An innovative strategy to access harm reduction resources
Increasing access to empirically supported harm reduction resources, including naloxone, safer injection kits, and fentanyl test strips, could help prevent overdose deaths and other drug use related harms. This study evaluated the impact of an automated harm reduction resource machine on the accessibility of harm reduction supplies and the local incidence of fatal overdoses and HIV during its first year in operation.
In particular, the Centers for Disease Control and Prevention have recommended that 10 of these harm reduction strategies be implemented, including distribution of naloxone (i.e., a drug that can reverse an opioid overdose) to those who are most likely to encounter an overdose and syringe services programs that provide access to sterile equipment and other harm reduction supplies and services. However, access to these services in the U.S. has been limited, in large part due to stigma. Because of the stigma and stereotypes against people who use drugs as undeserving of this type of care and untrustworthy, efforts to implement treatment and harm reduction services in neighborhoods have been protested against by the locals, consistent with “not in my back yard” (NIMBY) attitudes. Further, people who use drugs may be reluctant to access such services if offered because of how poorly they have been treated by healthcare professionals previously. Syringe dispensing machines may offer one way to help overcome this limitation.
Research has shown that syringe dispensing machines reduce needle sharing, increase access to sterile equipment, and are used by people who were less likely to attend in-person services. While several European countries and Australia have begun implementing syringe dispensing machines, the U.S. has been slow to do so. In 2017, Nevada became the first U.S. state to implement a syringe dispensing machine, with eventual inclusion of other harm reduction supplies, such as naloxone, and information about health services. Research that has examined the impact of these machines in the U.S., however, is limited, given the low rates of implementation, but early data is promising.
More recently, another machine was installed in Hamilton County in Cincinnati, Ohio, outside of an organization that provided in-person syringe services once a week (i.e., distribution of naloxone). County leaders did not allow syringes to be offered by the machine, but other harm reduction products were approved (e.g., naloxone, sterile equipment, fentanyl test strips, etc.). In this study, the research team evaluated the impact of this harm reduction dispensing machine on the accessibility of harm reduction supplies and the local incidence of fatal overdoses and HIV during its first year. Such research can help inform strategies for how to improve access to harm reduction products that have been shown to prevent overdose deaths and the spread of diseases transmitted through needle sharing.
HOW WAS THIS STUDY CONDUCTED?
The research team evaluated the impact of the harm reduction dispensing machine during its first year using an observational study design, in which the researchers tracked the number of supplies distributed by the machine and rates of fatal overdoses and HIV without intervening to try and change the outcomes.
To access the dispensing machine, clients anonymously registered over the phone with a coordinator, who gave them a unique access code and referred them as needed to other services, such as prenatal care and HIV testing. The access code allowed them to access the machine anytime (24 hours a day/7 days a week) and was valid for 90 days. After 90 days, they had to re-enroll and get another code, which provided another opportunity for the coordinators to connect them to additional services, if needed. During registration, clients were given the option to provide their name and contact information to allow the coordinators to follow up with them, as well as an option to participate in a survey that collected demographic information and other related information, such as previous use of harm reduction services. Providing contact information and participating in the survey were not required to be able to use the machine.
The machine contained 2 doses of intramuscular naloxone, 2 doses of naloxone nasal spray, a sharps container, a safer injection kit, a safer smoking kit, a Personal Protective Equipment kit, a safer sex kit, a pregnancy test, and a box of bandages. Clients could choose 1 of these items every 7 days throughout the 90 days that their code was valid.
The main outcome of interest was how many harm reduction supplies distributed by the machine alone in its first year (i.e., March 1, 2021 – March 1, 2022) compared to the amount of supplies distributed by the same organization within its brick-and-mortar service in the previous year. Additional outcomes the researchers were interested in included: (1) the number of naloxone doses and fentanyl test strips distributed by other syringe service programs in the county during the same time period, and (2) the incidence of fatal overdoses and HIV within the county compared to previous years.
Because this was an observational study, the researchers did not recruit people into the study or randomize them. Instead, they collected (optional) demographic information from the people who registered for a code to use the machine. During the machine’s first year, 637 people registered. The majority of people who registered were between 35 and 44 years old (41.1%) and White (90.9%). Approximately half identified as women and half identified as men. Twelve percent reported never having used harm reduction services previously. The 2 most requested products from the machine were smoking and injection kits, both which contained naloxone, making naloxone the most commonly distributed product.
Of the 637 people who initially registered, 105 registered for another code after 90 days. However, re-enrollment surveys were completed by a total of 124 people. This reflects 19 people who opted out of having their data collected and stored initially, but still used the machine and then decided to have their data collected and stored upon re-enrollment. Of note, there was an error that resulted in a delay in shutting off client access codes after 90 days that was not fixed until 2022, meaning that some people did not have to register for another code since they still had access. As such, the number of people who re-enrolled is lower than what it would have been if the system was working properly.
