 83% of opioid-involved overdose deaths involved another substance in addition to an opioid. The most common non-opioid substance involved in stimulant-involved overdose death in this study was alcohol, comprising 76.3% of stimulated plus non-opioid substance-involved overdose deaths. The second most common non-opioid substance group involved in stimulant-involved overdose death was barbiturates or benzodiazepines, comprising 19.1% of stimulant plus non-opioid overdose deaths. Thus, 95.4% of non-opioid substances included respiratory-depressing drugs, which increase the risk of overdose mortality generally and especially if used alongside opioids.
Polysubstance use is on the rise as well, and findings from this study confer that patients using multiple substances have more severe clinical profiles than their single substance using counterparts. In this study, patients using cocaine plus opioids were more likely to also be diagnosed with depressive disorder and opioid use disorder as well as report 3 or more other medical comorbidities. However, only 29.9% of patients who died of a stimulant-involved overdose were seen in specialty substance use settings in the past year, underscoring the need to increase resources for people who use substances (i.e., overdose prevention, intervention, and treatment). Furthermore, unique, modifiable treatment plans may be required for polysubstance use. For example, contingency management is the most empirically support treatment for stimulant use, and it may be coupled with medication for opioid use disorder to address stimulant and opioid co-use.
This study also pinpointed important differences between overdose deaths involving cocaine versus meth. Meth overdose death was more likely in rural settings, driven less by combined substances, more likely among older (65+) adults, and less likely to appear alongside a stimulant use disorder diagnosis compared to cocaine. While this finding fits with previous evidence that meth is more prevalent, easily accessible, and available at a low cost in rural settings, these trends are also changing. Although meth has been more prevalent in the Midwest, the largest relative increase in death rates occurred in the Northeast from 2018 to 2019 in the general population. The geographic changes in meth use are also accompanied by changes in potency, availability, and affordability broadly, which have all been increasing since the 1990s.
Additionally, stimulants being contaminated with fentanyl in the U.S. and Canada poses a significant risk, which would disproportionately impact opioid-naïve stimulant users due to their low tolerance and result in increased deaths. More empirical work is needed to explore if the shifting trends in meth and its use are also accompanied by changes in who uses it and experiences of related harms.
Taken together, this study draws attention to the rise in stimulant-related overdose deaths among Veterans as well as unique patient profiles associated with those deaths. The study pinpoints the need to prioritize prevention and treatment efforts among this vulnerable population. Moreover, the study amplifies the need to consider polysubstance use in screening, treatment, and retention planning. For example, patients with a co-involved stimulant and opioid overdose death were much less likely to have a stimulant use disorder diagnosis but more likely to have an opioid use disorder diagnosis. More research is needed to explore why these differences appear. Interventions aimed at reducing fatal overdoses may need to account more for stimulant and polysubstance use instead of focusing exclusively on opioid use.
Stimulant-related deaths, as well as other substance use-deaths, can only be identified to the degree that toxicology analyses are run, and substances are indicated on death certificates. This leads to under-reporting of substance involvement in deaths.
Cause of death coding only discriminates between cocaine and other psychostimulants. Although evidence suggests nearly all of the other psychostimulants are meth, the results here are unable to disentangle the other psychostimulants category.
The sample is limited to Veterans that have received care in the Veterans Health Administration. The degree to which these findings generalize outside the VA is not known.
BOTTOM LINE
Although opioids continue to drive the overdose crisis in the U.S., stimulant-involved overdose deaths have increased more than threefold from 2012 to 2018 among Veterans seen at a Veterans Health Administration medical facility in the year prior to death. Patient characteristics differ between cocaine and meth-involved deaths. Also, most stimulant-involved deaths involved another substance — primarily opioids. The rising stimulant polysubstance involved overdose deaths suggests that substance use treatment planning would likely benefit from identifying all substances a person uses or is likely to use along with stimulants, including alcohol and opioid. Policy that increases awareness and access to helpful treatments for polysubstance use would also be likely to reduce overdose deaths. Research that identifies effective screening, intervention, and treatment of potentially fatal stimulant use would likely reduce overdose mortality as well. More generally, public health policies are needed that can address the complex role of stimulants and polysubstance use in overdose deaths.
For individuals and families seeking recovery: Stimulant-involved overdose deaths are increasing across the U.S., including among vulnerable groups such as Veterans. Given how prevalent opioid use is among stimulant-involved overdose deaths, having naloxone around could prevent an overdose death. Also, it is possible that meth or cocaine may contain opioids like fentanyl without the end user knowing. Naloxone, an opioid overdose antidote, is also available with and without a prescription at most pharmacies as well as community-based harm reduction programs so, again, having this available may be lifesaving.
