Factors associated with hospitals’ adoption of harm reduction strategies
Hospitals are uniquely positioned to provide harm reduction services. Understanding the factors associated with their implementation can inform strategies to help expand them to other hospitals and health care settings. This study assessed what factors are associated with hospital adoption of harm reduction services and trends of adoption across time.
There are significant and numerous barriers to opioid use disorder treatment and recovery access, with only about 10% of people receiving specialty care. Harm reduction services have been shown to reduce criminal activity, overdose deaths, and the spread of infectious diseases. Harm reduction services, however, are difficult or impossible to access for the majority of US residents. Their limited scope is explained in part by concerns among policy makers and community members that they convey implicit approval of drug use that is federally illegal and associated with potential safety risks.
Hospitals can help fill this gap by offering these services. Because most people who are experiencing an overdose or health problems from injecting drugs go to the hospital to receive care, hospitals are well positioned to offer such services. Connecting people with opioid and other substance use disorders to harm reduction services during a hospital visit can also help retain people in medical care and provide an avenue to enter treatment.
Implementing harm reduction services within hospital settings has been shown to be well-accepted by patients and improve outcomes. This study examined factors associated with the provision of hospital-based harm reduction services to help inform policies and procedures for other hospitals who wish to implement harm reduction services, thereby expanding access and potentially improving public health.
HOW WAS THIS STUDY CONDUCTED?
This study assessed what factors are associated with hospital adoption of harm reduction and risk education strategies (e.g., medication take-back events, stigma reduction workshops, naloxone distribution, syringe exchange programs, etc.) and trends of adoption across time among nonprofit general hospitals across the US.
The researchers used data from a random, 20% sample of nonprofit general hospitals within each state and collected the most recent hospital community health needs assessments, required by the Affordable Care Act, and implementation strategies, which took place during the years 2019-2021. This data was then merged with several other data sources providing information on hospital, county, and state characteristics.
The researchers were interested in examining whether a number of these characteristics were associated with hospital adoption of harm reduction and risk education strategies. These included whether the hospital prioritized substance use among the top 3 needs on the needs assessment, whether the hospital wrote the needs assessment in collaboration with community partners, and whether the hospital adopted at least 3 other strategies for addressing substance use disorders, beyond risk education and harm reduction. Other hospital characteristics that were examined to assess the association with adoption of services included bed size, health system membership (i.e., two or more hospitals managed by a central organization), teaching hospital status, and the capacity for hospitals to comprehensively treat patients with substance use disorders.
County characteristics that were examined to assess the association with hospital adoption of harm reduction and risk education services included the percent of households with income well below the designated federal poverty level, the percent who are uninsured by county, county overdose rates, and rural or urban location based on the availability of other treatment options in the vicinity of the hospital. The only state characteristic was whether the state in which the hospitals were located expanded Medicaid prior to 2018.
The primary outcome was whether hospitals specifically included “harm reduction” or “risk education” programs within their implementation strategies. The researchers also assessed if hospitals’ implementation strategies included 6 other types of approaches for addressing substance use disorders to determine if adopting other programs beyond harm reduction was associated with hospital adoption of services: (1) substance use disorder treatment, (2) emergency department services, (3) prescriber guidelines, (4) programs to address the social determinants of health, (5) policy advocacy, and (6) community coalition building.
In total, 489 nonprofits hospitals were included in the study. The research team calculated the mean number of hospitals that implemented harm reduction and risk education strategies during the 2019-2021 needs assessments. To assess trends across time, they also calculated the mean number of hospitals that implemented strategies during the previous needs assessments that occurred between 2015 and 2018.
Then, the researchers analyzed associations between the hospital, county, and state characteristics and hospital implementation using 2 different statistical models. In the first model, the researchers simply examined the associations between the predictor variables (i.e., hospital, county, and state characteristics) and the outcome variable (i.e., whether hospitals included programs in their implementation strategies), without accounting for any other variables that may affect the association (i.e., “unadjusted” models). In the second model, the researchers accounted for the hospitals being “nested” within states, since hospitals within a given state likely share many environmental factors, as well as hospital, county, and state characteristics (“adjusted” models).
Of the 489 hospitals included in the study, the majority were system hospitals (75.6%) and only 9.4% were teaching hospitals. Most had 50-199 beds (33.9%) or 1-49 (28.8%). For county characteristics, the average percent of residents in surrounding counties who lived below the federal poverty line was 12.6%, the average percent of residents who were uninsured was 8.3%, the average county overdose rate was 21.9 deaths per 100,000 residents, and 25.7% of states were located in rural counties. The majority of hospitals (69.1%) were located in states that expanded Medicaid.
WHAT DID THIS STUDY FIND?
Hospitals implementing harm reduction and risk education strategies have grown over time.
During the most recent needs assessments from 2019 to 2021, 44.8% of nonprofit hospitals in the study reported implementing harm reduction or risk education programs, while 34.1% of hospitals reported doing so during the previous 2015-2018 needs assessments.