The demographics of the 105 people with both an initial and re-enrollment survey mirrored those of the full sample, with the majority being between 35 and 44 years old (51.4%) and White (96.2%). However, more women (62.9%) re-enrolled than men (36.2%)
WHAT DID THIS STUDY FIND?
The dispensing machine was associated with greater distribution of harm reduction supplies.
Of the 124 people who completed a re-enrollment survey: 86% reported receiving naloxone from the machine, with 71% reporting using it to reverse an overdose; 79% reported receiving fentanyl test strips from the machine, with 67% reporting that they detected fentanyl in their drug supply; 39% reported receiving a pregnancy test from the machine, which detected 13 pregnancies; and 12% reported receiving an HIV test from the machine, with no positive test results.
The machine alone distributed more sterile pipes, naloxone, fentanyl test strips, and pregnancy tests within its first year than the organization had within the previous year. Safer sex kits were the only item that the organization distributed more of than the machine.
Within the year, the dispensing machine was responsible for 100% of the sterile pipes, 69% of the naloxone doses, 72% of the fentanyl test strips, 100% of the pregnancy tests, and 27% of the safer sex kits distributed by the organization.
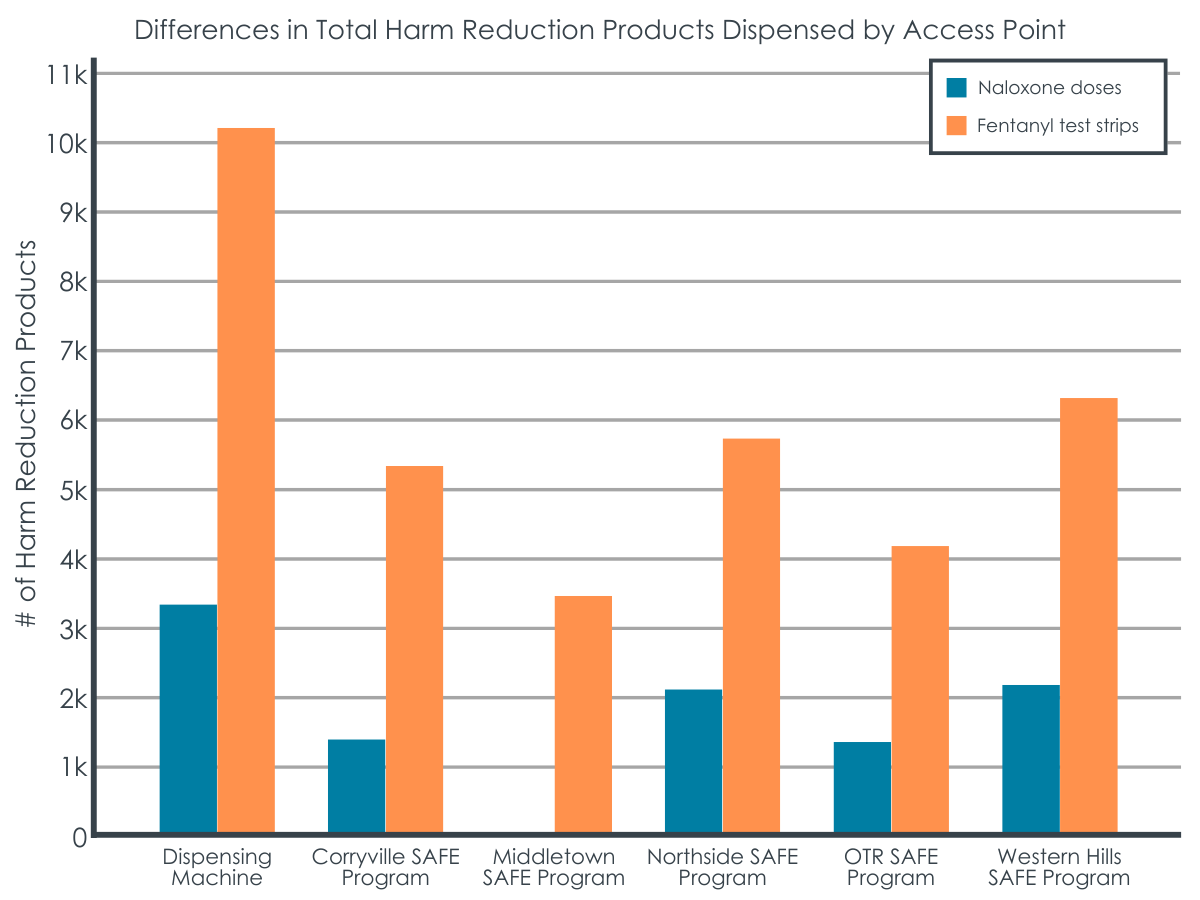
When compared to other syringe service programs in the county, the dispensing machine distributed over 1200 more doses of naloxone and 3800 more fentanyl test strips than the next largest program.