For treatment professionals and treatment systems: The authors found that stimulant-involved overdose deaths are increasing among Veterans seen at a Veterans Health Administration medical facility in the year prior to death. Most of these deaths involved another substance, mostly opioids. Those living in rural areas more likely to experience a meth-involved overdose death compared to those in urban areas. By targeting polysubstance use as well as other key factors such as locality, comorbidities, and health care access, treatment programs can address the unique constellations of risk and protective factors for individuals. Identifying these key characteristics will likely assist in aligning effective treatments at the right time for individuals.
For scientists: The overdose crisis continues to be among the most pressing public health concerns of our time. This study sought to explore stimulant-involved overdose deaths specifically by linking national mortality data with Veterans Health Administration data. Stimulant-involved overdoses increased threefold from 2012-2018, with most overdoses also involving another substance (e.g., opioids). The study also found that patient characteristics differed between cocaine and meth-involved overdose deaths. Research is needed to further bring to light the modifiable determinants of stimulant alone and stimulant co-involvement overdose deaths. More work is also needed to understand and address the racial and ethnic disparities found in simulant-involved overdose deaths, with black non-Hispanics being overrepresented in deaths. Future screening, prevention, and treatment would likely benefit from replicating this study among populations other than Veterans. Work that identifies what treatments, supports, and resources work best for whom can ultimately help to improve overdose prevention and response effort.
For policy makers: Although there has been growing public health policy support in the U.S. to address the opioid overdose crisis, more attention may need to be directed toward stimulants and polysubstance use. This study found increasing trends in stimulant-involved overdose deaths and high rates of polysubstance-involved overdoses, especially those that also include opioids. These findings highlight the need to advance the research on prevention, intervention, and treatment strategies for stimulant use and polysubstance use. Increasing access to health care and implementation of evidence-based supports will likely lead to improved public health.
More than 932,000 people have died since 1999 from a drug overdose in the U.S. There were an estimated 107,622 overdose deaths in 2021 alone, an increase of nearly 15% from 2020. Overdose death increases from 2020 to 2021 included synthetic opioids (primarily fentanyl), psychostimulants such as methamphetamine, and cocaine. From 2012 to 2019, the rate of overdose deaths involving cocaine increased more than 3-fold, and those involving psychostimulants (mostly methamphetamine) increase more than 6-fold. Furthermore, overdose deaths involving multiple substances have been increasing. In fact, most stimulant-involved overdose deaths have also involved other substances. However, national policy and research has centered opioids (i.e., the opioid epidemic). For example, efforts to address opioid overdoses have involved scaling up the availability of the opioid overdose antidote naloxone (“Narcan”). Yet much less has been done to address the overdose deaths involving stimulants.
Some populations, such as Veterans who use Veterans Health Administration (VHA) services, are at heightened risk of overdose and may require tailored prevention approaches. Thus, greater understanding of clinical characteristics and patterns of health care utilization among different stimulant overdose profiles can help inform future overdose prevention strategies among at-risk populations.
HOW WAS THIS STUDY CONDUCTED?
This study was a retrospective cohort study that linked National Death Index data from the National Vital Statistics System mortality files and U.S. Veterans Health Administration data. The National Death Index contains date and cause of death. The Veterans Health Administration is the only national health-care system in the U.S. and includes more than 9 million Veterans seen across 1,298 health care facilities. These two sources of data allowed the researchers to link health-care claims data (e.g., health care utilization, encounter types, and diagnoses) with the cause of death (e.g., overdose).
For the present study, Veterans were included if they were aged 18 or older, died from a stimulant-involved overdose between 2012 and 2018, and had at least one in- or out-patient visit at a VA facility, including emergency department visits, in the year prior to overdose death.
Fatal overdoses were grouped into six mutually exclusive categories based on toxicology reports using the International Classification of Diseases, 10th revision (ICD-10) codes: (1) cocaine only, (2) methamphetamine (hereafter referred to as “meth”) only, (3) cocaine + opioid, (4) meth + opioid, (5) stimulant + other non-opioid substance, and (6) cocaine + meth (with or without opioids). Non-opioid substances included alcohol, cannabis, benzodiazepines, and barbiturates. Meth and other psychostimulant deaths are grouped together under a single toxicology code, which also includes drugs such as caffeine, MDMA, and amphetamine; however, in recent years, 85-90% of death certificates with this code mention meth, and this is thought to be an underestimate. Thus, the researchers refer to the entire ‘psychostimulants with abuse potential’ toxicology code as meth in their study. The researchers then examine demographic, clinical, and treatment history characteristics among the six groups adjusting for VA site to which the participants had the most visits, which accounts for clustering within VA site.
