Can humanizing stories boost support for harm reduction? It depends on the message
Many people in the U.S. remain skeptical of substance use harm reduction services like syringe exchange programs and supervised consumption sites. One reason may be stigmatizing attitudes toward people who use drugs. This study tested whether descriptions of lowering personal responsibility or highlighting overdose risk in messaging can improve public support for harm reduction efforts.
Harm reduction strategies—including supervised consumption sites, syringe service programs, and naloxone distribution—have been shown to reduce drug overdose deaths and connect people to care. Yet despite their public health benefits, these services often face political resistance and limited implementation in the US.
Harm reduction services aim to minimize negative consequences of opioid use such as overdose, illness, and legal issues. They include:
• Overdose education: Teaching individuals and communities how to recognize and respond to an overdose.
• Naloxone (“Narcan”) distribution programs: Training and equipping laypersons with naloxone, a life-saving medication that reverses opioid overdoses. •Supervised consumption sites: Also called overdose prevention centers, these facilities allow individuals to use substances under medical supervision to prevent fatal overdoses. •Syringe service programs: Provide access to sterile injecting equipment to reduce the spread of infections like HIV and hepatitis C. •Drug checking services: Distribute tools to test drugs for dangerous adulterants like fentanyl, helping individuals make safer choices. •Decriminalization of heroin possession: Reduces or eliminates criminal penalties for possessing small amounts of drugs, aiming to redirect people toward health services rather than jail. •Heroin and medications for the treatment of opioid use disorder: Offers prescribed heroin for individuals unresponsive to other treatments, or methadone to manage withdrawal and cravings. • Good Samaritan Laws: Provide legal protection to individuals who call for emergency help during a drug overdose, encouraging timely medical intervention.