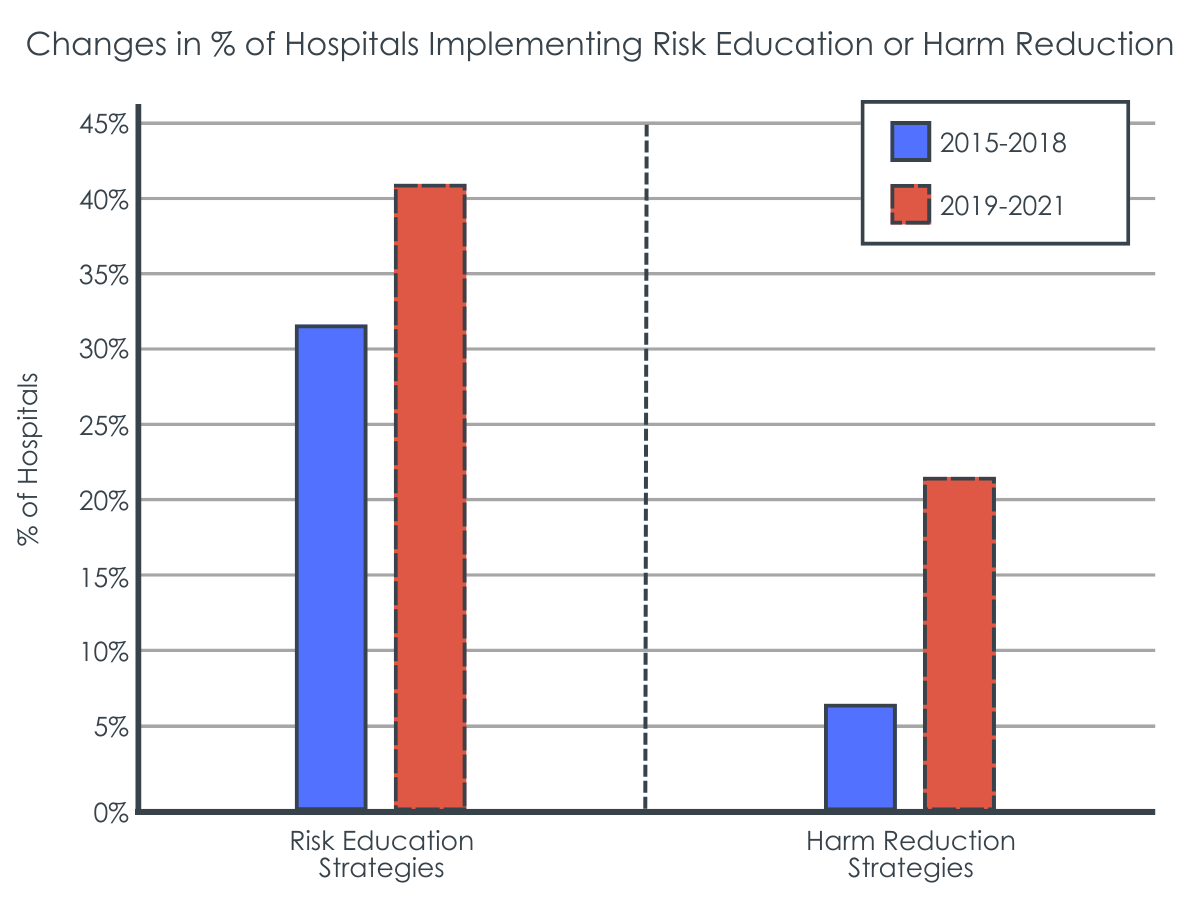
When broken down by type of strategy, 41.2% of hospitals reported implementing risk education strategies during the 2019-2021 assessments, while 31.7% did during the 2015-2018 assessments. Likewise, for harm reduction strategies, 21.8% of hospitals reported implementing such strategies during the more recent 2019-2021 assessments, compared to just 6.3% that did during the 2015–2018 assessments.
Factors associated with likelihood of offering harm reduction or risk education strategies.
Factors that were associated with the highest increases in the likelihood of hospitals implementing harm reduction or risk education strategies in the unadjusted model analyses included adopting 3 or more other programs that address substance use disorders, with an increased 7-fold likelihood, and prioritizing substance use disorders among the top three needs in the needs assessment, with an increased 3-fold likelihood. Other factors associated with an increased likelihood of implementation included the county overdose rate, writing the needs assessment in collaboration with a community organization, and being in a state that expanded Medicaid under the Affordable Care Act (ACA).
There were also several factors that were associated with a decreased likelihood of harm reduction services in the unadjusted models. As the percentage of the surrounding county population living below the federal poverty line and the percentage of those without health insurance increased, the likelihood of hospital implementation decreased.
