A 20-year study of heroin use disorder: Patterns and predictors of remission, recurrence, and continued use
Studies that follow people with addiction for long periods of time improve our understanding of its natural course and how different types of treatment may affect it. However, these types of studies are difficult and expensive to conduct and are therefore relatively rare in addiction treatment research. In this Australian study, however, people with heroin use disorder were followed for 20 years and the patterns and predictors of use were examined.
Opioid use disorder, particularly heroin use disorder, has been described as a chronic, relapsing disease. Long-term studies have shown that the mortality rate for people with heroin use disorder is up to 20 times higher than the general population. In addition, there is considerable variability in the life course of people with opioid use disorder. Substance use, as well as related health and social problems persist over time for many, while others initiate and sustain remission and recovery.
Longitudinal studies that follow people with addictions over many years are uncommon in addiction research but are crucial to better understanding the course of addiction over time and how different types of treatment affect it.
This is especially critical for people with opioid use disorder, where there is strong evidence that treatment with agonist medications, such as methadone and buprenorphine, improves many outcomes (e.g., mortality, retention, and illicit opioid use) but recommendations around duration of medication treatment are still ambiguous (e.g., lifelong vs time-limited treatment with medications). In this study, participants were recruited from both treatment and non-treatment settings in Australia and followed over a 20-year period. Researchers examined patterns of heroin use, heroin use disorder, and other substance use over time and whether any of these substance use outcomes were related to treatment, demographics, or health and social problems. A better understanding of the natural history of heroin users is vital to inform policy interventions and treatment recommendations.
HOW WAS THIS STUDY CONDUCTED?
This study used a naturalistic, longitudinal design that followed 401 people who met DSM-IV diagnostic criteria for heroin dependence (subsequently referred to as “people with severe heroin use disorder”) over a period of 18-20 years to examine substance use patterns, clinical and demographic characteristics, and health and social problems, as well as the relationships among these.
The study was conducted in Sydney, Australia as part of the Australian Treatment Outcome Study and authors analyzed data from the initial cohort of 615 individuals enrolled through different treatment modalities: 201 individuals were enrolled from methadone or buprenorphine (often prescribed in combination with naloxone, and known by its brand name Suboxone) pharmacotherapy, 201 individuals were enrolled from opioid detoxification, and 133 individuals were enrolled from residential programs, as well as 80 non-treatment seekers with severe heroin use disorder who were enrolled through a syringe service program.
Participants were randomly selected from within each treatment modality and came from a wide range of facilities (18) in the area. Participants were followed up after 1 month, 3 months, and 1,2,3,11, and 18-20 years. This study examines 65.2% of the original cohort who remained in the study after 18 to 20 years.
Study participants were measured at baseline and at follow-up on a wide range of characteristics using interview-based assessments. These characteristics included demographics (including age, sex, main source of income), past-month heroin and other drug use, severe heroin use disorder, treatment history, injection-related health problems, past-month criminal involvement, general physical and mental health, major depression, post-traumatic stress disorder, and personality disorders. Heroin dependence was measured using DSM-IV diagnostic criteria and treatment use was measured by asking participants the number of times they received treatment for heroin use since their last interview, the treatment type, and the duration of each treatment episode. Treatment was operationally defined in this study as detoxification, maintenance therapy (i.e., methadone, buprenorphine), or a residential program. Researchers used a “life chart” approach to aid memory recall over the 18- to 20-year period, which anchors interview questions to significant events in the participants’ lives.
At baseline, two-thirds were male and the average age was 29.3 years;6% reported having a university degree, most reported government assistance or criminal activity as their main source of income in the past month (46% and 24% respectively), 55% reported criminal activity in the past month, and 41% reported time spent in prison. Average duration of heroin use was 9.6 years, 25% met criteria for major depression in the past month, and 41% met criteria for lifetime post-traumatic stress disorder as measured by DSM-IV diagnostic criteria. The sample re-interviewed after 18-20 years was broadly representative of the initial cohort.
The researchers examined the trends in heroin use, heroin use disorder, and other substance use over time. They also tested whether demographics, clinical characteristics, or different types of treatment use were associated with these substance-related outcomes. In addition, the researchers examined if health and social problems (e.g., physical and mental health scores as measured by the Short-Form 12, injection-related health problems, nonfatal overdose, criminal activity) were associated with demographics, clinical characteristics, or different types of treatment use. Analyses controlled statistically for baseline characteristics and accounted for repeated measures within a longitudinal design. A similar type of analysis was conducted at 11-year follow-up with this same cohort. A protocol for this study is available for more information on the study design.
WHAT DID THIS STUDY FIND?
Heroin use and heroin use disorder dropped significantly over the time period, but mortality was high.