The dispensing machine was associated with decreases in fatal overdoses and HIV cases.
Contrary to rising opioid overdose incidence in Ohio and the United States overall, especially during COVID-19, Hamilton County (where the vending machine was located) reported a 10% decrease in unintentional overdose deaths, dropping from 499 in 2020 to 454 in 2021.
For HIV cases in counties neighboring Hamilton County, there was a decrease in the beginning of the pandemic, but cases then rose to pre-pandemic levels in 2021. Hamilton County avoided this trend and continued to observe decreases in 2021.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study evaluated the impact of installing an automated harm reduction dispensing machine on the accessibility of harm reduction supplies and the local incidence of fatal opioid overdoses and HIV during its first year. Results showed that implementation was associated with greater accessibility of harm reduction products and services and alower incidence of unintentional overdose death and HIV. It is noteworthy that the county observed approximately a 10% decrease in overdose rates while nationwide rates were greatly increasing. Although the research design prevents the researchers from being able to conclude that the machine caused greater access and fewer deaths and HIV cases, these promising results help justify future research that may be able to demonstrate a causal association.
These results cannot be disentangled from the effects of other harm reduction initiatives occurring in the same county or the broader social and political climate that supports such initiatives. It is likely that the observed results are attributable to a combination of initiatives that are made possible through the support of local government. While these findings are consistent with the early results from Las Vegas that similarly showed an association between installation of a dispensing machine and fewer opioid overdose deaths, both were likely implemented along with a variety of other harm reduction and recovery support services. Thus, when provided together, these services may potentially play a complementary role in helping to address the opioid crisis.
However, what is important and unique about the dispensing machine is that it can be accessed 24 hours a day, 7 days a week, and can bedone so with complete anonymity. As such, it can help expand access to harm reduction products when other services are not available and reach people who prefer to remain anonymous and avoid potential stigma. Indeed, 12% of people who used the machine reported that they had never used harm reduction products or services previously. Accordingly, the machines can help to fill a critical gap in existing harm reduction services and highlight the importance of accessibility and anonymity.
In general, the results of this study add to the research demonstrating the public health benefits of expanding access to harm reduction products and services. A key barrier to doing so, however, are drug laws that are not supported by scientific evidence and instead take a punitive approach. Drug laws are also variable across states, which further contributes to the difficulty involved in expansion. Consistent, evidence-based policies that take a public health approach could address these barriers, leading to increased access and lives saved.
The research design prevents the researchers from being able to conclude that the dispensing machinescaused greater access and fewer deaths and HIV cases. While associations were demonstrated between access to the harm reduction vending machine and improved public health outcomes in the county where the machine was located, the results may be in part also due to other harm reduction initiatives being implemented in the same county.
Results may not generalize to other cities where there is less social and political support for harm reduction initiatives, if implementation of a dispensing machine is even possible in such locations.
Because the study only evaluated the impact of the machine during its first year, its impact beyond one year is unknown. It may be that there is a novelty effect that increased the benefits observed and this will fade in the following years. On the other hand, it is also possible that awareness of the machine will increase over time, leading to stronger benefits as more people use the machine.
There was an error that resulted in a delay in shutting off client access codes after 90 days that was not fixed until 2022. Accordingly, these individuals did not have to re-register for a code to continue using the machine and were not counted among those who re-enrolled. This limits longer term data for those who continually used the machine, which may have led to an underestimate of the machine’s full impact on overdose reversals.
BOTTOM LINE
Implementing a harm reduction dispensing machine appears to be associated with greater accessibility of harm reduction products and services and a lower local incidence of unintentional overdose deaths from opioids and HIV cases. While the researchers cannot conclude that the machine caused these effects, the results are promising and help to justify future research that may be able to demonstrate a causal association. This research helps toinform strategies for how to improve access to evidence-based harm reduction products, which can save lives and prevent disease.
For individuals and families seeking recovery: Harm reduction dispensing machines are not yet widely available, but the results of this study are consistent with other studies showing harm reduction productscan save lives and prevent disease. Accordingly, individuals who use opioids, and their families, could take advantage of access to such products, when possiblegiven state laws, and have products on hand. This would allow them to access them when needed and could lead to similar benefits. Individuals and their families can find information about how to access naloxone in their state on websites such as SAFEProject and the National Harm Reduction Coalition.
For treatment professionals and treatment systems: Although harm reduction dispensing machines are not yet widely available, the results of this study are consistent with other studies demonstrating the benefits of access to harm reduction products. Accordingly, treatment professionals and systems that support and encourage the use of harm reduction products and services are likely to see similar public health benefits. For instance, clinicians may encourage their clients who use opioids and other drugs to have harm reduction products on hand (when possible, given state laws), such as naloxone and fentanyl testing strips.
