Buprenorphine and harm reduction supplies in primary care: Which combinations benefit patients and cut costs?
Given increased rates of opioid-related deaths and injection-related harms, it is essential to identify optimal ways to invest limited financial resources. This study evaluated the outcomes and cost-effectiveness of providing buprenorphine treatment and harm reduction supplies in primary care.
Medication treatments for opioid use disorder, like buprenorphine are often lifesaving, help support treatment and recovery, and reduce death and disability. However, some patients continue to inject illicit opioids during buprenorphine treatment, and injection opioid use comes with its own set of health risks that demand attention.
Harm reduction services are intended to reduce harms associated with risky health behaviors, like injection drug use. Harm reduction approaches include strategies like distribution of the opioid overdose reversal drug (naloxone) and sterile injection equipment (e.g., needles, wound care supplies, fentanyl test strips) to people who need them. These services are shown to be cost effective on their own, help lower risk of injection-related harms, and improve patient outcomes (e.g., reduced rates of infection and infectious diseases, reduced substance use, reduced injection drug use, prevention of fatal overdose).
Though an increasing number of patients are receiving buprenorphine treatment for opioid use disorder through primary care practices, harm reduction tools are not commonly provided alongside buprenorphine in these healthcare settings. Providing patients with both medication treatment and harm reduction services in one location might help to better address the opioid epidemic, by concurrently addressing opioid-related deaths and injection-related harms like infection to improve patient outcomes. However, it is unclear if the cost of integrating these services into primary care outweighs their beneficial effects on patient outcomes.
Effectiveness studies help determine the benefits of various treatments and cost-effectiveness studies help determine which treatments are best when considering both the benefits of the treatment and any investments and savings associated with providing them. Together, this information can inform policies regarding the most optimal types of treatment delivery settings and models that should be paid for and delivered. The current study examined long-term patient outcomes, healthcare costs, and the cost-effectiveness of integrating onsite buprenorphine treatment and harm reduction services into primary care models for the treatment of injection opioid use.
HOW WAS THIS STUDY CONDUCTED?
The authors conducted a model-based analysis of 2.25 million simulated people representative of the U.S. population that inject opioids to assess the effects of various primary care treatment strategies on long-term patient outcomes (i.e., drug-related deaths and healthcare events) and healthcare costs over the entire lifetime of the simulated study sample. Cost-effectiveness of each treatment was also evaluated.
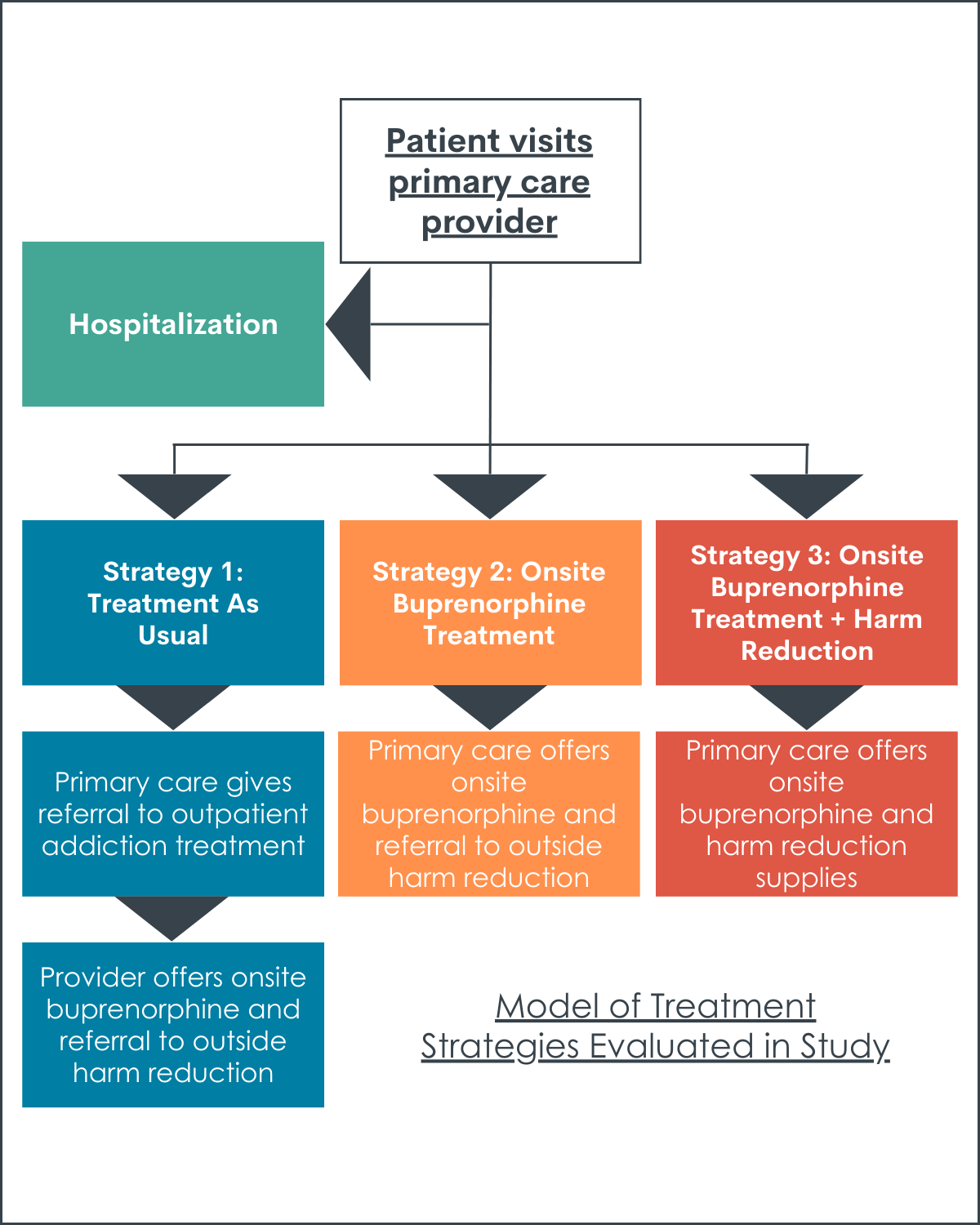
Values entered into the model were based on data from clinical trials and observational studies in the scientific literature. The researchers evaluated three treatment strategies, which included primary care services plus:
1) Outside referral to outpatient buprenorphine treatment (i.e., treatment as usual)
2) Onsite buprenorphine treatment and outside referral to community-based harm reduction services (i.e., onsite buprenorphine treatment)
3) Onsite buprenorphine treatment and onsite provision of harm reduction kits at every office-based primary care visit (i.e., onsite buprenorphine treatment + harm reduction)
Harm reduction kits were assumed to include 10 sterile syringes with injection preparation equipment, a safer smoking kit, skin hygiene supplies, and wound care supplies. The figure below shows the three possible treatment strategies and the paths a simulated patient can take within each strategy. When offered or referred to services, patients could either accept buprenorphine treatment or refuse buprenorphine treatment and leave care.