This study examined whether storytelling—a common and powerful communication tool—can shift public attitudes toward harm reduction. Across two experiments, the researchers manipulated key aspects of short stories about a person who uses heroin. In Study 1, the stories varied whether addiction was portrayed as controllable or uncontrollable. In Study 2, the stories either emphasized or omitted the risk of death from overdose. The researchers assessed how these different story elements influenced beliefs about personal responsibility for addiction and support for harm reduction policies.
HOW WAS THIS STUDY CONDUCTED?
The researchers conducted 2 online randomized trials to examine whether different types of storytelling could influence public support for harm reduction policies. A total of 536 US adults participated across both studies. Participants were recruited through a national online platform and represented a range of ages, political beliefs, and personal experiences with opioid use.
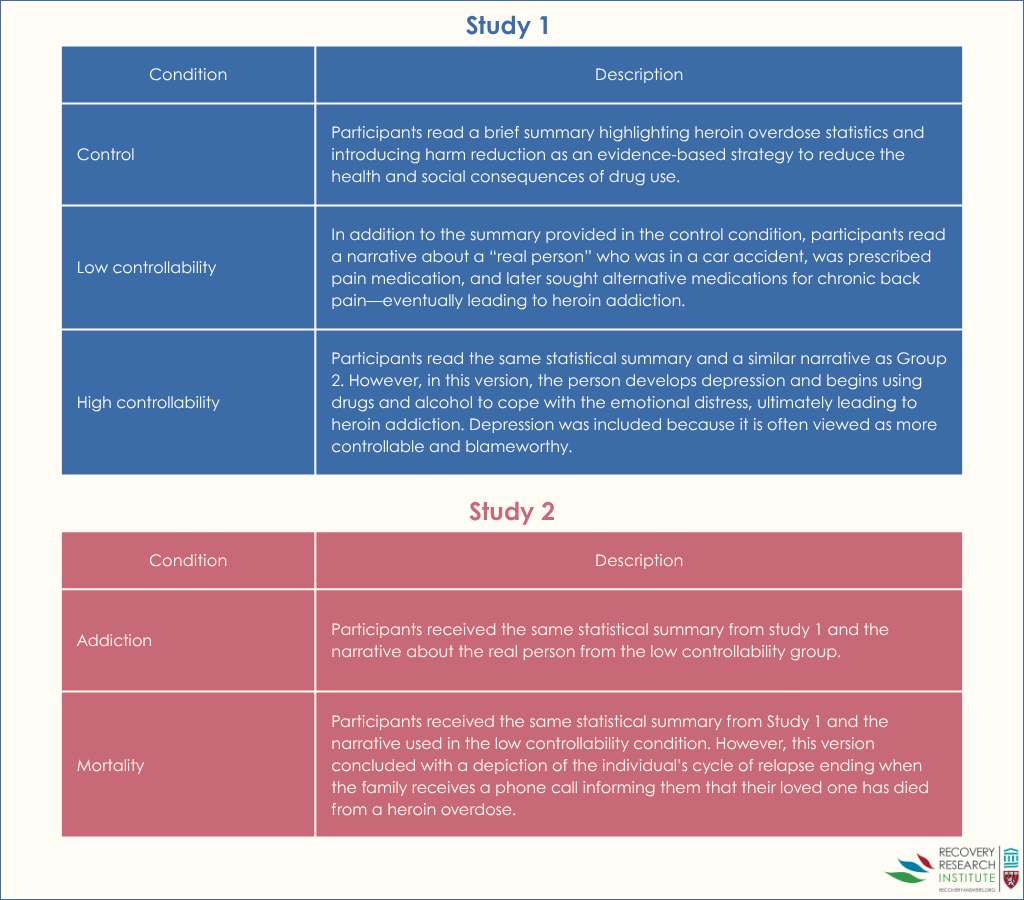
In Study 1, participants were randomly assigned to 1 of 3 conditions (see graphic below). One group read a neutral message with statistics about heroin and harm reduction. The other two groups read the same statistics followed by a humanizing story about a person who became addicted to heroin. In one version of the story (low-controllability), the person’s addiction stemmed from a car accident and pain management. In the other (high-controllability), the person’s addiction began during a period of depression, with the story suggesting more personal choice. After reading the messages, participants reported their beliefs about whether heroin addiction is controllable and how much they supported various harm reduction policies.
In Study 2, the researchers tested whether focusing on the severe outcome of overdose death might be more persuasive than changing beliefs about addiction (see graphic below). Participants read either the same humanizing narrative from the low-controllability condition in Study 1 or a nearly identical version that ended with the person dying of a heroin overdose. Participants then answered the same questions about harm reduction policy support. This allowed the researchers to isolate whether highlighting overdose risk increased support more than changing beliefs about controllability.
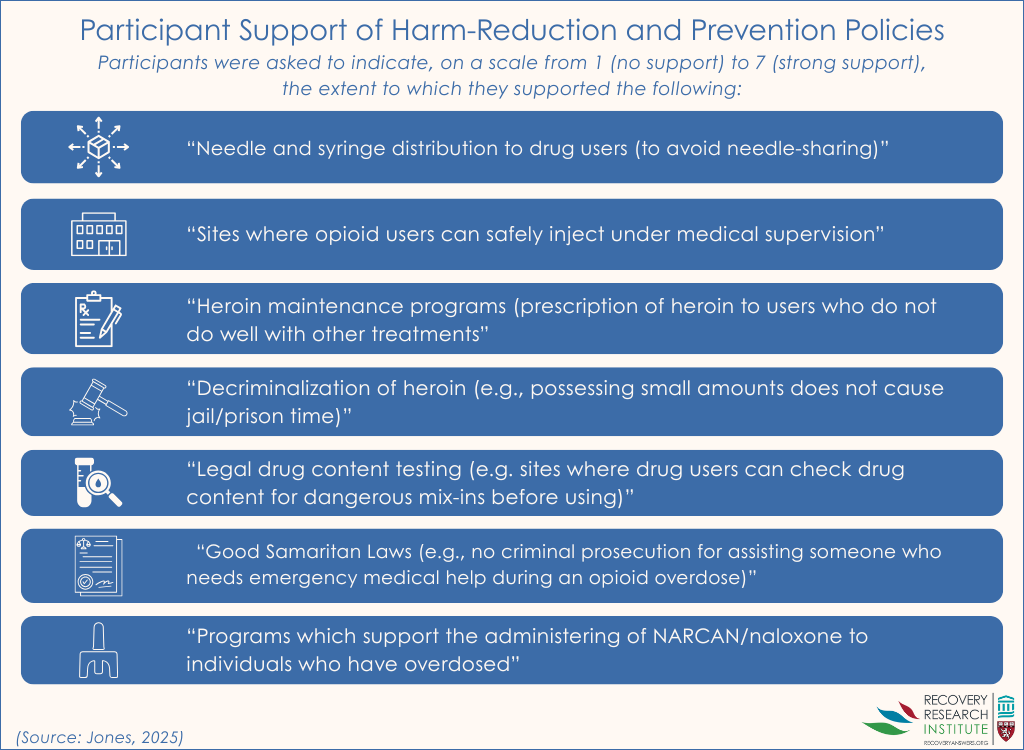
