Proximity reduces toxicity: Closer distance to supervised consumption sites is associated with fewer overdose deaths
The distance to supervised consumption sites from a neighborhood might impact the number of overdose deaths in that area and surrounding areas. This study used sophisticated spatial analyses to examine if being located more closely to these sites was associated with fewer deaths.
Research on supervised consumption sites suggest they may be helpful in the reduction of harms and deaths associated with injection drug use, including fewer overdose deaths, less syringe sharing and injecting in public, and increased participation in treatment. Encouragingly, some studies suggest potential benefits may “spill over” into the broader community and help people who use drugs but do not access these services. This may be because sites often distribute naloxone, provide referrals to treatment, and provide education on lower risk use. For example, prior research has shown that supervised consumption sites were associated with fewer calls for ambulances in the neighborhoods surrounding these sites. However, this research is limited, making the broader public health benefits of supervised consumption sites unclear.
Between 2017 and 2019, Toronto implemented 9 supervised consumption sites across the city, which provided an opportunity to examine their effect on mortality at the population-level and potential spill-over effects. The researchers in this study examined the association between supervised consumption site distance and population-level overdose mortality in Toronto, Ontario. This research can shed light on how the distance between supervised consumption sites and neighborhoods impacts rates of overdose deaths in that area and whether the public health benefits can extend beyond people served by such places to the surrounding neighborhoods.
HOW WAS THIS STUDY CONDUCTED?
The research team compared overdose mortality rates before and after implementation of supervised consumption sites across neighborhoods in Toronto, and examined the spatial association between site distance and overdose mortality events. The study period was between May 1, 2017 and December 31, 2019, during which 9 consumption sites were set up in Toronto. Sites that were integrated with other health services (e.g., sterile syringe, naloxone distribution) under medical supervision and low-threshold sites that did not include medical services were both included.
Site distance was defined as the distance from a given neighborhood’s center to the nearest consumption site. All of Toronto’s 140 neighborhoods were included and treated as the units of analysis. The researchers were also interested in the count of registered substance-use related health services (e.g., addiction medicine clinics, community health services) and sociodemographic predictors at the neighborhood-level, which included population density, median household income, median age, labor force participation in the construction industry, unemployment, visible minority population (defined by Statistics Canada as people who are non-White and non-Indigenous), and education level. The main outcome was overdose mortality incident location in Toronto between May 2017 and Dec 2019, expressed as a crude incidence rate per 100,000 people.
In the analyses, the researchers defined the pre-implementation period as May 1 – July 31, 2017, since the first site opened in August 2017. The post-implementation period was defined as May 1 – July 31, 2019, to match the pre-implementation period and account for seasonal influences on the number of overdoses. Fatal overdose incidents were mapped for the pre- and post-periods to compare the effect of site implementation on the spatial incidence of overdoses mortality. The researchers also included a radius buffer for all 9 sites of 500 meters (0.31 miles). However, to determine whether the buffer size affected changes in the detection of mortality incidence, the researchers also analyzed buffer radii of 250, 1000, 2500, and 5000 meters (0.15, 0.62, 1.55, and 3.11 miles).
The research team obtained the data from the Office of the Chief Coroner of Ontario by extracting cases of accidental death in Toronto. Cases were included in the study if the overdose incident location was within the City of Toronto; the death was deemed accidental; and the cause of death involved use of a naturally occurring opioid (e.g., “opiate” such as morphine), synthetic (e.g., fentanyl) or semi-synthetic opioid (e.g., oxycodone), or other psychoactive substance (via injection or non-injection). Among the 787 overdose deaths that met these criteria, the majority were among males (75%), involved fentanyl or a fentanyl analogue (66%), involved more than one class of drugs contributing to death (67%), and occurred outside of the decedent’s home (65%). Participants’ average age at the time of death was 44 years old.
WHAT DID THIS STUDY FIND?
