Does race influence likelihood that pregnant women with opioid use disorder receive medication?
For women who are pregnant and have opioid use disorder, empirically supported medicines like buprenorphine improve their health and the health of their babies; yet many pregnant women do not receive these treatments. There are also differences in medication receipt for opioid use disorder between individuals of different racial/ethnic backgrounds. This study examined whether the race/ethnicity of pregnant women resulted in different patterns of opioid use disorder medication, whether duration of medication receipt differed, and what types of medication were used.
Opioid use disorder (OUD) has increased among pregnant women and can result in a variety of negative outcomes for women and their children including preterm labor, stillbirth, neonatal abstinence syndrome, or maternal fatality. Evidence demonstrates that medication, such as methadone or buprenorphine, can be used successfully to treat OUD among pregnant women and improve health for mothers and their babies; yet, many pregnant women do not receive this treatment. Many factors influence whether an individual is offered and/or accepts OUD medications. Such factors include availability and clinical training for medication prescriptions, insurance coverage of these services, access to providers by geographic location, and stigma or misunderstanding about using medications for OUD treatment. Like other SUD treatments, these factors in uptake suggest racial/ethnic minorities may be less likely to receive these empirically supported OUD medicines. In this study, researchers examined whether a pregnant woman’s race/ethnicity resulted in several different outcomes of OUD medication treatment receipt including whether race/ethnicity affected patterns and duration of medication receipt to treat OUD and what types of medication were used.
HOW WAS THIS STUDY CONDUCTED?
This study was secondary data analysis of a statewide linked data set in Massachusetts (Public Health Data Warehouse), that is, a dataset combined from several public health datasets. The dataset captured over 270,000 live baby deliveries in Massachusetts between October 2011 and December 2015; of these, 5247 births were to women with OUD who were either of non-Hispanic White, Black, or Hispanic race/ethnicity and this is the subset of women who were included in this study’s analytic sample. In addition to participant characteristics (age, race/ethnicity), the dataset included treatment receipt, addiction treatment records, and data from the prescription monitoring program for these women for the nine months prior to the birth of a baby. The authors examined whether any of these three experiences varied by maternal race/ethnicity: (1) Use of any medication to treat OUD; (2) An individual’s extent of use of medication to treat OUD (using three categories which included inconsistent, consistent, and none; see paragraph below for more details); (3) The type of medication (buprenorphine, methadone) used to treat OUD.
The primary variables in the analysis were maternal race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic). Consistent use of medication to treat OUD was defined as monthly receipt for at least 6 months of treatment before delivery while inconsistent use of medication was defined as any medication to treat OUD in the year before delivery but with gaps in treatment months. The authors also used several control variables in the analysis to isolate the relationships between race/ethnicity and their questions of OUD medication treatment receipt. These variables included maternal age at delivery, maternal education, enrollment in Medicaid, marital status, geographic location of residence (rural/non-rural), maternal diagnosis of depression or anxiety, incarceration, homelessness, high use of unscheduled care, and adequacy of prenatal care based on the Kotelchuck index.
Of note, the authors identified women with OUD using the following indicators from the linked dataset: (1) a diagnosis of OUD from hospital discharge or all-payer claims database records; (2) an opioid overdose event from claims or ambulance data; (3) enrollment in a state-funded treatment program for an opioid problem; (4) receipt of methadone or buprenorphine treatment; or (5) an insurance claim for an infant diagnosis of neonatal abstinence syndrome (NAS). Mothers who were identified only by a NAS infant diagnosis were excluded if they had an opioid prescription in the 3 months before delivery or if their child was born at or before 34 weeks gestation to prevent misclassification of women with chronic pain and iatrogenic cases of NAS.
Study participants were the 5247 women with OUD who had delivered a baby in Massachusetts between October 2011 and December 2015. The average age of mothers at delivery was 29 years old. Most of the sample were white non-Hispanic (4551, 86.7%), while smaller numbers of women were Hispanic (462, 8.8%) and black non-Hispanic (234, 4.5%).
WHAT DID THIS STUDY FIND?
A majority, but not all women received medication to treat OUD during pregnancy and consistent receipt of medication was low across all racial/ethnic groups.