In both studies, the researchers used detailed, multi-item surveys to measure both controllability beliefs and support for 7 specific harm reduction policies (see graphic below), including syringe service programs, supervised consumption sites, heroin distribution or medication treatment for opioid use disorder, and Good Samaritan Laws. They also controlled for participant sex, political beliefs (especially support for small government), and personal or secondhand experience with opioid use. Such statistical adjustments help to isolate the effect of interest – i.e., whether the vignette type is independently related to harm reduction support.
WHAT DID THIS STUDY FIND?
Study 1: Humanizing stories reduced blame but did not increase policy support
Participants who read a humanizing story about a person who uses heroin were less likely to believe that addiction is fully within a person’s control. This suggests that storytelling can reduce stigma by shifting blame away from the individual. However, these changes in belief did not lead to increased support for harm-reduction policies. Even when the story emphasized that addiction was the result of medical or environmental factors, participants’ support for services like syringe programs or supervised consumption sites stayed about the same.
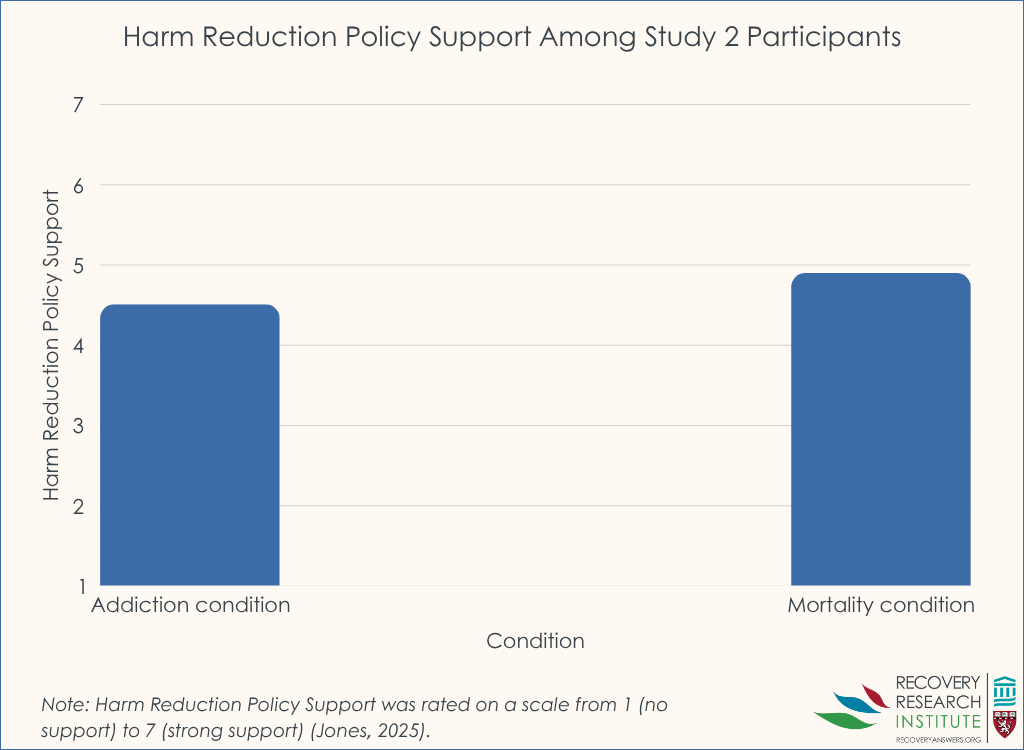
Study 2: Highlighting overdose death led to greater support for harm reduction
Participants who read about a person dying from a heroin overdose were more likely to support harm-reduction policies than those who read about addiction without that outcome. This effect remained even after accounting for participants’ political orientation and other factors. While the difference was not large, it was consistent and meaningful suggesting that even a small shift in how a story ends can influence public attitudes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that not all stigma-reduction messages are equally effective when it comes to shifting public support for harm-reduction policies. While humanizing narratives made participants less likely to blame individuals for their heroin use, they did not lead to stronger support for services like supervised consumption sites or naloxone distribution. In contrast, messages that highlighted the life-or-death consequences of opioid use—particularly the risk of fatal overdose—were better at changing attitudes toward policy.