The researchers evaluated the following long-term patient outcomes:
1) Life expectancy (years)
2) Deaths due to overdose, severe skin or soft tissue infection, and infective endocarditis (% or number per 10,000 people)
3) Number of lifetime hospitalizations per 100,000 people
4) Number of lifetime non-fatal skin and soft-tissue infections per 100,000 people
5) Average lifetime medical costs per person (see below for the costs considered)
To assess cost-effectiveness, the authors calculated the additional cost per person of implementing each treatment strategy and the life years gained (the additional number of years that a person lives as a result of receiving a treatment, with higher values indicating better outcomes) for each treatment modality. Costs included:
1) Background costs of being alive (i.e. age and sex stratified costs of being alive as estimated by the Medical Expenditure Panel Survey)
2) Injection drug use
3) Fatal and non-fatal overdose, without hospitalization
4) Untreated heart (endocarditis), skin, and soft-tissue infections
5) Hospitalization for overdose, and endocarditis, skin, and soft-tissue infections
6) Inpatient and outpatient service costs, including opioid use disorder medication treatment.
Cost effectiveness of each treatment was examined as the cost of treatment for each life year gained, relative to the next less expensive treatment. The researchers also evaluated the impact of providing buprenorphine and harm reduction kits on primary care practice budgets over a 5-year period. Cost savings in healthcare, criminal justice, and other systems, as a result of each treatment were not considered in analyses.
The researchers took sex, age, and injection behaviors into consideration in their simulated models. The models assumed that patients:
1) Were not receiving opioid use disorder medication treatment and did not have a history of overdose or infection at the start of the study
2) Who were hospitalized and not receiving medication treatment at that time would undergo medically supervised detoxification and would not receive medication treatment
3) Who were hospitalized and receiving medication treatment at that time would continue medication when discharged
4) Who received treatment as usual, or onsite buprenorphine treatment without onsite harm reduction services, received harm reduction kits through the community
5) Who received onsite buprenorphine and harm reduction kits also received naloxone during their first primary care visit
6) Who engaged in higher frequency injection drug use incurred more healthcare costs
At the start of the study, the simulated sample was primarily made up of men (70%) in their 40’s. Half of the sample engaged in high frequency injection opioid use, 10% engaged in low-frequency use, and 40% did not engage in injection use at study start. The majority of the sample engaged in unsterile injection opioid use (66%) and about one-third regularly shared injection equipment (35%).
WHAT DID THIS STUDY FIND?
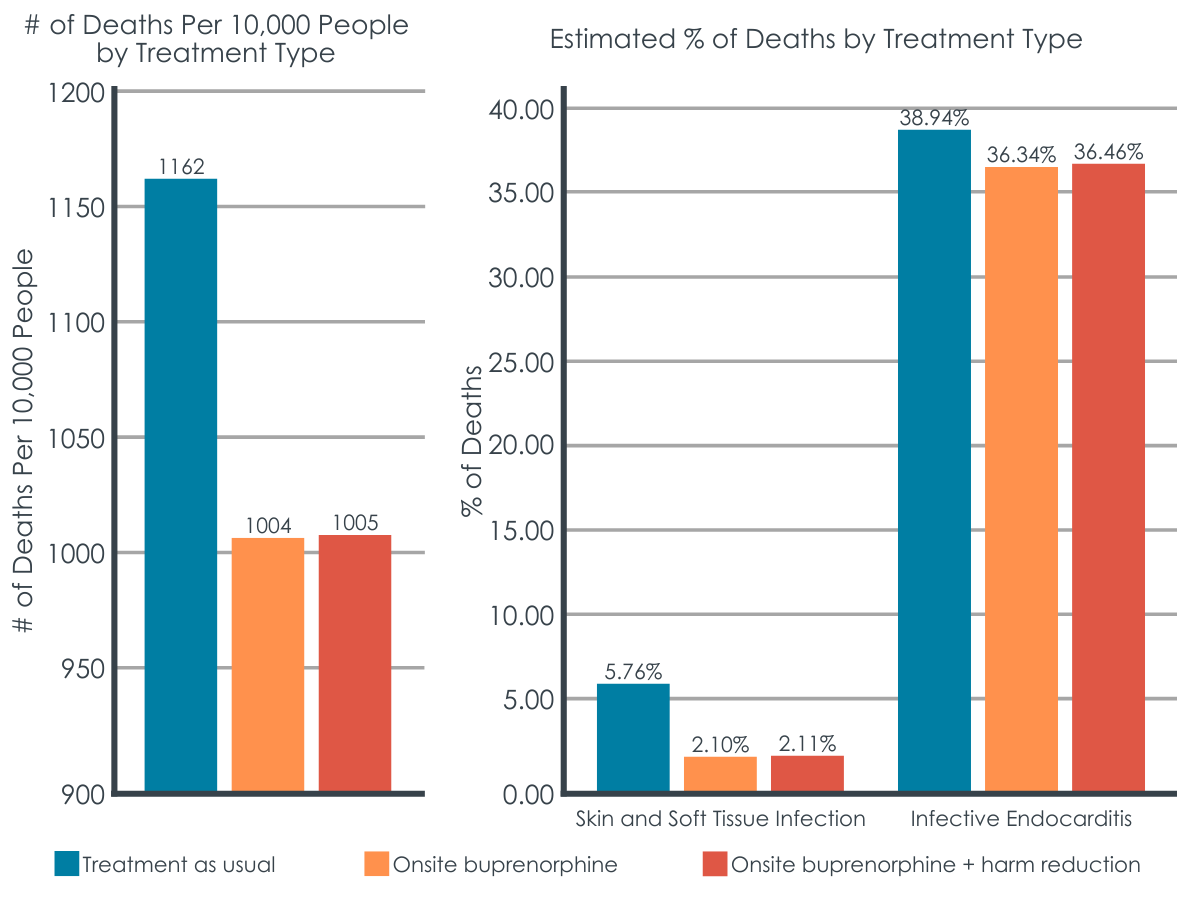
Onsite buprenorphine with and without harm reduction services was associated with fewer deaths than treatment as usual.
Compared to treatment as usual, onsite buprenorphine with and without onsite harm reduction services extended estimated life expectancy by about 2.7 years and resulted in a 33% decrease in estimated overdose- and infection-related deaths. There were 160 fewer overdose deaths per 10,000 people, 3.5% fewer deaths due to skin and soft tissue infections and 2.5% fewer deaths due to infective endocarditis in absolute terms (a 61% and 7% improvement over treatment as usual, respectively).
Figures 2.1 and 2.2 above depict the number of overdose deaths per 10,000 people (left) and the estimated percentage of deaths due to infection (right), for each treatment strategy.
