Feasibility of a hospital-based naloxone program for postpartum patients
Providing naloxone in reproductive healthcare settings can expand access to harm reduction services and may help to address rising opioid overdose rates in postpartum patients. However, naloxone provision is not typically integrated into reproductive services. This study examined the feasibility of a novel hospital-based program aimed at educating birthing-unit staff about harm reduction and providing naloxone to all postpartum patients.
Individuals who use substances during pregnancy and postpartum periods may also be at risk of experiencing discrimination from healthcare workers, which can impact the quality of care they receive. Addiction-related training is not standard among reproductive healthcare providers, and addiction treatment and harm reduction services are not widely integrated into reproductive services. Siloed services like this can reduce access to comprehensive care and contribute to drug-related harms. Despite increased opioid overdose rates among pregnant and postpartum individuals, research suggests that, pregnant people are less likely than non-pregnant people to receive the opioid overdose reversal drug, naloxone, during emergency hospital visits for opioid overdose. This study examined the feasibility of a novel hospital-based quality improvement program that helps train birthing-unit staff on implicit bias and harm reduction and provides postpartum patients with overdose education as well as naloxone.
HOW WAS THIS STUDY CONDUCTED?
This study was a pilot feasibility study of a novel hospital-based quality improvement program that involves the education of birthing-unit staff on implicit bias and harm reduction, as well as the provision of overdose education and naloxone-containing first aid kits to all postpartum individuals.
The study was conducted between 2021 and 2022 in a birthing unit within a small rural hospital in Maine. The unit consisted of four obstetrician-gynecologists, a midwife, and nursing staff. The county in which the study was conducted accounted for 1% of Maine’s overdose deaths and zero postpartum deaths in 2021. This study’s quality-improvement program was designed and overseen by the project workgroup, which consisted of hospital providers and staff (e.g., obstetrician-gynecologist, hospital nurses and pharmacists), as well as an individual from the recovery community. The group met monthly to solve potential problems, present program data, and support providers and staff participating in the program.
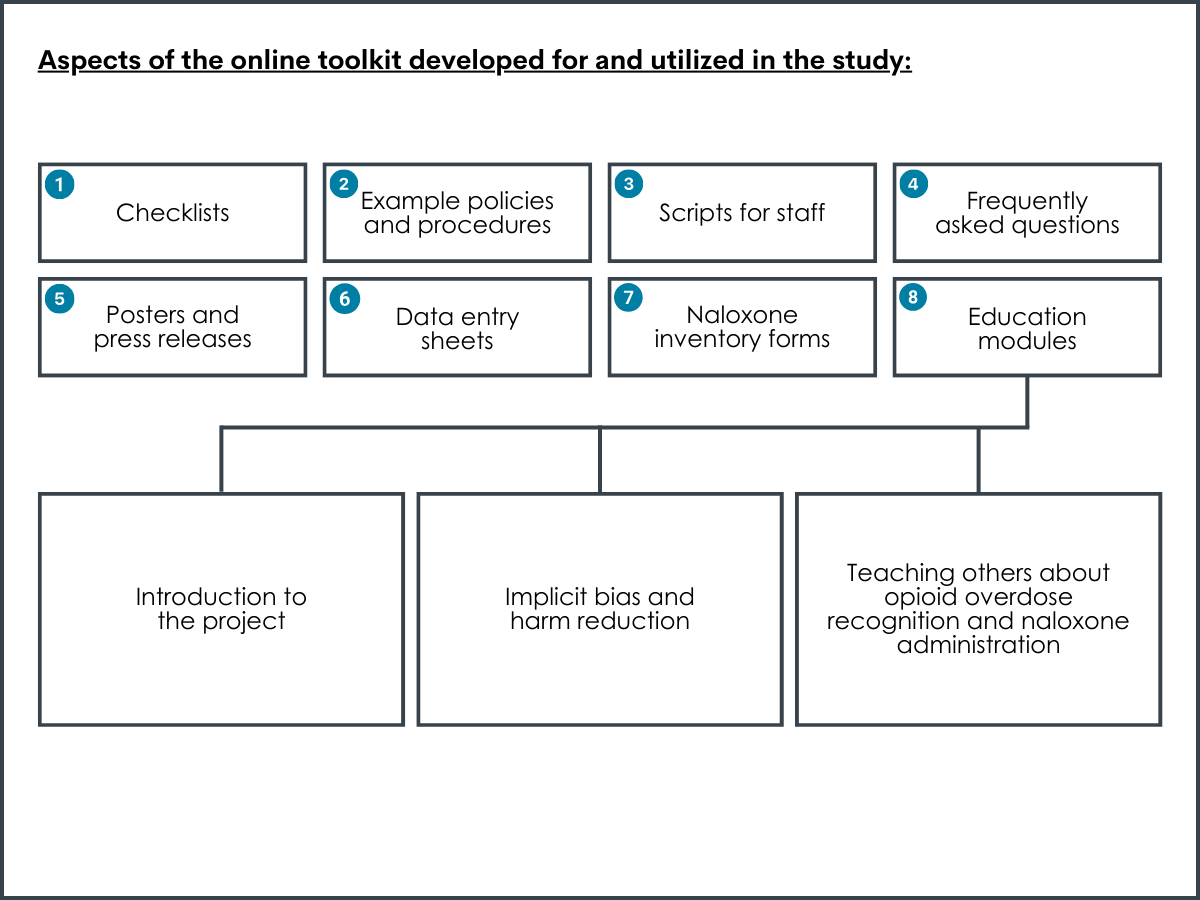
An online toolkit was created for healthcare providers and staff as part of the quality-improvement program, and included: checklists, example policies and procedures, scripts for staff, frequently asked questions, posters and press releases, data entry sheets, naloxone inventory forms, and education modules. Education modules intended for healthcare personnel training were created by the researchers, in collaboration with a harm-reduction specialist. Education modules concerned: (1) an introduction to the project, (2) implicit bias and harm reduction, and (3) teaching others about opioid overdose recognition and naloxone administration. Each module was accompanied by a post-module test of trainee knowledge – trainees were allowed to reference modules during testing and could retake the test an unlimited number of times. New providers and staff were required to complete the modules as part of their onboarding.