The researchers identified 3,631 Veterans who died from a stimulant-involved overdose between 2012 and 2018 and had a VA health visit in the year prior to death. Of those, 62% were aged 45-64 and 96% identified as male. Just over half (55%) were also White non-Hispanic; however, Black non-Hispanic were overrepresented in overdose deaths and made up 31% of overdose deaths involving stimulants. Almost all (91%) reported living in an urban setting and just over half (56%) had their primary care location at a VA medical center (compared to a community-based outpatient center). There was also a high prevalence of mental health disorders/conditions in the year prior to death among the sample: 28% post-traumatic stress disorder; 42% depressive disorder; 23% opioid use disorder; 38% stimulant use disorder; 44% other substance use disorder; and 13% HIV/HCV. Approximately 85% attended a primary care visit in the last 12 months while 30% attended a substance use disorder clinic.
WHAT DID THIS STUDY FIND?
Rates of stimulant-involved overdose deaths tripled over time.
Between 2012 and 2018, a total of 3,631 Veterans died from stimulant-involved overdoses, and the rate of stimulant-involved tripled (3.06 times) from 2012 to 2018. Of stimulant-involved overdose deaths, 67% involved cocaine and 38% involved meth. The greatest rate increase from 2012 to 2018 was in cocaine plus opioid-related overdose deaths, which was over four times (4.22 times) higher in 2018 compared to 2012.
Just over half of stimulant-involved overdose deaths included other substances.
Just over half (54%) of stimulant-involved overdose deaths also involved another substance. Most (88%) of polysubstance-involved overdose deaths involved opioids, with 48% of all stimulant-involved overdose deaths co-involving opioids. Of stimulant and opioid co-involved overdose deaths, 46% involved synthetic opioids (e.g., fentanyl), 45% involved heroin, and 26% involved prescription opioids. The most common substance besides opioids was alcohol, with 76% of stimulant-involved overdose deaths that involved another substance beside opioids involving alcohol.
Fatal overdoses involving cocaine differed from those involving meth.
Overdose deaths involving meth were more common in rural localities compared to those involving cocaine and cocaine plus opioids, 2.7 times higher among meth alone and 1.8 times higher among meth plus opioids respectively. For older adults (65+) compared to young adults (18-29), an overdose involving cocaine alone was 4.5 times more likely as one involving meth alone. An overdose death involving cocaine alone was also 14.3 times as likely among Black non-Hispanic versus White compared to those involving meth alone. Similarly, death involving meth plus opioids was 0.08 times less likely compared to death involving cocaine plus opioids among Black non-Hispanic versus White. Overdose death involving cocaine plus opioids were 3.1 times more likely among Hispanic versus White compared to meth plus opioid deaths.
Those involved in a cocaine alone or cocaine plus opioid death were 1.6 and 1.7 times more likely to also have a stimulant use disorder compared to meth along and meth plus opioid deaths respectively. Treatment utilization, however, was similar between cocaine- or meth-involved overdose deaths.
Patient characteristics differed among stimulant deaths that also involved opioids versus stimulants alone.
Overdose deaths that involved a stimulant plus opioids, rather than a stimulant alone, were more likely to occur among people under 30 years old compared to those in middle or later life. Similarly, overdose deaths involving both simulants and opioids, versus a stimulant alone, were more likely among Whites compared to Black non-Hispanics. Cocaine and opioid co-involved overdose deaths were 1.42 times more likely among those with a depressive disorder, 5.11 time more likely among those with an opioid use disorder and 0.55 times less likely among those with a stimulant use disorder compared to cocaine alone overdose deaths. Conversely, meth and opioid co-involved overdose deaths were 1.47 times more likely among those with a post-traumatic stress disorder, 6.29 times more likely among those with an opioid use disorder, and 0.44 times less likely among those with a stimulant use disorder. If opioids were co-involved with a stimulant, the individual was more likely to have an opioid use disorder diagnosis than a stimulant use disorder diagnosis.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The overdose crisis has been conceptualized as a triple wave phenomenon. The first wave was from 1999 to 2010 and was primarily due to prescription opioids. The second wave began in 2010 with sharp rises in heroin-related overdose deaths. The third wave began in 2014 when synthetic opioids-related (mainly fentanyl and fentanyl analogs) overdose rose dramatically. However, we may now be in a fourth wave of high mortality involving both opioids and stimulants. Perhaps overshadowed by the focus on opioids, stimulant-related overdose deaths have been on the rise, with a 3-fold and 6-fold increase in cocaine and meth involved overdoes dose deaths from 2012-2019.