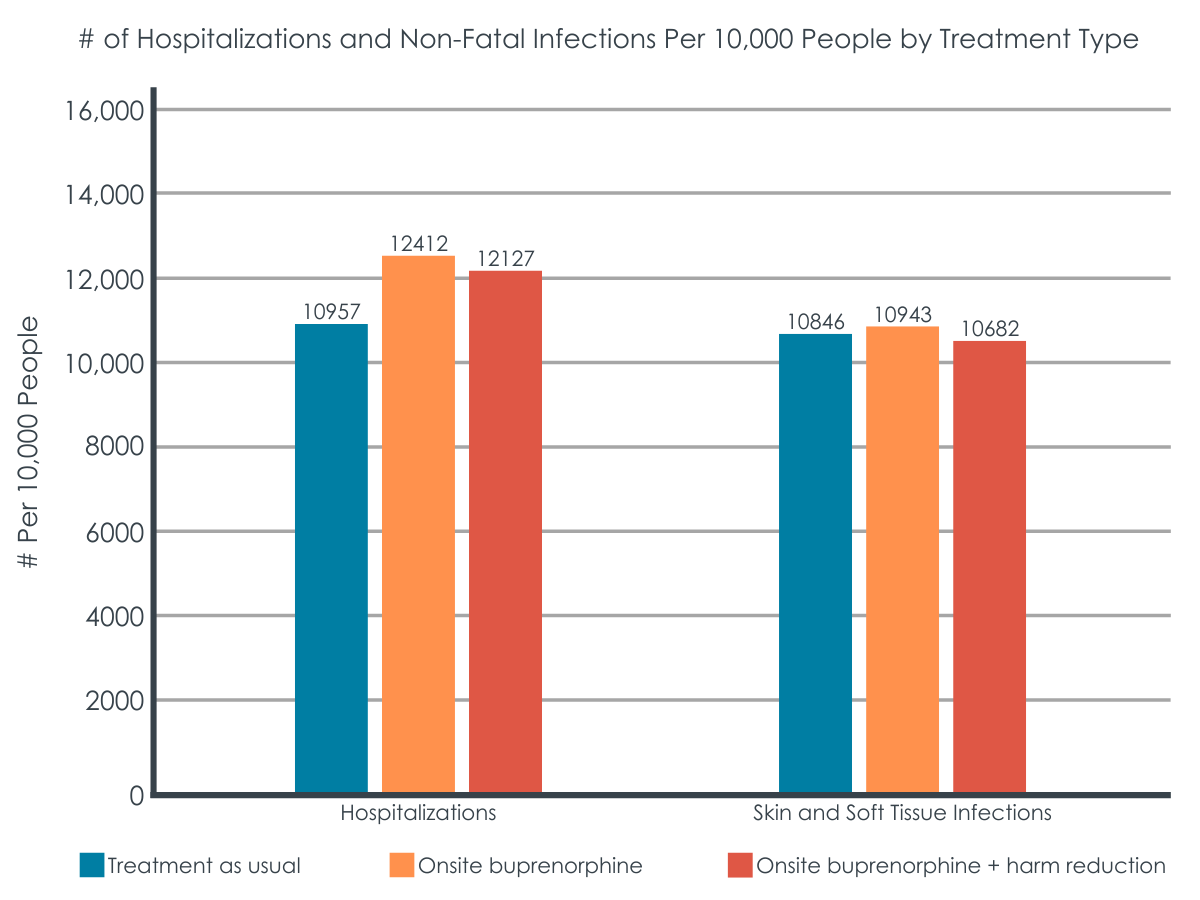
Buprenorphine alone was associated with more lifetime hospitalizations, but combined buprenorphine and harm-reduction was associated with fewer infections.
Because buprenorphine increased life expectancy, which meant more time and opportunity for people to continue using illicit substances and encounter adverse events requiring hospitalizations, a larger number of hospitalizations were estimated to occur with onsite buprenorphine alone and combined with harm reduction services, relative to treatment as usual. Non-fatal skin and soft-tissue infections were also more prevalent with onsite buprenorphine than treatment as usual. However, combined onsite buprenorphine and harm-reduction produced the fewest skin and soft-tissue infections.
Figure 3 shows the number of hospitalizations and non-fatal infections per 10,000 people, for each treatment strategy.
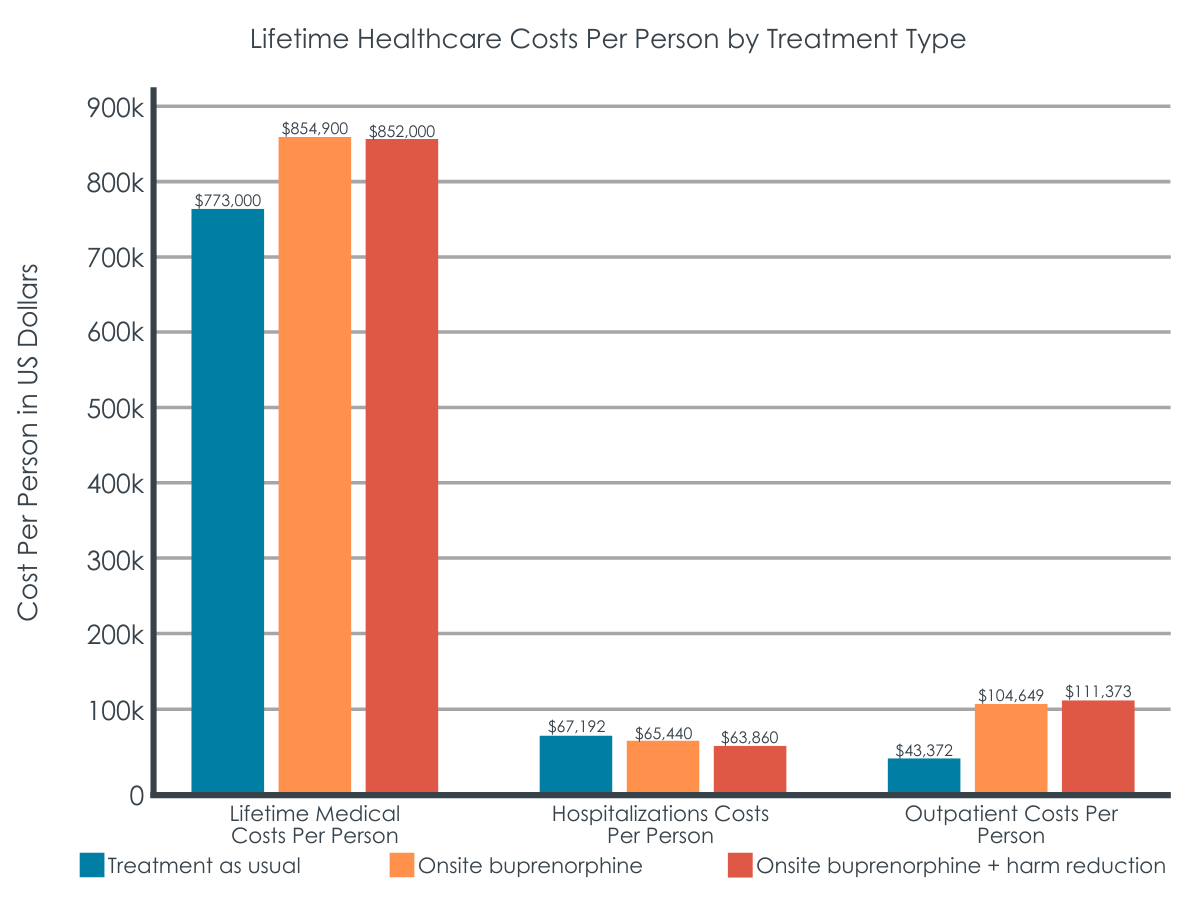
Onsite buprenorphine plus harm reduction was the most cost-effective strategy.
Compared to treatment as usual, lifetime medical costs per person were higher when patients received onsite buprenorphine alone or in combination with harm reduction, increasing by about 69% and 74%, respectively. While costs associated with hospitalization decreased, outpatient costs increased.
When the authors considered healthcare cost savings in the context of life years (i.e., cost effectiveness), only onsite buprenorphine plus harm reduction emerged as cost effective (i.e., costs $34,400 for each life year gained, per person, compared to treatment as usual). Integrating onsite buprenorphine treatment and harm reduction services was estimated to cost a primary care practice about $13,000 over a 5-year period.