These findings highlight the potential power of emotionally charged storytelling in public education campaigns. People may be more moved by stories that evoke concern for someone’s safety than by stories that simply reduce blame. Prior studies have shown that emotional appeals, such as messaging that elicits sympathy or pity, can be more effective than factual messages at shifting public opinion and increasing support for evidence-based policies.
Importantly, the results do not mean that reducing stigma is unimportant. Shifting beliefs about addiction as a moral failing or personal choice remains a critical goal, especially in healthcare and community settings where stigma can affect treatment access and quality of care. However, when the goal is to increase public support for harm-reduction policies, messages that underscore the real and immediate risks of overdose may be more persuasive. This emphasis on overdose risk may also apply to the names we use for these harm reduction services; for example, “overdose prevention sites” garner more public support than “safe consumption sites“.
For public health advocates and policymakers, these findings suggest that message framing matters. Campaigns that aim to build support for evidence-based harm reduction strategies may benefit from incorporating stories that reflect the harsh realities of opioid use, including the possibility of death. At the same time, these messages should be crafted carefully to avoid reinforcing hopelessness or stigma—highlighting the importance of combining emotional resonance with human dignity.
Participants’ knowledge of harm reduction was not measured. All participants were given a brief description of harm-reduction services, but the researchers did not assess what participants already knew—or misunderstood—about these services. People with more familiarity or stronger pre-existing opinions may have responded differently to the narratives.
The study focused only on heroin. The stories described a person using heroin, so the findings may not apply to other substances like fentanyl, methamphetamine, or prescription opioids. Public attitudes can differ depending on the drug involved, which could change how people respond to harm-reduction messaging.
The study only looked at short-term effects. Participants were surveyed right after reading the stories, so we don’t know if the changes in beliefs or policy support would last over time, or if this translates to actual changes in behavior, such as voting for or against a harm reduction policy. Long-term follow-up is needed to understand whether narrative messaging has a lasting impact.
BOTTOM LINE
Results suggest personal stories can help reduce stigma about addiction, but they may not be enough to increase public support for harm-reduction policies. Narratives that emphasize the risk of overdose death may be more effective in changing public attitudes toward these life-saving services.
For individuals and families seeking recovery: Stories can be powerful tools, especially those that help others understand the risks of untreated substance use. Talking openly about overdose risk may help build support for helpful services in your community.
For treatment professionals and treatment systems: When advocating for harm-reduction services, messages that underscore overdose risks may be more likely to shift public opinion than those focused only on reducing stigma.
For scientists: This randomized controlled online experiment indicates that while humanizing narratives can reduce stigma, they may not significantly increase public support for harm-reduction policies. In contrast, highlighting overdose death within a narrative led to a modest but statistically significant increase in policy support. Future research should explore the long-term effects of different narrative elements—such as emotional tone, framing, and content—on both stigma reduction and policy support, including actual policy support behavior. Additionally, examining how these effects vary across different substances and audience demographics could inform more effective public health messaging strategies.