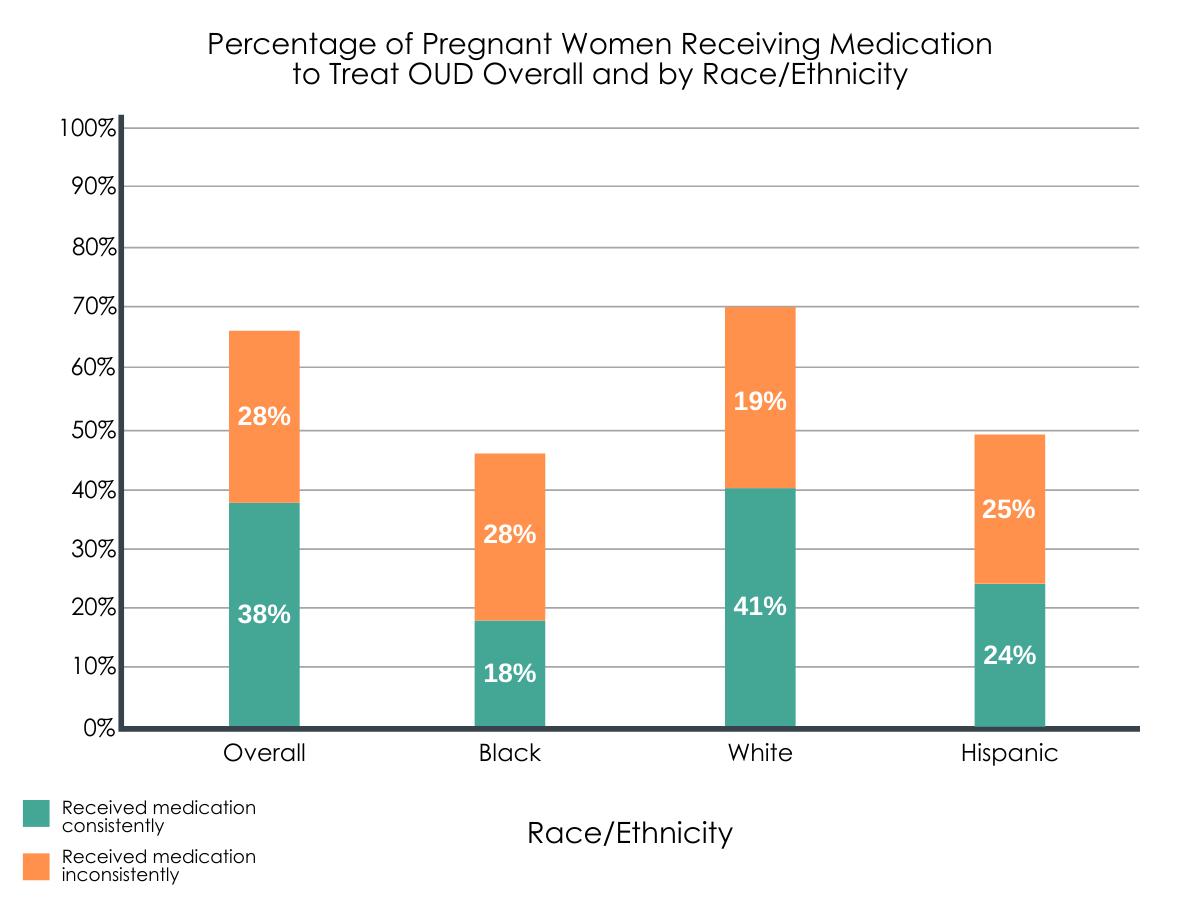
Two-thirds (66%) of women received medication to treat OUD during pregnancy, yet only 58% of these were consistent in their receipt of this medication. This finding indicates that in fact only 38% of women consistently received medication to treat OUD during pregnancy, while 28% had inconsistent medication receipt.
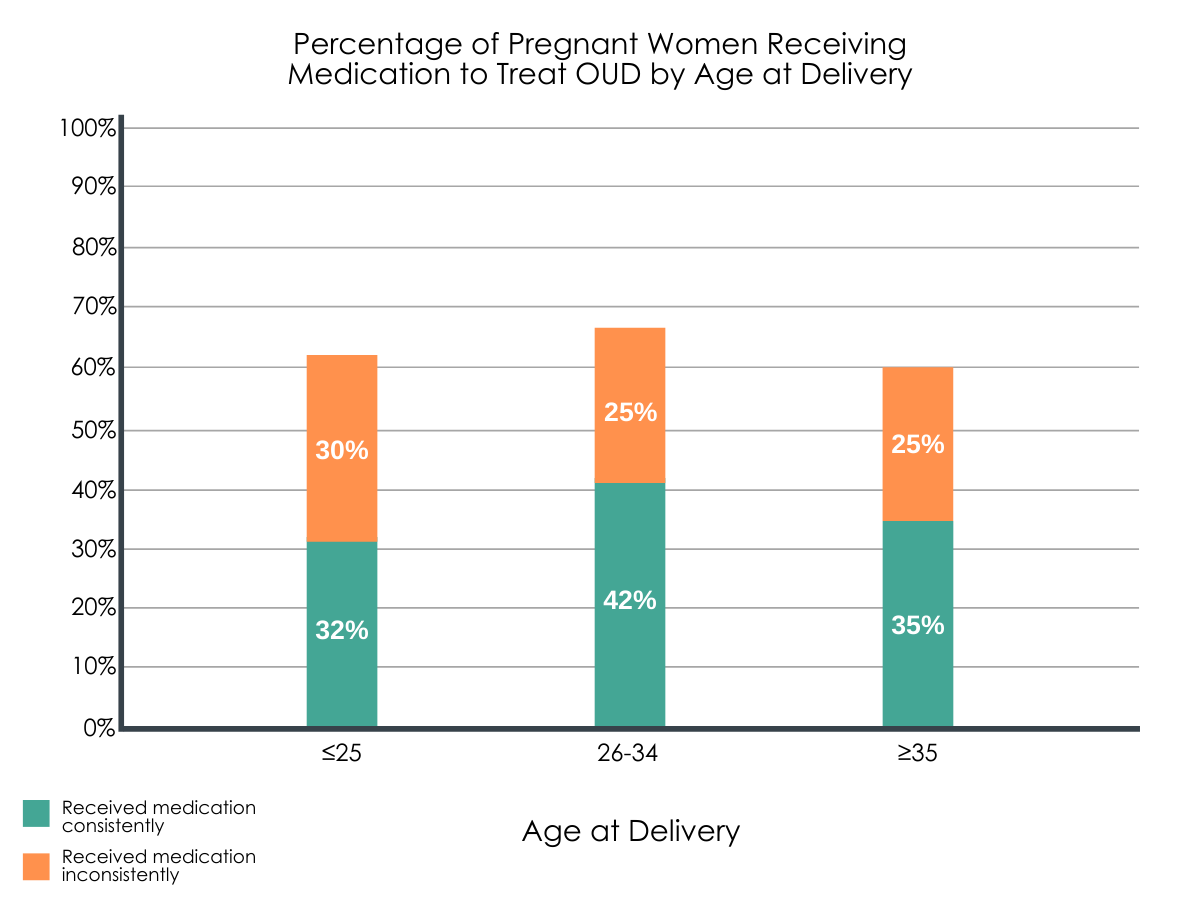
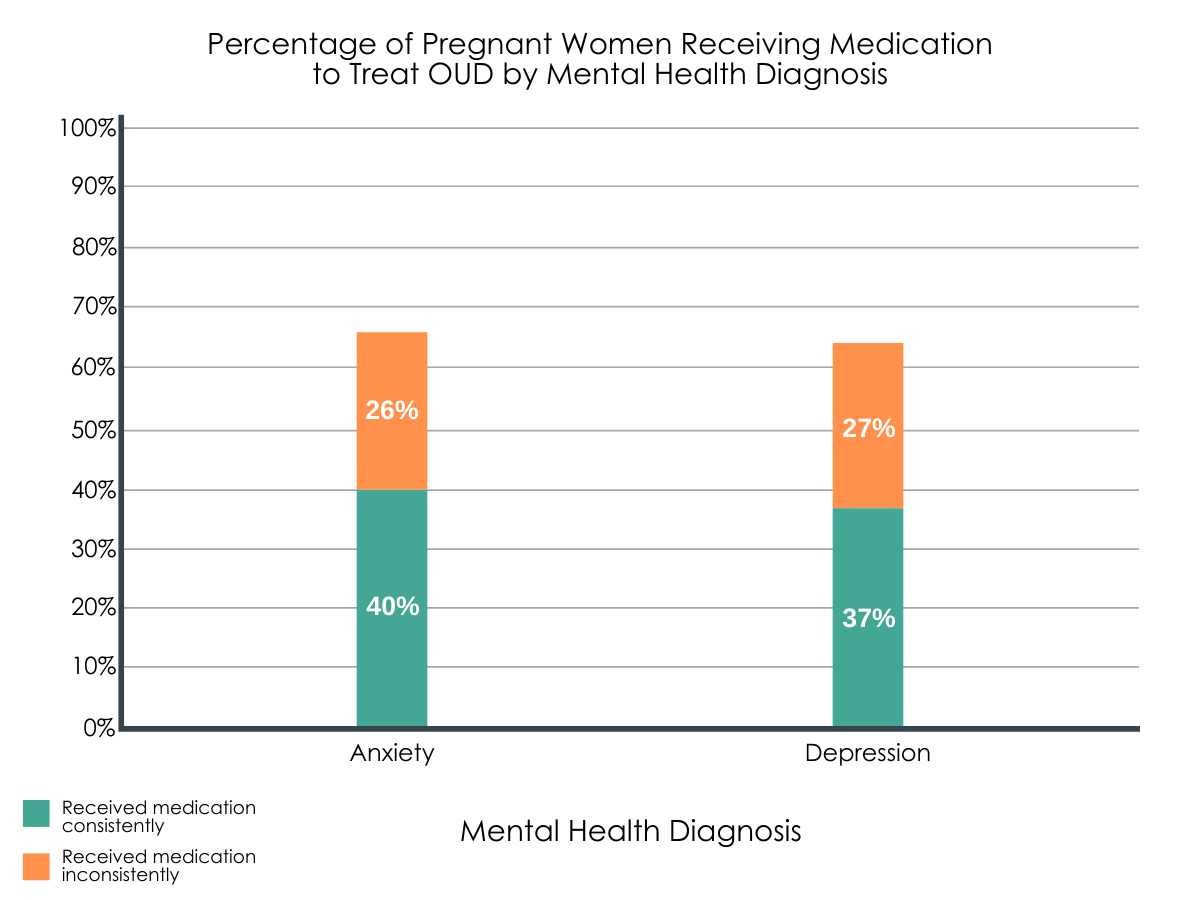
Figure 1, 2, 3. The full bars represent the total percentage of women in each category who received OUD medication, with a further breakdown within the bar of the consistency of that medication delivery. Consistent = monthly medication receipt; Inconsistent = received medication in the year before delivery but missing 1 or more treatment months.
Maternal race/ethnicity predicted medication treatment receipt, but it only explained a small amount of the differences.
White non-Hispanic women were more likely to have a diagnosis of OUD than black non-Hispanic or Hispanic women. Black non-Hispanic and Hispanic women were significantly less likely to receive any medication for the treatment of OUD or to consistently use medication to treat OUD in the 6 months before delivery, with and without adjusting for other maternal characteristics. When examining receipt of buprenorphine versus methadone, Black women were less likely than White women to receive buprenorphine, even after adjusting statistically for the set of control variables. Yet, race/ethnicity only explained 3% of the difference in medication receipt (use and type), indicating there are other important factors involved in OUD medication use among pregnant women.
Maternal age and mental health are important predictors of the extent and type of OUD medication treatment receipt.