For scientists:Given that the implementation of dispensing machines has been limited, evaluation of their impact is also limited. Additional research that evaluates the impact of implementing dispensing machines in different contexts would lead to an increased understanding of who they benefit, under what circumstances, and how. Also, future research that uses a more rigorous study design than an observational onecould go beyond the associations demonstrated in the current study and support a stronger link between the machine and benefits observed. Finally, future research that evaluates the impact of the machine for longer than 1 year would shed light on its impact over time.
For policy makers: Results from this study are consistent with other studies that have demonstrated the public health benefits that implementing a harm reduction dispensing machine can have on increasing access to harm reduction products, reducing opioid overdose rates, and decreasing new cases of HIV.Implementation of dispensing machines and rigorous evaluation of their impact has been limited, however. Funding for implementation and rigorous evaluation of increased access to harm reduction services would help shed light on their impact. At a broader level, support of consistent, evidence-based policies that promote harm reduction services could also help to expand services in general, leading to lives saved and the spread of diseases prevented.
In particular, the Centers for Disease Control and Prevention have recommended that 10 of these harm reduction strategies be implemented, including distribution of naloxone (i.e., a drug that can reverse an opioid overdose) to those who are most likely to encounter an overdose and syringe services programs that provide access to sterile equipment and other harm reduction supplies and services. However, access to these services in the U.S. has been limited, in large part due to stigma. Because of the stigma and stereotypes against people who use drugs as undeserving of this type of care and untrustworthy, efforts to implement treatment and harm reduction services in neighborhoods have been protested against by the locals, consistent with “not in my back yard” (NIMBY) attitudes. Further, people who use drugs may be reluctant to access such services if offered because of how poorly they have been treated by healthcare professionals previously. Syringe dispensing machines may offer one way to help overcome this limitation.
Research has shown that syringe dispensing machines reduce needle sharing, increase access to sterile equipment, and are used by people who were less likely to attend in-person services. While several European countries and Australia have begun implementing syringe dispensing machines, the U.S. has been slow to do so. In 2017, Nevada became the first U.S. state to implement a syringe dispensing machine, with eventual inclusion of other harm reduction supplies, such as naloxone, and information about health services. Research that has examined the impact of these machines in the U.S., however, is limited, given the low rates of implementation, but early data is promising.
More recently, another machine was installed in Hamilton County in Cincinnati, Ohio, outside of an organization that provided in-person syringe services once a week (i.e., distribution of naloxone). County leaders did not allow syringes to be offered by the machine, but other harm reduction products were approved (e.g., naloxone, sterile equipment, fentanyl test strips, etc.). In this study, the research team evaluated the impact of this harm reduction dispensing machine on the accessibility of harm reduction supplies and the local incidence of fatal overdoses and HIV during its first year. Such research can help inform strategies for how to improve access to harm reduction products that have been shown to prevent overdose deaths and the spread of diseases transmitted through needle sharing.
HOW WAS THIS STUDY CONDUCTED?
The research team evaluated the impact of the harm reduction dispensing machine during its first year using an observational study design, in which the researchers tracked the number of supplies distributed by the machine and rates of fatal overdoses and HIV without intervening to try and change the outcomes.
To access the dispensing machine, clients anonymously registered over the phone with a coordinator, who gave them a unique access code and referred them as needed to other services, such as prenatal care and HIV testing. The access code allowed them to access the machine anytime (24 hours a day/7 days a week) and was valid for 90 days. After 90 days, they had to re-enroll and get another code, which provided another opportunity for the coordinators to connect them to additional services, if needed. During registration, clients were given the option to provide their name and contact information to allow the coordinators to follow up with them, as well as an option to participate in a survey that collected demographic information and other related information, such as previous use of harm reduction services. Providing contact information and participating in the survey were not required to be able to use the machine.
The machine contained 2 doses of intramuscular naloxone, 2 doses of naloxone nasal spray, a sharps container, a safer injection kit, a safer smoking kit, a Personal Protective Equipment kit, a safer sex kit, a pregnancy test, and a box of bandages. Clients could choose 1 of these items every 7 days throughout the 90 days that their code was valid.
The main outcome of interest was how many harm reduction supplies distributed by the machine alone in its first year (i.e., March 1, 2021 – March 1, 2022) compared to the amount of supplies distributed by the same organization within its brick-and-mortar service in the previous year. Additional outcomes the researchers were interested in included: (1) the number of naloxone doses and fentanyl test strips distributed by other syringe service programs in the county during the same time period, and (2) the incidence of fatal overdoses and HIV within the county compared to previous years.
Because this was an observational study, the researchers did not recruit people into the study or randomize them. Instead, they collected (optional) demographic information from the people who registered for a code to use the machine. During the machine’s first year, 637 people registered. The majority of people who registered were between 35 and 44 years old (41.1%) and White (90.9%). Approximately half identified as women and half identified as men. Twelve percent reported never having used harm reduction services previously. The 2 most requested products from the machine were smoking and injection kits, both which contained naloxone, making naloxone the most commonly distributed product.