In the second set of analyses where researchers adjusted for the effects of other variables, 3 factors were associated with the chances of hospital implementation. Previously adopting 3 or more other programs that address substance use disorders was associated with a 10-fold increased likelihood of harm reduction service provision. Writing the needs assessment in collaboration with a community organization and prioritizing substance use disorders among the top 3 needs in the needs assessment also increased the likelihood of implementation, with increases of 2- to 2.5-fold.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study assessed characteristics associated with hospitals’ implementation of harm reduction and risk education strategies. Results showed that hospitals that have already adopted at least 3 other programs for addressing substance use disorders, that wrote their needs assessments in collaboration with a community-based organization, and prioritized substance use disorders among the top 3 needs in the needs assessments increased the likelihood of the hospital implementing harm reduction and risk education strategies
It is perhaps not surprising that hospitals that have already adopted other programs for addressing substance use disorders were more likely to implement harm reduction and risk education strategies. This is likely reflective of the hospitals’ existing substance use disorder infrastructure. This infrastructure may be a result of the hospitals’ attitudes and beliefs that substance use disorders should be addressed comprehensively within medical settings, along with other complementary services, as well as having the necessary resources to be able to do so. Comprehensive strategies to addressing substance use disorders in the hospital has been shown to improve overall health, treatment outcomes, and rates of entering addiction treatment.
Hospitals that wrote their needs assessments in collaboration with a community-based organization being more likely to implement harm reduction and risk education strategies underscores the importance of connecting with the community, especially in this context where harm reduction approaches are inconsistent with traditional medical care. The goal of harm reduction services is to reduce the health risks associated with substance use, such as overdose and disease transmission, while the goal of medical care has traditionally focused on abstinence. As a result, harm reduction services are often offered by community-based organizations, rather than medical facilities. Hospitals who partner with community-based organizations that are typically populated with people with lived experience of addiction may therefore gain greater nuanced and specific knowledge that can increase their service provision sensitivity and enhance capacity for implementing services that are likely to make a difference.
Lastly, hospitals who prioritized substance use disorders among the top 3 needs in the needs assessmentsweremore likely to implement harm reduction and risk education strategies. This may indicate a greater magnitude of the problem in the community. Communities with more people who have a substance use disorder appear to be more likely to build on traditional abstinence-based approaches than those who have less people with substance use disorder. This may be because counties with higher rates of drug overdoses are also more likely to be densely populated cities, where people and policy makers are often more progressive and accepting of non-traditional approaches. For example, conservative states have been historically slower to adopt policies that support naloxone access, which can reverse overdose and prevent death. This suggests that having higher rates of substance use disorder or drug overdoses does not necessarily causehospitals to be more likely to implement harm reduction and risk education, but rather that there are likely to be other factors that play a role in the association.
The hospitals included in the study were nonprofit hospitals in the US. Accordingly, the results may not generalize to public and for-profit hospitals. Results are also likely to differ in other countries, given varying levels of public and policy support for harm reduction services between countries.
There are no standard requirements for what hospitals need to include in their implementation strategies. This means that it is possible for hospitals to have implemented harm reduction or risk education strategies, but not have documented it, which could have led to under-reporting of strategies implemented.
Hospitals also may not have actually implemented strategies that they planned to in the implementation plans. As such, the strategies would have been counted in the study as having been implemented, when they were not. This could have led to over-reporting of strategies implemented.
Because the variables were categorical (i.e., present or absent), details of the specific programs offered, including quality measures related to implementation, are not available.
Broader harm reduction approaches were not examined in the study, such as making treatment for substance use disorders more accessible and patient centered. Including these broader approaches may have influenced the characteristics that were associated with hospital implementation or harm reduction and risk education strategies.
BOTTOM LINE
Adopting other programs for addressing substance use disorders, collaborating with a community-based organization, and prioritizing substance use disorders are associated with greater implementation of harm reduction and risk education strategies among nonprofit hospitals in the US. Although the study cannot conclude that these factors cause greater implementation, they can be considered important markers. This highlights the importance of a hospital focus on addressing highly prevalent and clinically impactful substance use disorders, connecting with the community to help inform the hospital of the real-world needs of affected individuals and families in those communities, and making substance use disorders a priority for increasing hospitals’ likelihood of adopting and implementing harm reduction and risk education strategies.
For individuals and families seeking recovery: When individuals with substance use disorder go to the hospital to receive care for health problems related to substance use or an overdose, it may be an opportunity for them to engage with harm reduction and risk education services, as well as enter treatment. Individuals who accept these services may be less likely to leave the hospital before their treatment is completed and have a greater chance of improved outcomes.
For treatment professionals and treatment systems: The study’s results point to three factors associated with hospitals’ implementation of harm reduction and risk education services: existing infrastructure for addressing substance use disorders, making substance use disorders a priority, and connecting with the community. These may reflect hospital administrators’ general attitudes towards, and prioritization of substance use and community-based public health. Accordingly, shifting attitudes and beliefs may lead to greater implementation.
For scientists: Because the current study examined nonprofit hospitals in the US only, future research that examines public and for-profit hospitals, as well as hospitals in other countries, would provide more information on the factors that are associated with greater implementation in these other contexts. Additionally, the researchers coded documents of the hospitals’ implementation plans. This risks under- and over-estimates of the strategies implemented since programs that were actually implemented but not included in the documents, and programs that were planned but not actually implemented, would not have been captured. Future research that uses other methods less prone to these risks may provide more accurate estimates, such as tracking actual implementation over time. Additional research that assesses the details of the types of programs implemented, instead of only being present or absent, including quality in implementation, would also shed more light on how hospitals are implementing harm reduction and risk education services. Finally, research that examines whether the harm reduction services were implemented before or after the other factors examined would help shed light on causality.