This study highlights the rising trend of stimulant-involved overdose deaths among Veterans in the U.S. from 2012 to 2018 and explores clinical and health-care utilization characteristics of patients across stimulant-related overdose deaths. The study found that stimulant-involved overdose deaths was 3.06 times higher in 2018 than 2012. The sharpest increase in overdose deaths was cocaine plus opioids (4.22 times higher in 2018 than 2012).
This study also found that Black non-Hispanic patients were overrepresented across stimulant-involved overdose deaths, particularly cocaine-involved, relative to the racial and ethnic composition of the Veterans Health Administration. This mirrors findings from the general U.S. population on the racial disparities in opioid involved death rates – the rate of opioid involved death rates has increased more among African Americans than Whites (199% vs 77% from 2013-2018). Racial disparities in overdose deaths, among the general population and the VA, highlight the need for equity in overdose prevention, intervention, and treatment resources.
Polysubstance involved overdose deaths made up over half (54%) of overdose deaths related to stimulants, with most (88%) comprising of a stimulant and an opioid. Similarly, in Massachusetts from 2014 to 2015, 83% of opioid-involved overdose deaths involved another substance in addition to an opioid. The most common non-opioid substance involved in stimulant-involved overdose death in this study was alcohol, comprising 76.3% of stimulated plus non-opioid substance-involved overdose deaths. The second most common non-opioid substance group involved in stimulant-involved overdose death was barbiturates or benzodiazepines, comprising 19.1% of stimulant plus non-opioid overdose deaths. Thus, 95.4% of non-opioid substances included respiratory-depressing drugs, which increase the risk of overdose mortality generally and especially if used alongside opioids.
Polysubstance use is on the rise as well, and findings from this study confer that patients using multiple substances have more severe clinical profiles than their single substance using counterparts. In this study, patients using cocaine plus opioids were more likely to also be diagnosed with depressive disorder and opioid use disorder as well as report 3 or more other medical comorbidities. However, only 29.9% of patients who died of a stimulant-involved overdose were seen in specialty substance use settings in the past year, underscoring the need to increase resources for people who use substances (i.e., overdose prevention, intervention, and treatment). Furthermore, unique, modifiable treatment plans may be required for polysubstance use. For example, contingency management is the most empirically support treatment for stimulant use, and it may be coupled with medication for opioid use disorder to address stimulant and opioid co-use.
This study also pinpointed important differences between overdose deaths involving cocaine versus meth. Meth overdose death was more likely in rural settings, driven less by combined substances, more likely among older (65+) adults, and less likely to appear alongside a stimulant use disorder diagnosis compared to cocaine. While this finding fits with previous evidence that meth is more prevalent, easily accessible, and available at a low cost in rural settings, these trends are also changing. Although meth has been more prevalent in the Midwest, the largest relative increase in death rates occurred in the Northeast from 2018 to 2019 in the general population. The geographic changes in meth use are also accompanied by changes in potency, availability, and affordability broadly, which have all been increasing since the 1990s.
Additionally, stimulants being contaminated with fentanyl in the U.S. and Canada poses a significant risk, which would disproportionately impact opioid-naïve stimulant users due to their low tolerance and result in increased deaths. More empirical work is needed to explore if the shifting trends in meth and its use are also accompanied by changes in who uses it and experiences of related harms.
Taken together, this study draws attention to the rise in stimulant-related overdose deaths among Veterans as well as unique patient profiles associated with those deaths. The study pinpoints the need to prioritize prevention and treatment efforts among this vulnerable population. Moreover, the study amplifies the need to consider polysubstance use in screening, treatment, and retention planning. For example, patients with a co-involved stimulant and opioid overdose death were much less likely to have a stimulant use disorder diagnosis but more likely to have an opioid use disorder diagnosis. More research is needed to explore why these differences appear. Interventions aimed at reducing fatal overdoses may need to account more for stimulant and polysubstance use instead of focusing exclusively on opioid use.
Stimulant-related deaths, as well as other substance use-deaths, can only be identified to the degree that toxicology analyses are run, and substances are indicated on death certificates. This leads to under-reporting of substance involvement in deaths.
Cause of death coding only discriminates between cocaine and other psychostimulants. Although evidence suggests nearly all of the other psychostimulants are meth, the results here are unable to disentangle the other psychostimulants category.