When authors examined racial/ethnic differences in OUD medication practices by age, they found differences were greatest among the youngest participants. That is, for women 25 years and younger, black non-Hispanic and Hispanic women were less likely than white non-Hispanic women to receive any medication for OUD treatment. Alternatively, although black non-Hispanic and Hispanic women aged 26 or greater were still less likely than white non-Hispanic women to receive medication for OUD treatment, their likelihood doubled compared to younger women.
Figure 2.
When examining the extent of medication use and type of medication used to treat OUD, the differences between races for individuals with depression or anxiety were less substantial, suggesting that, among pregnant women with co-occurring psychiatric disorders, racial/ethnic differences between White, Black, and Hispanic women are not as pronounced.
Figure 3. These categories only include women in the study population who have received a diagnosis for anxiety or depression.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that there are differences between racial/ethnic groups in the use of medications to treat OUD during pregnancy and that black non-Hispanic and Hispanic women were significantly less likely to use medications consistently or at all compared with white non-Hispanic women. However, the study also identified other factors, such as maternal age and mental health that were also important to OUD medication treatment receipt during pregnancy.
There are significant gaps in OUD medication treatment for pregnant women; a third of the sample had not received any OUD medication treatment. There are also racial/ethnic differences in OUD medication treatment receipt and the exact causes of these differences are unknown. Although research has indicated that black individuals have not experienced an increase in access to buprenorphine on the same scale as white individuals, other evidence suggests factors aside from race/ethnicity are important, such as maternal age, which could be a result of difficulty retaining younger women in treatment. Yet, there may also be cultural factors influencing the use and receipt of OUD medication treatment such as cultural beliefs around the appropriateness of using drugs to treat substance use or instead relying on other traditional or faith-based practices for treatment. Furthermore, due to negative historical experiences among minorities in the healthcare system, some individuals may mistrust the healthcare system, and in parallel, any medications prescribed by health care providers, leading to less engagement in OUD medication treatment. Depending on the prescribing options available at the clinical locations these women attend, there may also be differences based on medication modality; buprenorphine is often prescribed in office settings and allow longer intervals between visits whereas methadone involves daily clinical visits. These different modalities may make it more difficult for women to be willing to engage in this treatment or to be retained, especially if accessing medication interferes with other necessary life tasks like keeping regular work hours.
The design of this study does not allow for conclusions to be drawn about why black and Hispanic pregnant women have different OUD medication patterns, and further research that delves into their unique experiences and perspectives from a qualitative perspective, are important next steps. Finally, because women with a diagnosis of depression or anxiety were less likely to experience gaps in medication use, it seems that this group may be better linked to the healthcare system overall and receiving better care during their pregnancy, regardless of their race/ethnicity.
As this study analyzed public health data from one state, the findings from this study may not generalize to samples located in other states/geographic areas.
The authors’ identification of women with OUD may have missed some women, for example, individuals outside the public addiction treatment system.
Because this was an analysis of treatment and payer system data, the study was only able to capture whether pregnant women received OUD medication and not whether they actually took it.
The dataset lacks information on potential comorbid diagnoses aside from anxiety and depression, and so there could be other diagnoses (e.g., additional substance use disorders) influencing OUD medication treatment receipt that these analyses do not capture.
BOTTOM LINE
For individuals and families seeking recovery: This study used public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically supported medicines buprenorphine or methadone. The study also found that these differences were greater among younger women (i.e., much less likely to get a prescription) and were lower among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. It is likely that additional education and outreach that relays the benefits and safety of medication treatment for OUD during pregnancy may improve access and engagement in these services; as well, identifying and linking women with OUD treatment services early in their pregnancy may help improve outcomes for mothers and their babies. There is also a need for clinical systems and staff who serve minority women to actively implement strategies to understand and address perceived barriers to use of medication to treat OUD during pregnancy.
For treatment professionals and treatment systems: This study used public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically-supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. It is likely that attention to education and outreach by doctors and hospitals in the public health system who see these women to relay the benefits and safety of medication treatment for OUD during pregnancy may improve access and engagement in these services. Given stereotypes and negative stigma of medication for OUD treatment during pregnancy, training on approaching these conversations with pregnant women may also help with engagement. Identifying and linking women with these services early in their pregnancy may help improve outcomes for mothers and their babies. There is also a need for clinical systems and staff who serve minority women to actively implement strategies to address perceived barriers to use of medication to treat OUD during pregnancy. For example, the use of culturally sensitive patient-centered approaches may assist with increasing medication use.
For scientists:This study examined public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically-supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. However, the findings also indicate that race/ethnicity is only a modest predictor of OUD medication treatment engagement and so there is a need to better understand why many pregnant women with OUD are not receiving OUD medication treatment and why this difference persists for young women and between different racial/ethnic groups. Additional attention to contextual factors may be necessary as there may be historical or cultural reasons that certain racial/ethnic groups are less likely to engage in medication treatment for OUD. Furthermore, attention to the key stakeholders in the public health treatment system to better understand whether and how conversations with patients around medication for OUD treatment occur, may shed identify additional barriers to OUD medication access and engagement.
For policy makers: This study examined public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. There is a need to better understand why pregnant women with OUD are not receiving OUD medication treatment and why this difference persists for young women and between different racial/ethnic groups. Funding to address research within the healthcare system and for examination of particular groups of patients with reduced access may be necessary to highlight areas for potential intervention. In addition, funding to improve provider training to reduce stereotypes and negative stigma of medication for OUD treatment during pregnancy, may also address the gap in access between individuals.