Supervised consumption site implementation associated with reduced overdose mortality
Overall, a city-wide reduction in overdose mortality rate of 42% was observed between the pre-implementation period and the post-implementation period. During the pre-implementation period, there were 64 overdose deaths (for a rate of 2 in 34 per 100,000 people), compared to 37 overdose deaths during the post-implementation period (for a rate of 1 in 35 per 100,000 people).
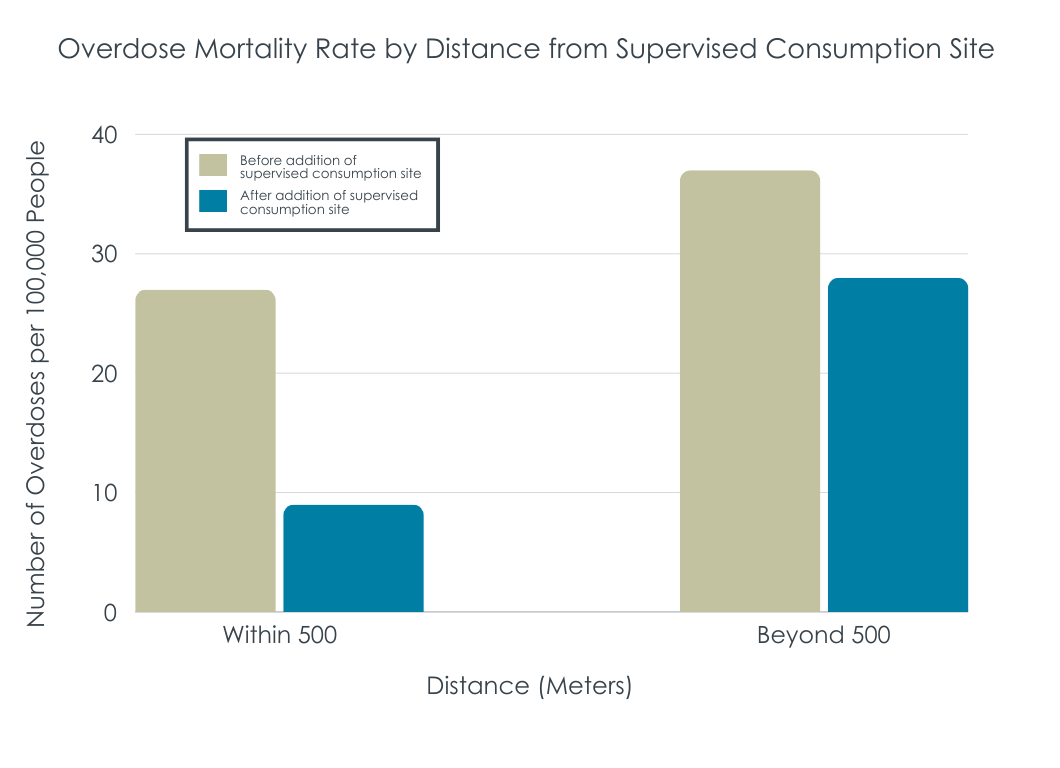
Among neighborhoods that were within 500 meters of a consumption site, the overdose mortality rate decreased by 67% between the pre- and post-implementation periods. During the pre-implementation period, there were 27 overdose deaths (for a rate of 8 in 10 per 100,000 people) in these neighborhoods, compared to 9 overdose deaths during the post-implementation period (for a rate of 2 in 70 per 100,000 people).
Overdose death reductions between the pre- and post-implementation periods persisted when changing the buffer radii. A 67% reduction was observed at 250 meters, a 69% reduction at 1000 meters, a 60% reduction at 2500 meters, and a 59% reduction at 5000 meters.