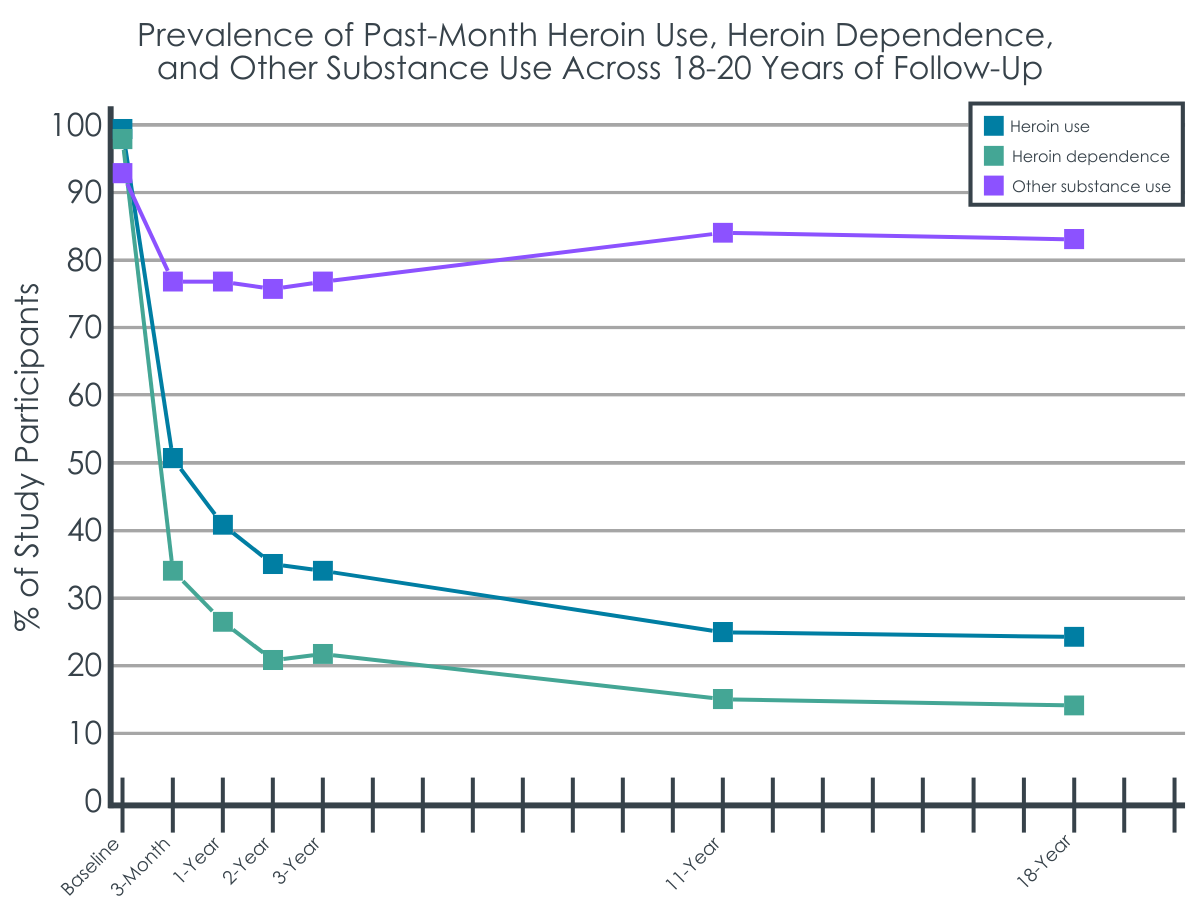
There were sharp declines in heroin use and severe heroin use disorder in the first two years of this cohort study followed by steady declines until 18-20 years. At this latest interview, only 24% of study participants reported heroin use in the past month and 14% met criteria for severe heroin use disorder (i.e., met DSM-IV diagnostic criteria for heroin dependence). However, 83% reported other substance use collapsed across all other substance classes (e.g., alcohol, stimulants, cannabis, etc.). More than 100 study participants (n = 109) from the original cohort were deceased at the 18-20 year follow-up, representing 18% of the study participants. Given that the average age at baseline was 29.3 years, this represents a staggering number of years of life lost and is similar to the substantially shorter lifespans observed in other substance use disorders, such as alcohol use disorder.
Treatment use was high and there were different relationships between types of treatment and heroin use, severe heroin use disorder, and other substance use.
At the 18–20-year follow-up, nearly half of study participants reported currently receiving treatment for their heroin use, with 36% receiving maintenance therapies. During the follow-up period (from 11 years since the study began to 18-20 years since the study began), 68% reported any treatment use, 64% reported maintenance therapy, 19% reported detoxification, and 18% reported residential rehabilitation. Detoxification was associated with increased heroin use, severe heroin use disorder, and other substance use, residential program attendance was associated with a decrease in these same outcomes, and maintenance therapy was associated with increased likelihood of other substance use.
People with major depression generally did not do as well.
Study participants who had major depression at baseline did consistently worse than study participants who did not have this condition. Major depression was associated with increased heroin use, severe heroin use disorder, and other substance use as well as injection-related health problems, needle sharing, criminal activity, and worse physical and mental health scores.
Treatment was associated with decreased health and social problems in some cases, increased health and social problems in others.
Injection-related health problems, needle sharing, criminal activity, and nonfatal overdose dropped sharply in the first two years of this cohort study followed by stable rates up until 18-20 years. Physical and mental health scores increased slightly in the first two years of this cohort study followed by stable rates up until 18-20 years. Maintenance therapy since the last follow-up was associated with decreased nonfatal overdoses, detoxification was associated with worsening health and social problems generally, and residential rehabilitation was associated with decreased injection-related health problems, less needle sharing and criminal activity, but increased nonfatal overdose.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Around one-fourth of participants reported heroin use, 14% reported severe heroin use disorder, and 83% reported other substance use nearly 20 years after enrolling in the cohort study, with 18% of the original cohort deceased. Maintenance pharmacotherapies and residential rehabilitation were associated with differential positive effects while detoxification was associated with many different negative effects. People with psychiatric illness, especially major depression, tended to have worse outcomes.
The impact of treatment was not straightforward in this study as evident by the different relationships between treatment use and substance use outcomes. Detoxification was associated with many different negative effects and supports the body of literature that detoxification alone is harmful for people with opioid use disorder. Maintenance therapies, which are supported by strong evidence showing mortality reduction, were expectedly associated with decreased nonfatal overdoses but were also associated with increased likelihood of other substance use and surprisingly was not associated with heroin use and severe heroin use disorder rates. Residential program attendance was associated with decreased heroin use, severe heroin use disorder, and other substance use but was also associated with increased nonfatal overdoses.