Providers and staff at the hospital’s birthing unit were asked to complete the education modules. Providers and staff who completed these models used scripts to introduce the project to pregnant people during their third trimester of pregnancy, with a reminder at term. All pregnant patients were approached, regardless of their substance use history. Posters about naloxone and overdose were also posted in exam rooms.
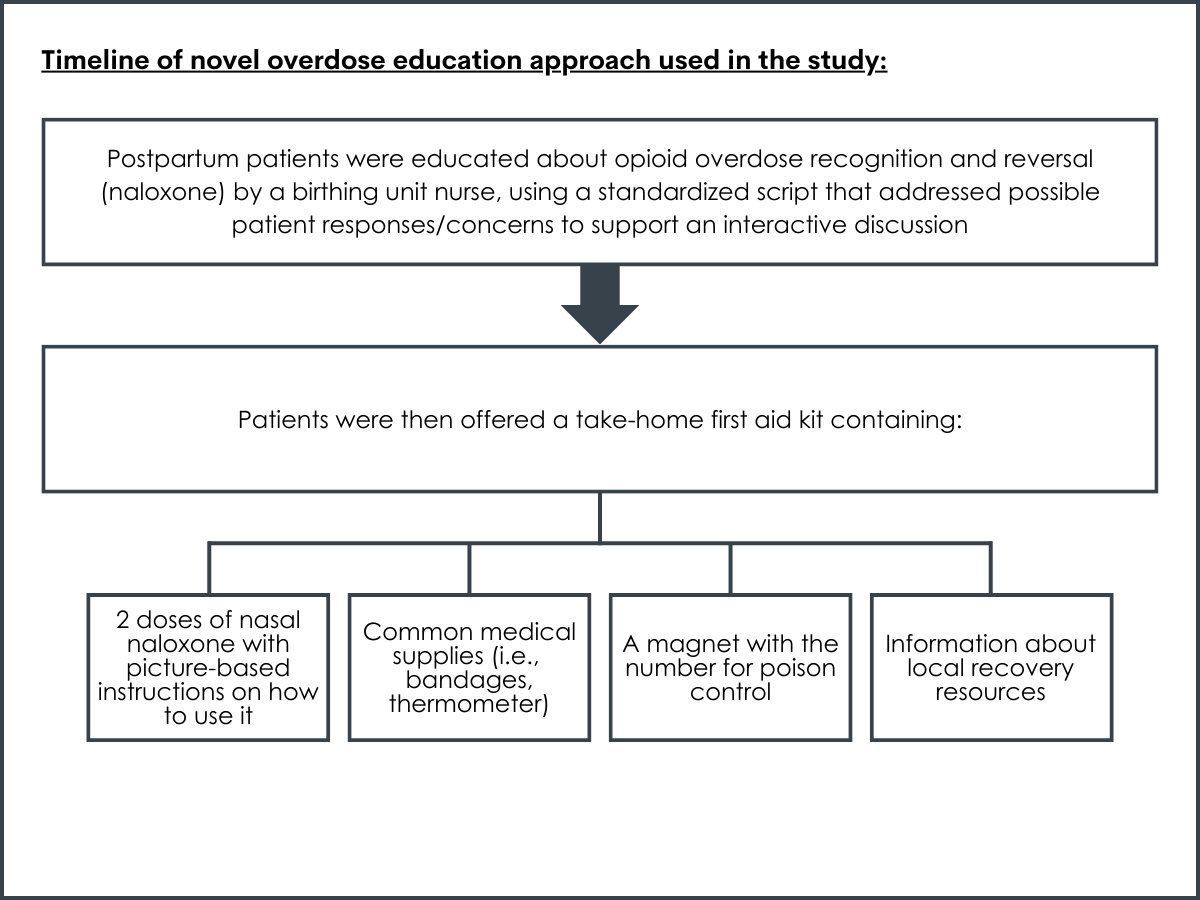
After giving birth, and before discharge from the hospital, postpartum patients were educated about opioid overdose recognition and reversal (naloxone) by a birthing unit nurse, using a standardized script that addressed possible patient responses/concerns to support an interactive discussion. Patients were then offered a take-home first aid kit containing: (1) 2 doses of nasal naloxone with picture-based instructions on how to use it, (2) common medical supplies (i.e. adhesive bandages, thermometer), (3) a magnet with the number for poison control, and (4) information about local recovery resources. The naloxone in the kit was supplied for free by the state of Maine and naloxone distribution was recorded in patients’ electronic health records by the nurse. Patients could choose to accept or decline the naloxone, the other kit contents, or the entire kit.