Site distance associated with greater reductions in overdose mortality
While the association between site distance and overdose mortality varied across the city and between years, the results showed a consistent inverse association between the location of the site and mortality incidents (i.e., the closer the site, the greater the reduction in deaths). The greatest reductions between 2018 and 2019 were observed in downtown neighborhoods that were closest to consumption sites. In other words, after sites were implemented, there was a stronger inverse correlationbetween distance to a supervised consumption site and reduced risk for overdose death (i.e., closer distance, reduced risk).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Study findings showed there were reductions in overdose deaths in neighborhoods with consumption sites after implementation and that the closer a neighborhood was to a site, the stronger its risk reduction. At the same time, the risk reduction in terms of absolute numbers of overdose deaths held out to 5000 meters – just over 3 miles. This supports the notion of spill over effects into the areas immediately surrounding the site, which could be due to the services provided by the site that can have widespread impact, such as naloxone distribution and education on lower risk drug use.
These findings add to the growing number of studies demonstrating that access to harm reduction services can help save lives and reduce health risks associated with drug use. Notably, while Canada has been expanding these services in recent years, the US has lagged behind, seemingly due to laws prohibiting implementation, public stigma, and “not in my back yard” (NIMBY) attitudes among the public. A few exceptions to this, however, include harm reduction dispensing machines that have been implemented in Nevada and Ohio, both of which have been associated with fewer deaths in surrounding neighborhoods. Research on strategies to improve public attitudes toward supervised consumption sites are limited, though the language used to describe these sites (e.g., overdose prevention versus safe/supervised injection) may make a difference.
Importantly, although associations were found between consumption site implementation and distance with reduced overdose deaths in this study, these results do not necessarily mean that effects were causal in nature. This is consistent with a recent study in which the existing literature on supervised consumption sites was carefully assessed for study quality, adverse consequences, and causality. The researchers in that study found that while the literature does not currently support causal evidence between consumption sites and beneficial public health outcomes, there was little evidence for adverse effects. They suggest that this has different implications for different types of policymakers, with politicians being justified in moving forward with supporting the opening of a new supervised consumption site, but with other city planners who have to decide how to use scarce resources proceeding with greater consideration for weighing the benefits in context of the financial costs.
Because this study was interested in the population-level effects of implementing supervised consumption sites on overdose risk, individual-level factors were not assessed.
The pre- and post-implementation periods that were studied were limited to 3 months, which limits the extent to which we can draw insight about the long-term effects of implementing supervised consumption sites.
Because of privacy concerns, the researchers were not able to examine whether the results differed by demographic factors such as race/ethnicity. Accordingly, it is unclear whether the results will generalize equally across different groups of individuals who use drugs.
Both supervised consumption sites that typically offer medical services and lower-threshold sites that do not offer medical services were included. Therefore, the researchers cannot distinguish whether one type of site had more of an impact on overdose deaths than the other.
BOTTOM LINE
Implementation of supervised consumption sitesis associated with public health benefits, including fewer overdose deaths. This study additionally shows that closer distances of supervised consumption sitesmay be associated with greater reductions in overdose deaths, though positive outcomes were observed out to 5000 meters (3 miles) from a single site, supporting the notion that the benefits can spill over into surrounding areas.
For individuals and families seeking recovery: Because this study showed that reduced overdose deaths were associated with implementation of supervised consumption sites, individuals who use drugs and take advantage of these services are likely to have reduced risk of overdose and associated drug use related harms. Further, because this reduced risk of death from overdose was observed at the population-level (i.e., was not limited just to people who used the services) and was greater when the site was closer to one’s neighborhood, people who support implementation of supervised consumption sites in their neighborhoods are likely to see public health benefits.
For treatment professionals and treatment systems: Treatment professionals who help promote awareness of supervised consumption sites to their clients who use drugs but do not want to stop or cannot stop, if services are available, may help to reduce their risk of overdose death. Further, treatment professionals who provide education about supervised drug use, which is a service offered by these sites, may likewise help to reduce risk of overdose risk to not only their clients, but to the broader community as well.
For scientists:Becausethe current study design limits the extent to which conclusions can be drawn about causality, future research that examines causality by using, for example, natural experiments and sophisticated modeling, would shed light on whether supervised consumption sites cause reductions in overdose deaths. Further, because differences by demographic factors like race/ethnicity could not be assessed, additional research that investigates these differences would help us understand whether effects generalize across different groups of people who use drugs. Finally, longitudinal studies that examine effects beyond 3 months will allow us to understand the longer-term effects of supervised consumption space implementation and how such service may help not only with preventing overdose deaths but also facilitating remission and recovery.