Opioid use disorder (OUD) has increased among pregnant women and can result in a variety of negative outcomes for women and their children including preterm labor, stillbirth, neonatal abstinence syndrome, or maternal fatality. Evidence demonstrates that medication, such as methadone or buprenorphine, can be used successfully to treat OUD among pregnant women and improve health for mothers and their babies; yet, many pregnant women do not receive this treatment. Many factors influence whether an individual is offered and/or accepts OUD medications. Such factors include availability and clinical training for medication prescriptions, insurance coverage of these services, access to providers by geographic location, and stigma or misunderstanding about using medications for OUD treatment. Like other SUD treatments, these factors in uptake suggest racial/ethnic minorities may be less likely to receive these empirically supported OUD medicines. In this study, researchers examined whether a pregnant woman’s race/ethnicity resulted in several different outcomes of OUD medication treatment receipt including whether race/ethnicity affected patterns and duration of medication receipt to treat OUD and what types of medication were used.
HOW WAS THIS STUDY CONDUCTED?
This study was secondary data analysis of a statewide linked data set in Massachusetts (Public Health Data Warehouse), that is, a dataset combined from several public health datasets. The dataset captured over 270,000 live baby deliveries in Massachusetts between October 2011 and December 2015; of these, 5247 births were to women with OUD who were either of non-Hispanic White, Black, or Hispanic race/ethnicity and this is the subset of women who were included in this study’s analytic sample. In addition to participant characteristics (age, race/ethnicity), the dataset included treatment receipt, addiction treatment records, and data from the prescription monitoring program for these women for the nine months prior to the birth of a baby. The authors examined whether any of these three experiences varied by maternal race/ethnicity: (1) Use of any medication to treat OUD; (2) An individual’s extent of use of medication to treat OUD (using three categories which included inconsistent, consistent, and none; see paragraph below for more details); (3) The type of medication (buprenorphine, methadone) used to treat OUD.
The primary variables in the analysis were maternal race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic). Consistent use of medication to treat OUD was defined as monthly receipt for at least 6 months of treatment before delivery while inconsistent use of medication was defined as any medication to treat OUD in the year before delivery but with gaps in treatment months. The authors also used several control variables in the analysis to isolate the relationships between race/ethnicity and their questions of OUD medication treatment receipt. These variables included maternal age at delivery, maternal education, enrollment in Medicaid, marital status, geographic location of residence (rural/non-rural), maternal diagnosis of depression or anxiety, incarceration, homelessness, high use of unscheduled care, and adequacy of prenatal care based on the Kotelchuck index.
Of note, the authors identified women with OUD using the following indicators from the linked dataset: (1) a diagnosis of OUD from hospital discharge or all-payer claims database records; (2) an opioid overdose event from claims or ambulance data; (3) enrollment in a state-funded treatment program for an opioid problem; (4) receipt of methadone or buprenorphine treatment; or (5) an insurance claim for an infant diagnosis of neonatal abstinence syndrome (NAS). Mothers who were identified only by a NAS infant diagnosis were excluded if they had an opioid prescription in the 3 months before delivery or if their child was born at or before 34 weeks gestation to prevent misclassification of women with chronic pain and iatrogenic cases of NAS.
Study participants were the 5247 women with OUD who had delivered a baby in Massachusetts between October 2011 and December 2015. The average age of mothers at delivery was 29 years old. Most of the sample were white non-Hispanic (4551, 86.7%), while smaller numbers of women were Hispanic (462, 8.8%) and black non-Hispanic (234, 4.5%).
WHAT DID THIS STUDY FIND?
A majority, but not all women received medication to treat OUD during pregnancy and consistent receipt of medication was low across all racial/ethnic groups.
Two-thirds (66%) of women received medication to treat OUD during pregnancy, yet only 58% of these were consistent in their receipt of this medication. This finding indicates that in fact only 38% of women consistently received medication to treat OUD during pregnancy, while 28% had inconsistent medication receipt.
Figure 1, 2, 3. The full bars represent the total percentage of women in each category who received OUD medication, with a further breakdown within the bar of the consistency of that medication delivery. Consistent = monthly medication receipt; Inconsistent = received medication in the year before delivery but missing 1 or more treatment months.
Maternal race/ethnicity predicted medication treatment receipt, but it only explained a small amount of the differences.
White non-Hispanic women were more likely to have a diagnosis of OUD than black non-Hispanic or Hispanic women. Black non-Hispanic and Hispanic women were significantly less likely to receive any medication for the treatment of OUD or to consistently use medication to treat OUD in the 6 months before delivery, with and without adjusting for other maternal characteristics. When examining receipt of buprenorphine versus methadone, Black women were less likely than White women to receive buprenorphine, even after adjusting statistically for the set of control variables. Yet, race/ethnicity only explained 3% of the difference in medication receipt (use and type), indicating there are other important factors involved in OUD medication use among pregnant women.
Maternal age and mental health are important predictors of the extent and type of OUD medication treatment receipt.
When authors examined racial/ethnic differences in OUD medication practices by age, they found differences were greatest among the youngest participants. That is, for women 25 years and younger, black non-Hispanic and Hispanic women were less likely than white non-Hispanic women to receive any medication for OUD treatment. Alternatively, although black non-Hispanic and Hispanic women aged 26 or greater were still less likely than white non-Hispanic women to receive medication for OUD treatment, their likelihood doubled compared to younger women.