The sample is limited to Veterans that have received care in the Veterans Health Administration. The degree to which these findings generalize outside the VA is not known.
BOTTOM LINE
Although opioids continue to drive the overdose crisis in the U.S., stimulant-involved overdose deaths have increased more than threefold from 2012 to 2018 among Veterans seen at a Veterans Health Administration medical facility in the year prior to death. Patient characteristics differ between cocaine and meth-involved deaths. Also, most stimulant-involved deaths involved another substance — primarily opioids. The rising stimulant polysubstance involved overdose deaths suggests that substance use treatment planning would likely benefit from identifying all substances a person uses or is likely to use along with stimulants, including alcohol and opioid. Policy that increases awareness and access to helpful treatments for polysubstance use would also be likely to reduce overdose deaths. Research that identifies effective screening, intervention, and treatment of potentially fatal stimulant use would likely reduce overdose mortality as well. More generally, public health policies are needed that can address the complex role of stimulants and polysubstance use in overdose deaths.
For individuals and families seeking recovery: Stimulant-involved overdose deaths are increasing across the U.S., including among vulnerable groups such as Veterans. Given how prevalent opioid use is among stimulant-involved overdose deaths, having naloxone around could prevent an overdose death. Also, it is possible that meth or cocaine may contain opioids like fentanyl without the end user knowing. Naloxone, an opioid overdose antidote, is also available with and without a prescription at most pharmacies as well as community-based harm reduction programs so, again, having this available may be lifesaving.
For treatment professionals and treatment systems: The authors found that stimulant-involved overdose deaths are increasing among Veterans seen at a Veterans Health Administration medical facility in the year prior to death. Most of these deaths involved another substance, mostly opioids. Those living in rural areas more likely to experience a meth-involved overdose death compared to those in urban areas. By targeting polysubstance use as well as other key factors such as locality, comorbidities, and health care access, treatment programs can address the unique constellations of risk and protective factors for individuals. Identifying these key characteristics will likely assist in aligning effective treatments at the right time for individuals.
For scientists: The overdose crisis continues to be among the most pressing public health concerns of our time. This study sought to explore stimulant-involved overdose deaths specifically by linking national mortality data with Veterans Health Administration data. Stimulant-involved overdoses increased threefold from 2012-2018, with most overdoses also involving another substance (e.g., opioids). The study also found that patient characteristics differed between cocaine and meth-involved overdose deaths. Research is needed to further bring to light the modifiable determinants of stimulant alone and stimulant co-involvement overdose deaths. More work is also needed to understand and address the racial and ethnic disparities found in simulant-involved overdose deaths, with black non-Hispanics being overrepresented in deaths. Future screening, prevention, and treatment would likely benefit from replicating this study among populations other than Veterans. Work that identifies what treatments, supports, and resources work best for whom can ultimately help to improve overdose prevention and response effort.
For policy makers: Although there has been growing public health policy support in the U.S. to address the opioid overdose crisis, more attention may need to be directed toward stimulants and polysubstance use. This study found increasing trends in stimulant-involved overdose deaths and high rates of polysubstance-involved overdoses, especially those that also include opioids. These findings highlight the need to advance the research on prevention, intervention, and treatment strategies for stimulant use and polysubstance use. Increasing access to health care and implementation of evidence-based supports will likely lead to improved public health.
More than 932,000 people have died since 1999 from a drug overdose in the U.S. There were an estimated 107,622 overdose deaths in 2021 alone, an increase of nearly 15% from 2020. Overdose death increases from 2020 to 2021 included synthetic opioids (primarily fentanyl), psychostimulants such as methamphetamine, and cocaine. From 2012 to 2019, the rate of overdose deaths involving cocaine increased more than 3-fold, and those involving psychostimulants (mostly methamphetamine) increase more than 6-fold. Furthermore, overdose deaths involving multiple substances have been increasing. In fact, most stimulant-involved overdose deaths have also involved other substances. However, national policy and research has centered opioids (i.e., the opioid epidemic). For example, efforts to address opioid overdoses have involved scaling up the availability of the opioid overdose antidote naloxone (“Narcan”). Yet much less has been done to address the overdose deaths involving stimulants.
Some populations, such as Veterans who use Veterans Health Administration (VHA) services, are at heightened risk of overdose and may require tailored prevention approaches. Thus, greater understanding of clinical characteristics and patterns of health care utilization among different stimulant overdose profiles can help inform future overdose prevention strategies among at-risk populations.
HOW WAS THIS STUDY CONDUCTED?