For policy makers: Results from this study demonstrated that hospitals that adopt other programs for addressing substance use disorders, collaborate with a community-based organization, and prioritize substance use disorders also have a greater likelihood of implementation of harm reduction and risk education strategies. In other words, making substance use disorder a top priority focus within hospitals may well result also in adoption of harm reduction and risk reduction strategies as part of this explicit focus. Accordingly, policy makers may help expand implementation to other hospitals by supporting policies that help promote a prioritized substance use health care focus. In addition, funding for further research to examine the factors associated with hospitals’ implementation in other contexts and that uses more comprehensive methods will provide a greater understanding of how to better support hospitals.
There are significant and numerous barriers to opioid use disorder treatment and recovery access, with only about 10% of people receiving specialty care. Harm reduction services have been shown to reduce criminal activity, overdose deaths, and the spread of infectious diseases. Harm reduction services, however, are difficult or impossible to access for the majority of US residents. Their limited scope is explained in part by concerns among policy makers and community members that they convey implicit approval of drug use that is federally illegal and associated with potential safety risks.
Hospitals can help fill this gap by offering these services. Because most people who are experiencing an overdose or health problems from injecting drugs go to the hospital to receive care, hospitals are well positioned to offer such services. Connecting people with opioid and other substance use disorders to harm reduction services during a hospital visit can also help retain people in medical care and provide an avenue to enter treatment.
Implementing harm reduction services within hospital settings has been shown to be well-accepted by patients and improve outcomes. This study examined factors associated with the provision of hospital-based harm reduction services to help inform policies and procedures for other hospitals who wish to implement harm reduction services, thereby expanding access and potentially improving public health.
HOW WAS THIS STUDY CONDUCTED?
This study assessed what factors are associated with hospital adoption of harm reduction and risk education strategies (e.g., medication take-back events, stigma reduction workshops, naloxone distribution, syringe exchange programs, etc.) and trends of adoption across time among nonprofit general hospitals across the US.
The researchers used data from a random, 20% sample of nonprofit general hospitals within each state and collected the most recent hospital community health needs assessments, required by the Affordable Care Act, and implementation strategies, which took place during the years 2019-2021. This data was then merged with several other data sources providing information on hospital, county, and state characteristics.
The researchers were interested in examining whether a number of these characteristics were associated with hospital adoption of harm reduction and risk education strategies. These included whether the hospital prioritized substance use among the top 3 needs on the needs assessment, whether the hospital wrote the needs assessment in collaboration with community partners, and whether the hospital adopted at least 3 other strategies for addressing substance use disorders, beyond risk education and harm reduction. Other hospital characteristics that were examined to assess the association with adoption of services included bed size, health system membership (i.e., two or more hospitals managed by a central organization), teaching hospital status, and the capacity for hospitals to comprehensively treat patients with substance use disorders.
County characteristics that were examined to assess the association with hospital adoption of harm reduction and risk education services included the percent of households with income well below the designated federal poverty level, the percent who are uninsured by county, county overdose rates, and rural or urban location based on the availability of other treatment options in the vicinity of the hospital. The only state characteristic was whether the state in which the hospitals were located expanded Medicaid prior to 2018.
The primary outcome was whether hospitals specifically included “harm reduction” or “risk education” programs within their implementation strategies. The researchers also assessed if hospitals’ implementation strategies included 6 other types of approaches for addressing substance use disorders to determine if adopting other programs beyond harm reduction was associated with hospital adoption of services: (1) substance use disorder treatment, (2) emergency department services, (3) prescriber guidelines, (4) programs to address the social determinants of health, (5) policy advocacy, and (6) community coalition building.
In total, 489 nonprofits hospitals were included in the study. The research team calculated the mean number of hospitals that implemented harm reduction and risk education strategies during the 2019-2021 needs assessments. To assess trends across time, they also calculated the mean number of hospitals that implemented strategies during the previous needs assessments that occurred between 2015 and 2018.
Then, the researchers analyzed associations between the hospital, county, and state characteristics and hospital implementation using 2 different statistical models. In the first model, the researchers simply examined the associations between the predictor variables (i.e., hospital, county, and state characteristics) and the outcome variable (i.e., whether hospitals included programs in their implementation strategies), without accounting for any other variables that may affect the association (i.e., “unadjusted” models). In the second model, the researchers accounted for the hospitals being “nested” within states, since hospitals within a given state likely share many environmental factors, as well as hospital, county, and state characteristics (“adjusted” models).
Of the 489 hospitals included in the study, the majority were system hospitals (75.6%) and only 9.4% were teaching hospitals. Most had 50-199 beds (33.9%) or 1-49 (28.8%). For county characteristics, the average percent of residents in surrounding counties who lived below the federal poverty line was 12.6%, the average percent of residents who were uninsured was 8.3%, the average county overdose rate was 21.9 deaths per 100,000 residents, and 25.7% of states were located in rural counties. The majority of hospitals (69.1%) were located in states that expanded Medicaid.