More research is needed to derive treatment recommendations from these study results. Because mortality was not accounted for in this study (i.e., the study did not account for how mortality may have varied depending on different treatment exposures and only examined people who were still alive after 18-20 years), using these observational findings to decide treatment recommendations should be done very cautiously. For example, many more people exposed to residential rehabilitation may have experienced death compared to those exposed to maintenance therapies over this long study period, leaving a selected subset of people who found success with residential rehabilitation. Furthermore, other research has suggested that residential rehabilitation plus maintenance therapy could produce the best results. Given that study participants with other psychiatric illnesses, especially major depression, generally had worse outcomes, aggressively addressing co-occurring mental health conditions treatment may be life-saving.
Another limitation of this study that clouds treatment recommendations is that we cannot say for sure whether certain types of treatment led to an improvement in substance use outcomes or if these outcomes, in some cases, were predictors of treatment-seeking for certain types of treatment (also known as bidirectional causality). Prospective studies can minimize this limitation and this study’s substance use outcomes were reported for the past 30 days whereas treatment use could have occurred anytime from the period from 11 years to 18-20 years since the study. However, we cannot be certain that treatment use preceded substance use outcomes for all study participants as many of these individuals were currently in treatment as reported in the follow-up interview.
There may also be a subset of individuals who have achieved long-term abstinence from heroin and other substances and who did not report treatment use during the period from 11 years to 18-20 years since the study began because they have been in recovery for a decade or more. Although this group of individuals would be interesting to examine, a different study design would be needed. A previous study using this same cohort up to the 11-year follow-up was done to look at different clusters of individuals, such as this unique cluster who achieved long-term abstinence soon after the study began, which represented 13% of study participants.
There is evidence from this study that clinically significant levels of improvement can be maintained over the long term without necessarily achieving abstinence from all substances. More than 80% of study participants reported other substance use, although it is unclear if this use is problematic or not. While abstinence from all substances may be the most suitable and stable pathway to wellness for some, and is associated with higher levels of quality of life and functioning, these data are consistent with the National Recovery Study which shows that for United States adults who report resolving a substance use problem, about half continue to use alcohol or other drugs. More research is needed to understand flesh out such findings, but what is clear is the important role that harm reduction services can play for people with heroin use disorder, as this cohort had high rates of heroin use, injection-related health problems, and mortality and very high rates of other substance use.
Finally, the context within which this study was done is very important in generalizing these findings to other parts of the world. Australia has a universal healthcare system and their drug policy, although differing by state, tends to support lighter penalties and diversion from the criminal justice system compared with other countries. Drug policy, treatment access, and substance use may be very different in other countries, such as the United States, limiting the generalizability of these study findings.
Although the attrition rate (i.e., people dropping out of the study) was relatively low for a study this long, a large portion of the cohort died during the study period. Without accounting for characteristics associated with these deaths, association of treatment use and outcomes as well as other relationships in this study could be misleading.
Generalizing these findings to other countries or states should be done with caution given the potential for differences in drug policy, treatment access, and substance use.
Substance use and other outcomes were measured using a structured interview and participants had to recall events that may have happened years ago. Social desirability bias and recall bias may have affected these measurements.
The study does not appear to capture other types of treatment, such as outpatient treatment, mutual help organizations, and behavioral health counseling, which may have impacted substance use outcomes.
This cohort study began with people with severe heroin use disorder (i.e., met DSM-IV diagnostic criteria for heroin dependence). Ideally, a cohort study would want to follow the general population to see who would use heroin and who would develop heroin use disorder so that protective and risk factors could be examined.
BOTTOM LINE
This study that followed 401 people with severe heroin use over a period of 18-20 years found that one-fourth of participants reported heroin use, 14% reported severe heroin use disorder, and 83% reported other current substance use nearly 20 years after enrolling in the cohort study, with 18% of the original cohort decreased. Maintenance therapies and residential program attendance were associated with differential positive effects while detoxification was associated with many different negative effects, presumably because detoxification that is not paired with treatment is likely to produce harms. People with co-occurring psychiatric disorders at baseline, especially major depression, tended to have worse outcomes.
For individuals and families seeking recovery: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. Harm reduction strategies are critical during periods of substance use. Maintenance therapies and residential programs may have differential positive effects and may have the greatest impact when used together. Treating underlying mental health conditions, such as major depression, should be a component of any type of treatment for heroin use disorder.
For treatment professionals and treatment systems: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. Because mortality was not accounted for in this study (i.e., the study did not account for how mortality may have varied depending on different treatment exposures and only examined people who were still alive after 18-20 years), using these results to inform or recommend different types of treatment should be done cautiously. For example, many more people exposed to residential programs may have experienced death compared to those exposed to maintenance therapies over this long study period, leaving a selected subset of people who found success with residential treatment. What is clear is: 1) the important role of harm reduction in people with heroin use disorder, as this cohort had high rates of heroin use, injection-related health problems, and mortality and very high rates of other substance use, 2) treating underlying mental health conditions, such as the presence of independently co-occurring major depression, should be a component of any type of treatment for heroin use disorder.
For scientists:Long-term cohort studies, especially in addiction research, are rare given the costs, time, and human resources needed to conduct such a study. Other study designs could be employed to further examine this cohort, such as clustering analyses that look at different classes that may exhibit the phenomenon of natural recovery or individuals who do not respond well to treatment. Predictors of mortality (both drug- and non-drug-related) could be incorporated into study findings to improve treatment and policy recommendations.