For policy makers: This study demonstrated that implementation and closer distance of supervised consumption sitesrelative to a given neighborhood was associated with fewer overdose deaths in that area. Accordingly, policymakers who support opening of supervised consumption sites are likely to see fewer overdose deaths at the population-level in the area surrounding the site. However, because it remains unclear if these effects are causal, funding for additional research to examine causality would shed light on whether implementation of supervised consumption sites caused the reduction in overdose deaths.
Research on supervised consumption sites suggest they may be helpful in the reduction of harms and deaths associated with injection drug use, including fewer overdose deaths, less syringe sharing and injecting in public, and increased participation in treatment. Encouragingly, some studies suggest potential benefits may “spill over” into the broader community and help people who use drugs but do not access these services. This may be because sites often distribute naloxone, provide referrals to treatment, and provide education on lower risk use. For example, prior research has shown that supervised consumption sites were associated with fewer calls for ambulances in the neighborhoods surrounding these sites. However, this research is limited, making the broader public health benefits of supervised consumption sites unclear.
Between 2017 and 2019, Toronto implemented 9 supervised consumption sites across the city, which provided an opportunity to examine their effect on mortality at the population-level and potential spill-over effects. The researchers in this study examined the association between supervised consumption site distance and population-level overdose mortality in Toronto, Ontario. This research can shed light on how the distance between supervised consumption sites and neighborhoods impacts rates of overdose deaths in that area and whether the public health benefits can extend beyond people served by such places to the surrounding neighborhoods.
HOW WAS THIS STUDY CONDUCTED?
The research team compared overdose mortality rates before and after implementation of supervised consumption sites across neighborhoods in Toronto, and examined the spatial association between site distance and overdose mortality events. The study period was between May 1, 2017 and December 31, 2019, during which 9 consumption sites were set up in Toronto. Sites that were integrated with other health services (e.g., sterile syringe, naloxone distribution) under medical supervision and low-threshold sites that did not include medical services were both included.
Site distance was defined as the distance from a given neighborhood’s center to the nearest consumption site. All of Toronto’s 140 neighborhoods were included and treated as the units of analysis. The researchers were also interested in the count of registered substance-use related health services (e.g., addiction medicine clinics, community health services) and sociodemographic predictors at the neighborhood-level, which included population density, median household income, median age, labor force participation in the construction industry, unemployment, visible minority population (defined by Statistics Canada as people who are non-White and non-Indigenous), and education level. The main outcome was overdose mortality incident location in Toronto between May 2017 and Dec 2019, expressed as a crude incidence rate per 100,000 people.
In the analyses, the researchers defined the pre-implementation period as May 1 – July 31, 2017, since the first site opened in August 2017. The post-implementation period was defined as May 1 – July 31, 2019, to match the pre-implementation period and account for seasonal influences on the number of overdoses. Fatal overdose incidents were mapped for the pre- and post-periods to compare the effect of site implementation on the spatial incidence of overdoses mortality. The researchers also included a radius buffer for all 9 sites of 500 meters (0.31 miles). However, to determine whether the buffer size affected changes in the detection of mortality incidence, the researchers also analyzed buffer radii of 250, 1000, 2500, and 5000 meters (0.15, 0.62, 1.55, and 3.11 miles).
The research team obtained the data from the Office of the Chief Coroner of Ontario by extracting cases of accidental death in Toronto. Cases were included in the study if the overdose incident location was within the City of Toronto; the death was deemed accidental; and the cause of death involved use of a naturally occurring opioid (e.g., “opiate” such as morphine), synthetic (e.g., fentanyl) or semi-synthetic opioid (e.g., oxycodone), or other psychoactive substance (via injection or non-injection). Among the 787 overdose deaths that met these criteria, the majority were among males (75%), involved fentanyl or a fentanyl analogue (66%), involved more than one class of drugs contributing to death (67%), and occurred outside of the decedent’s home (65%). Participants’ average age at the time of death was 44 years old.