For policy makers: Public support is key to advancing harm-reduction strategies. Messaging that centers on the serious consequences of untreated opioid use may be more persuasive in building that support.
Harm reduction strategies—including supervised consumption sites, syringe service programs, and naloxone distribution—have been shown to reduce drug overdose deaths and connect people to care. Yet despite their public health benefits, these services often face political resistance and limited implementation in the US.
Harm reduction services aim to minimize negative consequences of opioid use such as overdose, illness, and legal issues. They include:
• Overdose education: Teaching individuals and communities how to recognize and respond to an overdose.
• Naloxone (“Narcan”) distribution programs: Training and equipping laypersons with naloxone, a life-saving medication that reverses opioid overdoses. •Supervised consumption sites: Also called overdose prevention centers, these facilities allow individuals to use substances under medical supervision to prevent fatal overdoses. •Syringe service programs: Provide access to sterile injecting equipment to reduce the spread of infections like HIV and hepatitis C. •Drug checking services: Distribute tools to test drugs for dangerous adulterants like fentanyl, helping individuals make safer choices. •Decriminalization of heroin possession: Reduces or eliminates criminal penalties for possessing small amounts of drugs, aiming to redirect people toward health services rather than jail. •Heroin and medications for the treatment of opioid use disorder: Offers prescribed heroin for individuals unresponsive to other treatments, or methadone to manage withdrawal and cravings. • Good Samaritan Laws: Provide legal protection to individuals who call for emergency help during a drug overdose, encouraging timely medical intervention.
This study examined whether storytelling—a common and powerful communication tool—can shift public attitudes toward harm reduction. Across two experiments, the researchers manipulated key aspects of short stories about a person who uses heroin. In Study 1, the stories varied whether addiction was portrayed as controllable or uncontrollable. In Study 2, the stories either emphasized or omitted the risk of death from overdose. The researchers assessed how these different story elements influenced beliefs about personal responsibility for addiction and support for harm reduction policies.
HOW WAS THIS STUDY CONDUCTED?
The researchers conducted 2 online randomized trials to examine whether different types of storytelling could influence public support for harm reduction policies. A total of 536 US adults participated across both studies. Participants were recruited through a national online platform and represented a range of ages, political beliefs, and personal experiences with opioid use.
In Study 1, participants were randomly assigned to 1 of 3 conditions (see graphic below). One group read a neutral message with statistics about heroin and harm reduction. The other two groups read the same statistics followed by a humanizing story about a person who became addicted to heroin. In one version of the story (low-controllability), the person’s addiction stemmed from a car accident and pain management. In the other (high-controllability), the person’s addiction began during a period of depression, with the story suggesting more personal choice. After reading the messages, participants reported their beliefs about whether heroin addiction is controllable and how much they supported various harm reduction policies.
In Study 2, the researchers tested whether focusing on the severe outcome of overdose death might be more persuasive than changing beliefs about addiction (see graphic below). Participants read either the same humanizing narrative from the low-controllability condition in Study 1 or a nearly identical version that ended with the person dying of a heroin overdose. Participants then answered the same questions about harm reduction policy support. This allowed the researchers to isolate whether highlighting overdose risk increased support more than changing beliefs about controllability.
In both studies, the researchers used detailed, multi-item surveys to measure both controllability beliefs and support for 7 specific harm reduction policies (see graphic below), including syringe service programs, supervised consumption sites, heroin distribution or medication treatment for opioid use disorder, and Good Samaritan Laws. They also controlled for participant sex, political beliefs (especially support for small government), and personal or secondhand experience with opioid use. Such statistical adjustments help to isolate the effect of interest – i.e., whether the vignette type is independently related to harm reduction support.
WHAT DID THIS STUDY FIND?