For policy makers: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. The best treatment modalities are likely comprehensive ones that incorporate maintenance therapies, such as buprenorphine and methadone, with aspects of residential care and include treatment for underlying mental health conditions, such as major depression, linkage to recovery support services, and the use of harm reduction strategies. Many people with heroin use disorder often will experience multiple episodes of treatment sometimes followed by recurrence of use, so policies that support reengagement in treatment rather than punishment for recurrent use (e.g., criminal justice consequences) are paramount. This type of study (a long-term cohort study) is expensive and resource-intensive but may elucidate treatment and policy recommendations that cannot be gleaned from more short-term studies.
Opioid use disorder, particularly heroin use disorder, has been described as a chronic, relapsing disease. Long-term studies have shown that the mortality rate for people with heroin use disorder is up to 20 times higher than the general population. In addition, there is considerable variability in the life course of people with opioid use disorder. Substance use, as well as related health and social problems persist over time for many, while others initiate and sustain remission and recovery.
Longitudinal studies that follow people with addictions over many years are uncommon in addiction research but are crucial to better understanding the course of addiction over time and how different types of treatment affect it.
This is especially critical for people with opioid use disorder, where there is strong evidence that treatment with agonist medications, such as methadone and buprenorphine, improves many outcomes (e.g., mortality, retention, and illicit opioid use) but recommendations around duration of medication treatment are still ambiguous (e.g., lifelong vs time-limited treatment with medications). In this study, participants were recruited from both treatment and non-treatment settings in Australia and followed over a 20-year period. Researchers examined patterns of heroin use, heroin use disorder, and other substance use over time and whether any of these substance use outcomes were related to treatment, demographics, or health and social problems. A better understanding of the natural history of heroin users is vital to inform policy interventions and treatment recommendations.
HOW WAS THIS STUDY CONDUCTED?
This study used a naturalistic, longitudinal design that followed 401 people who met DSM-IV diagnostic criteria for heroin dependence (subsequently referred to as “people with severe heroin use disorder”) over a period of 18-20 years to examine substance use patterns, clinical and demographic characteristics, and health and social problems, as well as the relationships among these.
The study was conducted in Sydney, Australia as part of the Australian Treatment Outcome Study and authors analyzed data from the initial cohort of 615 individuals enrolled through different treatment modalities: 201 individuals were enrolled from methadone or buprenorphine (often prescribed in combination with naloxone, and known by its brand name Suboxone) pharmacotherapy, 201 individuals were enrolled from opioid detoxification, and 133 individuals were enrolled from residential programs, as well as 80 non-treatment seekers with severe heroin use disorder who were enrolled through a syringe service program.
Participants were randomly selected from within each treatment modality and came from a wide range of facilities (18) in the area. Participants were followed up after 1 month, 3 months, and 1,2,3,11, and 18-20 years. This study examines 65.2% of the original cohort who remained in the study after 18 to 20 years.
Study participants were measured at baseline and at follow-up on a wide range of characteristics using interview-based assessments. These characteristics included demographics (including age, sex, main source of income), past-month heroin and other drug use, severe heroin use disorder, treatment history, injection-related health problems, past-month criminal involvement, general physical and mental health, major depression, post-traumatic stress disorder, and personality disorders. Heroin dependence was measured using DSM-IV diagnostic criteria and treatment use was measured by asking participants the number of times they received treatment for heroin use since their last interview, the treatment type, and the duration of each treatment episode. Treatment was operationally defined in this study as detoxification, maintenance therapy (i.e., methadone, buprenorphine), or a residential program. Researchers used a “life chart” approach to aid memory recall over the 18- to 20-year period, which anchors interview questions to significant events in the participants’ lives.
At baseline, two-thirds were male and the average age was 29.3 years;6% reported having a university degree, most reported government assistance or criminal activity as their main source of income in the past month (46% and 24% respectively), 55% reported criminal activity in the past month, and 41% reported time spent in prison. Average duration of heroin use was 9.6 years, 25% met criteria for major depression in the past month, and 41% met criteria for lifetime post-traumatic stress disorder as measured by DSM-IV diagnostic criteria. The sample re-interviewed after 18-20 years was broadly representative of the initial cohort.
The researchers examined the trends in heroin use, heroin use disorder, and other substance use over time. They also tested whether demographics, clinical characteristics, or different types of treatment use were associated with these substance-related outcomes. In addition, the researchers examined if health and social problems (e.g., physical and mental health scores as measured by the Short-Form 12, injection-related health problems, nonfatal overdose, criminal activity) were associated with demographics, clinical characteristics, or different types of treatment use. Analyses controlled statistically for baseline characteristics and accounted for repeated measures within a longitudinal design. A similar type of analysis was conducted at 11-year follow-up with this same cohort. A protocol for this study is available for more information on the study design.
WHAT DID THIS STUDY FIND?
Heroin use and heroin use disorder dropped significantly over the time period, but mortality was high.
There were sharp declines in heroin use and severe heroin use disorder in the first two years of this cohort study followed by steady declines until 18-20 years. At this latest interview, only 24% of study participants reported heroin use in the past month and 14% met criteria for severe heroin use disorder (i.e., met DSM-IV diagnostic criteria for heroin dependence). However, 83% reported other substance use collapsed across all other substance classes (e.g., alcohol, stimulants, cannabis, etc.). More than 100 study participants (n = 109) from the original cohort were deceased at the 18-20 year follow-up, representing 18% of the study participants. Given that the average age at baseline was 29.3 years, this represents a staggering number of years of life lost and is similar to the substantially shorter lifespans observed in other substance use disorders, such as alcohol use disorder.