WHAT DID THIS STUDY FIND?
Hospitals implementing harm reduction and risk education strategies have grown over time.
During the most recent needs assessments from 2019 to 2021, 44.8% of nonprofit hospitals in the study reported implementing harm reduction or risk education programs, while 34.1% of hospitals reported doing so during the previous 2015-2018 needs assessments.
When broken down by type of strategy, 41.2% of hospitals reported implementing risk education strategies during the 2019-2021 assessments, while 31.7% did during the 2015-2018 assessments. Likewise, for harm reduction strategies, 21.8% of hospitals reported implementing such strategies during the more recent 2019-2021 assessments, compared to just 6.3% that did during the 2015–2018 assessments.
Factors associated with likelihood of offering harm reduction or risk education strategies.
Factors that were associated with the highest increases in the likelihood of hospitals implementing harm reduction or risk education strategies in the unadjusted model analyses included adopting 3 or more other programs that address substance use disorders, with an increased 7-fold likelihood, and prioritizing substance use disorders among the top three needs in the needs assessment, with an increased 3-fold likelihood. Other factors associated with an increased likelihood of implementation included the county overdose rate, writing the needs assessment in collaboration with a community organization, and being in a state that expanded Medicaid under the Affordable Care Act (ACA).
There were also several factors that were associated with a decreased likelihood of harm reduction services in the unadjusted models. As the percentage of the surrounding county population living below the federal poverty line and the percentage of those without health insurance increased, the likelihood of hospital implementation decreased.
In the second set of analyses where researchers adjusted for the effects of other variables, 3 factors were associated with the chances of hospital implementation. Previously adopting 3 or more other programs that address substance use disorders was associated with a 10-fold increased likelihood of harm reduction service provision. Writing the needs assessment in collaboration with a community organization and prioritizing substance use disorders among the top 3 needs in the needs assessment also increased the likelihood of implementation, with increases of 2- to 2.5-fold.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study assessed characteristics associated with hospitals’ implementation of harm reduction and risk education strategies. Results showed that hospitals that have already adopted at least 3 other programs for addressing substance use disorders, that wrote their needs assessments in collaboration with a community-based organization, and prioritized substance use disorders among the top 3 needs in the needs assessments increased the likelihood of the hospital implementing harm reduction and risk education strategies
It is perhaps not surprising that hospitals that have already adopted other programs for addressing substance use disorders were more likely to implement harm reduction and risk education strategies. This is likely reflective of the hospitals’ existing substance use disorder infrastructure. This infrastructure may be a result of the hospitals’ attitudes and beliefs that substance use disorders should be addressed comprehensively within medical settings, along with other complementary services, as well as having the necessary resources to be able to do so. Comprehensive strategies to addressing substance use disorders in the hospital has been shown to improve overall health, treatment outcomes, and rates of entering addiction treatment.
Hospitals that wrote their needs assessments in collaboration with a community-based organization being more likely to implement harm reduction and risk education strategies underscores the importance of connecting with the community, especially in this context where harm reduction approaches are inconsistent with traditional medical care. The goal of harm reduction services is to reduce the health risks associated with substance use, such as overdose and disease transmission, while the goal of medical care has traditionally focused on abstinence. As a result, harm reduction services are often offered by community-based organizations, rather than medical facilities. Hospitals who partner with community-based organizations that are typically populated with people with lived experience of addiction may therefore gain greater nuanced and specific knowledge that can increase their service provision sensitivity and enhance capacity for implementing services that are likely to make a difference.
Lastly, hospitals who prioritized substance use disorders among the top 3 needs in the needs assessmentsweremore likely to implement harm reduction and risk education strategies. This may indicate a greater magnitude of the problem in the community. Communities with more people who have a substance use disorder appear to be more likely to build on traditional abstinence-based approaches than those who have less people with substance use disorder. This may be because counties with higher rates of drug overdoses are also more likely to be densely populated cities, where people and policy makers are often more progressive and accepting of non-traditional approaches. For example, conservative states have been historically slower to adopt policies that support naloxone access, which can reverse overdose and prevent death. This suggests that having higher rates of substance use disorder or drug overdoses does not necessarily causehospitals to be more likely to implement harm reduction and risk education, but rather that there are likely to be other factors that play a role in the association.
The hospitals included in the study were nonprofit hospitals in the US. Accordingly, the results may not generalize to public and for-profit hospitals. Results are also likely to differ in other countries, given varying levels of public and policy support for harm reduction services between countries.
There are no standard requirements for what hospitals need to include in their implementation strategies. This means that it is possible for hospitals to have implemented harm reduction or risk education strategies, but not have documented it, which could have led to under-reporting of strategies implemented.
Hospitals also may not have actually implemented strategies that they planned to in the implementation plans. As such, the strategies would have been counted in the study as having been implemented, when they were not. This could have led to over-reporting of strategies implemented.
Because the variables were categorical (i.e., present or absent), details of the specific programs offered, including quality measures related to implementation, are not available.