Of the 637 people who initially registered, 105 registered for another code after 90 days. However, re-enrollment surveys were completed by a total of 124 people. This reflects 19 people who opted out of having their data collected and stored initially, but still used the machine and then decided to have their data collected and stored upon re-enrollment. Of note, there was an error that resulted in a delay in shutting off client access codes after 90 days that was not fixed until 2022, meaning that some people did not have to register for another code since they still had access. As such, the number of people who re-enrolled is lower than what it would have been if the system was working properly.
The demographics of the 105 people with both an initial and re-enrollment survey mirrored those of the full sample, with the majority being between 35 and 44 years old (51.4%) and White (96.2%). However, more women (62.9%) re-enrolled than men (36.2%)
WHAT DID THIS STUDY FIND?
The dispensing machine was associated with greater distribution of harm reduction supplies.
Of the 124 people who completed a re-enrollment survey: 86% reported receiving naloxone from the machine, with 71% reporting using it to reverse an overdose; 79% reported receiving fentanyl test strips from the machine, with 67% reporting that they detected fentanyl in their drug supply; 39% reported receiving a pregnancy test from the machine, which detected 13 pregnancies; and 12% reported receiving an HIV test from the machine, with no positive test results.
The machine alone distributed more sterile pipes, naloxone, fentanyl test strips, and pregnancy tests within its first year than the organization had within the previous year. Safer sex kits were the only item that the organization distributed more of than the machine.
Within the year, the dispensing machine was responsible for 100% of the sterile pipes, 69% of the naloxone doses, 72% of the fentanyl test strips, 100% of the pregnancy tests, and 27% of the safer sex kits distributed by the organization.
When compared to other syringe service programs in the county, the dispensing machine distributed over 1200 more doses of naloxone and 3800 more fentanyl test strips than the next largest program.
The dispensing machine was associated with decreases in fatal overdoses and HIV cases.
Contrary to rising opioid overdose incidence in Ohio and the United States overall, especially during COVID-19, Hamilton County (where the vending machine was located) reported a 10% decrease in unintentional overdose deaths, dropping from 499 in 2020 to 454 in 2021.
For HIV cases in counties neighboring Hamilton County, there was a decrease in the beginning of the pandemic, but cases then rose to pre-pandemic levels in 2021. Hamilton County avoided this trend and continued to observe decreases in 2021.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study evaluated the impact of installing an automated harm reduction dispensing machine on the accessibility of harm reduction supplies and the local incidence of fatal opioid overdoses and HIV during its first year. Results showed that implementation was associated with greater accessibility of harm reduction products and services and alower incidence of unintentional overdose death and HIV. It is noteworthy that the county observed approximately a 10% decrease in overdose rates while nationwide rates were greatly increasing. Although the research design prevents the researchers from being able to conclude that the machine caused greater access and fewer deaths and HIV cases, these promising results help justify future research that may be able to demonstrate a causal association.
These results cannot be disentangled from the effects of other harm reduction initiatives occurring in the same county or the broader social and political climate that supports such initiatives. It is likely that the observed results are attributable to a combination of initiatives that are made possible through the support of local government. While these findings are consistent with the early results from Las Vegas that similarly showed an association between installation of a dispensing machine and fewer opioid overdose deaths, both were likely implemented along with a variety of other harm reduction and recovery support services. Thus, when provided together, these services may potentially play a complementary role in helping to address the opioid crisis.
However, what is important and unique about the dispensing machine is that it can be accessed 24 hours a day, 7 days a week, and can bedone so with complete anonymity. As such, it can help expand access to harm reduction products when other services are not available and reach people who prefer to remain anonymous and avoid potential stigma. Indeed, 12% of people who used the machine reported that they had never used harm reduction products or services previously. Accordingly, the machines can help to fill a critical gap in existing harm reduction services and highlight the importance of accessibility and anonymity.
In general, the results of this study add to the research demonstrating the public health benefits of expanding access to harm reduction products and services. A key barrier to doing so, however, are drug laws that are not supported by scientific evidence and instead take a punitive approach. Drug laws are also variable across states, which further contributes to the difficulty involved in expansion. Consistent, evidence-based policies that take a public health approach could address these barriers, leading to increased access and lives saved.
The research design prevents the researchers from being able to conclude that the dispensing machinescaused greater access and fewer deaths and HIV cases. While associations were demonstrated between access to the harm reduction vending machine and improved public health outcomes in the county where the machine was located, the results may be in part also due to other harm reduction initiatives being implemented in the same county.
Results may not generalize to other cities where there is less social and political support for harm reduction initiatives, if implementation of a dispensing machine is even possible in such locations.