Treatment use was high and there were different relationships between types of treatment and heroin use, severe heroin use disorder, and other substance use.
At the 18–20-year follow-up, nearly half of study participants reported currently receiving treatment for their heroin use, with 36% receiving maintenance therapies. During the follow-up period (from 11 years since the study began to 18-20 years since the study began), 68% reported any treatment use, 64% reported maintenance therapy, 19% reported detoxification, and 18% reported residential rehabilitation. Detoxification was associated with increased heroin use, severe heroin use disorder, and other substance use, residential program attendance was associated with a decrease in these same outcomes, and maintenance therapy was associated with increased likelihood of other substance use.
People with major depression generally did not do as well.
Study participants who had major depression at baseline did consistently worse than study participants who did not have this condition. Major depression was associated with increased heroin use, severe heroin use disorder, and other substance use as well as injection-related health problems, needle sharing, criminal activity, and worse physical and mental health scores.
Treatment was associated with decreased health and social problems in some cases, increased health and social problems in others.
Injection-related health problems, needle sharing, criminal activity, and nonfatal overdose dropped sharply in the first two years of this cohort study followed by stable rates up until 18-20 years. Physical and mental health scores increased slightly in the first two years of this cohort study followed by stable rates up until 18-20 years. Maintenance therapy since the last follow-up was associated with decreased nonfatal overdoses, detoxification was associated with worsening health and social problems generally, and residential rehabilitation was associated with decreased injection-related health problems, less needle sharing and criminal activity, but increased nonfatal overdose.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Around one-fourth of participants reported heroin use, 14% reported severe heroin use disorder, and 83% reported other substance use nearly 20 years after enrolling in the cohort study, with 18% of the original cohort deceased. Maintenance pharmacotherapies and residential rehabilitation were associated with differential positive effects while detoxification was associated with many different negative effects. People with psychiatric illness, especially major depression, tended to have worse outcomes.
The impact of treatment was not straightforward in this study as evident by the different relationships between treatment use and substance use outcomes. Detoxification was associated with many different negative effects and supports the body of literature that detoxification alone is harmful for people with opioid use disorder. Maintenance therapies, which are supported by strong evidence showing mortality reduction, were expectedly associated with decreased nonfatal overdoses but were also associated with increased likelihood of other substance use and surprisingly was not associated with heroin use and severe heroin use disorder rates. Residential program attendance was associated with decreased heroin use, severe heroin use disorder, and other substance use but was also associated with increased nonfatal overdoses.
More research is needed to derive treatment recommendations from these study results. Because mortality was not accounted for in this study (i.e., the study did not account for how mortality may have varied depending on different treatment exposures and only examined people who were still alive after 18-20 years), using these observational findings to decide treatment recommendations should be done very cautiously. For example, many more people exposed to residential rehabilitation may have experienced death compared to those exposed to maintenance therapies over this long study period, leaving a selected subset of people who found success with residential rehabilitation. Furthermore, other research has suggested that residential rehabilitation plus maintenance therapy could produce the best results. Given that study participants with other psychiatric illnesses, especially major depression, generally had worse outcomes, aggressively addressing co-occurring mental health conditions treatment may be life-saving.
Another limitation of this study that clouds treatment recommendations is that we cannot say for sure whether certain types of treatment led to an improvement in substance use outcomes or if these outcomes, in some cases, were predictors of treatment-seeking for certain types of treatment (also known as bidirectional causality). Prospective studies can minimize this limitation and this study’s substance use outcomes were reported for the past 30 days whereas treatment use could have occurred anytime from the period from 11 years to 18-20 years since the study. However, we cannot be certain that treatment use preceded substance use outcomes for all study participants as many of these individuals were currently in treatment as reported in the follow-up interview.
There may also be a subset of individuals who have achieved long-term abstinence from heroin and other substances and who did not report treatment use during the period from 11 years to 18-20 years since the study began because they have been in recovery for a decade or more. Although this group of individuals would be interesting to examine, a different study design would be needed. A previous study using this same cohort up to the 11-year follow-up was done to look at different clusters of individuals, such as this unique cluster who achieved long-term abstinence soon after the study began, which represented 13% of study participants.
There is evidence from this study that clinically significant levels of improvement can be maintained over the long term without necessarily achieving abstinence from all substances. More than 80% of study participants reported other substance use, although it is unclear if this use is problematic or not. While abstinence from all substances may be the most suitable and stable pathway to wellness for some, and is associated with higher levels of quality of life and functioning, these data are consistent with the National Recovery Study which shows that for United States adults who report resolving a substance use problem, about half continue to use alcohol or other drugs. More research is needed to understand flesh out such findings, but what is clear is the important role that harm reduction services can play for people with heroin use disorder, as this cohort had high rates of heroin use, injection-related health problems, and mortality and very high rates of other substance use.
Finally, the context within which this study was done is very important in generalizing these findings to other parts of the world. Australia has a universal healthcare system and their drug policy, although differing by state, tends to support lighter penalties and diversion from the criminal justice system compared with other countries. Drug policy, treatment access, and substance use may be very different in other countries, such as the United States, limiting the generalizability of these study findings.
Although the attrition rate (i.e., people dropping out of the study) was relatively low for a study this long, a large portion of the cohort died during the study period. Without accounting for characteristics associated with these deaths, association of treatment use and outcomes as well as other relationships in this study could be misleading.
Generalizing these findings to other countries or states should be done with caution given the potential for differences in drug policy, treatment access, and substance use.