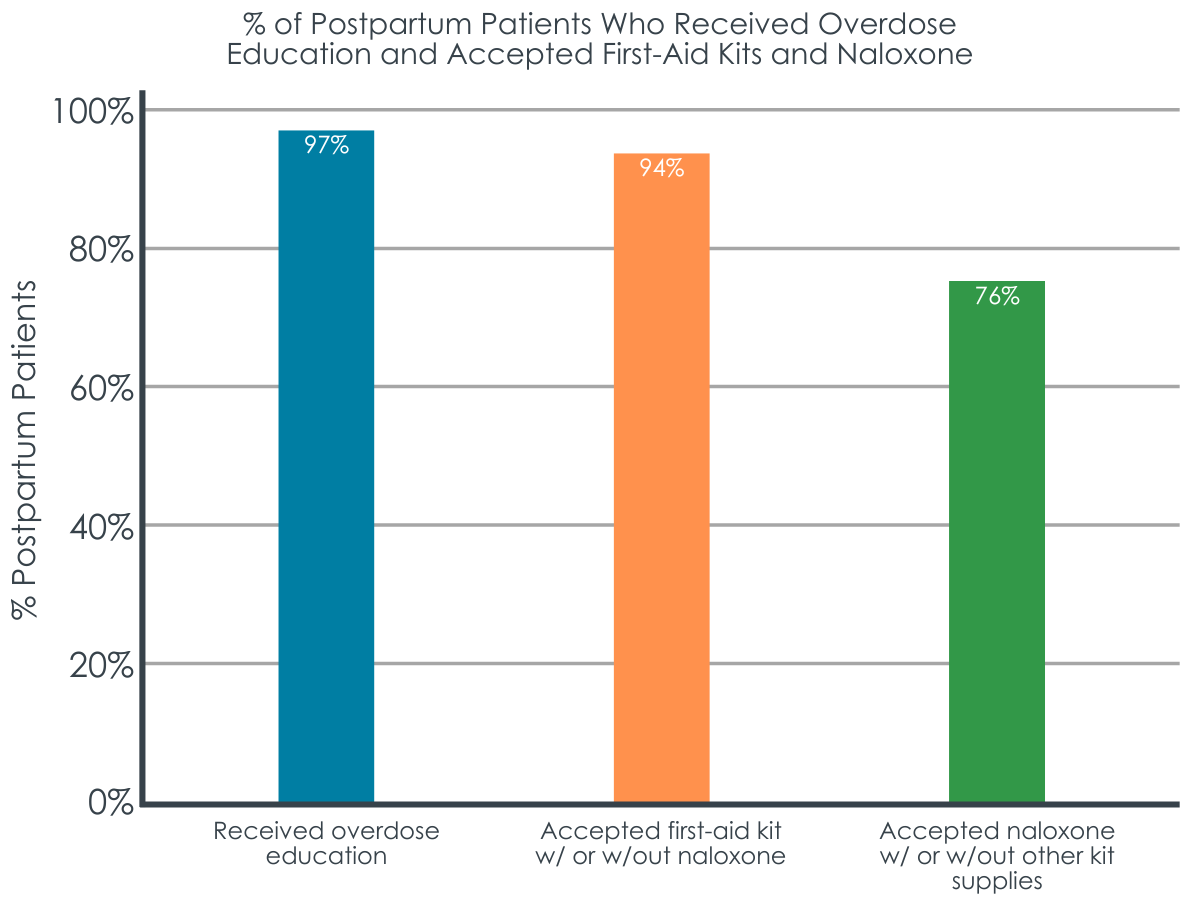
One hundred and ninety-seven postpartum individuals were discharged from the hospital during the study. Outcomes of interest included (1) the percentage of providers and staff who completed the three training modules (i.e. education-based training), as well as the percentage of postpartum individuals (2) who received harm-reduction education from nursing staff, (3) who accepted the first aid kits with or without naloxone, and (4) who accepted naloxone with or without the other kit supplies. Patient demographics, insurance coverage, and current/past substance use were not assessed.
WHAT DID THIS STUDY FIND?
The majority of postpartum patients received overdose education and accepted take-home naloxone.
Individuals engaging with peer support alongside other treatments experienced fewer emergency and acute care visits, with 8.6%, compared to 21.2% in the group only receiving outpatient services . Importantly, this improved outcome was maintained in the 90 days following the end of peer support.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined the feasibility of a novel hospital-based program that educates reproductive healthcare providers and staff on implicit bias and harm reduction and provides postpartum patients with overdose education and take-home naloxone. Findings suggest that this new overdose education and naloxone provision program for postpartum patients is feasible to implement in a hospital setting, with the majority of staff engaging in implicit bias and harm reduction training, and the majority of postpartum patients receiving overdose education and accepting take-home naloxone.
Developing and evaluating programs like this one is important because postpartum individuals are at increased risk of substance use and overdose. New parents might be reluctant to seek help for substance use problems, fearing punitive policies that target perinatal or postpartum individuals who use drugs. The provision of naloxone is a simple option for reducing overdose-related harms among pregnant and postpartum individuals, given that naloxone is not typically provided to patients in reproductive healthcare settings.
Importantly, this program offered overdose education and naloxone to all postpartum patients, regardless of their substance use history. By providing naloxone universally to all patients, providers who lack expertise in addiction and substance use disorder diagnosis, specifically, are able to offer patients brief harm-reduction services and resources without intensive diagnostic training. It also ensures that harm-reduction education and naloxone provision is done in a non-targeted way that has the potential to address drug-related consequences while preventing stigmatization and discrimination of patients who use drugs within healthcare systems.
Healthcare provider bias and discrimination toward pregnant and postpartum patients who use drugs can impact the quality of healthcare that patients receive. In this study, the majority of birthing-clinic staff completed implicit bias and harm reduction training, supporting the feasibility of hospital staff training at least in smaller rural hospitals. Encouraging staff training with incentives or requiring training as part of employment may help to equip larger hospitals with staff that are properly informed about addiction and harm-reduction resources that benefit patients.