WHAT DID THIS STUDY FIND?
Supervised consumption site implementation associated with reduced overdose mortality
Overall, a city-wide reduction in overdose mortality rate of 42% was observed between the pre-implementation period and the post-implementation period. During the pre-implementation period, there were 64 overdose deaths (for a rate of 2 in 34 per 100,000 people), compared to 37 overdose deaths during the post-implementation period (for a rate of 1 in 35 per 100,000 people).
Among neighborhoods that were within 500 meters of a consumption site, the overdose mortality rate decreased by 67% between the pre- and post-implementation periods. During the pre-implementation period, there were 27 overdose deaths (for a rate of 8 in 10 per 100,000 people) in these neighborhoods, compared to 9 overdose deaths during the post-implementation period (for a rate of 2 in 70 per 100,000 people).
Overdose death reductions between the pre- and post-implementation periods persisted when changing the buffer radii. A 67% reduction was observed at 250 meters, a 69% reduction at 1000 meters, a 60% reduction at 2500 meters, and a 59% reduction at 5000 meters.
Site distance associated with greater reductions in overdose mortality
While the association between site distance and overdose mortality varied across the city and between years, the results showed a consistent inverse association between the location of the site and mortality incidents (i.e., the closer the site, the greater the reduction in deaths). The greatest reductions between 2018 and 2019 were observed in downtown neighborhoods that were closest to consumption sites. In other words, after sites were implemented, there was a stronger inverse correlationbetween distance to a supervised consumption site and reduced risk for overdose death (i.e., closer distance, reduced risk).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Study findings showed there were reductions in overdose deaths in neighborhoods with consumption sites after implementation and that the closer a neighborhood was to a site, the stronger its risk reduction. At the same time, the risk reduction in terms of absolute numbers of overdose deaths held out to 5000 meters – just over 3 miles. This supports the notion of spill over effects into the areas immediately surrounding the site, which could be due to the services provided by the site that can have widespread impact, such as naloxone distribution and education on lower risk drug use.
These findings add to the growing number of studies demonstrating that access to harm reduction services can help save lives and reduce health risks associated with drug use. Notably, while Canada has been expanding these services in recent years, the US has lagged behind, seemingly due to laws prohibiting implementation, public stigma, and “not in my back yard” (NIMBY) attitudes among the public. A few exceptions to this, however, include harm reduction dispensing machines that have been implemented in Nevada and Ohio, both of which have been associated with fewer deaths in surrounding neighborhoods. Research on strategies to improve public attitudes toward supervised consumption sites are limited, though the language used to describe these sites (e.g., overdose prevention versus safe/supervised injection) may make a difference.
Importantly, although associations were found between consumption site implementation and distance with reduced overdose deaths in this study, these results do not necessarily mean that effects were causal in nature. This is consistent with a recent study in which the existing literature on supervised consumption sites was carefully assessed for study quality, adverse consequences, and causality. The researchers in that study found that while the literature does not currently support causal evidence between consumption sites and beneficial public health outcomes, there was little evidence for adverse effects. They suggest that this has different implications for different types of policymakers, with politicians being justified in moving forward with supporting the opening of a new supervised consumption site, but with other city planners who have to decide how to use scarce resources proceeding with greater consideration for weighing the benefits in context of the financial costs.
Because this study was interested in the population-level effects of implementing supervised consumption sites on overdose risk, individual-level factors were not assessed.
The pre- and post-implementation periods that were studied were limited to 3 months, which limits the extent to which we can draw insight about the long-term effects of implementing supervised consumption sites.
Because of privacy concerns, the researchers were not able to examine whether the results differed by demographic factors such as race/ethnicity. Accordingly, it is unclear whether the results will generalize equally across different groups of individuals who use drugs.