Substance use and other outcomes were measured using a structured interview and participants had to recall events that may have happened years ago. Social desirability bias and recall bias may have affected these measurements.
The study does not appear to capture other types of treatment, such as outpatient treatment, mutual help organizations, and behavioral health counseling, which may have impacted substance use outcomes.
This cohort study began with people with severe heroin use disorder (i.e., met DSM-IV diagnostic criteria for heroin dependence). Ideally, a cohort study would want to follow the general population to see who would use heroin and who would develop heroin use disorder so that protective and risk factors could be examined.
BOTTOM LINE
This study that followed 401 people with severe heroin use over a period of 18-20 years found that one-fourth of participants reported heroin use, 14% reported severe heroin use disorder, and 83% reported other current substance use nearly 20 years after enrolling in the cohort study, with 18% of the original cohort decreased. Maintenance therapies and residential program attendance were associated with differential positive effects while detoxification was associated with many different negative effects, presumably because detoxification that is not paired with treatment is likely to produce harms. People with co-occurring psychiatric disorders at baseline, especially major depression, tended to have worse outcomes.
For individuals and families seeking recovery: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. Harm reduction strategies are critical during periods of substance use. Maintenance therapies and residential programs may have differential positive effects and may have the greatest impact when used together. Treating underlying mental health conditions, such as major depression, should be a component of any type of treatment for heroin use disorder.
For treatment professionals and treatment systems: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. Because mortality was not accounted for in this study (i.e., the study did not account for how mortality may have varied depending on different treatment exposures and only examined people who were still alive after 18-20 years), using these results to inform or recommend different types of treatment should be done cautiously. For example, many more people exposed to residential programs may have experienced death compared to those exposed to maintenance therapies over this long study period, leaving a selected subset of people who found success with residential treatment. What is clear is: 1) the important role of harm reduction in people with heroin use disorder, as this cohort had high rates of heroin use, injection-related health problems, and mortality and very high rates of other substance use, 2) treating underlying mental health conditions, such as the presence of independently co-occurring major depression, should be a component of any type of treatment for heroin use disorder.
For scientists:Long-term cohort studies, especially in addiction research, are rare given the costs, time, and human resources needed to conduct such a study. Other study designs could be employed to further examine this cohort, such as clustering analyses that look at different classes that may exhibit the phenomenon of natural recovery or individuals who do not respond well to treatment. Predictors of mortality (both drug- and non-drug-related) could be incorporated into study findings to improve treatment and policy recommendations.
For policy makers: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. The best treatment modalities are likely comprehensive ones that incorporate maintenance therapies, such as buprenorphine and methadone, with aspects of residential care and include treatment for underlying mental health conditions, such as major depression, linkage to recovery support services, and the use of harm reduction strategies. Many people with heroin use disorder often will experience multiple episodes of treatment sometimes followed by recurrence of use, so policies that support reengagement in treatment rather than punishment for recurrent use (e.g., criminal justice consequences) are paramount. This type of study (a long-term cohort study) is expensive and resource-intensive but may elucidate treatment and policy recommendations that cannot be gleaned from more short-term studies.
Opioid use disorder, particularly heroin use disorder, has been described as a chronic, relapsing disease. Long-term studies have shown that the mortality rate for people with heroin use disorder is up to 20 times higher than the general population. In addition, there is considerable variability in the life course of people with opioid use disorder. Substance use, as well as related health and social problems persist over time for many, while others initiate and sustain remission and recovery.
Longitudinal studies that follow people with addictions over many years are uncommon in addiction research but are crucial to better understanding the course of addiction over time and how different types of treatment affect it.
This is especially critical for people with opioid use disorder, where there is strong evidence that treatment with agonist medications, such as methadone and buprenorphine, improves many outcomes (e.g., mortality, retention, and illicit opioid use) but recommendations around duration of medication treatment are still ambiguous (e.g., lifelong vs time-limited treatment with medications). In this study, participants were recruited from both treatment and non-treatment settings in Australia and followed over a 20-year period. Researchers examined patterns of heroin use, heroin use disorder, and other substance use over time and whether any of these substance use outcomes were related to treatment, demographics, or health and social problems. A better understanding of the natural history of heroin users is vital to inform policy interventions and treatment recommendations.
HOW WAS THIS STUDY CONDUCTED?
This study used a naturalistic, longitudinal design that followed 401 people who met DSM-IV diagnostic criteria for heroin dependence (subsequently referred to as “people with severe heroin use disorder”) over a period of 18-20 years to examine substance use patterns, clinical and demographic characteristics, and health and social problems, as well as the relationships among these.
The study was conducted in Sydney, Australia as part of the Australian Treatment Outcome Study and authors analyzed data from the initial cohort of 615 individuals enrolled through different treatment modalities: 201 individuals were enrolled from methadone or buprenorphine (often prescribed in combination with naloxone, and known by its brand name Suboxone) pharmacotherapy, 201 individuals were enrolled from opioid detoxification, and 133 individuals were enrolled from residential programs, as well as 80 non-treatment seekers with severe heroin use disorder who were enrolled through a syringe service program.
Participants were randomly selected from within each treatment modality and came from a wide range of facilities (18) in the area. Participants were followed up after 1 month, 3 months, and 1,2,3,11, and 18-20 years. This study examines 65.2% of the original cohort who remained in the study after 18 to 20 years.