Broader harm reduction approaches were not examined in the study, such as making treatment for substance use disorders more accessible and patient centered. Including these broader approaches may have influenced the characteristics that were associated with hospital implementation or harm reduction and risk education strategies.
BOTTOM LINE
Adopting other programs for addressing substance use disorders, collaborating with a community-based organization, and prioritizing substance use disorders are associated with greater implementation of harm reduction and risk education strategies among nonprofit hospitals in the US. Although the study cannot conclude that these factors cause greater implementation, they can be considered important markers. This highlights the importance of a hospital focus on addressing highly prevalent and clinically impactful substance use disorders, connecting with the community to help inform the hospital of the real-world needs of affected individuals and families in those communities, and making substance use disorders a priority for increasing hospitals’ likelihood of adopting and implementing harm reduction and risk education strategies.
For individuals and families seeking recovery: When individuals with substance use disorder go to the hospital to receive care for health problems related to substance use or an overdose, it may be an opportunity for them to engage with harm reduction and risk education services, as well as enter treatment. Individuals who accept these services may be less likely to leave the hospital before their treatment is completed and have a greater chance of improved outcomes.
For treatment professionals and treatment systems: The study’s results point to three factors associated with hospitals’ implementation of harm reduction and risk education services: existing infrastructure for addressing substance use disorders, making substance use disorders a priority, and connecting with the community. These may reflect hospital administrators’ general attitudes towards, and prioritization of substance use and community-based public health. Accordingly, shifting attitudes and beliefs may lead to greater implementation.
For scientists: Because the current study examined nonprofit hospitals in the US only, future research that examines public and for-profit hospitals, as well as hospitals in other countries, would provide more information on the factors that are associated with greater implementation in these other contexts. Additionally, the researchers coded documents of the hospitals’ implementation plans. This risks under- and over-estimates of the strategies implemented since programs that were actually implemented but not included in the documents, and programs that were planned but not actually implemented, would not have been captured. Future research that uses other methods less prone to these risks may provide more accurate estimates, such as tracking actual implementation over time. Additional research that assesses the details of the types of programs implemented, instead of only being present or absent, including quality in implementation, would also shed more light on how hospitals are implementing harm reduction and risk education services. Finally, research that examines whether the harm reduction services were implemented before or after the other factors examined would help shed light on causality.
For policy makers: Results from this study demonstrated that hospitals that adopt other programs for addressing substance use disorders, collaborate with a community-based organization, and prioritize substance use disorders also have a greater likelihood of implementation of harm reduction and risk education strategies. In other words, making substance use disorder a top priority focus within hospitals may well result also in adoption of harm reduction and risk reduction strategies as part of this explicit focus. Accordingly, policy makers may help expand implementation to other hospitals by supporting policies that help promote a prioritized substance use health care focus. In addition, funding for further research to examine the factors associated with hospitals’ implementation in other contexts and that uses more comprehensive methods will provide a greater understanding of how to better support hospitals.
There are significant and numerous barriers to opioid use disorder treatment and recovery access, with only about 10% of people receiving specialty care. Harm reduction services have been shown to reduce criminal activity, overdose deaths, and the spread of infectious diseases. Harm reduction services, however, are difficult or impossible to access for the majority of US residents. Their limited scope is explained in part by concerns among policy makers and community members that they convey implicit approval of drug use that is federally illegal and associated with potential safety risks.
Hospitals can help fill this gap by offering these services. Because most people who are experiencing an overdose or health problems from injecting drugs go to the hospital to receive care, hospitals are well positioned to offer such services. Connecting people with opioid and other substance use disorders to harm reduction services during a hospital visit can also help retain people in medical care and provide an avenue to enter treatment.
Implementing harm reduction services within hospital settings has been shown to be well-accepted by patients and improve outcomes. This study examined factors associated with the provision of hospital-based harm reduction services to help inform policies and procedures for other hospitals who wish to implement harm reduction services, thereby expanding access and potentially improving public health.
HOW WAS THIS STUDY CONDUCTED?
This study assessed what factors are associated with hospital adoption of harm reduction and risk education strategies (e.g., medication take-back events, stigma reduction workshops, naloxone distribution, syringe exchange programs, etc.) and trends of adoption across time among nonprofit general hospitals across the US.
The researchers used data from a random, 20% sample of nonprofit general hospitals within each state and collected the most recent hospital community health needs assessments, required by the Affordable Care Act, and implementation strategies, which took place during the years 2019-2021. This data was then merged with several other data sources providing information on hospital, county, and state characteristics.
The researchers were interested in examining whether a number of these characteristics were associated with hospital adoption of harm reduction and risk education strategies. These included whether the hospital prioritized substance use among the top 3 needs on the needs assessment, whether the hospital wrote the needs assessment in collaboration with community partners, and whether the hospital adopted at least 3 other strategies for addressing substance use disorders, beyond risk education and harm reduction. Other hospital characteristics that were examined to assess the association with adoption of services included bed size, health system membership (i.e., two or more hospitals managed by a central organization), teaching hospital status, and the capacity for hospitals to comprehensively treat patients with substance use disorders.