Though nearly all patients accepted one or more of the supplies in the first aid kit, only about 75% accepted the naloxone. This may be due to the universal nature of the program, whereby all patients were offered naloxone – it is possible that people who did not use drugs did not see a need to accept the naloxone. Additional educational material addressing the broader community’s potential impact on overdose deaths may be needed to promote universal patient acceptance of naloxone. Given that fentanyl is often found in drugs sold as non-opioid substances, and that it is responsible for a large number of overdose deaths, it is important to increase the number of people who carry naloxone within the community. However, substance use history was not evaluated in this study and the reasons for naloxone refusal among 25% of patients are unclear.
Interestingly, the current program was initially seen as controversial by the local community and the hospital where the study was conducted, but concerns were eased by educating hospital colleagues and the local community about the program and its intention. Prior research suggests that several factors impact adoption of naloxone distribution programs and initiatives, including geographic location and the political and religious ideologies of the people who live and work in that region. Additional research will help determine best training practices and methods for promoting program uptake within healthcare systems and local communities to better address substance use and overdose among pregnant and postpartum individuals.
Given rising opioid overdose rates among postpartum individuals, ongoing research examining naloxone education and provision programs like this is essential for adequately equipping providers with the knowledge they need to support patients who use drugs, and for adequately equipping patients with harm-reduction resources they might not otherwise receive. Given that black women experience disproportionally high rates of maternal mortality and have a reduced likelihood of being prescribed medication treatment for opioid use disorder, making them more prone to opioid overdose, studies that examine overdose prevention strategies among this population are particularly needed to address racial health disparities.
With postpartum overdose risk being highest between seven- and twelve-months post childbirth, additional research will also help inform whether post-birth education and naloxone distribution programs are sufficient for addressing postpartum overdose or if continuing patient education and follow-up are needed to promote patient safety in the long term. Although this study did not examine the effects of this novel naloxone education and provision intervention on patient outcomes, similar approaches have shown positive outcomes, such as reduced opioid-related mortality and improved ability to effectively manage an overdose.
This study was conducted in a rural hospital in a county containing only 2% of Maine’s population and 1% of overdose deaths, with no postpartum overdose deaths. This precluded the evaluation of the program’s effects on local mortality rates. Additional studies are needed in other healthcare settings (e.g., large urban hospitals) where postpartum overdose deaths are more common.
Data were recorded by nursing staff participating in the quality improvement program and it is unclear if data documentation by a third party would result in different outcomes. Though education of patients about overdose identification and reversal was scripted, nurse delivery of the material was not observed and adherence to the script is unknown.
New providers and staff were required to complete the program’s training modules as part of their onboarding process. It is also unclear how established providers and staff were asked/told to complete training or if it was incentivized. These limitations have the potential to influence training completion rates.
BOTTOM LINE
This hospital-based overdose education and naloxone provision program for postpartum patients was feasible for providers and patients in a small birthing unit in a rural region. The majority of staff completed implicit bias and harm reduction training. Nearly all postpartum patients received overdose education from staff and three-quarters accepted take-home naloxone. Though additional research is needed to evaluate the impact of this overdose education and naloxone provision program on healthcare practices and patient outcomes, low-threshold, universal harm-reduction programs like this, that reduce opioid-related harms while limiting discrimination and stigmatization of pregnant and postpartum people who use drugs are important for addressing opioid overdose in this at-risk population.
For individuals and families seeking recovery: Naloxone is an easy-to-administer medication that can reverse the effect of an opioid overdose and reduce a person’s risk of overdose-related death. Given that the opioid fentanyl is often found in illicit drugs marketed as non-opioid substances, naloxone should be carried by all individuals using drugs, as well as their family and friends. Naloxone is not typically available in primary care or reproductive healthcare practices, but it is often available through the community. In the US, Naloxone can be purchased online and at local pharmacies without a prescription. Interested individuals can also find naloxone near them through the National Harm Reduction Coalition.
For treatment professionals and treatment systems: This study helps us examine new ways to expand naloxone distribution among postpartum individuals in hospital-based settings, which can help address rising rates of opioid-related overdoses among pregnant and postpartum women. Naloxone is a life-saving medication with no misuse liability that can reverse the effect of an opioid overdose. It should be carried by all individuals who use drugs and their family and friends, as well as healthcare providers and staff. Encouraging local healthcare systems to support naloxone distribution initiatives could potentially increase naloxone access and save lives.
For scientists: Additional research, including multi-site studies that evaluate provider practices and long-term patient outcomes, are needed to extend these findings. Studies in urban healthcare settings and other states with high postpartum overdose rates, that control for potentially confounding factors like patient and provider characteristics, are needed. Research is needed to examine the most effective components of overdose education and naloxone distribution programs like this, and to identify other factors impacting naloxone acceptance/refusal among patients. Additional research may also help identify and address barriers and facilitators to naloxone provision in various healthcare settings and among different patient populations.
For policy makers: Studies like this highlight potential ways to expand access to naloxone, a life-saving medication with no misuse liability that can reverse the effect of an opioid overdose. Given that the opioid fentanyl is often found in illicit drugs marketed as non-opioid substances, and that fentanyl is responsible for a sharp rise in opioid-related overdoses, widespread access to naloxone is essential for preventing overdose-related deaths. Federal and state initiatives have helped increase the availability of naloxone, but efforts are still needed, particularly among pregnant and postpartum individuals, who are at increased risk of substance use and overdose. Community-based overdose education and naloxone distribution programs like this one have the potential to help address opioid overdose deaths by increasing access to naloxone. Additional funding will help identify the best education and distribution models for promoting naloxone distribution among various patient cohorts in different community settings.