Study 1: Humanizing stories reduced blame but did not increase policy support
Participants who read a humanizing story about a person who uses heroin were less likely to believe that addiction is fully within a person’s control. This suggests that storytelling can reduce stigma by shifting blame away from the individual. However, these changes in belief did not lead to increased support for harm-reduction policies. Even when the story emphasized that addiction was the result of medical or environmental factors, participants’ support for services like syringe programs or supervised consumption sites stayed about the same.
Study 2: Highlighting overdose death led to greater support for harm reduction
Participants who read about a person dying from a heroin overdose were more likely to support harm-reduction policies than those who read about addiction without that outcome. This effect remained even after accounting for participants’ political orientation and other factors. While the difference was not large, it was consistent and meaningful suggesting that even a small shift in how a story ends can influence public attitudes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that not all stigma-reduction messages are equally effective when it comes to shifting public support for harm-reduction policies. While humanizing narratives made participants less likely to blame individuals for their heroin use, they did not lead to stronger support for services like supervised consumption sites or naloxone distribution. In contrast, messages that highlighted the life-or-death consequences of opioid use—particularly the risk of fatal overdose—were better at changing attitudes toward policy.
These findings highlight the potential power of emotionally charged storytelling in public education campaigns. People may be more moved by stories that evoke concern for someone’s safety than by stories that simply reduce blame. Prior studies have shown that emotional appeals, such as messaging that elicits sympathy or pity, can be more effective than factual messages at shifting public opinion and increasing support for evidence-based policies.
Importantly, the results do not mean that reducing stigma is unimportant. Shifting beliefs about addiction as a moral failing or personal choice remains a critical goal, especially in healthcare and community settings where stigma can affect treatment access and quality of care. However, when the goal is to increase public support for harm-reduction policies, messages that underscore the real and immediate risks of overdose may be more persuasive. This emphasis on overdose risk may also apply to the names we use for these harm reduction services; for example, “overdose prevention sites” garner more public support than “safe consumption sites“.
For public health advocates and policymakers, these findings suggest that message framing matters. Campaigns that aim to build support for evidence-based harm reduction strategies may benefit from incorporating stories that reflect the harsh realities of opioid use, including the possibility of death. At the same time, these messages should be crafted carefully to avoid reinforcing hopelessness or stigma—highlighting the importance of combining emotional resonance with human dignity.
Participants’ knowledge of harm reduction was not measured. All participants were given a brief description of harm-reduction services, but the researchers did not assess what participants already knew—or misunderstood—about these services. People with more familiarity or stronger pre-existing opinions may have responded differently to the narratives.
The study focused only on heroin. The stories described a person using heroin, so the findings may not apply to other substances like fentanyl, methamphetamine, or prescription opioids. Public attitudes can differ depending on the drug involved, which could change how people respond to harm-reduction messaging.
The study only looked at short-term effects. Participants were surveyed right after reading the stories, so we don’t know if the changes in beliefs or policy support would last over time, or if this translates to actual changes in behavior, such as voting for or against a harm reduction policy. Long-term follow-up is needed to understand whether narrative messaging has a lasting impact.
BOTTOM LINE
Results suggest personal stories can help reduce stigma about addiction, but they may not be enough to increase public support for harm-reduction policies. Narratives that emphasize the risk of overdose death may be more effective in changing public attitudes toward these life-saving services.
For individuals and families seeking recovery: Stories can be powerful tools, especially those that help others understand the risks of untreated substance use. Talking openly about overdose risk may help build support for helpful services in your community.
For treatment professionals and treatment systems: When advocating for harm-reduction services, messages that underscore overdose risks may be more likely to shift public opinion than those focused only on reducing stigma.
For scientists: This randomized controlled online experiment indicates that while humanizing narratives can reduce stigma, they may not significantly increase public support for harm-reduction policies. In contrast, highlighting overdose death within a narrative led to a modest but statistically significant increase in policy support. Future research should explore the long-term effects of different narrative elements—such as emotional tone, framing, and content—on both stigma reduction and policy support, including actual policy support behavior. Additionally, examining how these effects vary across different substances and audience demographics could inform more effective public health messaging strategies.