Study participants were measured at baseline and at follow-up on a wide range of characteristics using interview-based assessments. These characteristics included demographics (including age, sex, main source of income), past-month heroin and other drug use, severe heroin use disorder, treatment history, injection-related health problems, past-month criminal involvement, general physical and mental health, major depression, post-traumatic stress disorder, and personality disorders. Heroin dependence was measured using DSM-IV diagnostic criteria and treatment use was measured by asking participants the number of times they received treatment for heroin use since their last interview, the treatment type, and the duration of each treatment episode. Treatment was operationally defined in this study as detoxification, maintenance therapy (i.e., methadone, buprenorphine), or a residential program. Researchers used a “life chart” approach to aid memory recall over the 18- to 20-year period, which anchors interview questions to significant events in the participants’ lives.
At baseline, two-thirds were male and the average age was 29.3 years;6% reported having a university degree, most reported government assistance or criminal activity as their main source of income in the past month (46% and 24% respectively), 55% reported criminal activity in the past month, and 41% reported time spent in prison. Average duration of heroin use was 9.6 years, 25% met criteria for major depression in the past month, and 41% met criteria for lifetime post-traumatic stress disorder as measured by DSM-IV diagnostic criteria. The sample re-interviewed after 18-20 years was broadly representative of the initial cohort.
The researchers examined the trends in heroin use, heroin use disorder, and other substance use over time. They also tested whether demographics, clinical characteristics, or different types of treatment use were associated with these substance-related outcomes. In addition, the researchers examined if health and social problems (e.g., physical and mental health scores as measured by the Short-Form 12, injection-related health problems, nonfatal overdose, criminal activity) were associated with demographics, clinical characteristics, or different types of treatment use. Analyses controlled statistically for baseline characteristics and accounted for repeated measures within a longitudinal design. A similar type of analysis was conducted at 11-year follow-up with this same cohort. A protocol for this study is available for more information on the study design.
WHAT DID THIS STUDY FIND?
Heroin use and heroin use disorder dropped significantly over the time period, but mortality was high.
There were sharp declines in heroin use and severe heroin use disorder in the first two years of this cohort study followed by steady declines until 18-20 years. At this latest interview, only 24% of study participants reported heroin use in the past month and 14% met criteria for severe heroin use disorder (i.e., met DSM-IV diagnostic criteria for heroin dependence). However, 83% reported other substance use collapsed across all other substance classes (e.g., alcohol, stimulants, cannabis, etc.). More than 100 study participants (n = 109) from the original cohort were deceased at the 18-20 year follow-up, representing 18% of the study participants. Given that the average age at baseline was 29.3 years, this represents a staggering number of years of life lost and is similar to the substantially shorter lifespans observed in other substance use disorders, such as alcohol use disorder.
Treatment use was high and there were different relationships between types of treatment and heroin use, severe heroin use disorder, and other substance use.
At the 18–20-year follow-up, nearly half of study participants reported currently receiving treatment for their heroin use, with 36% receiving maintenance therapies. During the follow-up period (from 11 years since the study began to 18-20 years since the study began), 68% reported any treatment use, 64% reported maintenance therapy, 19% reported detoxification, and 18% reported residential rehabilitation. Detoxification was associated with increased heroin use, severe heroin use disorder, and other substance use, residential program attendance was associated with a decrease in these same outcomes, and maintenance therapy was associated with increased likelihood of other substance use.
People with major depression generally did not do as well.
Study participants who had major depression at baseline did consistently worse than study participants who did not have this condition. Major depression was associated with increased heroin use, severe heroin use disorder, and other substance use as well as injection-related health problems, needle sharing, criminal activity, and worse physical and mental health scores.
Treatment was associated with decreased health and social problems in some cases, increased health and social problems in others.
Injection-related health problems, needle sharing, criminal activity, and nonfatal overdose dropped sharply in the first two years of this cohort study followed by stable rates up until 18-20 years. Physical and mental health scores increased slightly in the first two years of this cohort study followed by stable rates up until 18-20 years. Maintenance therapy since the last follow-up was associated with decreased nonfatal overdoses, detoxification was associated with worsening health and social problems generally, and residential rehabilitation was associated with decreased injection-related health problems, less needle sharing and criminal activity, but increased nonfatal overdose.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Around one-fourth of participants reported heroin use, 14% reported severe heroin use disorder, and 83% reported other substance use nearly 20 years after enrolling in the cohort study, with 18% of the original cohort deceased. Maintenance pharmacotherapies and residential rehabilitation were associated with differential positive effects while detoxification was associated with many different negative effects. People with psychiatric illness, especially major depression, tended to have worse outcomes.
The impact of treatment was not straightforward in this study as evident by the different relationships between treatment use and substance use outcomes. Detoxification was associated with many different negative effects and supports the body of literature that detoxification alone is harmful for people with opioid use disorder. Maintenance therapies, which are supported by strong evidence showing mortality reduction, were expectedly associated with decreased nonfatal overdoses but were also associated with increased likelihood of other substance use and surprisingly was not associated with heroin use and severe heroin use disorder rates. Residential program attendance was associated with decreased heroin use, severe heroin use disorder, and other substance use but was also associated with increased nonfatal overdoses.
More research is needed to derive treatment recommendations from these study results. Because mortality was not accounted for in this study (i.e., the study did not account for how mortality may have varied depending on different treatment exposures and only examined people who were still alive after 18-20 years), using these observational findings to decide treatment recommendations should be done very cautiously. For example, many more people exposed to residential rehabilitation may have experienced death compared to those exposed to maintenance therapies over this long study period, leaving a selected subset of people who found success with residential rehabilitation. Furthermore, other research has suggested that residential rehabilitation plus maintenance therapy could produce the best results. Given that study participants with other psychiatric illnesses, especially major depression, generally had worse outcomes, aggressively addressing co-occurring mental health conditions treatment may be life-saving.