Both supervised consumption sites that typically offer medical services and lower-threshold sites that do not offer medical services were included. Therefore, the researchers cannot distinguish whether one type of site had more of an impact on overdose deaths than the other.
BOTTOM LINE
Implementation of supervised consumption sitesis associated with public health benefits, including fewer overdose deaths. This study additionally shows that closer distances of supervised consumption sitesmay be associated with greater reductions in overdose deaths, though positive outcomes were observed out to 5000 meters (3 miles) from a single site, supporting the notion that the benefits can spill over into surrounding areas.
For individuals and families seeking recovery: Because this study showed that reduced overdose deaths were associated with implementation of supervised consumption sites, individuals who use drugs and take advantage of these services are likely to have reduced risk of overdose and associated drug use related harms. Further, because this reduced risk of death from overdose was observed at the population-level (i.e., was not limited just to people who used the services) and was greater when the site was closer to one’s neighborhood, people who support implementation of supervised consumption sites in their neighborhoods are likely to see public health benefits.
For treatment professionals and treatment systems: Treatment professionals who help promote awareness of supervised consumption sites to their clients who use drugs but do not want to stop or cannot stop, if services are available, may help to reduce their risk of overdose death. Further, treatment professionals who provide education about supervised drug use, which is a service offered by these sites, may likewise help to reduce risk of overdose risk to not only their clients, but to the broader community as well.
For scientists:Becausethe current study design limits the extent to which conclusions can be drawn about causality, future research that examines causality by using, for example, natural experiments and sophisticated modeling, would shed light on whether supervised consumption sites cause reductions in overdose deaths. Further, because differences by demographic factors like race/ethnicity could not be assessed, additional research that investigates these differences would help us understand whether effects generalize across different groups of people who use drugs. Finally, longitudinal studies that examine effects beyond 3 months will allow us to understand the longer-term effects of supervised consumption space implementation and how such service may help not only with preventing overdose deaths but also facilitating remission and recovery.
For policy makers: This study demonstrated that implementation and closer distance of supervised consumption sitesrelative to a given neighborhood was associated with fewer overdose deaths in that area. Accordingly, policymakers who support opening of supervised consumption sites are likely to see fewer overdose deaths at the population-level in the area surrounding the site. However, because it remains unclear if these effects are causal, funding for additional research to examine causality would shed light on whether implementation of supervised consumption sites caused the reduction in overdose deaths.
Research on supervised consumption sites suggest they may be helpful in the reduction of harms and deaths associated with injection drug use, including fewer overdose deaths, less syringe sharing and injecting in public, and increased participation in treatment. Encouragingly, some studies suggest potential benefits may “spill over” into the broader community and help people who use drugs but do not access these services. This may be because sites often distribute naloxone, provide referrals to treatment, and provide education on lower risk use. For example, prior research has shown that supervised consumption sites were associated with fewer calls for ambulances in the neighborhoods surrounding these sites. However, this research is limited, making the broader public health benefits of supervised consumption sites unclear.
Between 2017 and 2019, Toronto implemented 9 supervised consumption sites across the city, which provided an opportunity to examine their effect on mortality at the population-level and potential spill-over effects. The researchers in this study examined the association between supervised consumption site distance and population-level overdose mortality in Toronto, Ontario. This research can shed light on how the distance between supervised consumption sites and neighborhoods impacts rates of overdose deaths in that area and whether the public health benefits can extend beyond people served by such places to the surrounding neighborhoods.
HOW WAS THIS STUDY CONDUCTED?
The research team compared overdose mortality rates before and after implementation of supervised consumption sites across neighborhoods in Toronto, and examined the spatial association between site distance and overdose mortality events. The study period was between May 1, 2017 and December 31, 2019, during which 9 consumption sites were set up in Toronto. Sites that were integrated with other health services (e.g., sterile syringe, naloxone distribution) under medical supervision and low-threshold sites that did not include medical services were both included.