County characteristics that were examined to assess the association with hospital adoption of harm reduction and risk education services included the percent of households with income well below the designated federal poverty level, the percent who are uninsured by county, county overdose rates, and rural or urban location based on the availability of other treatment options in the vicinity of the hospital. The only state characteristic was whether the state in which the hospitals were located expanded Medicaid prior to 2018.
The primary outcome was whether hospitals specifically included “harm reduction” or “risk education” programs within their implementation strategies. The researchers also assessed if hospitals’ implementation strategies included 6 other types of approaches for addressing substance use disorders to determine if adopting other programs beyond harm reduction was associated with hospital adoption of services: (1) substance use disorder treatment, (2) emergency department services, (3) prescriber guidelines, (4) programs to address the social determinants of health, (5) policy advocacy, and (6) community coalition building.
In total, 489 nonprofits hospitals were included in the study. The research team calculated the mean number of hospitals that implemented harm reduction and risk education strategies during the 2019-2021 needs assessments. To assess trends across time, they also calculated the mean number of hospitals that implemented strategies during the previous needs assessments that occurred between 2015 and 2018.
Then, the researchers analyzed associations between the hospital, county, and state characteristics and hospital implementation using 2 different statistical models. In the first model, the researchers simply examined the associations between the predictor variables (i.e., hospital, county, and state characteristics) and the outcome variable (i.e., whether hospitals included programs in their implementation strategies), without accounting for any other variables that may affect the association (i.e., “unadjusted” models). In the second model, the researchers accounted for the hospitals being “nested” within states, since hospitals within a given state likely share many environmental factors, as well as hospital, county, and state characteristics (“adjusted” models).
Of the 489 hospitals included in the study, the majority were system hospitals (75.6%) and only 9.4% were teaching hospitals. Most had 50-199 beds (33.9%) or 1-49 (28.8%). For county characteristics, the average percent of residents in surrounding counties who lived below the federal poverty line was 12.6%, the average percent of residents who were uninsured was 8.3%, the average county overdose rate was 21.9 deaths per 100,000 residents, and 25.7% of states were located in rural counties. The majority of hospitals (69.1%) were located in states that expanded Medicaid.
WHAT DID THIS STUDY FIND?
Hospitals implementing harm reduction and risk education strategies have grown over time.
During the most recent needs assessments from 2019 to 2021, 44.8% of nonprofit hospitals in the study reported implementing harm reduction or risk education programs, while 34.1% of hospitals reported doing so during the previous 2015-2018 needs assessments.
When broken down by type of strategy, 41.2% of hospitals reported implementing risk education strategies during the 2019-2021 assessments, while 31.7% did during the 2015-2018 assessments. Likewise, for harm reduction strategies, 21.8% of hospitals reported implementing such strategies during the more recent 2019-2021 assessments, compared to just 6.3% that did during the 2015–2018 assessments.
Factors associated with likelihood of offering harm reduction or risk education strategies.
Factors that were associated with the highest increases in the likelihood of hospitals implementing harm reduction or risk education strategies in the unadjusted model analyses included adopting 3 or more other programs that address substance use disorders, with an increased 7-fold likelihood, and prioritizing substance use disorders among the top three needs in the needs assessment, with an increased 3-fold likelihood. Other factors associated with an increased likelihood of implementation included the county overdose rate, writing the needs assessment in collaboration with a community organization, and being in a state that expanded Medicaid under the Affordable Care Act (ACA).
There were also several factors that were associated with a decreased likelihood of harm reduction services in the unadjusted models. As the percentage of the surrounding county population living below the federal poverty line and the percentage of those without health insurance increased, the likelihood of hospital implementation decreased.
In the second set of analyses where researchers adjusted for the effects of other variables, 3 factors were associated with the chances of hospital implementation. Previously adopting 3 or more other programs that address substance use disorders was associated with a 10-fold increased likelihood of harm reduction service provision. Writing the needs assessment in collaboration with a community organization and prioritizing substance use disorders among the top 3 needs in the needs assessment also increased the likelihood of implementation, with increases of 2- to 2.5-fold.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study assessed characteristics associated with hospitals’ implementation of harm reduction and risk education strategies. Results showed that hospitals that have already adopted at least 3 other programs for addressing substance use disorders, that wrote their needs assessments in collaboration with a community-based organization, and prioritized substance use disorders among the top 3 needs in the needs assessments increased the likelihood of the hospital implementing harm reduction and risk education strategies
It is perhaps not surprising that hospitals that have already adopted other programs for addressing substance use disorders were more likely to implement harm reduction and risk education strategies. This is likely reflective of the hospitals’ existing substance use disorder infrastructure. This infrastructure may be a result of the hospitals’ attitudes and beliefs that substance use disorders should be addressed comprehensively within medical settings, along with other complementary services, as well as having the necessary resources to be able to do so. Comprehensive strategies to addressing substance use disorders in the hospital has been shown to improve overall health, treatment outcomes, and rates of entering addiction treatment.