Because the study only evaluated the impact of the machine during its first year, its impact beyond one year is unknown. It may be that there is a novelty effect that increased the benefits observed and this will fade in the following years. On the other hand, it is also possible that awareness of the machine will increase over time, leading to stronger benefits as more people use the machine.
There was an error that resulted in a delay in shutting off client access codes after 90 days that was not fixed until 2022. Accordingly, these individuals did not have to re-register for a code to continue using the machine and were not counted among those who re-enrolled. This limits longer term data for those who continually used the machine, which may have led to an underestimate of the machine’s full impact on overdose reversals.
BOTTOM LINE
Implementing a harm reduction dispensing machine appears to be associated with greater accessibility of harm reduction products and services and a lower local incidence of unintentional overdose deaths from opioids and HIV cases. While the researchers cannot conclude that the machine caused these effects, the results are promising and help to justify future research that may be able to demonstrate a causal association. This research helps toinform strategies for how to improve access to evidence-based harm reduction products, which can save lives and prevent disease.
For individuals and families seeking recovery: Harm reduction dispensing machines are not yet widely available, but the results of this study are consistent with other studies showing harm reduction productscan save lives and prevent disease. Accordingly, individuals who use opioids, and their families, could take advantage of access to such products, when possiblegiven state laws, and have products on hand. This would allow them to access them when needed and could lead to similar benefits. Individuals and their families can find information about how to access naloxone in their state on websites such as SAFEProject and the National Harm Reduction Coalition.
For treatment professionals and treatment systems: Although harm reduction dispensing machines are not yet widely available, the results of this study are consistent with other studies demonstrating the benefits of access to harm reduction products. Accordingly, treatment professionals and systems that support and encourage the use of harm reduction products and services are likely to see similar public health benefits. For instance, clinicians may encourage their clients who use opioids and other drugs to have harm reduction products on hand (when possible, given state laws), such as naloxone and fentanyl testing strips.
For scientists:Given that the implementation of dispensing machines has been limited, evaluation of their impact is also limited. Additional research that evaluates the impact of implementing dispensing machines in different contexts would lead to an increased understanding of who they benefit, under what circumstances, and how. Also, future research that uses a more rigorous study design than an observational onecould go beyond the associations demonstrated in the current study and support a stronger link between the machine and benefits observed. Finally, future research that evaluates the impact of the machine for longer than 1 year would shed light on its impact over time.
For policy makers: Results from this study are consistent with other studies that have demonstrated the public health benefits that implementing a harm reduction dispensing machine can have on increasing access to harm reduction products, reducing opioid overdose rates, and decreasing new cases of HIV.Implementation of dispensing machines and rigorous evaluation of their impact has been limited, however. Funding for implementation and rigorous evaluation of increased access to harm reduction services would help shed light on their impact. At a broader level, support of consistent, evidence-based policies that promote harm reduction services could also help to expand services in general, leading to lives saved and the spread of diseases prevented.
In particular, the Centers for Disease Control and Prevention have recommended that 10 of these harm reduction strategies be implemented, including distribution of naloxone (i.e., a drug that can reverse an opioid overdose) to those who are most likely to encounter an overdose and syringe services programs that provide access to sterile equipment and other harm reduction supplies and services. However, access to these services in the U.S. has been limited, in large part due to stigma. Because of the stigma and stereotypes against people who use drugs as undeserving of this type of care and untrustworthy, efforts to implement treatment and harm reduction services in neighborhoods have been protested against by the locals, consistent with “not in my back yard” (NIMBY) attitudes. Further, people who use drugs may be reluctant to access such services if offered because of how poorly they have been treated by healthcare professionals previously. Syringe dispensing machines may offer one way to help overcome this limitation.
Research has shown that syringe dispensing machines reduce needle sharing, increase access to sterile equipment, and are used by people who were less likely to attend in-person services. While several European countries and Australia have begun implementing syringe dispensing machines, the U.S. has been slow to do so. In 2017, Nevada became the first U.S. state to implement a syringe dispensing machine, with eventual inclusion of other harm reduction supplies, such as naloxone, and information about health services. Research that has examined the impact of these machines in the U.S., however, is limited, given the low rates of implementation, but early data is promising.
More recently, another machine was installed in Hamilton County in Cincinnati, Ohio, outside of an organization that provided in-person syringe services once a week (i.e., distribution of naloxone). County leaders did not allow syringes to be offered by the machine, but other harm reduction products were approved (e.g., naloxone, sterile equipment, fentanyl test strips, etc.). In this study, the research team evaluated the impact of this harm reduction dispensing machine on the accessibility of harm reduction supplies and the local incidence of fatal overdoses and HIV during its first year. Such research can help inform strategies for how to improve access to harm reduction products that have been shown to prevent overdose deaths and the spread of diseases transmitted through needle sharing.