Figure 4 depicts total medical costs accrued during each person’s lifetime, as well as lifetime hospitalization costs for overdose/infection and lifetime outpatient costs per person, for each treatment strategy.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better identify cost-effective methods for enhancing standard treatments for opioid use disorder that improve patient outcomes. This study found that the provision of buprenorphine alone or in combination with harm reduction kits is associated with lower rates of drug-related deaths (i.e., due to overdose, skin and soft tissue infection, and infective endocarditis) and a longer life expectancy (2.7 life years gained per person), compared to treatment as usual (i.e., referral to outpatient addiction treatment). Because increased life expectancy resulted in more time available for a person to experience drug-related harms and engage in the use of healthcare services, buprenorphine with or without harm reduction resulted in more hospitalizations than treatment as usual. Increased non-fatal skin and soft-tissue infections were also more prevalent with onsite buprenorphine treatment, but only when it was provided without onsite harm reduction services. Thus, providing harm-reduction services alongside buprenorphine in primary care settings might help increase patients’ use of sterile injection equipment and, in turn, help reduce their risk of infection-related health problems.
Though lifetime medical costs generally increased when implementing buprenorphine with or without harm reduction, these increased costs were largely driven by the cost of outpatient treatment, as opposed to drug-related harms and critical-care events. Thus, integration of addiction treatment into primary care services might increase the use of non-emergency healthcare services (e.g., regular primary care visits), which is consistent with previous research. Again, increased life expectancy with buprenorphine meant that patients had greater opportunity to engage in the healthcare system, resulting in greater healthcare costs. Despite this seeming increase in overall costs, the reduced cost of acute medical emergencies and hospitalizations might help to offset outpatient costs within healthcare systems. Increased outpatient service use is beneficial, as patients will have increased opportunity to engage in buprenorphine treatment, as well as address other chronic illnesses and injection-related harms during primary care visits. This would help avoid serious complications from infections related to injection opioid use that might otherwise result in acute hospitalization or mortality.
Interestingly, only the combined onsite provision of buprenorphine and harm reduction was deemed cost effective. The onsite provision of buprenorphine treatment without harm reduction services proved to be more expensive and less effective in terms of life years gained. Combined onsite buprenorphine and harm reduction services improved patient outcomes, decreased drug-related deaths, and increased life expectancy, compared to treatment as usual. It may be that buprenorphine alone is not enough to offset the cost of injection-related harms (e.g., infections & related health-care use), and providing harm-reduction kits alongside buprenorphine in primary care can help save on healthcare costs in the long run, by preventing harms associated with using unsterile injection equipment. Indeed, other research using computer simulations has shown that combining harm reduction with other services, like recovery support services, has the greatest benefit (e.g., reduces patient harm like overdose) in the long-term. Onsite harm reduction kits are not provided as the standard of care in primary care settings. Integrating these kits into primary care settings might enhance treatment engagement and/or provide useful tools for reducing injection-related risks during times of active opioid use. Importantly, the benefits of harm reduction kits were seen even though the researchers’ simulated model assumed that a fixed amount of safe injection equipment was included in the kits that would only last about 1 week for people engaging in frequent injection drug use. This highlights the potential benefits of convenient access to harm-reduction kits for reducing injection-related harms, health complications, and lengthy hospital stays.
Importantly, this study evaluated costs from a healthcare perspective and compared onsite buprenorphine and harm reduction services relative to a buprenorphine treatment referral. Prior research looking at patient and healthcare system costs have found buprenorphine to be cost effective on its own, without harm reduction, when compared to no treatment. This study extends this area of research by suggesting that providing buprenorphine plus add-on harm reduction services in primary care might be the most cost-effective treatment model from a healthcare perspective. Though offering combined buprenorphine and harm reduction services in primary care may cost practices an additional $13,000 every five years, these costs might be offset by the savings in broader healthcare system costs, with fewer patients needing lengthy hospital stays to address complications (e.g., infection). The costs estimated in this study also included X-waiver training, which used to be required in order for providers to prescribe buprenorphine (no longer needed as of June 2023), meaning that this cost is likely overestimated. Additional research is needed to evaluate cost-effective treatment models in the absence of X waivers, given that associated costs no longer apply.
These analyses and models were simulated and based on available data. Additionally, race/ethnicity, incarceration, treatment retention, and other patient-oriented outcomes (e.g., quality of life) were not factored into the model. Outcomes are likely close-to but not an exact reflection of actual costs accrued by individuals and longitudinal studies in diverse populations are needed to confirm these findings.
Other medication treatments, such as extended-release buprenorphine (i.e., Sublocade) and extended -release naltrexone (i.e., Vivitrol) were not assessed in this study and additional research is needed to determine their effects and cost-effectiveness when combined with harm reduction services.
Patients receiving treatment as usual, or onsite buprenorphine treatment without onsite harm reduction services, were assumed to have received harm reduction kits through the community. Given that not all patients are aware of harm reduction services, and not all who receive harm reduction referrals actually pursue them, this might have underestimated the beneficial effects of providing combined onsite buprenorphine and harm reduction services in primary care.
BOTTOM LINE
Studies like this help us better identify the most effective and financially sustainable treatment models for opioid use disorder, which can inform policies and reveal service models that are worth pursuing. This study found that, compared to treatment as usual (i.e., outpatient referral to buprenorphine treatment by a primary care physician), the provision of buprenorphine and harm reduction kits in primary care settings improved patient outcomes, decreased drug-related deaths, increased life expectancy, and was more cost effective than providing onsite buprenorphine without harm reduction kits.
For individuals and families seeking recovery: Individuals who are receiving opioid use disorder medication treatment might benefit from add-on services like harm reduction, as they could improve patient outcomes, reduce the risk of drug-related death, and increase a person’s life expectancy. Harm reduction services are not typically offered in primary care treatment settings, but they are often available through the community. Interested individuals can find harm reduction services near them through the National Harm Reduction Coalition.
For treatment professionals and treatment systems: Healthcare systems might consider providing harm reduction kits with opioid use disorder medication treatment, as this seems to be a cost-effective option that can help prevent drug-related deaths and complications (e.g., overdose, infection), and increase patients’ life expectancy. Since providing medication and harm reduction kits in primary care practices is more cost effective and results in better outcomes than referrals to offsite harm reduction services, offering these services within primary care practices is ideal when possible.
For scientists: Additional research is needed to determine the patient benefits and cost-effectiveness of providing concurrent opioid use disorder medication and harm reduction services within primary care practices, including research using real-world data. Studies are needed to identify (1) effects other than drug-related deaths and service use, (2) the patient populations that benefit most from harm reduction services and other recovery supports, (3) the most cost-effective treatment models in different types of healthcare settings, and (4) cost-effectiveness in the absence of the X waiver.
For policy makers: Providing harm reduction services alongside medication treatment is cost effective compared to treatment as usual (i.e., referral to addiction treatment and harm reduction services), costing about $34,000 for each life year gained, per person, compared to treatment as usual. Providing buprenorphine without harm reduction services was more expensive and less effective. Though provision of buprenorphine and harm reduction kits within primary care is associated with increased costs to healthcare systems, it was the most cost-effective option in the long run, improved patient outcomes, decreased drug-related deaths, and increased life expectancy. Thus, providing medication treatment and harm reduction in primary care practices is a potential cost-effective option for enhancing medication treatment and reducing opioid-related deaths. Additional funding may help identify cost-effectiveness in the absence of the X waiver and other services that improve patient outcomes and help expand access to harm reduction services.