Individuals who use substances during pregnancy and postpartum periods may also be at risk of experiencing discrimination from healthcare workers, which can impact the quality of care they receive. Addiction-related training is not standard among reproductive healthcare providers, and addiction treatment and harm reduction services are not widely integrated into reproductive services. Siloed services like this can reduce access to comprehensive care and contribute to drug-related harms. Despite increased opioid overdose rates among pregnant and postpartum individuals, research suggests that, pregnant people are less likely than non-pregnant people to receive the opioid overdose reversal drug, naloxone, during emergency hospital visits for opioid overdose. This study examined the feasibility of a novel hospital-based quality improvement program that helps train birthing-unit staff on implicit bias and harm reduction and provides postpartum patients with overdose education as well as naloxone.
HOW WAS THIS STUDY CONDUCTED?
This study was a pilot feasibility study of a novel hospital-based quality improvement program that involves the education of birthing-unit staff on implicit bias and harm reduction, as well as the provision of overdose education and naloxone-containing first aid kits to all postpartum individuals.
The study was conducted between 2021 and 2022 in a birthing unit within a small rural hospital in Maine. The unit consisted of four obstetrician-gynecologists, a midwife, and nursing staff. The county in which the study was conducted accounted for 1% of Maine’s overdose deaths and zero postpartum deaths in 2021. This study’s quality-improvement program was designed and overseen by the project workgroup, which consisted of hospital providers and staff (e.g., obstetrician-gynecologist, hospital nurses and pharmacists), as well as an individual from the recovery community. The group met monthly to solve potential problems, present program data, and support providers and staff participating in the program.
An online toolkit was created for healthcare providers and staff as part of the quality-improvement program, and included: checklists, example policies and procedures, scripts for staff, frequently asked questions, posters and press releases, data entry sheets, naloxone inventory forms, and education modules. Education modules intended for healthcare personnel training were created by the researchers, in collaboration with a harm-reduction specialist. Education modules concerned: (1) an introduction to the project, (2) implicit bias and harm reduction, and (3) teaching others about opioid overdose recognition and naloxone administration. Each module was accompanied by a post-module test of trainee knowledge – trainees were allowed to reference modules during testing and could retake the test an unlimited number of times. New providers and staff were required to complete the modules as part of their onboarding.
Providers and staff at the hospital’s birthing unit were asked to complete the education modules. Providers and staff who completed these models used scripts to introduce the project to pregnant people during their third trimester of pregnancy, with a reminder at term. All pregnant patients were approached, regardless of their substance use history. Posters about naloxone and overdose were also posted in exam rooms.
After giving birth, and before discharge from the hospital, postpartum patients were educated about opioid overdose recognition and reversal (naloxone) by a birthing unit nurse, using a standardized script that addressed possible patient responses/concerns to support an interactive discussion. Patients were then offered a take-home first aid kit containing: (1) 2 doses of nasal naloxone with picture-based instructions on how to use it, (2) common medical supplies (i.e. adhesive bandages, thermometer), (3) a magnet with the number for poison control, and (4) information about local recovery resources. The naloxone in the kit was supplied for free by the state of Maine and naloxone distribution was recorded in patients’ electronic health records by the nurse. Patients could choose to accept or decline the naloxone, the other kit contents, or the entire kit.
One hundred and ninety-seven postpartum individuals were discharged from the hospital during the study. Outcomes of interest included (1) the percentage of providers and staff who completed the three training modules (i.e. education-based training), as well as the percentage of postpartum individuals (2) who received harm-reduction education from nursing staff, (3) who accepted the first aid kits with or without naloxone, and (4) who accepted naloxone with or without the other kit supplies. Patient demographics, insurance coverage, and current/past substance use were not assessed.
WHAT DID THIS STUDY FIND?
The majority of postpartum patients received overdose education and accepted take-home naloxone.
Individuals engaging with peer support alongside other treatments experienced fewer emergency and acute care visits, with 8.6%, compared to 21.2% in the group only receiving outpatient services . Importantly, this improved outcome was maintained in the 90 days following the end of peer support.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined the feasibility of a novel hospital-based program that educates reproductive healthcare providers and staff on implicit bias and harm reduction and provides postpartum patients with overdose education and take-home naloxone. Findings suggest that this new overdose education and naloxone provision program for postpartum patients is feasible to implement in a hospital setting, with the majority of staff engaging in implicit bias and harm reduction training, and the majority of postpartum patients receiving overdose education and accepting take-home naloxone.
Developing and evaluating programs like this one is important because postpartum individuals are at increased risk of substance use and overdose. New parents might be reluctant to seek help for substance use problems, fearing punitive policies that target perinatal or postpartum individuals who use drugs. The provision of naloxone is a simple option for reducing overdose-related harms among pregnant and postpartum individuals, given that naloxone is not typically provided to patients in reproductive healthcare settings.
Importantly, this program offered overdose education and naloxone to all postpartum patients, regardless of their substance use history. By providing naloxone universally to all patients, providers who lack expertise in addiction and substance use disorder diagnosis, specifically, are able to offer patients brief harm-reduction services and resources without intensive diagnostic training. It also ensures that harm-reduction education and naloxone provision is done in a non-targeted way that has the potential to address drug-related consequences while preventing stigmatization and discrimination of patients who use drugs within healthcare systems.
Healthcare provider bias and discrimination toward pregnant and postpartum patients who use drugs can impact the quality of healthcare that patients receive. In this study, the majority of birthing-clinic staff completed implicit bias and harm reduction training, supporting the feasibility of hospital staff training at least in smaller rural hospitals. Encouraging staff training with incentives or requiring training as part of employment may help to equip larger hospitals with staff that are properly informed about addiction and harm-reduction resources that benefit patients.