HOW WAS THIS STUDY CONDUCTED?
The research team evaluated the impact of the harm reduction dispensing machine during its first year using an observational study design, in which the researchers tracked the number of supplies distributed by the machine and rates of fatal overdoses and HIV without intervening to try and change the outcomes.
To access the dispensing machine, clients anonymously registered over the phone with a coordinator, who gave them a unique access code and referred them as needed to other services, such as prenatal care and HIV testing. The access code allowed them to access the machine anytime (24 hours a day/7 days a week) and was valid for 90 days. After 90 days, they had to re-enroll and get another code, which provided another opportunity for the coordinators to connect them to additional services, if needed. During registration, clients were given the option to provide their name and contact information to allow the coordinators to follow up with them, as well as an option to participate in a survey that collected demographic information and other related information, such as previous use of harm reduction services. Providing contact information and participating in the survey were not required to be able to use the machine.
The machine contained 2 doses of intramuscular naloxone, 2 doses of naloxone nasal spray, a sharps container, a safer injection kit, a safer smoking kit, a Personal Protective Equipment kit, a safer sex kit, a pregnancy test, and a box of bandages. Clients could choose 1 of these items every 7 days throughout the 90 days that their code was valid.
The main outcome of interest was how many harm reduction supplies distributed by the machine alone in its first year (i.e., March 1, 2021 – March 1, 2022) compared to the amount of supplies distributed by the same organization within its brick-and-mortar service in the previous year. Additional outcomes the researchers were interested in included: (1) the number of naloxone doses and fentanyl test strips distributed by other syringe service programs in the county during the same time period, and (2) the incidence of fatal overdoses and HIV within the county compared to previous years.
Because this was an observational study, the researchers did not recruit people into the study or randomize them. Instead, they collected (optional) demographic information from the people who registered for a code to use the machine. During the machine’s first year, 637 people registered. The majority of people who registered were between 35 and 44 years old (41.1%) and White (90.9%). Approximately half identified as women and half identified as men. Twelve percent reported never having used harm reduction services previously. The 2 most requested products from the machine were smoking and injection kits, both which contained naloxone, making naloxone the most commonly distributed product.
Of the 637 people who initially registered, 105 registered for another code after 90 days. However, re-enrollment surveys were completed by a total of 124 people. This reflects 19 people who opted out of having their data collected and stored initially, but still used the machine and then decided to have their data collected and stored upon re-enrollment. Of note, there was an error that resulted in a delay in shutting off client access codes after 90 days that was not fixed until 2022, meaning that some people did not have to register for another code since they still had access. As such, the number of people who re-enrolled is lower than what it would have been if the system was working properly.
The demographics of the 105 people with both an initial and re-enrollment survey mirrored those of the full sample, with the majority being between 35 and 44 years old (51.4%) and White (96.2%). However, more women (62.9%) re-enrolled than men (36.2%)
WHAT DID THIS STUDY FIND?
The dispensing machine was associated with greater distribution of harm reduction supplies.
Of the 124 people who completed a re-enrollment survey: 86% reported receiving naloxone from the machine, with 71% reporting using it to reverse an overdose; 79% reported receiving fentanyl test strips from the machine, with 67% reporting that they detected fentanyl in their drug supply; 39% reported receiving a pregnancy test from the machine, which detected 13 pregnancies; and 12% reported receiving an HIV test from the machine, with no positive test results.
The machine alone distributed more sterile pipes, naloxone, fentanyl test strips, and pregnancy tests within its first year than the organization had within the previous year. Safer sex kits were the only item that the organization distributed more of than the machine.
Within the year, the dispensing machine was responsible for 100% of the sterile pipes, 69% of the naloxone doses, 72% of the fentanyl test strips, 100% of the pregnancy tests, and 27% of the safer sex kits distributed by the organization.
When compared to other syringe service programs in the county, the dispensing machine distributed over 1200 more doses of naloxone and 3800 more fentanyl test strips than the next largest program.
The dispensing machine was associated with decreases in fatal overdoses and HIV cases.
Contrary to rising opioid overdose incidence in Ohio and the United States overall, especially during COVID-19, Hamilton County (where the vending machine was located) reported a 10% decrease in unintentional overdose deaths, dropping from 499 in 2020 to 454 in 2021.
For HIV cases in counties neighboring Hamilton County, there was a decrease in the beginning of the pandemic, but cases then rose to pre-pandemic levels in 2021. Hamilton County avoided this trend and continued to observe decreases in 2021.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study evaluated the impact of installing an automated harm reduction dispensing machine on the accessibility of harm reduction supplies and the local incidence of fatal opioid overdoses and HIV during its first year. Results showed that implementation was associated with greater accessibility of harm reduction products and services and alower incidence of unintentional overdose death and HIV. It is noteworthy that the county observed approximately a 10% decrease in overdose rates while nationwide rates were greatly increasing. Although the research design prevents the researchers from being able to conclude that the machine caused greater access and fewer deaths and HIV cases, these promising results help justify future research that may be able to demonstrate a causal association.