For policy makers: Public support is key to advancing harm-reduction strategies. Messaging that centers on the serious consequences of untreated opioid use may be more persuasive in building that support.
Harm reduction strategies—including supervised consumption sites, syringe service programs, and naloxone distribution—have been shown to reduce drug overdose deaths and connect people to care. Yet despite their public health benefits, these services often face political resistance and limited implementation in the US.
Harm reduction services aim to minimize negative consequences of opioid use such as overdose, illness, and legal issues. They include:
• Overdose education: Teaching individuals and communities how to recognize and respond to an overdose.
• Naloxone (“Narcan”) distribution programs: Training and equipping laypersons with naloxone, a life-saving medication that reverses opioid overdoses. •Supervised consumption sites: Also called overdose prevention centers, these facilities allow individuals to use substances under medical supervision to prevent fatal overdoses. •Syringe service programs: Provide access to sterile injecting equipment to reduce the spread of infections like HIV and hepatitis C. •Drug checking services: Distribute tools to test drugs for dangerous adulterants like fentanyl, helping individuals make safer choices. •Decriminalization of heroin possession: Reduces or eliminates criminal penalties for possessing small amounts of drugs, aiming to redirect people toward health services rather than jail. •Heroin and medications for the treatment of opioid use disorder: Offers prescribed heroin for individuals unresponsive to other treatments, or methadone to manage withdrawal and cravings. • Good Samaritan Laws: Provide legal protection to individuals who call for emergency help during a drug overdose, encouraging timely medical intervention.
This study examined whether storytelling—a common and powerful communication tool—can shift public attitudes toward harm reduction. Across two experiments, the researchers manipulated key aspects of short stories about a person who uses heroin. In Study 1, the stories varied whether addiction was portrayed as controllable or uncontrollable. In Study 2, the stories either emphasized or omitted the risk of death from overdose. The researchers assessed how these different story elements influenced beliefs about personal responsibility for addiction and support for harm reduction policies.
HOW WAS THIS STUDY CONDUCTED?
The researchers conducted 2 online randomized trials to examine whether different types of storytelling could influence public support for harm reduction policies. A total of 536 US adults participated across both studies. Participants were recruited through a national online platform and represented a range of ages, political beliefs, and personal experiences with opioid use.
In Study 1, participants were randomly assigned to 1 of 3 conditions (see graphic below). One group read a neutral message with statistics about heroin and harm reduction. The other two groups read the same statistics followed by a humanizing story about a person who became addicted to heroin. In one version of the story (low-controllability), the person’s addiction stemmed from a car accident and pain management. In the other (high-controllability), the person’s addiction began during a period of depression, with the story suggesting more personal choice. After reading the messages, participants reported their beliefs about whether heroin addiction is controllable and how much they supported various harm reduction policies.
In Study 2, the researchers tested whether focusing on the severe outcome of overdose death might be more persuasive than changing beliefs about addiction (see graphic below). Participants read either the same humanizing narrative from the low-controllability condition in Study 1 or a nearly identical version that ended with the person dying of a heroin overdose. Participants then answered the same questions about harm reduction policy support. This allowed the researchers to isolate whether highlighting overdose risk increased support more than changing beliefs about controllability.
In both studies, the researchers used detailed, multi-item surveys to measure both controllability beliefs and support for 7 specific harm reduction policies (see graphic below), including syringe service programs, supervised consumption sites, heroin distribution or medication treatment for opioid use disorder, and Good Samaritan Laws. They also controlled for participant sex, political beliefs (especially support for small government), and personal or secondhand experience with opioid use. Such statistical adjustments help to isolate the effect of interest – i.e., whether the vignette type is independently related to harm reduction support.
WHAT DID THIS STUDY FIND?
Study 1: Humanizing stories reduced blame but did not increase policy support
Participants who read a humanizing story about a person who uses heroin were less likely to believe that addiction is fully within a person’s control. This suggests that storytelling can reduce stigma by shifting blame away from the individual. However, these changes in belief did not lead to increased support for harm-reduction policies. Even when the story emphasized that addiction was the result of medical or environmental factors, participants’ support for services like syringe programs or supervised consumption sites stayed about the same.