Medication treatments for opioid use disorder, like buprenorphine are often lifesaving, help support treatment and recovery, and reduce death and disability. However, some patients continue to inject illicit opioids during buprenorphine treatment, and injection opioid use comes with its own set of health risks that demand attention.
Harm reduction services are intended to reduce harms associated with risky health behaviors, like injection drug use. Harm reduction approaches include strategies like distribution of the opioid overdose reversal drug (naloxone) and sterile injection equipment (e.g., needles, wound care supplies, fentanyl test strips) to people who need them. These services are shown to be cost effective on their own, help lower risk of injection-related harms, and improve patient outcomes (e.g., reduced rates of infection and infectious diseases, reduced substance use, reduced injection drug use, prevention of fatal overdose).
Though an increasing number of patients are receiving buprenorphine treatment for opioid use disorder through primary care practices, harm reduction tools are not commonly provided alongside buprenorphine in these healthcare settings. Providing patients with both medication treatment and harm reduction services in one location might help to better address the opioid epidemic, by concurrently addressing opioid-related deaths and injection-related harms like infection to improve patient outcomes. However, it is unclear if the cost of integrating these services into primary care outweighs their beneficial effects on patient outcomes.
Effectiveness studies help determine the benefits of various treatments and cost-effectiveness studies help determine which treatments are best when considering both the benefits of the treatment and any investments and savings associated with providing them. Together, this information can inform policies regarding the most optimal types of treatment delivery settings and models that should be paid for and delivered. The current study examined long-term patient outcomes, healthcare costs, and the cost-effectiveness of integrating onsite buprenorphine treatment and harm reduction services into primary care models for the treatment of injection opioid use.
HOW WAS THIS STUDY CONDUCTED?
The authors conducted a model-based analysis of 2.25 million simulated people representative of the U.S. population that inject opioids to assess the effects of various primary care treatment strategies on long-term patient outcomes (i.e., drug-related deaths and healthcare events) and healthcare costs over the entire lifetime of the simulated study sample. Cost-effectiveness of each treatment was also evaluated.
Values entered into the model were based on data from clinical trials and observational studies in the scientific literature. The researchers evaluated three treatment strategies, which included primary care services plus:
1) Outside referral to outpatient buprenorphine treatment (i.e., treatment as usual)
2) Onsite buprenorphine treatment and outside referral to community-based harm reduction services (i.e., onsite buprenorphine treatment)
3) Onsite buprenorphine treatment and onsite provision of harm reduction kits at every office-based primary care visit (i.e., onsite buprenorphine treatment + harm reduction)
Harm reduction kits were assumed to include 10 sterile syringes with injection preparation equipment, a safer smoking kit, skin hygiene supplies, and wound care supplies. The figure below shows the three possible treatment strategies and the paths a simulated patient can take within each strategy. When offered or referred to services, patients could either accept buprenorphine treatment or refuse buprenorphine treatment and leave care.
The researchers evaluated the following long-term patient outcomes:
1) Life expectancy (years)
2) Deaths due to overdose, severe skin or soft tissue infection, and infective endocarditis (% or number per 10,000 people)
3) Number of lifetime hospitalizations per 100,000 people
4) Number of lifetime non-fatal skin and soft-tissue infections per 100,000 people
5) Average lifetime medical costs per person (see below for the costs considered)
To assess cost-effectiveness, the authors calculated the additional cost per person of implementing each treatment strategy and the life years gained (the additional number of years that a person lives as a result of receiving a treatment, with higher values indicating better outcomes) for each treatment modality. Costs included:
1) Background costs of being alive (i.e. age and sex stratified costs of being alive as estimated by the Medical Expenditure Panel Survey)
2) Injection drug use
3) Fatal and non-fatal overdose, without hospitalization
4) Untreated heart (endocarditis), skin, and soft-tissue infections
5) Hospitalization for overdose, and endocarditis, skin, and soft-tissue infections
6) Inpatient and outpatient service costs, including opioid use disorder medication treatment.
Cost effectiveness of each treatment was examined as the cost of treatment for each life year gained, relative to the next less expensive treatment. The researchers also evaluated the impact of providing buprenorphine and harm reduction kits on primary care practice budgets over a 5-year period. Cost savings in healthcare, criminal justice, and other systems, as a result of each treatment were not considered in analyses.
The researchers took sex, age, and injection behaviors into consideration in their simulated models. The models assumed that patients:
1) Were not receiving opioid use disorder medication treatment and did not have a history of overdose or infection at the start of the study
2) Who were hospitalized and not receiving medication treatment at that time would undergo medically supervised detoxification and would not receive medication treatment
3) Who were hospitalized and receiving medication treatment at that time would continue medication when discharged
4) Who received treatment as usual, or onsite buprenorphine treatment without onsite harm reduction services, received harm reduction kits through the community
5) Who received onsite buprenorphine and harm reduction kits also received naloxone during their first primary care visit
6) Who engaged in higher frequency injection drug use incurred more healthcare costs
At the start of the study, the simulated sample was primarily made up of men (70%) in their 40’s. Half of the sample engaged in high frequency injection opioid use, 10% engaged in low-frequency use, and 40% did not engage in injection use at study start. The majority of the sample engaged in unsterile injection opioid use (66%) and about one-third regularly shared injection equipment (35%).
WHAT DID THIS STUDY FIND?
Onsite buprenorphine with and without harm reduction services was associated with fewer deaths than treatment as usual.
Compared to treatment as usual, onsite buprenorphine with and without onsite harm reduction services extended estimated life expectancy by about 2.7 years and resulted in a 33% decrease in estimated overdose- and infection-related deaths. There were 160 fewer overdose deaths per 10,000 people, 3.5% fewer deaths due to skin and soft tissue infections and 2.5% fewer deaths due to infective endocarditis in absolute terms (a 61% and 7% improvement over treatment as usual, respectively).
Figures 2.1 and 2.2 above depict the number of overdose deaths per 10,000 people (left) and the estimated percentage of deaths due to infection (right), for each treatment strategy.
Buprenorphine alone was associated with more lifetime hospitalizations, but combined buprenorphine and harm-reduction was associated with fewer infections.
Because buprenorphine increased life expectancy, which meant more time and opportunity for people to continue using illicit substances and encounter adverse events requiring hospitalizations, a larger number of hospitalizations were estimated to occur with onsite buprenorphine alone and combined with harm reduction services, relative to treatment as usual. Non-fatal skin and soft-tissue infections were also more prevalent with onsite buprenorphine than treatment as usual. However, combined onsite buprenorphine and harm-reduction produced the fewest skin and soft-tissue infections.
Figure 3 shows the number of hospitalizations and non-fatal infections per 10,000 people, for each treatment strategy.
Onsite buprenorphine plus harm reduction was the most cost-effective strategy.
Compared to treatment as usual, lifetime medical costs per person were higher when patients received onsite buprenorphine alone or in combination with harm reduction, increasing by about 69% and 74%, respectively. While costs associated with hospitalization decreased, outpatient costs increased.
When the authors considered healthcare cost savings in the context of life years (i.e., cost effectiveness), only onsite buprenorphine plus harm reduction emerged as cost effective (i.e., costs $34,400 for each life year gained, per person, compared to treatment as usual). Integrating onsite buprenorphine treatment and harm reduction services was estimated to cost a primary care practice about $13,000 over a 5-year period.