These results cannot be disentangled from the effects of other harm reduction initiatives occurring in the same county or the broader social and political climate that supports such initiatives. It is likely that the observed results are attributable to a combination of initiatives that are made possible through the support of local government. While these findings are consistent with the early results from Las Vegas that similarly showed an association between installation of a dispensing machine and fewer opioid overdose deaths, both were likely implemented along with a variety of other harm reduction and recovery support services. Thus, when provided together, these services may potentially play a complementary role in helping to address the opioid crisis.
However, what is important and unique about the dispensing machine is that it can be accessed 24 hours a day, 7 days a week, and can bedone so with complete anonymity. As such, it can help expand access to harm reduction products when other services are not available and reach people who prefer to remain anonymous and avoid potential stigma. Indeed, 12% of people who used the machine reported that they had never used harm reduction products or services previously. Accordingly, the machines can help to fill a critical gap in existing harm reduction services and highlight the importance of accessibility and anonymity.
In general, the results of this study add to the research demonstrating the public health benefits of expanding access to harm reduction products and services. A key barrier to doing so, however, are drug laws that are not supported by scientific evidence and instead take a punitive approach. Drug laws are also variable across states, which further contributes to the difficulty involved in expansion. Consistent, evidence-based policies that take a public health approach could address these barriers, leading to increased access and lives saved.
The research design prevents the researchers from being able to conclude that the dispensing machinescaused greater access and fewer deaths and HIV cases. While associations were demonstrated between access to the harm reduction vending machine and improved public health outcomes in the county where the machine was located, the results may be in part also due to other harm reduction initiatives being implemented in the same county.
Results may not generalize to other cities where there is less social and political support for harm reduction initiatives, if implementation of a dispensing machine is even possible in such locations.
Because the study only evaluated the impact of the machine during its first year, its impact beyond one year is unknown. It may be that there is a novelty effect that increased the benefits observed and this will fade in the following years. On the other hand, it is also possible that awareness of the machine will increase over time, leading to stronger benefits as more people use the machine.
There was an error that resulted in a delay in shutting off client access codes after 90 days that was not fixed until 2022. Accordingly, these individuals did not have to re-register for a code to continue using the machine and were not counted among those who re-enrolled. This limits longer term data for those who continually used the machine, which may have led to an underestimate of the machine’s full impact on overdose reversals.
BOTTOM LINE
Implementing a harm reduction dispensing machine appears to be associated with greater accessibility of harm reduction products and services and a lower local incidence of unintentional overdose deaths from opioids and HIV cases. While the researchers cannot conclude that the machine caused these effects, the results are promising and help to justify future research that may be able to demonstrate a causal association. This research helps toinform strategies for how to improve access to evidence-based harm reduction products, which can save lives and prevent disease.
For individuals and families seeking recovery: Harm reduction dispensing machines are not yet widely available, but the results of this study are consistent with other studies showing harm reduction productscan save lives and prevent disease. Accordingly, individuals who use opioids, and their families, could take advantage of access to such products, when possiblegiven state laws, and have products on hand. This would allow them to access them when needed and could lead to similar benefits. Individuals and their families can find information about how to access naloxone in their state on websites such as SAFEProject and the National Harm Reduction Coalition.
For treatment professionals and treatment systems: Although harm reduction dispensing machines are not yet widely available, the results of this study are consistent with other studies demonstrating the benefits of access to harm reduction products. Accordingly, treatment professionals and systems that support and encourage the use of harm reduction products and services are likely to see similar public health benefits. For instance, clinicians may encourage their clients who use opioids and other drugs to have harm reduction products on hand (when possible, given state laws), such as naloxone and fentanyl testing strips.
For scientists:Given that the implementation of dispensing machines has been limited, evaluation of their impact is also limited. Additional research that evaluates the impact of implementing dispensing machines in different contexts would lead to an increased understanding of who they benefit, under what circumstances, and how. Also, future research that uses a more rigorous study design than an observational onecould go beyond the associations demonstrated in the current study and support a stronger link between the machine and benefits observed. Finally, future research that evaluates the impact of the machine for longer than 1 year would shed light on its impact over time.
For policy makers: Results from this study are consistent with other studies that have demonstrated the public health benefits that implementing a harm reduction dispensing machine can have on increasing access to harm reduction products, reducing opioid overdose rates, and decreasing new cases of HIV.Implementation of dispensing machines and rigorous evaluation of their impact has been limited, however. Funding for implementation and rigorous evaluation of increased access to harm reduction services would help shed light on their impact. At a broader level, support of consistent, evidence-based policies that promote harm reduction services could also help to expand services in general, leading to lives saved and the spread of diseases prevented.