This study was a retrospective cohort study that linked National Death Index data from the National Vital Statistics System mortality files and U.S. Veterans Health Administration data. The National Death Index contains date and cause of death. The Veterans Health Administration is the only national health-care system in the U.S. and includes more than 9 million Veterans seen across 1,298 health care facilities. These two sources of data allowed the researchers to link health-care claims data (e.g., health care utilization, encounter types, and diagnoses) with the cause of death (e.g., overdose).
For the present study, Veterans were included if they were aged 18 or older, died from a stimulant-involved overdose between 2012 and 2018, and had at least one in- or out-patient visit at a VA facility, including emergency department visits, in the year prior to overdose death.
Fatal overdoses were grouped into six mutually exclusive categories based on toxicology reports using the International Classification of Diseases, 10th revision (ICD-10) codes: (1) cocaine only, (2) methamphetamine (hereafter referred to as “meth”) only, (3) cocaine + opioid, (4) meth + opioid, (5) stimulant + other non-opioid substance, and (6) cocaine + meth (with or without opioids). Non-opioid substances included alcohol, cannabis, benzodiazepines, and barbiturates. Meth and other psychostimulant deaths are grouped together under a single toxicology code, which also includes drugs such as caffeine, MDMA, and amphetamine; however, in recent years, 85-90% of death certificates with this code mention meth, and this is thought to be an underestimate. Thus, the researchers refer to the entire ‘psychostimulants with abuse potential’ toxicology code as meth in their study. The researchers then examine demographic, clinical, and treatment history characteristics among the six groups adjusting for VA site to which the participants had the most visits, which accounts for clustering within VA site.
The researchers identified 3,631 Veterans who died from a stimulant-involved overdose between 2012 and 2018 and had a VA health visit in the year prior to death. Of those, 62% were aged 45-64 and 96% identified as male. Just over half (55%) were also White non-Hispanic; however, Black non-Hispanic were overrepresented in overdose deaths and made up 31% of overdose deaths involving stimulants. Almost all (91%) reported living in an urban setting and just over half (56%) had their primary care location at a VA medical center (compared to a community-based outpatient center). There was also a high prevalence of mental health disorders/conditions in the year prior to death among the sample: 28% post-traumatic stress disorder; 42% depressive disorder; 23% opioid use disorder; 38% stimulant use disorder; 44% other substance use disorder; and 13% HIV/HCV. Approximately 85% attended a primary care visit in the last 12 months while 30% attended a substance use disorder clinic.
WHAT DID THIS STUDY FIND?
Rates of stimulant-involved overdose deaths tripled over time.
Between 2012 and 2018, a total of 3,631 Veterans died from stimulant-involved overdoses, and the rate of stimulant-involved tripled (3.06 times) from 2012 to 2018. Of stimulant-involved overdose deaths, 67% involved cocaine and 38% involved meth. The greatest rate increase from 2012 to 2018 was in cocaine plus opioid-related overdose deaths, which was over four times (4.22 times) higher in 2018 compared to 2012.
Just over half of stimulant-involved overdose deaths included other substances.
Just over half (54%) of stimulant-involved overdose deaths also involved another substance. Most (88%) of polysubstance-involved overdose deaths involved opioids, with 48% of all stimulant-involved overdose deaths co-involving opioids. Of stimulant and opioid co-involved overdose deaths, 46% involved synthetic opioids (e.g., fentanyl), 45% involved heroin, and 26% involved prescription opioids. The most common substance besides opioids was alcohol, with 76% of stimulant-involved overdose deaths that involved another substance beside opioids involving alcohol.
Fatal overdoses involving cocaine differed from those involving meth.
Overdose deaths involving meth were more common in rural localities compared to those involving cocaine and cocaine plus opioids, 2.7 times higher among meth alone and 1.8 times higher among meth plus opioids respectively. For older adults (65+) compared to young adults (18-29), an overdose involving cocaine alone was 4.5 times more likely as one involving meth alone. An overdose death involving cocaine alone was also 14.3 times as likely among Black non-Hispanic versus White compared to those involving meth alone. Similarly, death involving meth plus opioids was 0.08 times less likely compared to death involving cocaine plus opioids among Black non-Hispanic versus White. Overdose death involving cocaine plus opioids were 3.1 times more likely among Hispanic versus White compared to meth plus opioid deaths.
Those involved in a cocaine alone or cocaine plus opioid death were 1.6 and 1.7 times more likely to also have a stimulant use disorder compared to meth along and meth plus opioid deaths respectively. Treatment utilization, however, was similar between cocaine- or meth-involved overdose deaths.
Patient characteristics differed among stimulant deaths that also involved opioids versus stimulants alone.