Figure 2.
When examining the extent of medication use and type of medication used to treat OUD, the differences between races for individuals with depression or anxiety were less substantial, suggesting that, among pregnant women with co-occurring psychiatric disorders, racial/ethnic differences between White, Black, and Hispanic women are not as pronounced.
Figure 3. These categories only include women in the study population who have received a diagnosis for anxiety or depression.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that there are differences between racial/ethnic groups in the use of medications to treat OUD during pregnancy and that black non-Hispanic and Hispanic women were significantly less likely to use medications consistently or at all compared with white non-Hispanic women. However, the study also identified other factors, such as maternal age and mental health that were also important to OUD medication treatment receipt during pregnancy.
There are significant gaps in OUD medication treatment for pregnant women; a third of the sample had not received any OUD medication treatment. There are also racial/ethnic differences in OUD medication treatment receipt and the exact causes of these differences are unknown. Although research has indicated that black individuals have not experienced an increase in access to buprenorphine on the same scale as white individuals, other evidence suggests factors aside from race/ethnicity are important, such as maternal age, which could be a result of difficulty retaining younger women in treatment. Yet, there may also be cultural factors influencing the use and receipt of OUD medication treatment such as cultural beliefs around the appropriateness of using drugs to treat substance use or instead relying on other traditional or faith-based practices for treatment. Furthermore, due to negative historical experiences among minorities in the healthcare system, some individuals may mistrust the healthcare system, and in parallel, any medications prescribed by health care providers, leading to less engagement in OUD medication treatment. Depending on the prescribing options available at the clinical locations these women attend, there may also be differences based on medication modality; buprenorphine is often prescribed in office settings and allow longer intervals between visits whereas methadone involves daily clinical visits. These different modalities may make it more difficult for women to be willing to engage in this treatment or to be retained, especially if accessing medication interferes with other necessary life tasks like keeping regular work hours.
The design of this study does not allow for conclusions to be drawn about why black and Hispanic pregnant women have different OUD medication patterns, and further research that delves into their unique experiences and perspectives from a qualitative perspective, are important next steps. Finally, because women with a diagnosis of depression or anxiety were less likely to experience gaps in medication use, it seems that this group may be better linked to the healthcare system overall and receiving better care during their pregnancy, regardless of their race/ethnicity.
As this study analyzed public health data from one state, the findings from this study may not generalize to samples located in other states/geographic areas.
The authors’ identification of women with OUD may have missed some women, for example, individuals outside the public addiction treatment system.
Because this was an analysis of treatment and payer system data, the study was only able to capture whether pregnant women received OUD medication and not whether they actually took it.
The dataset lacks information on potential comorbid diagnoses aside from anxiety and depression, and so there could be other diagnoses (e.g., additional substance use disorders) influencing OUD medication treatment receipt that these analyses do not capture.
BOTTOM LINE
For individuals and families seeking recovery: This study used public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically supported medicines buprenorphine or methadone. The study also found that these differences were greater among younger women (i.e., much less likely to get a prescription) and were lower among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. It is likely that additional education and outreach that relays the benefits and safety of medication treatment for OUD during pregnancy may improve access and engagement in these services; as well, identifying and linking women with OUD treatment services early in their pregnancy may help improve outcomes for mothers and their babies. There is also a need for clinical systems and staff who serve minority women to actively implement strategies to understand and address perceived barriers to use of medication to treat OUD during pregnancy.
For treatment professionals and treatment systems: This study used public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically-supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. It is likely that attention to education and outreach by doctors and hospitals in the public health system who see these women to relay the benefits and safety of medication treatment for OUD during pregnancy may improve access and engagement in these services. Given stereotypes and negative stigma of medication for OUD treatment during pregnancy, training on approaching these conversations with pregnant women may also help with engagement. Identifying and linking women with these services early in their pregnancy may help improve outcomes for mothers and their babies. There is also a need for clinical systems and staff who serve minority women to actively implement strategies to address perceived barriers to use of medication to treat OUD during pregnancy. For example, the use of culturally sensitive patient-centered approaches may assist with increasing medication use.
For scientists:This study examined public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically-supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. However, the findings also indicate that race/ethnicity is only a modest predictor of OUD medication treatment engagement and so there is a need to better understand why many pregnant women with OUD are not receiving OUD medication treatment and why this difference persists for young women and between different racial/ethnic groups. Additional attention to contextual factors may be necessary as there may be historical or cultural reasons that certain racial/ethnic groups are less likely to engage in medication treatment for OUD. Furthermore, attention to the key stakeholders in the public health treatment system to better understand whether and how conversations with patients around medication for OUD treatment occur, may shed identify additional barriers to OUD medication access and engagement.
For policy makers: This study examined public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. There is a need to better understand why pregnant women with OUD are not receiving OUD medication treatment and why this difference persists for young women and between different racial/ethnic groups. Funding to address research within the healthcare system and for examination of particular groups of patients with reduced access may be necessary to highlight areas for potential intervention. In addition, funding to improve provider training to reduce stereotypes and negative stigma of medication for OUD treatment during pregnancy, may also address the gap in access between individuals.