Figure 4 depicts total medical costs accrued during each person’s lifetime, as well as lifetime hospitalization costs for overdose/infection and lifetime outpatient costs per person, for each treatment strategy.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better identify cost-effective methods for enhancing standard treatments for opioid use disorder that improve patient outcomes. This study found that the provision of buprenorphine alone or in combination with harm reduction kits is associated with lower rates of drug-related deaths (i.e., due to overdose, skin and soft tissue infection, and infective endocarditis) and a longer life expectancy (2.7 life years gained per person), compared to treatment as usual (i.e., referral to outpatient addiction treatment). Because increased life expectancy resulted in more time available for a person to experience drug-related harms and engage in the use of healthcare services, buprenorphine with or without harm reduction resulted in more hospitalizations than treatment as usual. Increased non-fatal skin and soft-tissue infections were also more prevalent with onsite buprenorphine treatment, but only when it was provided without onsite harm reduction services. Thus, providing harm-reduction services alongside buprenorphine in primary care settings might help increase patients’ use of sterile injection equipment and, in turn, help reduce their risk of infection-related health problems.
Though lifetime medical costs generally increased when implementing buprenorphine with or without harm reduction, these increased costs were largely driven by the cost of outpatient treatment, as opposed to drug-related harms and critical-care events. Thus, integration of addiction treatment into primary care services might increase the use of non-emergency healthcare services (e.g., regular primary care visits), which is consistent with previous research. Again, increased life expectancy with buprenorphine meant that patients had greater opportunity to engage in the healthcare system, resulting in greater healthcare costs. Despite this seeming increase in overall costs, the reduced cost of acute medical emergencies and hospitalizations might help to offset outpatient costs within healthcare systems. Increased outpatient service use is beneficial, as patients will have increased opportunity to engage in buprenorphine treatment, as well as address other chronic illnesses and injection-related harms during primary care visits. This would help avoid serious complications from infections related to injection opioid use that might otherwise result in acute hospitalization or mortality.
Interestingly, only the combined onsite provision of buprenorphine and harm reduction was deemed cost effective. The onsite provision of buprenorphine treatment without harm reduction services proved to be more expensive and less effective in terms of life years gained. Combined onsite buprenorphine and harm reduction services improved patient outcomes, decreased drug-related deaths, and increased life expectancy, compared to treatment as usual. It may be that buprenorphine alone is not enough to offset the cost of injection-related harms (e.g., infections & related health-care use), and providing harm-reduction kits alongside buprenorphine in primary care can help save on healthcare costs in the long run, by preventing harms associated with using unsterile injection equipment. Indeed, other research using computer simulations has shown that combining harm reduction with other services, like recovery support services, has the greatest benefit (e.g., reduces patient harm like overdose) in the long-term. Onsite harm reduction kits are not provided as the standard of care in primary care settings. Integrating these kits into primary care settings might enhance treatment engagement and/or provide useful tools for reducing injection-related risks during times of active opioid use. Importantly, the benefits of harm reduction kits were seen even though the researchers’ simulated model assumed that a fixed amount of safe injection equipment was included in the kits that would only last about 1 week for people engaging in frequent injection drug use. This highlights the potential benefits of convenient access to harm-reduction kits for reducing injection-related harms, health complications, and lengthy hospital stays.
Importantly, this study evaluated costs from a healthcare perspective and compared onsite buprenorphine and harm reduction services relative to a buprenorphine treatment referral. Prior research looking at patient and healthcare system costs have found buprenorphine to be cost effective on its own, without harm reduction, when compared to no treatment. This study extends this area of research by suggesting that providing buprenorphine plus add-on harm reduction services in primary care might be the most cost-effective treatment model from a healthcare perspective. Though offering combined buprenorphine and harm reduction services in primary care may cost practices an additional $13,000 every five years, these costs might be offset by the savings in broader healthcare system costs, with fewer patients needing lengthy hospital stays to address complications (e.g., infection). The costs estimated in this study also included X-waiver training, which used to be required in order for providers to prescribe buprenorphine (no longer needed as of June 2023), meaning that this cost is likely overestimated. Additional research is needed to evaluate cost-effective treatment models in the absence of X waivers, given that associated costs no longer apply.
These analyses and models were simulated and based on available data. Additionally, race/ethnicity, incarceration, treatment retention, and other patient-oriented outcomes (e.g., quality of life) were not factored into the model. Outcomes are likely close-to but not an exact reflection of actual costs accrued by individuals and longitudinal studies in diverse populations are needed to confirm these findings.
Other medication treatments, such as extended-release buprenorphine (i.e., Sublocade) and extended -release naltrexone (i.e., Vivitrol) were not assessed in this study and additional research is needed to determine their effects and cost-effectiveness when combined with harm reduction services.
Patients receiving treatment as usual, or onsite buprenorphine treatment without onsite harm reduction services, were assumed to have received harm reduction kits through the community. Given that not all patients are aware of harm reduction services, and not all who receive harm reduction referrals actually pursue them, this might have underestimated the beneficial effects of providing combined onsite buprenorphine and harm reduction services in primary care.
BOTTOM LINE
Studies like this help us better identify the most effective and financially sustainable treatment models for opioid use disorder, which can inform policies and reveal service models that are worth pursuing. This study found that, compared to treatment as usual (i.e., outpatient referral to buprenorphine treatment by a primary care physician), the provision of buprenorphine and harm reduction kits in primary care settings improved patient outcomes, decreased drug-related deaths, increased life expectancy, and was more cost effective than providing onsite buprenorphine without harm reduction kits.
For individuals and families seeking recovery: Individuals who are receiving opioid use disorder medication treatment might benefit from add-on services like harm reduction, as they could improve patient outcomes, reduce the risk of drug-related death, and increase a person’s life expectancy. Harm reduction services are not typically offered in primary care treatment settings, but they are often available through the community. Interested individuals can find harm reduction services near them through the National Harm Reduction Coalition.
For treatment professionals and treatment systems: Healthcare systems might consider providing harm reduction kits with opioid use disorder medication treatment, as this seems to be a cost-effective option that can help prevent drug-related deaths and complications (e.g., overdose, infection), and increase patients’ life expectancy. Since providing medication and harm reduction kits in primary care practices is more cost effective and results in better outcomes than referrals to offsite harm reduction services, offering these services within primary care practices is ideal when possible.
For scientists: Additional research is needed to determine the patient benefits and cost-effectiveness of providing concurrent opioid use disorder medication and harm reduction services within primary care practices, including research using real-world data. Studies are needed to identify (1) effects other than drug-related deaths and service use, (2) the patient populations that benefit most from harm reduction services and other recovery supports, (3) the most cost-effective treatment models in different types of healthcare settings, and (4) cost-effectiveness in the absence of the X waiver.
For policy makers: Providing harm reduction services alongside medication treatment is cost effective compared to treatment as usual (i.e., referral to addiction treatment and harm reduction services), costing about $34,000 for each life year gained, per person, compared to treatment as usual. Providing buprenorphine without harm reduction services was more expensive and less effective. Though provision of buprenorphine and harm reduction kits within primary care is associated with increased costs to healthcare systems, it was the most cost-effective option in the long run, improved patient outcomes, decreased drug-related deaths, and increased life expectancy. Thus, providing medication treatment and harm reduction in primary care practices is a potential cost-effective option for enhancing medication treatment and reducing opioid-related deaths. Additional funding may help identify cost-effectiveness in the absence of the X waiver and other services that improve patient outcomes and help expand access to harm reduction services.