Site distance was defined as the distance from a given neighborhood’s center to the nearest consumption site. All of Toronto’s 140 neighborhoods were included and treated as the units of analysis. The researchers were also interested in the count of registered substance-use related health services (e.g., addiction medicine clinics, community health services) and sociodemographic predictors at the neighborhood-level, which included population density, median household income, median age, labor force participation in the construction industry, unemployment, visible minority population (defined by Statistics Canada as people who are non-White and non-Indigenous), and education level. The main outcome was overdose mortality incident location in Toronto between May 2017 and Dec 2019, expressed as a crude incidence rate per 100,000 people.
In the analyses, the researchers defined the pre-implementation period as May 1 – July 31, 2017, since the first site opened in August 2017. The post-implementation period was defined as May 1 – July 31, 2019, to match the pre-implementation period and account for seasonal influences on the number of overdoses. Fatal overdose incidents were mapped for the pre- and post-periods to compare the effect of site implementation on the spatial incidence of overdoses mortality. The researchers also included a radius buffer for all 9 sites of 500 meters (0.31 miles). However, to determine whether the buffer size affected changes in the detection of mortality incidence, the researchers also analyzed buffer radii of 250, 1000, 2500, and 5000 meters (0.15, 0.62, 1.55, and 3.11 miles).
The research team obtained the data from the Office of the Chief Coroner of Ontario by extracting cases of accidental death in Toronto. Cases were included in the study if the overdose incident location was within the City of Toronto; the death was deemed accidental; and the cause of death involved use of a naturally occurring opioid (e.g., “opiate” such as morphine), synthetic (e.g., fentanyl) or semi-synthetic opioid (e.g., oxycodone), or other psychoactive substance (via injection or non-injection). Among the 787 overdose deaths that met these criteria, the majority were among males (75%), involved fentanyl or a fentanyl analogue (66%), involved more than one class of drugs contributing to death (67%), and occurred outside of the decedent’s home (65%). Participants’ average age at the time of death was 44 years old.
WHAT DID THIS STUDY FIND?
Supervised consumption site implementation associated with reduced overdose mortality
Overall, a city-wide reduction in overdose mortality rate of 42% was observed between the pre-implementation period and the post-implementation period. During the pre-implementation period, there were 64 overdose deaths (for a rate of 2 in 34 per 100,000 people), compared to 37 overdose deaths during the post-implementation period (for a rate of 1 in 35 per 100,000 people).
Among neighborhoods that were within 500 meters of a consumption site, the overdose mortality rate decreased by 67% between the pre- and post-implementation periods. During the pre-implementation period, there were 27 overdose deaths (for a rate of 8 in 10 per 100,000 people) in these neighborhoods, compared to 9 overdose deaths during the post-implementation period (for a rate of 2 in 70 per 100,000 people).
Overdose death reductions between the pre- and post-implementation periods persisted when changing the buffer radii. A 67% reduction was observed at 250 meters, a 69% reduction at 1000 meters, a 60% reduction at 2500 meters, and a 59% reduction at 5000 meters.
Site distance associated with greater reductions in overdose mortality
While the association between site distance and overdose mortality varied across the city and between years, the results showed a consistent inverse association between the location of the site and mortality incidents (i.e., the closer the site, the greater the reduction in deaths). The greatest reductions between 2018 and 2019 were observed in downtown neighborhoods that were closest to consumption sites. In other words, after sites were implemented, there was a stronger inverse correlationbetween distance to a supervised consumption site and reduced risk for overdose death (i.e., closer distance, reduced risk).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Study findings showed there were reductions in overdose deaths in neighborhoods with consumption sites after implementation and that the closer a neighborhood was to a site, the stronger its risk reduction. At the same time, the risk reduction in terms of absolute numbers of overdose deaths held out to 5000 meters – just over 3 miles. This supports the notion of spill over effects into the areas immediately surrounding the site, which could be due to the services provided by the site that can have widespread impact, such as naloxone distribution and education on lower risk drug use.