Study 2: Highlighting overdose death led to greater support for harm reduction
Participants who read about a person dying from a heroin overdose were more likely to support harm-reduction policies than those who read about addiction without that outcome. This effect remained even after accounting for participants’ political orientation and other factors. While the difference was not large, it was consistent and meaningful suggesting that even a small shift in how a story ends can influence public attitudes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that not all stigma-reduction messages are equally effective when it comes to shifting public support for harm-reduction policies. While humanizing narratives made participants less likely to blame individuals for their heroin use, they did not lead to stronger support for services like supervised consumption sites or naloxone distribution. In contrast, messages that highlighted the life-or-death consequences of opioid use—particularly the risk of fatal overdose—were better at changing attitudes toward policy.
These findings highlight the potential power of emotionally charged storytelling in public education campaigns. People may be more moved by stories that evoke concern for someone’s safety than by stories that simply reduce blame. Prior studies have shown that emotional appeals, such as messaging that elicits sympathy or pity, can be more effective than factual messages at shifting public opinion and increasing support for evidence-based policies.
Importantly, the results do not mean that reducing stigma is unimportant. Shifting beliefs about addiction as a moral failing or personal choice remains a critical goal, especially in healthcare and community settings where stigma can affect treatment access and quality of care. However, when the goal is to increase public support for harm-reduction policies, messages that underscore the real and immediate risks of overdose may be more persuasive. This emphasis on overdose risk may also apply to the names we use for these harm reduction services; for example, “overdose prevention sites” garner more public support than “safe consumption sites“.
For public health advocates and policymakers, these findings suggest that message framing matters. Campaigns that aim to build support for evidence-based harm reduction strategies may benefit from incorporating stories that reflect the harsh realities of opioid use, including the possibility of death. At the same time, these messages should be crafted carefully to avoid reinforcing hopelessness or stigma—highlighting the importance of combining emotional resonance with human dignity.
Participants’ knowledge of harm reduction was not measured. All participants were given a brief description of harm-reduction services, but the researchers did not assess what participants already knew—or misunderstood—about these services. People with more familiarity or stronger pre-existing opinions may have responded differently to the narratives.
The study focused only on heroin. The stories described a person using heroin, so the findings may not apply to other substances like fentanyl, methamphetamine, or prescription opioids. Public attitudes can differ depending on the drug involved, which could change how people respond to harm-reduction messaging.
The study only looked at short-term effects. Participants were surveyed right after reading the stories, so we don’t know if the changes in beliefs or policy support would last over time, or if this translates to actual changes in behavior, such as voting for or against a harm reduction policy. Long-term follow-up is needed to understand whether narrative messaging has a lasting impact.
BOTTOM LINE
Results suggest personal stories can help reduce stigma about addiction, but they may not be enough to increase public support for harm-reduction policies. Narratives that emphasize the risk of overdose death may be more effective in changing public attitudes toward these life-saving services.
For individuals and families seeking recovery: Stories can be powerful tools, especially those that help others understand the risks of untreated substance use. Talking openly about overdose risk may help build support for helpful services in your community.
For treatment professionals and treatment systems: When advocating for harm-reduction services, messages that underscore overdose risks may be more likely to shift public opinion than those focused only on reducing stigma.
For scientists: This randomized controlled online experiment indicates that while humanizing narratives can reduce stigma, they may not significantly increase public support for harm-reduction policies. In contrast, highlighting overdose death within a narrative led to a modest but statistically significant increase in policy support. Future research should explore the long-term effects of different narrative elements—such as emotional tone, framing, and content—on both stigma reduction and policy support, including actual policy support behavior. Additionally, examining how these effects vary across different substances and audience demographics could inform more effective public health messaging strategies.
For policy makers: Public support is key to advancing harm-reduction strategies. Messaging that centers on the serious consequences of untreated opioid use may be more persuasive in building that support.