Though nearly all patients accepted one or more of the supplies in the first aid kit, only about 75% accepted the naloxone. This may be due to the universal nature of the program, whereby all patients were offered naloxone – it is possible that people who did not use drugs did not see a need to accept the naloxone. Additional educational material addressing the broader community’s potential impact on overdose deaths may be needed to promote universal patient acceptance of naloxone. Given that fentanyl is often found in drugs sold as non-opioid substances, and that it is responsible for a large number of overdose deaths, it is important to increase the number of people who carry naloxone within the community. However, substance use history was not evaluated in this study and the reasons for naloxone refusal among 25% of patients are unclear.
Interestingly, the current program was initially seen as controversial by the local community and the hospital where the study was conducted, but concerns were eased by educating hospital colleagues and the local community about the program and its intention. Prior research suggests that several factors impact adoption of naloxone distribution programs and initiatives, including geographic location and the political and religious ideologies of the people who live and work in that region. Additional research will help determine best training practices and methods for promoting program uptake within healthcare systems and local communities to better address substance use and overdose among pregnant and postpartum individuals.
Given rising opioid overdose rates among postpartum individuals, ongoing research examining naloxone education and provision programs like this is essential for adequately equipping providers with the knowledge they need to support patients who use drugs, and for adequately equipping patients with harm-reduction resources they might not otherwise receive. Given that black women experience disproportionally high rates of maternal mortality and have a reduced likelihood of being prescribed medication treatment for opioid use disorder, making them more prone to opioid overdose, studies that examine overdose prevention strategies among this population are particularly needed to address racial health disparities.
With postpartum overdose risk being highest between seven- and twelve-months post childbirth, additional research will also help inform whether post-birth education and naloxone distribution programs are sufficient for addressing postpartum overdose or if continuing patient education and follow-up are needed to promote patient safety in the long term. Although this study did not examine the effects of this novel naloxone education and provision intervention on patient outcomes, similar approaches have shown positive outcomes, such as reduced opioid-related mortality and improved ability to effectively manage an overdose.
This study was conducted in a rural hospital in a county containing only 2% of Maine’s population and 1% of overdose deaths, with no postpartum overdose deaths. This precluded the evaluation of the program’s effects on local mortality rates. Additional studies are needed in other healthcare settings (e.g., large urban hospitals) where postpartum overdose deaths are more common.
Data were recorded by nursing staff participating in the quality improvement program and it is unclear if data documentation by a third party would result in different outcomes. Though education of patients about overdose identification and reversal was scripted, nurse delivery of the material was not observed and adherence to the script is unknown.
New providers and staff were required to complete the program’s training modules as part of their onboarding process. It is also unclear how established providers and staff were asked/told to complete training or if it was incentivized. These limitations have the potential to influence training completion rates.
BOTTOM LINE
This hospital-based overdose education and naloxone provision program for postpartum patients was feasible for providers and patients in a small birthing unit in a rural region. The majority of staff completed implicit bias and harm reduction training. Nearly all postpartum patients received overdose education from staff and three-quarters accepted take-home naloxone. Though additional research is needed to evaluate the impact of this overdose education and naloxone provision program on healthcare practices and patient outcomes, low-threshold, universal harm-reduction programs like this, that reduce opioid-related harms while limiting discrimination and stigmatization of pregnant and postpartum people who use drugs are important for addressing opioid overdose in this at-risk population.
For individuals and families seeking recovery: Naloxone is an easy-to-administer medication that can reverse the effect of an opioid overdose and reduce a person’s risk of overdose-related death. Given that the opioid fentanyl is often found in illicit drugs marketed as non-opioid substances, naloxone should be carried by all individuals using drugs, as well as their family and friends. Naloxone is not typically available in primary care or reproductive healthcare practices, but it is often available through the community. In the US, Naloxone can be purchased online and at local pharmacies without a prescription. Interested individuals can also find naloxone near them through the National Harm Reduction Coalition.
For treatment professionals and treatment systems: This study helps us examine new ways to expand naloxone distribution among postpartum individuals in hospital-based settings, which can help address rising rates of opioid-related overdoses among pregnant and postpartum women. Naloxone is a life-saving medication with no misuse liability that can reverse the effect of an opioid overdose. It should be carried by all individuals who use drugs and their family and friends, as well as healthcare providers and staff. Encouraging local healthcare systems to support naloxone distribution initiatives could potentially increase naloxone access and save lives.
For scientists: Additional research, including multi-site studies that evaluate provider practices and long-term patient outcomes, are needed to extend these findings. Studies in urban healthcare settings and other states with high postpartum overdose rates, that control for potentially confounding factors like patient and provider characteristics, are needed. Research is needed to examine the most effective components of overdose education and naloxone distribution programs like this, and to identify other factors impacting naloxone acceptance/refusal among patients. Additional research may also help identify and address barriers and facilitators to naloxone provision in various healthcare settings and among different patient populations.
For policy makers: Studies like this highlight potential ways to expand access to naloxone, a life-saving medication with no misuse liability that can reverse the effect of an opioid overdose. Given that the opioid fentanyl is often found in illicit drugs marketed as non-opioid substances, and that fentanyl is responsible for a sharp rise in opioid-related overdoses, widespread access to naloxone is essential for preventing overdose-related deaths. Federal and state initiatives have helped increase the availability of naloxone, but efforts are still needed, particularly among pregnant and postpartum individuals, who are at increased risk of substance use and overdose. Community-based overdose education and naloxone distribution programs like this one have the potential to help address opioid overdose deaths by increasing access to naloxone. Additional funding will help identify the best education and distribution models for promoting naloxone distribution among various patient cohorts in different community settings.