These findings add to the growing number of studies demonstrating that access to harm reduction services can help save lives and reduce health risks associated with drug use. Notably, while Canada has been expanding these services in recent years, the US has lagged behind, seemingly due to laws prohibiting implementation, public stigma, and “not in my back yard” (NIMBY) attitudes among the public. A few exceptions to this, however, include harm reduction dispensing machines that have been implemented in Nevada and Ohio, both of which have been associated with fewer deaths in surrounding neighborhoods. Research on strategies to improve public attitudes toward supervised consumption sites are limited, though the language used to describe these sites (e.g., overdose prevention versus safe/supervised injection) may make a difference.
Importantly, although associations were found between consumption site implementation and distance with reduced overdose deaths in this study, these results do not necessarily mean that effects were causal in nature. This is consistent with a recent study in which the existing literature on supervised consumption sites was carefully assessed for study quality, adverse consequences, and causality. The researchers in that study found that while the literature does not currently support causal evidence between consumption sites and beneficial public health outcomes, there was little evidence for adverse effects. They suggest that this has different implications for different types of policymakers, with politicians being justified in moving forward with supporting the opening of a new supervised consumption site, but with other city planners who have to decide how to use scarce resources proceeding with greater consideration for weighing the benefits in context of the financial costs.
Because this study was interested in the population-level effects of implementing supervised consumption sites on overdose risk, individual-level factors were not assessed.
The pre- and post-implementation periods that were studied were limited to 3 months, which limits the extent to which we can draw insight about the long-term effects of implementing supervised consumption sites.
Because of privacy concerns, the researchers were not able to examine whether the results differed by demographic factors such as race/ethnicity. Accordingly, it is unclear whether the results will generalize equally across different groups of individuals who use drugs.
Both supervised consumption sites that typically offer medical services and lower-threshold sites that do not offer medical services were included. Therefore, the researchers cannot distinguish whether one type of site had more of an impact on overdose deaths than the other.
BOTTOM LINE
Implementation of supervised consumption sitesis associated with public health benefits, including fewer overdose deaths. This study additionally shows that closer distances of supervised consumption sitesmay be associated with greater reductions in overdose deaths, though positive outcomes were observed out to 5000 meters (3 miles) from a single site, supporting the notion that the benefits can spill over into surrounding areas.
For individuals and families seeking recovery: Because this study showed that reduced overdose deaths were associated with implementation of supervised consumption sites, individuals who use drugs and take advantage of these services are likely to have reduced risk of overdose and associated drug use related harms. Further, because this reduced risk of death from overdose was observed at the population-level (i.e., was not limited just to people who used the services) and was greater when the site was closer to one’s neighborhood, people who support implementation of supervised consumption sites in their neighborhoods are likely to see public health benefits.
For treatment professionals and treatment systems: Treatment professionals who help promote awareness of supervised consumption sites to their clients who use drugs but do not want to stop or cannot stop, if services are available, may help to reduce their risk of overdose death. Further, treatment professionals who provide education about supervised drug use, which is a service offered by these sites, may likewise help to reduce risk of overdose risk to not only their clients, but to the broader community as well.
For scientists:Becausethe current study design limits the extent to which conclusions can be drawn about causality, future research that examines causality by using, for example, natural experiments and sophisticated modeling, would shed light on whether supervised consumption sites cause reductions in overdose deaths. Further, because differences by demographic factors like race/ethnicity could not be assessed, additional research that investigates these differences would help us understand whether effects generalize across different groups of people who use drugs. Finally, longitudinal studies that examine effects beyond 3 months will allow us to understand the longer-term effects of supervised consumption space implementation and how such service may help not only with preventing overdose deaths but also facilitating remission and recovery.
For policy makers: This study demonstrated that implementation and closer distance of supervised consumption sitesrelative to a given neighborhood was associated with fewer overdose deaths in that area. Accordingly, policymakers who support opening of supervised consumption sites are likely to see fewer overdose deaths at the population-level in the area surrounding the site. However, because it remains unclear if these effects are causal, funding for additional research to examine causality would shed light on whether implementation of supervised consumption sites caused the reduction in overdose deaths.