Another limitation of this study that clouds treatment recommendations is that we cannot say for sure whether certain types of treatment led to an improvement in substance use outcomes or if these outcomes, in some cases, were predictors of treatment-seeking for certain types of treatment (also known as bidirectional causality). Prospective studies can minimize this limitation and this study’s substance use outcomes were reported for the past 30 days whereas treatment use could have occurred anytime from the period from 11 years to 18-20 years since the study. However, we cannot be certain that treatment use preceded substance use outcomes for all study participants as many of these individuals were currently in treatment as reported in the follow-up interview.
There may also be a subset of individuals who have achieved long-term abstinence from heroin and other substances and who did not report treatment use during the period from 11 years to 18-20 years since the study began because they have been in recovery for a decade or more. Although this group of individuals would be interesting to examine, a different study design would be needed. A previous study using this same cohort up to the 11-year follow-up was done to look at different clusters of individuals, such as this unique cluster who achieved long-term abstinence soon after the study began, which represented 13% of study participants.
There is evidence from this study that clinically significant levels of improvement can be maintained over the long term without necessarily achieving abstinence from all substances. More than 80% of study participants reported other substance use, although it is unclear if this use is problematic or not. While abstinence from all substances may be the most suitable and stable pathway to wellness for some, and is associated with higher levels of quality of life and functioning, these data are consistent with the National Recovery Study which shows that for United States adults who report resolving a substance use problem, about half continue to use alcohol or other drugs. More research is needed to understand flesh out such findings, but what is clear is the important role that harm reduction services can play for people with heroin use disorder, as this cohort had high rates of heroin use, injection-related health problems, and mortality and very high rates of other substance use.
Finally, the context within which this study was done is very important in generalizing these findings to other parts of the world. Australia has a universal healthcare system and their drug policy, although differing by state, tends to support lighter penalties and diversion from the criminal justice system compared with other countries. Drug policy, treatment access, and substance use may be very different in other countries, such as the United States, limiting the generalizability of these study findings.
Although the attrition rate (i.e., people dropping out of the study) was relatively low for a study this long, a large portion of the cohort died during the study period. Without accounting for characteristics associated with these deaths, association of treatment use and outcomes as well as other relationships in this study could be misleading.
Generalizing these findings to other countries or states should be done with caution given the potential for differences in drug policy, treatment access, and substance use.
Substance use and other outcomes were measured using a structured interview and participants had to recall events that may have happened years ago. Social desirability bias and recall bias may have affected these measurements.
The study does not appear to capture other types of treatment, such as outpatient treatment, mutual help organizations, and behavioral health counseling, which may have impacted substance use outcomes.
This cohort study began with people with severe heroin use disorder (i.e., met DSM-IV diagnostic criteria for heroin dependence). Ideally, a cohort study would want to follow the general population to see who would use heroin and who would develop heroin use disorder so that protective and risk factors could be examined.
BOTTOM LINE
This study that followed 401 people with severe heroin use over a period of 18-20 years found that one-fourth of participants reported heroin use, 14% reported severe heroin use disorder, and 83% reported other current substance use nearly 20 years after enrolling in the cohort study, with 18% of the original cohort decreased. Maintenance therapies and residential program attendance were associated with differential positive effects while detoxification was associated with many different negative effects, presumably because detoxification that is not paired with treatment is likely to produce harms. People with co-occurring psychiatric disorders at baseline, especially major depression, tended to have worse outcomes.
For individuals and families seeking recovery: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. Harm reduction strategies are critical during periods of substance use. Maintenance therapies and residential programs may have differential positive effects and may have the greatest impact when used together. Treating underlying mental health conditions, such as major depression, should be a component of any type of treatment for heroin use disorder.
For treatment professionals and treatment systems: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. Because mortality was not accounted for in this study (i.e., the study did not account for how mortality may have varied depending on different treatment exposures and only examined people who were still alive after 18-20 years), using these results to inform or recommend different types of treatment should be done cautiously. For example, many more people exposed to residential programs may have experienced death compared to those exposed to maintenance therapies over this long study period, leaving a selected subset of people who found success with residential treatment. What is clear is: 1) the important role of harm reduction in people with heroin use disorder, as this cohort had high rates of heroin use, injection-related health problems, and mortality and very high rates of other substance use, 2) treating underlying mental health conditions, such as the presence of independently co-occurring major depression, should be a component of any type of treatment for heroin use disorder.
For scientists:Long-term cohort studies, especially in addiction research, are rare given the costs, time, and human resources needed to conduct such a study. Other study designs could be employed to further examine this cohort, such as clustering analyses that look at different classes that may exhibit the phenomenon of natural recovery or individuals who do not respond well to treatment. Predictors of mortality (both drug- and non-drug-related) could be incorporated into study findings to improve treatment and policy recommendations.
For policy makers: People with heroin use disorder have high mortality rates and may cycle in and out of problematic heroin use. The best treatment modalities are likely comprehensive ones that incorporate maintenance therapies, such as buprenorphine and methadone, with aspects of residential care and include treatment for underlying mental health conditions, such as major depression, linkage to recovery support services, and the use of harm reduction strategies. Many people with heroin use disorder often will experience multiple episodes of treatment sometimes followed by recurrence of use, so policies that support reengagement in treatment rather than punishment for recurrent use (e.g., criminal justice consequences) are paramount. This type of study (a long-term cohort study) is expensive and resource-intensive but may elucidate treatment and policy recommendations that cannot be gleaned from more short-term studies.