Opioid use disorder (OUD) has increased among pregnant women and can result in a variety of negative outcomes for women and their children including preterm labor, stillbirth, neonatal abstinence syndrome, or maternal fatality. Evidence demonstrates that medication, such as methadone or buprenorphine, can be used successfully to treat OUD among pregnant women and improve health for mothers and their babies; yet, many pregnant women do not receive this treatment. Many factors influence whether an individual is offered and/or accepts OUD medications. Such factors include availability and clinical training for medication prescriptions, insurance coverage of these services, access to providers by geographic location, and stigma or misunderstanding about using medications for OUD treatment. Like other SUD treatments, these factors in uptake suggest racial/ethnic minorities may be less likely to receive these empirically supported OUD medicines. In this study, researchers examined whether a pregnant woman’s race/ethnicity resulted in several different outcomes of OUD medication treatment receipt including whether race/ethnicity affected patterns and duration of medication receipt to treat OUD and what types of medication were used.
HOW WAS THIS STUDY CONDUCTED?
This study was secondary data analysis of a statewide linked data set in Massachusetts (Public Health Data Warehouse), that is, a dataset combined from several public health datasets. The dataset captured over 270,000 live baby deliveries in Massachusetts between October 2011 and December 2015; of these, 5247 births were to women with OUD who were either of non-Hispanic White, Black, or Hispanic race/ethnicity and this is the subset of women who were included in this study’s analytic sample. In addition to participant characteristics (age, race/ethnicity), the dataset included treatment receipt, addiction treatment records, and data from the prescription monitoring program for these women for the nine months prior to the birth of a baby. The authors examined whether any of these three experiences varied by maternal race/ethnicity: (1) Use of any medication to treat OUD; (2) An individual’s extent of use of medication to treat OUD (using three categories which included inconsistent, consistent, and none; see paragraph below for more details); (3) The type of medication (buprenorphine, methadone) used to treat OUD.
The primary variables in the analysis were maternal race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic). Consistent use of medication to treat OUD was defined as monthly receipt for at least 6 months of treatment before delivery while inconsistent use of medication was defined as any medication to treat OUD in the year before delivery but with gaps in treatment months. The authors also used several control variables in the analysis to isolate the relationships between race/ethnicity and their questions of OUD medication treatment receipt. These variables included maternal age at delivery, maternal education, enrollment in Medicaid, marital status, geographic location of residence (rural/non-rural), maternal diagnosis of depression or anxiety, incarceration, homelessness, high use of unscheduled care, and adequacy of prenatal care based on the Kotelchuck index.
Of note, the authors identified women with OUD using the following indicators from the linked dataset: (1) a diagnosis of OUD from hospital discharge or all-payer claims database records; (2) an opioid overdose event from claims or ambulance data; (3) enrollment in a state-funded treatment program for an opioid problem; (4) receipt of methadone or buprenorphine treatment; or (5) an insurance claim for an infant diagnosis of neonatal abstinence syndrome (NAS). Mothers who were identified only by a NAS infant diagnosis were excluded if they had an opioid prescription in the 3 months before delivery or if their child was born at or before 34 weeks gestation to prevent misclassification of women with chronic pain and iatrogenic cases of NAS.
Study participants were the 5247 women with OUD who had delivered a baby in Massachusetts between October 2011 and December 2015. The average age of mothers at delivery was 29 years old. Most of the sample were white non-Hispanic (4551, 86.7%), while smaller numbers of women were Hispanic (462, 8.8%) and black non-Hispanic (234, 4.5%).
WHAT DID THIS STUDY FIND?
A majority, but not all women received medication to treat OUD during pregnancy and consistent receipt of medication was low across all racial/ethnic groups.
Two-thirds (66%) of women received medication to treat OUD during pregnancy, yet only 58% of these were consistent in their receipt of this medication. This finding indicates that in fact only 38% of women consistently received medication to treat OUD during pregnancy, while 28% had inconsistent medication receipt.
Figure 1, 2, 3. The full bars represent the total percentage of women in each category who received OUD medication, with a further breakdown within the bar of the consistency of that medication delivery. Consistent = monthly medication receipt; Inconsistent = received medication in the year before delivery but missing 1 or more treatment months.
Maternal race/ethnicity predicted medication treatment receipt, but it only explained a small amount of the differences.
White non-Hispanic women were more likely to have a diagnosis of OUD than black non-Hispanic or Hispanic women. Black non-Hispanic and Hispanic women were significantly less likely to receive any medication for the treatment of OUD or to consistently use medication to treat OUD in the 6 months before delivery, with and without adjusting for other maternal characteristics. When examining receipt of buprenorphine versus methadone, Black women were less likely than White women to receive buprenorphine, even after adjusting statistically for the set of control variables. Yet, race/ethnicity only explained 3% of the difference in medication receipt (use and type), indicating there are other important factors involved in OUD medication use among pregnant women.
Maternal age and mental health are important predictors of the extent and type of OUD medication treatment receipt.
When authors examined racial/ethnic differences in OUD medication practices by age, they found differences were greatest among the youngest participants. That is, for women 25 years and younger, black non-Hispanic and Hispanic women were less likely than white non-Hispanic women to receive any medication for OUD treatment. Alternatively, although black non-Hispanic and Hispanic women aged 26 or greater were still less likely than white non-Hispanic women to receive medication for OUD treatment, their likelihood doubled compared to younger women.
Figure 2.
When examining the extent of medication use and type of medication used to treat OUD, the differences between races for individuals with depression or anxiety were less substantial, suggesting that, among pregnant women with co-occurring psychiatric disorders, racial/ethnic differences between White, Black, and Hispanic women are not as pronounced.