Overdose deaths that involved a stimulant plus opioids, rather than a stimulant alone, were more likely to occur among people under 30 years old compared to those in middle or later life. Similarly, overdose deaths involving both simulants and opioids, versus a stimulant alone, were more likely among Whites compared to Black non-Hispanics. Cocaine and opioid co-involved overdose deaths were 1.42 times more likely among those with a depressive disorder, 5.11 time more likely among those with an opioid use disorder and 0.55 times less likely among those with a stimulant use disorder compared to cocaine alone overdose deaths. Conversely, meth and opioid co-involved overdose deaths were 1.47 times more likely among those with a post-traumatic stress disorder, 6.29 times more likely among those with an opioid use disorder, and 0.44 times less likely among those with a stimulant use disorder. If opioids were co-involved with a stimulant, the individual was more likely to have an opioid use disorder diagnosis than a stimulant use disorder diagnosis.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The overdose crisis has been conceptualized as a triple wave phenomenon. The first wave was from 1999 to 2010 and was primarily due to prescription opioids. The second wave began in 2010 with sharp rises in heroin-related overdose deaths. The third wave began in 2014 when synthetic opioids-related (mainly fentanyl and fentanyl analogs) overdose rose dramatically. However, we may now be in a fourth wave of high mortality involving both opioids and stimulants. Perhaps overshadowed by the focus on opioids, stimulant-related overdose deaths have been on the rise, with a 3-fold and 6-fold increase in cocaine and meth involved overdoes dose deaths from 2012-2019.
This study highlights the rising trend of stimulant-involved overdose deaths among Veterans in the U.S. from 2012 to 2018 and explores clinical and health-care utilization characteristics of patients across stimulant-related overdose deaths. The study found that stimulant-involved overdose deaths was 3.06 times higher in 2018 than 2012. The sharpest increase in overdose deaths was cocaine plus opioids (4.22 times higher in 2018 than 2012).
This study also found that Black non-Hispanic patients were overrepresented across stimulant-involved overdose deaths, particularly cocaine-involved, relative to the racial and ethnic composition of the Veterans Health Administration. This mirrors findings from the general U.S. population on the racial disparities in opioid involved death rates – the rate of opioid involved death rates has increased more among African Americans than Whites (199% vs 77% from 2013-2018). Racial disparities in overdose deaths, among the general population and the VA, highlight the need for equity in overdose prevention, intervention, and treatment resources.
Polysubstance involved overdose deaths made up over half (54%) of overdose deaths related to stimulants, with most (88%) comprising of a stimulant and an opioid. Similarly, in Massachusetts from 2014 to 2015, 83% of opioid-involved overdose deaths involved another substance in addition to an opioid. The most common non-opioid substance involved in stimulant-involved overdose death in this study was alcohol, comprising 76.3% of stimulated plus non-opioid substance-involved overdose deaths. The second most common non-opioid substance group involved in stimulant-involved overdose death was barbiturates or benzodiazepines, comprising 19.1% of stimulant plus non-opioid overdose deaths. Thus, 95.4% of non-opioid substances included respiratory-depressing drugs, which increase the risk of overdose mortality generally and especially if used alongside opioids.
Polysubstance use is on the rise as well, and findings from this study confer that patients using multiple substances have more severe clinical profiles than their single substance using counterparts. In this study, patients using cocaine plus opioids were more likely to also be diagnosed with depressive disorder and opioid use disorder as well as report 3 or more other medical comorbidities. However, only 29.9% of patients who died of a stimulant-involved overdose were seen in specialty substance use settings in the past year, underscoring the need to increase resources for people who use substances (i.e., overdose prevention, intervention, and treatment). Furthermore, unique, modifiable treatment plans may be required for polysubstance use. For example, contingency management is the most empirically support treatment for stimulant use, and it may be coupled with medication for opioid use disorder to address stimulant and opioid co-use.
This study also pinpointed important differences between overdose deaths involving cocaine versus meth. Meth overdose death was more likely in rural settings, driven less by combined substances, more likely among older (65+) adults, and less likely to appear alongside a stimulant use disorder diagnosis compared to cocaine. While this finding fits with previous evidence that meth is more prevalent, easily accessible, and available at a low cost in rural settings, these trends are also changing. Although meth has been more prevalent in the Midwest, the largest relative increase in death rates occurred in the Northeast from 2018 to 2019 in the general population. The geographic changes in meth use are also accompanied by changes in potency, availability, and affordability broadly, which have all been increasing since the 1990s.