Medication treatments for opioid use disorder, like buprenorphine are often lifesaving, help support treatment and recovery, and reduce death and disability. However, some patients continue to inject illicit opioids during buprenorphine treatment, and injection opioid use comes with its own set of health risks that demand attention.
Harm reduction services are intended to reduce harms associated with risky health behaviors, like injection drug use. Harm reduction approaches include strategies like distribution of the opioid overdose reversal drug (naloxone) and sterile injection equipment (e.g., needles, wound care supplies, fentanyl test strips) to people who need them. These services are shown to be cost effective on their own, help lower risk of injection-related harms, and improve patient outcomes (e.g., reduced rates of infection and infectious diseases, reduced substance use, reduced injection drug use, prevention of fatal overdose).
Though an increasing number of patients are receiving buprenorphine treatment for opioid use disorder through primary care practices, harm reduction tools are not commonly provided alongside buprenorphine in these healthcare settings. Providing patients with both medication treatment and harm reduction services in one location might help to better address the opioid epidemic, by concurrently addressing opioid-related deaths and injection-related harms like infection to improve patient outcomes. However, it is unclear if the cost of integrating these services into primary care outweighs their beneficial effects on patient outcomes.
Effectiveness studies help determine the benefits of various treatments and cost-effectiveness studies help determine which treatments are best when considering both the benefits of the treatment and any investments and savings associated with providing them. Together, this information can inform policies regarding the most optimal types of treatment delivery settings and models that should be paid for and delivered. The current study examined long-term patient outcomes, healthcare costs, and the cost-effectiveness of integrating onsite buprenorphine treatment and harm reduction services into primary care models for the treatment of injection opioid use.
HOW WAS THIS STUDY CONDUCTED?
The authors conducted a model-based analysis of 2.25 million simulated people representative of the U.S. population that inject opioids to assess the effects of various primary care treatment strategies on long-term patient outcomes (i.e., drug-related deaths and healthcare events) and healthcare costs over the entire lifetime of the simulated study sample. Cost-effectiveness of each treatment was also evaluated.
Values entered into the model were based on data from clinical trials and observational studies in the scientific literature. The researchers evaluated three treatment strategies, which included primary care services plus:
1) Outside referral to outpatient buprenorphine treatment (i.e., treatment as usual)
2) Onsite buprenorphine treatment and outside referral to community-based harm reduction services (i.e., onsite buprenorphine treatment)
3) Onsite buprenorphine treatment and onsite provision of harm reduction kits at every office-based primary care visit (i.e., onsite buprenorphine treatment + harm reduction)
Harm reduction kits were assumed to include 10 sterile syringes with injection preparation equipment, a safer smoking kit, skin hygiene supplies, and wound care supplies. The figure below shows the three possible treatment strategies and the paths a simulated patient can take within each strategy. When offered or referred to services, patients could either accept buprenorphine treatment or refuse buprenorphine treatment and leave care.
The researchers evaluated the following long-term patient outcomes:
1) Life expectancy (years)
2) Deaths due to overdose, severe skin or soft tissue infection, and infective endocarditis (% or number per 10,000 people)
3) Number of lifetime hospitalizations per 100,000 people
4) Number of lifetime non-fatal skin and soft-tissue infections per 100,000 people
5) Average lifetime medical costs per person (see below for the costs considered)
To assess cost-effectiveness, the authors calculated the additional cost per person of implementing each treatment strategy and the life years gained (the additional number of years that a person lives as a result of receiving a treatment, with higher values indicating better outcomes) for each treatment modality. Costs included:
1) Background costs of being alive (i.e. age and sex stratified costs of being alive as estimated by the Medical Expenditure Panel Survey)
2) Injection drug use
3) Fatal and non-fatal overdose, without hospitalization
4) Untreated heart (endocarditis), skin, and soft-tissue infections
5) Hospitalization for overdose, and endocarditis, skin, and soft-tissue infections
6) Inpatient and outpatient service costs, including opioid use disorder medication treatment.
Cost effectiveness of each treatment was examined as the cost of treatment for each life year gained, relative to the next less expensive treatment. The researchers also evaluated the impact of providing buprenorphine and harm reduction kits on primary care practice budgets over a 5-year period. Cost savings in healthcare, criminal justice, and other systems, as a result of each treatment were not considered in analyses.
The researchers took sex, age, and injection behaviors into consideration in their simulated models. The models assumed that patients:
1) Were not receiving opioid use disorder medication treatment and did not have a history of overdose or infection at the start of the study
2) Who were hospitalized and not receiving medication treatment at that time would undergo medically supervised detoxification and would not receive medication treatment
3) Who were hospitalized and receiving medication treatment at that time would continue medication when discharged
4) Who received treatment as usual, or onsite buprenorphine treatment without onsite harm reduction services, received harm reduction kits through the community
5) Who received onsite buprenorphine and harm reduction kits also received naloxone during their first primary care visit
6) Who engaged in higher frequency injection drug use incurred more healthcare costs
At the start of the study, the simulated sample was primarily made up of men (70%) in their 40’s. Half of the sample engaged in high frequency injection opioid use, 10% engaged in low-frequency use, and 40% did not engage in injection use at study start. The majority of the sample engaged in unsterile injection opioid use (66%) and about one-third regularly shared injection equipment (35%).
WHAT DID THIS STUDY FIND?
Onsite buprenorphine with and without harm reduction services was associated with fewer deaths than treatment as usual.
Compared to treatment as usual, onsite buprenorphine with and without onsite harm reduction services extended estimated life expectancy by about 2.7 years and resulted in a 33% decrease in estimated overdose- and infection-related deaths. There were 160 fewer overdose deaths per 10,000 people, 3.5% fewer deaths due to skin and soft tissue infections and 2.5% fewer deaths due to infective endocarditis in absolute terms (a 61% and 7% improvement over treatment as usual, respectively).
Figures 2.1 and 2.2 above depict the number of overdose deaths per 10,000 people (left) and the estimated percentage of deaths due to infection (right), for each treatment strategy.
Buprenorphine alone was associated with more lifetime hospitalizations, but combined buprenorphine and harm-reduction was associated with fewer infections.
Because buprenorphine increased life expectancy, which meant more time and opportunity for people to continue using illicit substances and encounter adverse events requiring hospitalizations, a larger number of hospitalizations were estimated to occur with onsite buprenorphine alone and combined with harm reduction services, relative to treatment as usual. Non-fatal skin and soft-tissue infections were also more prevalent with onsite buprenorphine than treatment as usual. However, combined onsite buprenorphine and harm-reduction produced the fewest skin and soft-tissue infections.
Figure 3 shows the number of hospitalizations and non-fatal infections per 10,000 people, for each treatment strategy.
Onsite buprenorphine plus harm reduction was the most cost-effective strategy.
Compared to treatment as usual, lifetime medical costs per person were higher when patients received onsite buprenorphine alone or in combination with harm reduction, increasing by about 69% and 74%, respectively. While costs associated with hospitalization decreased, outpatient costs increased.
When the authors considered healthcare cost savings in the context of life years (i.e., cost effectiveness), only onsite buprenorphine plus harm reduction emerged as cost effective (i.e., costs $34,400 for each life year gained, per person, compared to treatment as usual). Integrating onsite buprenorphine treatment and harm reduction services was estimated to cost a primary care practice about $13,000 over a 5-year period.