Individuals who use substances during pregnancy and postpartum periods may also be at risk of experiencing discrimination from healthcare workers, which can impact the quality of care they receive. Addiction-related training is not standard among reproductive healthcare providers, and addiction treatment and harm reduction services are not widely integrated into reproductive services. Siloed services like this can reduce access to comprehensive care and contribute to drug-related harms. Despite increased opioid overdose rates among pregnant and postpartum individuals, research suggests that, pregnant people are less likely than non-pregnant people to receive the opioid overdose reversal drug, naloxone, during emergency hospital visits for opioid overdose. This study examined the feasibility of a novel hospital-based quality improvement program that helps train birthing-unit staff on implicit bias and harm reduction and provides postpartum patients with overdose education as well as naloxone.
HOW WAS THIS STUDY CONDUCTED?
This study was a pilot feasibility study of a novel hospital-based quality improvement program that involves the education of birthing-unit staff on implicit bias and harm reduction, as well as the provision of overdose education and naloxone-containing first aid kits to all postpartum individuals.
The study was conducted between 2021 and 2022 in a birthing unit within a small rural hospital in Maine. The unit consisted of four obstetrician-gynecologists, a midwife, and nursing staff. The county in which the study was conducted accounted for 1% of Maine’s overdose deaths and zero postpartum deaths in 2021. This study’s quality-improvement program was designed and overseen by the project workgroup, which consisted of hospital providers and staff (e.g., obstetrician-gynecologist, hospital nurses and pharmacists), as well as an individual from the recovery community. The group met monthly to solve potential problems, present program data, and support providers and staff participating in the program.
An online toolkit was created for healthcare providers and staff as part of the quality-improvement program, and included: checklists, example policies and procedures, scripts for staff, frequently asked questions, posters and press releases, data entry sheets, naloxone inventory forms, and education modules. Education modules intended for healthcare personnel training were created by the researchers, in collaboration with a harm-reduction specialist. Education modules concerned: (1) an introduction to the project, (2) implicit bias and harm reduction, and (3) teaching others about opioid overdose recognition and naloxone administration. Each module was accompanied by a post-module test of trainee knowledge – trainees were allowed to reference modules during testing and could retake the test an unlimited number of times. New providers and staff were required to complete the modules as part of their onboarding.
Providers and staff at the hospital’s birthing unit were asked to complete the education modules. Providers and staff who completed these models used scripts to introduce the project to pregnant people during their third trimester of pregnancy, with a reminder at term. All pregnant patients were approached, regardless of their substance use history. Posters about naloxone and overdose were also posted in exam rooms.
After giving birth, and before discharge from the hospital, postpartum patients were educated about opioid overdose recognition and reversal (naloxone) by a birthing unit nurse, using a standardized script that addressed possible patient responses/concerns to support an interactive discussion. Patients were then offered a take-home first aid kit containing: (1) 2 doses of nasal naloxone with picture-based instructions on how to use it, (2) common medical supplies (i.e. adhesive bandages, thermometer), (3) a magnet with the number for poison control, and (4) information about local recovery resources. The naloxone in the kit was supplied for free by the state of Maine and naloxone distribution was recorded in patients’ electronic health records by the nurse. Patients could choose to accept or decline the naloxone, the other kit contents, or the entire kit.
One hundred and ninety-seven postpartum individuals were discharged from the hospital during the study. Outcomes of interest included (1) the percentage of providers and staff who completed the three training modules (i.e. education-based training), as well as the percentage of postpartum individuals (2) who received harm-reduction education from nursing staff, (3) who accepted the first aid kits with or without naloxone, and (4) who accepted naloxone with or without the other kit supplies. Patient demographics, insurance coverage, and current/past substance use were not assessed.
WHAT DID THIS STUDY FIND?
The majority of postpartum patients received overdose education and accepted take-home naloxone.
Individuals engaging with peer support alongside other treatments experienced fewer emergency and acute care visits, with 8.6%, compared to 21.2% in the group only receiving outpatient services . Importantly, this improved outcome was maintained in the 90 days following the end of peer support.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined the feasibility of a novel hospital-based program that educates reproductive healthcare providers and staff on implicit bias and harm reduction and provides postpartum patients with overdose education and take-home naloxone. Findings suggest that this new overdose education and naloxone provision program for postpartum patients is feasible to implement in a hospital setting, with the majority of staff engaging in implicit bias and harm reduction training, and the majority of postpartum patients receiving overdose education and accepting take-home naloxone.
Developing and evaluating programs like this one is important because postpartum individuals are at increased risk of substance use and overdose. New parents might be reluctant to seek help for substance use problems, fearing punitive policies that target perinatal or postpartum individuals who use drugs. The provision of naloxone is a simple option for reducing overdose-related harms among pregnant and postpartum individuals, given that naloxone is not typically provided to patients in reproductive healthcare settings.
Importantly, this program offered overdose education and naloxone to all postpartum patients, regardless of their substance use history. By providing naloxone universally to all patients, providers who lack expertise in addiction and substance use disorder diagnosis, specifically, are able to offer patients brief harm-reduction services and resources without intensive diagnostic training. It also ensures that harm-reduction education and naloxone provision is done in a non-targeted way that has the potential to address drug-related consequences while preventing stigmatization and discrimination of patients who use drugs within healthcare systems.
Healthcare provider bias and discrimination toward pregnant and postpartum patients who use drugs can impact the quality of healthcare that patients receive. In this study, the majority of birthing-clinic staff completed implicit bias and harm reduction training, supporting the feasibility of hospital staff training at least in smaller rural hospitals. Encouraging staff training with incentives or requiring training as part of employment may help to equip larger hospitals with staff that are properly informed about addiction and harm-reduction resources that benefit patients.