Additionally, stimulants being contaminated with fentanyl in the U.S. and Canada poses a significant risk, which would disproportionately impact opioid-naïve stimulant users due to their low tolerance and result in increased deaths. More empirical work is needed to explore if the shifting trends in meth and its use are also accompanied by changes in who uses it and experiences of related harms.
Taken together, this study draws attention to the rise in stimulant-related overdose deaths among Veterans as well as unique patient profiles associated with those deaths. The study pinpoints the need to prioritize prevention and treatment efforts among this vulnerable population. Moreover, the study amplifies the need to consider polysubstance use in screening, treatment, and retention planning. For example, patients with a co-involved stimulant and opioid overdose death were much less likely to have a stimulant use disorder diagnosis but more likely to have an opioid use disorder diagnosis. More research is needed to explore why these differences appear. Interventions aimed at reducing fatal overdoses may need to account more for stimulant and polysubstance use instead of focusing exclusively on opioid use.
Stimulant-related deaths, as well as other substance use-deaths, can only be identified to the degree that toxicology analyses are run, and substances are indicated on death certificates. This leads to under-reporting of substance involvement in deaths.
Cause of death coding only discriminates between cocaine and other psychostimulants. Although evidence suggests nearly all of the other psychostimulants are meth, the results here are unable to disentangle the other psychostimulants category.
The sample is limited to Veterans that have received care in the Veterans Health Administration. The degree to which these findings generalize outside the VA is not known.
BOTTOM LINE
Although opioids continue to drive the overdose crisis in the U.S., stimulant-involved overdose deaths have increased more than threefold from 2012 to 2018 among Veterans seen at a Veterans Health Administration medical facility in the year prior to death. Patient characteristics differ between cocaine and meth-involved deaths. Also, most stimulant-involved deaths involved another substance — primarily opioids. The rising stimulant polysubstance involved overdose deaths suggests that substance use treatment planning would likely benefit from identifying all substances a person uses or is likely to use along with stimulants, including alcohol and opioid. Policy that increases awareness and access to helpful treatments for polysubstance use would also be likely to reduce overdose deaths. Research that identifies effective screening, intervention, and treatment of potentially fatal stimulant use would likely reduce overdose mortality as well. More generally, public health policies are needed that can address the complex role of stimulants and polysubstance use in overdose deaths.
For individuals and families seeking recovery: Stimulant-involved overdose deaths are increasing across the U.S., including among vulnerable groups such as Veterans. Given how prevalent opioid use is among stimulant-involved overdose deaths, having naloxone around could prevent an overdose death. Also, it is possible that meth or cocaine may contain opioids like fentanyl without the end user knowing. Naloxone, an opioid overdose antidote, is also available with and without a prescription at most pharmacies as well as community-based harm reduction programs so, again, having this available may be lifesaving.
For treatment professionals and treatment systems: The authors found that stimulant-involved overdose deaths are increasing among Veterans seen at a Veterans Health Administration medical facility in the year prior to death. Most of these deaths involved another substance, mostly opioids. Those living in rural areas more likely to experience a meth-involved overdose death compared to those in urban areas. By targeting polysubstance use as well as other key factors such as locality, comorbidities, and health care access, treatment programs can address the unique constellations of risk and protective factors for individuals. Identifying these key characteristics will likely assist in aligning effective treatments at the right time for individuals.
For scientists: The overdose crisis continues to be among the most pressing public health concerns of our time. This study sought to explore stimulant-involved overdose deaths specifically by linking national mortality data with Veterans Health Administration data. Stimulant-involved overdoses increased threefold from 2012-2018, with most overdoses also involving another substance (e.g., opioids). The study also found that patient characteristics differed between cocaine and meth-involved overdose deaths. Research is needed to further bring to light the modifiable determinants of stimulant alone and stimulant co-involvement overdose deaths. More work is also needed to understand and address the racial and ethnic disparities found in simulant-involved overdose deaths, with black non-Hispanics being overrepresented in deaths. Future screening, prevention, and treatment would likely benefit from replicating this study among populations other than Veterans. Work that identifies what treatments, supports, and resources work best for whom can ultimately help to improve overdose prevention and response effort.
For policy makers: Although there has been growing public health policy support in the U.S. to address the opioid overdose crisis, more attention may need to be directed toward stimulants and polysubstance use. This study found increasing trends in stimulant-involved overdose deaths and high rates of polysubstance-involved overdoses, especially those that also include opioids. These findings highlight the need to advance the research on prevention, intervention, and treatment strategies for stimulant use and polysubstance use. Increasing access to health care and implementation of evidence-based supports will likely lead to improved public health.