Figure 4 depicts total medical costs accrued during each person’s lifetime, as well as lifetime hospitalization costs for overdose/infection and lifetime outpatient costs per person, for each treatment strategy.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better identify cost-effective methods for enhancing standard treatments for opioid use disorder that improve patient outcomes. This study found that the provision of buprenorphine alone or in combination with harm reduction kits is associated with lower rates of drug-related deaths (i.e., due to overdose, skin and soft tissue infection, and infective endocarditis) and a longer life expectancy (2.7 life years gained per person), compared to treatment as usual (i.e., referral to outpatient addiction treatment). Because increased life expectancy resulted in more time available for a person to experience drug-related harms and engage in the use of healthcare services, buprenorphine with or without harm reduction resulted in more hospitalizations than treatment as usual. Increased non-fatal skin and soft-tissue infections were also more prevalent with onsite buprenorphine treatment, but only when it was provided without onsite harm reduction services. Thus, providing harm-reduction services alongside buprenorphine in primary care settings might help increase patients’ use of sterile injection equipment and, in turn, help reduce their risk of infection-related health problems.
Though lifetime medical costs generally increased when implementing buprenorphine with or without harm reduction, these increased costs were largely driven by the cost of outpatient treatment, as opposed to drug-related harms and critical-care events. Thus, integration of addiction treatment into primary care services might increase the use of non-emergency healthcare services (e.g., regular primary care visits), which is consistent with previous research. Again, increased life expectancy with buprenorphine meant that patients had greater opportunity to engage in the healthcare system, resulting in greater healthcare costs. Despite this seeming increase in overall costs, the reduced cost of acute medical emergencies and hospitalizations might help to offset outpatient costs within healthcare systems. Increased outpatient service use is beneficial, as patients will have increased opportunity to engage in buprenorphine treatment, as well as address other chronic illnesses and injection-related harms during primary care visits. This would help avoid serious complications from infections related to injection opioid use that might otherwise result in acute hospitalization or mortality.
Interestingly, only the combined onsite provision of buprenorphine and harm reduction was deemed cost effective. The onsite provision of buprenorphine treatment without harm reduction services proved to be more expensive and less effective in terms of life years gained. Combined onsite buprenorphine and harm reduction services improved patient outcomes, decreased drug-related deaths, and increased life expectancy, compared to treatment as usual. It may be that buprenorphine alone is not enough to offset the cost of injection-related harms (e.g., infections & related health-care use), and providing harm-reduction kits alongside buprenorphine in primary care can help save on healthcare costs in the long run, by preventing harms associated with using unsterile injection equipment. Indeed, other research using computer simulations has shown that combining harm reduction with other services, like recovery support services, has the greatest benefit (e.g., reduces patient harm like overdose) in the long-term. Onsite harm reduction kits are not provided as the standard of care in primary care settings. Integrating these kits into primary care settings might enhance treatment engagement and/or provide useful tools for reducing injection-related risks during times of active opioid use. Importantly, the benefits of harm reduction kits were seen even though the researchers’ simulated model assumed that a fixed amount of safe injection equipment was included in the kits that would only last about 1 week for people engaging in frequent injection drug use. This highlights the potential benefits of convenient access to harm-reduction kits for reducing injection-related harms, health complications, and lengthy hospital stays.
Importantly, this study evaluated costs from a healthcare perspective and compared onsite buprenorphine and harm reduction services relative to a buprenorphine treatment referral. Prior research looking at patient and healthcare system costs have found buprenorphine to be cost effective on its own, without harm reduction, when compared to no treatment. This study extends this area of research by suggesting that providing buprenorphine plus add-on harm reduction services in primary care might be the most cost-effective treatment model from a healthcare perspective. Though offering combined buprenorphine and harm reduction services in primary care may cost practices an additional $13,000 every five years, these costs might be offset by the savings in broader healthcare system costs, with fewer patients needing lengthy hospital stays to address complications (e.g., infection). The costs estimated in this study also included X-waiver training, which used to be required in order for providers to prescribe buprenorphine (no longer needed as of June 2023), meaning that this cost is likely overestimated. Additional research is needed to evaluate cost-effective treatment models in the absence of X waivers, given that associated costs no longer apply.
These analyses and models were simulated and based on available data. Additionally, race/ethnicity, incarceration, treatment retention, and other patient-oriented outcomes (e.g., quality of life) were not factored into the model. Outcomes are likely close-to but not an exact reflection of actual costs accrued by individuals and longitudinal studies in diverse populations are needed to confirm these findings.
Other medication treatments, such as extended-release buprenorphine (i.e., Sublocade) and extended -release naltrexone (i.e., Vivitrol) were not assessed in this study and additional research is needed to determine their effects and cost-effectiveness when combined with harm reduction services.
Patients receiving treatment as usual, or onsite buprenorphine treatment without onsite harm reduction services, were assumed to have received harm reduction kits through the community. Given that not all patients are aware of harm reduction services, and not all who receive harm reduction referrals actually pursue them, this might have underestimated the beneficial effects of providing combined onsite buprenorphine and harm reduction services in primary care.
BOTTOM LINE
Studies like this help us better identify the most effective and financially sustainable treatment models for opioid use disorder, which can inform policies and reveal service models that are worth pursuing. This study found that, compared to treatment as usual (i.e., outpatient referral to buprenorphine treatment by a primary care physician), the provision of buprenorphine and harm reduction kits in primary care settings improved patient outcomes, decreased drug-related deaths, increased life expectancy, and was more cost effective than providing onsite buprenorphine without harm reduction kits.
For individuals and families seeking recovery: Individuals who are receiving opioid use disorder medication treatment might benefit from add-on services like harm reduction, as they could improve patient outcomes, reduce the risk of drug-related death, and increase a person’s life expectancy. Harm reduction services are not typically offered in primary care treatment settings, but they are often available through the community. Interested individuals can find harm reduction services near them through the National Harm Reduction Coalition.
For treatment professionals and treatment systems: Healthcare systems might consider providing harm reduction kits with opioid use disorder medication treatment, as this seems to be a cost-effective option that can help prevent drug-related deaths and complications (e.g., overdose, infection), and increase patients’ life expectancy. Since providing medication and harm reduction kits in primary care practices is more cost effective and results in better outcomes than referrals to offsite harm reduction services, offering these services within primary care practices is ideal when possible.
For scientists: Additional research is needed to determine the patient benefits and cost-effectiveness of providing concurrent opioid use disorder medication and harm reduction services within primary care practices, including research using real-world data. Studies are needed to identify (1) effects other than drug-related deaths and service use, (2) the patient populations that benefit most from harm reduction services and other recovery supports, (3) the most cost-effective treatment models in different types of healthcare settings, and (4) cost-effectiveness in the absence of the X waiver.
For policy makers: Providing harm reduction services alongside medication treatment is cost effective compared to treatment as usual (i.e., referral to addiction treatment and harm reduction services), costing about $34,000 for each life year gained, per person, compared to treatment as usual. Providing buprenorphine without harm reduction services was more expensive and less effective. Though provision of buprenorphine and harm reduction kits within primary care is associated with increased costs to healthcare systems, it was the most cost-effective option in the long run, improved patient outcomes, decreased drug-related deaths, and increased life expectancy. Thus, providing medication treatment and harm reduction in primary care practices is a potential cost-effective option for enhancing medication treatment and reducing opioid-related deaths. Additional funding may help identify cost-effectiveness in the absence of the X waiver and other services that improve patient outcomes and help expand access to harm reduction services.