Figure 3. These categories only include women in the study population who have received a diagnosis for anxiety or depression.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that there are differences between racial/ethnic groups in the use of medications to treat OUD during pregnancy and that black non-Hispanic and Hispanic women were significantly less likely to use medications consistently or at all compared with white non-Hispanic women. However, the study also identified other factors, such as maternal age and mental health that were also important to OUD medication treatment receipt during pregnancy.
There are significant gaps in OUD medication treatment for pregnant women; a third of the sample had not received any OUD medication treatment. There are also racial/ethnic differences in OUD medication treatment receipt and the exact causes of these differences are unknown. Although research has indicated that black individuals have not experienced an increase in access to buprenorphine on the same scale as white individuals, other evidence suggests factors aside from race/ethnicity are important, such as maternal age, which could be a result of difficulty retaining younger women in treatment. Yet, there may also be cultural factors influencing the use and receipt of OUD medication treatment such as cultural beliefs around the appropriateness of using drugs to treat substance use or instead relying on other traditional or faith-based practices for treatment. Furthermore, due to negative historical experiences among minorities in the healthcare system, some individuals may mistrust the healthcare system, and in parallel, any medications prescribed by health care providers, leading to less engagement in OUD medication treatment. Depending on the prescribing options available at the clinical locations these women attend, there may also be differences based on medication modality; buprenorphine is often prescribed in office settings and allow longer intervals between visits whereas methadone involves daily clinical visits. These different modalities may make it more difficult for women to be willing to engage in this treatment or to be retained, especially if accessing medication interferes with other necessary life tasks like keeping regular work hours.
The design of this study does not allow for conclusions to be drawn about why black and Hispanic pregnant women have different OUD medication patterns, and further research that delves into their unique experiences and perspectives from a qualitative perspective, are important next steps. Finally, because women with a diagnosis of depression or anxiety were less likely to experience gaps in medication use, it seems that this group may be better linked to the healthcare system overall and receiving better care during their pregnancy, regardless of their race/ethnicity.
As this study analyzed public health data from one state, the findings from this study may not generalize to samples located in other states/geographic areas.
The authors’ identification of women with OUD may have missed some women, for example, individuals outside the public addiction treatment system.
Because this was an analysis of treatment and payer system data, the study was only able to capture whether pregnant women received OUD medication and not whether they actually took it.
The dataset lacks information on potential comorbid diagnoses aside from anxiety and depression, and so there could be other diagnoses (e.g., additional substance use disorders) influencing OUD medication treatment receipt that these analyses do not capture.
BOTTOM LINE
For individuals and families seeking recovery: This study used public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically supported medicines buprenorphine or methadone. The study also found that these differences were greater among younger women (i.e., much less likely to get a prescription) and were lower among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. It is likely that additional education and outreach that relays the benefits and safety of medication treatment for OUD during pregnancy may improve access and engagement in these services; as well, identifying and linking women with OUD treatment services early in their pregnancy may help improve outcomes for mothers and their babies. There is also a need for clinical systems and staff who serve minority women to actively implement strategies to understand and address perceived barriers to use of medication to treat OUD during pregnancy.
For treatment professionals and treatment systems: This study used public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically-supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. It is likely that attention to education and outreach by doctors and hospitals in the public health system who see these women to relay the benefits and safety of medication treatment for OUD during pregnancy may improve access and engagement in these services. Given stereotypes and negative stigma of medication for OUD treatment during pregnancy, training on approaching these conversations with pregnant women may also help with engagement. Identifying and linking women with these services early in their pregnancy may help improve outcomes for mothers and their babies. There is also a need for clinical systems and staff who serve minority women to actively implement strategies to address perceived barriers to use of medication to treat OUD during pregnancy. For example, the use of culturally sensitive patient-centered approaches may assist with increasing medication use.
For scientists:This study examined public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically-supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. However, the findings also indicate that race/ethnicity is only a modest predictor of OUD medication treatment engagement and so there is a need to better understand why many pregnant women with OUD are not receiving OUD medication treatment and why this difference persists for young women and between different racial/ethnic groups. Additional attention to contextual factors may be necessary as there may be historical or cultural reasons that certain racial/ethnic groups are less likely to engage in medication treatment for OUD. Furthermore, attention to the key stakeholders in the public health treatment system to better understand whether and how conversations with patients around medication for OUD treatment occur, may shed identify additional barriers to OUD medication access and engagement.
For policy makers: This study examined public health data of women who delivered a baby in Massachusetts between 2011 and 2015 and found that Black and Hispanic women with opioid use disorder (OUD) were less likely than White women to receive a prescription for the empirically supported medicines buprenorphine or methadone. The study also found that these disparities were amplified among younger women (i.e., much less likely to get a prescription) and muted among those with mental health difficulties like depression and anxiety (i.e., much more likely to get a prescription). These findings indicate that despite the benefits to pregnant women with OUD, many women are not receiving medication treatment to address OUD during pregnancy and this difference is more pronounced for younger mothers and for black non-Hispanic and Hispanic women. There is a need to better understand why pregnant women with OUD are not receiving OUD medication treatment and why this difference persists for young women and between different racial/ethnic groups. Funding to address research within the healthcare system and for examination of particular groups of patients with reduced access may be necessary to highlight areas for potential intervention. In addition, funding to improve provider training to reduce stereotypes and negative stigma of medication for OUD treatment during pregnancy, may also address the gap in access between individuals.