Though nearly all patients accepted one or more of the supplies in the first aid kit, only about 75% accepted the naloxone. This may be due to the universal nature of the program, whereby all patients were offered naloxone – it is possible that people who did not use drugs did not see a need to accept the naloxone. Additional educational material addressing the broader community’s potential impact on overdose deaths may be needed to promote universal patient acceptance of naloxone. Given that fentanyl is often found in drugs sold as non-opioid substances, and that it is responsible for a large number of overdose deaths, it is important to increase the number of people who carry naloxone within the community. However, substance use history was not evaluated in this study and the reasons for naloxone refusal among 25% of patients are unclear.
Interestingly, the current program was initially seen as controversial by the local community and the hospital where the study was conducted, but concerns were eased by educating hospital colleagues and the local community about the program and its intention. Prior research suggests that several factors impact adoption of naloxone distribution programs and initiatives, including geographic location and the political and religious ideologies of the people who live and work in that region. Additional research will help determine best training practices and methods for promoting program uptake within healthcare systems and local communities to better address substance use and overdose among pregnant and postpartum individuals.
Given rising opioid overdose rates among postpartum individuals, ongoing research examining naloxone education and provision programs like this is essential for adequately equipping providers with the knowledge they need to support patients who use drugs, and for adequately equipping patients with harm-reduction resources they might not otherwise receive. Given that black women experience disproportionally high rates of maternal mortality and have a reduced likelihood of being prescribed medication treatment for opioid use disorder, making them more prone to opioid overdose, studies that examine overdose prevention strategies among this population are particularly needed to address racial health disparities.
With postpartum overdose risk being highest between seven- and twelve-months post childbirth, additional research will also help inform whether post-birth education and naloxone distribution programs are sufficient for addressing postpartum overdose or if continuing patient education and follow-up are needed to promote patient safety in the long term. Although this study did not examine the effects of this novel naloxone education and provision intervention on patient outcomes, similar approaches have shown positive outcomes, such as reduced opioid-related mortality and improved ability to effectively manage an overdose.
This study was conducted in a rural hospital in a county containing only 2% of Maine’s population and 1% of overdose deaths, with no postpartum overdose deaths. This precluded the evaluation of the program’s effects on local mortality rates. Additional studies are needed in other healthcare settings (e.g., large urban hospitals) where postpartum overdose deaths are more common.
Data were recorded by nursing staff participating in the quality improvement program and it is unclear if data documentation by a third party would result in different outcomes. Though education of patients about overdose identification and reversal was scripted, nurse delivery of the material was not observed and adherence to the script is unknown.
New providers and staff were required to complete the program’s training modules as part of their onboarding process. It is also unclear how established providers and staff were asked/told to complete training or if it was incentivized. These limitations have the potential to influence training completion rates.
BOTTOM LINE
This hospital-based overdose education and naloxone provision program for postpartum patients was feasible for providers and patients in a small birthing unit in a rural region. The majority of staff completed implicit bias and harm reduction training. Nearly all postpartum patients received overdose education from staff and three-quarters accepted take-home naloxone. Though additional research is needed to evaluate the impact of this overdose education and naloxone provision program on healthcare practices and patient outcomes, low-threshold, universal harm-reduction programs like this, that reduce opioid-related harms while limiting discrimination and stigmatization of pregnant and postpartum people who use drugs are important for addressing opioid overdose in this at-risk population.
For individuals and families seeking recovery: Naloxone is an easy-to-administer medication that can reverse the effect of an opioid overdose and reduce a person’s risk of overdose-related death. Given that the opioid fentanyl is often found in illicit drugs marketed as non-opioid substances, naloxone should be carried by all individuals using drugs, as well as their family and friends. Naloxone is not typically available in primary care or reproductive healthcare practices, but it is often available through the community. In the US, Naloxone can be purchased online and at local pharmacies without a prescription. Interested individuals can also find naloxone near them through the National Harm Reduction Coalition.
For treatment professionals and treatment systems: This study helps us examine new ways to expand naloxone distribution among postpartum individuals in hospital-based settings, which can help address rising rates of opioid-related overdoses among pregnant and postpartum women. Naloxone is a life-saving medication with no misuse liability that can reverse the effect of an opioid overdose. It should be carried by all individuals who use drugs and their family and friends, as well as healthcare providers and staff. Encouraging local healthcare systems to support naloxone distribution initiatives could potentially increase naloxone access and save lives.
For scientists: Additional research, including multi-site studies that evaluate provider practices and long-term patient outcomes, are needed to extend these findings. Studies in urban healthcare settings and other states with high postpartum overdose rates, that control for potentially confounding factors like patient and provider characteristics, are needed. Research is needed to examine the most effective components of overdose education and naloxone distribution programs like this, and to identify other factors impacting naloxone acceptance/refusal among patients. Additional research may also help identify and address barriers and facilitators to naloxone provision in various healthcare settings and among different patient populations.
For policy makers: Studies like this highlight potential ways to expand access to naloxone, a life-saving medication with no misuse liability that can reverse the effect of an opioid overdose. Given that the opioid fentanyl is often found in illicit drugs marketed as non-opioid substances, and that fentanyl is responsible for a sharp rise in opioid-related overdoses, widespread access to naloxone is essential for preventing overdose-related deaths. Federal and state initiatives have helped increase the availability of naloxone, but efforts are still needed, particularly among pregnant and postpartum individuals, who are at increased risk of substance use and overdose. Community-based overdose education and naloxone distribution programs like this one have the potential to help address opioid overdose deaths by increasing access to naloxone. Additional funding will help identify the best education and distribution models for promoting naloxone distribution among various patient cohorts in different community settings.