Hospitals that wrote their needs assessments in collaboration with a community-based organization being more likely to implement harm reduction and risk education strategies underscores the importance of connecting with the community, especially in this context where harm reduction approaches are inconsistent with traditional medical care. The goal of harm reduction services is to reduce the health risks associated with substance use, such as overdose and disease transmission, while the goal of medical care has traditionally focused on abstinence. As a result, harm reduction services are often offered by community-based organizations, rather than medical facilities. Hospitals who partner with community-based organizations that are typically populated with people with lived experience of addiction may therefore gain greater nuanced and specific knowledge that can increase their service provision sensitivity and enhance capacity for implementing services that are likely to make a difference.
Lastly, hospitals who prioritized substance use disorders among the top 3 needs in the needs assessmentsweremore likely to implement harm reduction and risk education strategies. This may indicate a greater magnitude of the problem in the community. Communities with more people who have a substance use disorder appear to be more likely to build on traditional abstinence-based approaches than those who have less people with substance use disorder. This may be because counties with higher rates of drug overdoses are also more likely to be densely populated cities, where people and policy makers are often more progressive and accepting of non-traditional approaches. For example, conservative states have been historically slower to adopt policies that support naloxone access, which can reverse overdose and prevent death. This suggests that having higher rates of substance use disorder or drug overdoses does not necessarily causehospitals to be more likely to implement harm reduction and risk education, but rather that there are likely to be other factors that play a role in the association.
The hospitals included in the study were nonprofit hospitals in the US. Accordingly, the results may not generalize to public and for-profit hospitals. Results are also likely to differ in other countries, given varying levels of public and policy support for harm reduction services between countries.
There are no standard requirements for what hospitals need to include in their implementation strategies. This means that it is possible for hospitals to have implemented harm reduction or risk education strategies, but not have documented it, which could have led to under-reporting of strategies implemented.
Hospitals also may not have actually implemented strategies that they planned to in the implementation plans. As such, the strategies would have been counted in the study as having been implemented, when they were not. This could have led to over-reporting of strategies implemented.
Because the variables were categorical (i.e., present or absent), details of the specific programs offered, including quality measures related to implementation, are not available.
Broader harm reduction approaches were not examined in the study, such as making treatment for substance use disorders more accessible and patient centered. Including these broader approaches may have influenced the characteristics that were associated with hospital implementation or harm reduction and risk education strategies.
BOTTOM LINE
Adopting other programs for addressing substance use disorders, collaborating with a community-based organization, and prioritizing substance use disorders are associated with greater implementation of harm reduction and risk education strategies among nonprofit hospitals in the US. Although the study cannot conclude that these factors cause greater implementation, they can be considered important markers. This highlights the importance of a hospital focus on addressing highly prevalent and clinically impactful substance use disorders, connecting with the community to help inform the hospital of the real-world needs of affected individuals and families in those communities, and making substance use disorders a priority for increasing hospitals’ likelihood of adopting and implementing harm reduction and risk education strategies.
For individuals and families seeking recovery: When individuals with substance use disorder go to the hospital to receive care for health problems related to substance use or an overdose, it may be an opportunity for them to engage with harm reduction and risk education services, as well as enter treatment. Individuals who accept these services may be less likely to leave the hospital before their treatment is completed and have a greater chance of improved outcomes.
For treatment professionals and treatment systems: The study’s results point to three factors associated with hospitals’ implementation of harm reduction and risk education services: existing infrastructure for addressing substance use disorders, making substance use disorders a priority, and connecting with the community. These may reflect hospital administrators’ general attitudes towards, and prioritization of substance use and community-based public health. Accordingly, shifting attitudes and beliefs may lead to greater implementation.
For scientists: Because the current study examined nonprofit hospitals in the US only, future research that examines public and for-profit hospitals, as well as hospitals in other countries, would provide more information on the factors that are associated with greater implementation in these other contexts. Additionally, the researchers coded documents of the hospitals’ implementation plans. This risks under- and over-estimates of the strategies implemented since programs that were actually implemented but not included in the documents, and programs that were planned but not actually implemented, would not have been captured. Future research that uses other methods less prone to these risks may provide more accurate estimates, such as tracking actual implementation over time. Additional research that assesses the details of the types of programs implemented, instead of only being present or absent, including quality in implementation, would also shed more light on how hospitals are implementing harm reduction and risk education services. Finally, research that examines whether the harm reduction services were implemented before or after the other factors examined would help shed light on causality.
For policy makers: Results from this study demonstrated that hospitals that adopt other programs for addressing substance use disorders, collaborate with a community-based organization, and prioritize substance use disorders also have a greater likelihood of implementation of harm reduction and risk education strategies. In other words, making substance use disorder a top priority focus within hospitals may well result also in adoption of harm reduction and risk reduction strategies as part of this explicit focus. Accordingly, policy makers may help expand implementation to other hospitals by supporting policies that help promote a prioritized substance use health care focus. In addition, funding for further research to examine the factors associated with hospitals’ implementation in other contexts and that uses more comprehensive methods will provide a greater understanding of how to better support hospitals.