Mindfulness trait may buffer negative effects of trauma for women
Women in substance use disorder treatment report exposure to traumatic events more often than men, and trauma is linked to more craving and worse outcomes. Addressing the consequences of trauma can help to improve substance use and other outcomes and “mindfulness” has been shown to help. This study investigated if exposure to traumatic events is associated with drug craving among women in treatment, and if mindfulness buffers this relationship. It also examined whether the historical timing of traumatic exposure influenced the degree of traumatic symptoms and craving.
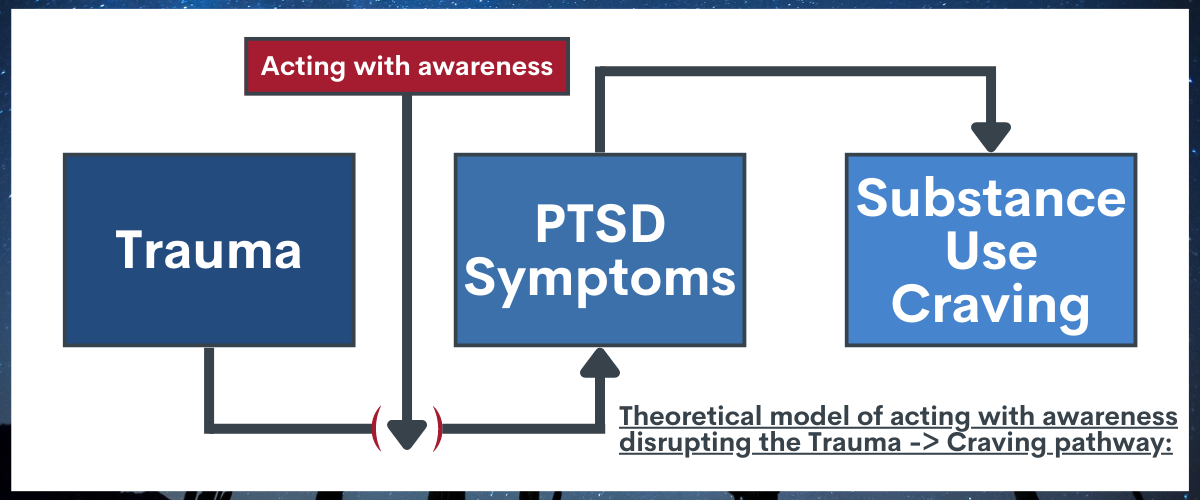
The researchers in this study hypothesized that the symptoms associated with PTSD, such as intrusive memories and increased arousal to a stressor, may be associated with craving, which in turn can increase the risk of substance use. If an individual is experiencing trauma symptoms, they have less capacity to cope with day-to-day stressors and thus experience more craving. Because women in SUD treatment report higher rates of trauma, determining if trauma exposure is associated with craving could help clinicians and researchers identify a target for future treatments. Furthermore, identifying the effect of when trauma occurs could also help provide appropriate treatment. An intervention that buffers the effect of trauma on craving consequently could increase treatment success and improve health and wellness of women with a substance use disorder who have experienced trauma across the life course.
Although a history of trauma cannot be changed, there may be modifiable traits such as mindfulness that may buffer the negative effects of trauma. Mindfulness is an approach to paying attention that is focused on the present moment with compassion and without judgement or reaction. One meta-analysis, examining the results of many studies at once, found that those with more mindfulness had fewer substance use behaviors (e.g., fewer substance use problems, lower levels of substance use), although the size of this relationship was small. However, the meta-analysis also found that the relationship between mindfulness and substance use behaviors may be stronger for some. For example, the relationship is stronger for more severe inpatients versus outpatients and non-clinical samples. Although mindfulness-based relapse prevention treatments shows some promise to improving treatment outcomes, the time and effort required to train clinicians may limit the cost-benefit ratio of the intervention. Yet, if mindfulness buffers the effects of specific factors of substance use behaviors (i.e., craving) for those with heightened craving (i.e., women with a history of trauma), then mindfulness may be a viable target in specific instances. The relationship between mindfulness and trauma may also depend on when the trauma was experienced (childhood, adulthood, or both). Understanding if and when trauma occurs as well as who may benefit from mindfulness training could improve clinicians’ ability align patient needs and treatments, which could improve treatment effectiveness.
This study aimed to determine if trauma exposure at different times during the life course (i.e., childhood, adulthood, or both) is linked with PTSD symptoms and craving. The study also sought to determine if mindfulness buffered this relationship.
HOW WAS THIS STUDY CONDUCTED?
This cross-sectional study (i.e., where individuals are measured at only one time point) included 245 women receiving treatment for a substance use disorder. Women were eligible to participate if they were 18-65 years old, had a substance use disorder diagnosis, did not have an untreated psychotic disorder or severe chronic mental health condition, had not reported suicidality in the last 30 days, were not more than 6 months pregnant, and were enrolled in the gender-specific residential treatment program.
All women were asked about their exposure to trauma, when the exposure occurred, current PTSD symptoms and their severity, alcohol and drug craving, addiction severity, and mindfulness. Exposure to trauma was classified as yes or no based on responding yes to at least one experience of sexual, physical, and emotional trauma (e.g., “Were you ever abused or physically attacked [not sexually] by someone you knew [for example, a parent, boyfriend, or husband hit, slapped, choked, burned, or beat you up]?). The developmental period of exposure was classified as childhood (17 years old or younger), adulthood (18 years old or older), both, or neither. A post-traumatic stress disorder scale was used to calculate a trauma symptom severity score, and a scale that combined measures of frequency, intensity, and duration of craving for both alcohol and other drugs was also used. The posttraumatic symptom severity score can range from 0-51. The symptom severity ratings are: 0 = none; 1–10 = mild, 11–20 = moderate, 21–35 = moderate to severe, and >35 = severe. The craving scale consisted of five items that each range from 0 to 6, with a higher average score representing higher levels (i.e., more severe) alcohol and drug craving. Mindfulness was measured in a way that featured an overall trait mindfulness score as well as scores across five subscales of mindfulness: observing, describing, acting with awareness, nonjudgmental acceptance, and non-reactivity. Addiction severity, education, race/ethnicity, gender, and housing status was also measured.
A total of 245 women participated in the study. Most identified as Hispanic (58%) with about 21% and 21% identifying as non-Hispanic White and non-Hispanic Black, respectively. Almost half (48%) had not completed high school, and 23% were experiencing homelessness. Although 18% did not have any children, 48% had minor children but did not have custody. Additionally, 74% of the women were never married. Most (76%) of the women had a drug use disorder only, 10% had alcohol use disorder only, and 14% had both. About half (58%) had a mental health diagnosis other than a substance use disorder, with 27% having post-traumatic stress disorder. Methamphetamine was the most common substance used in the 8 months prior to treatment entry, followed by marijuana and alcohol-to-intoxication.
WHAT DID THIS STUDY FIND?
Presence and chronicity of traumatic incidents associated with craving.
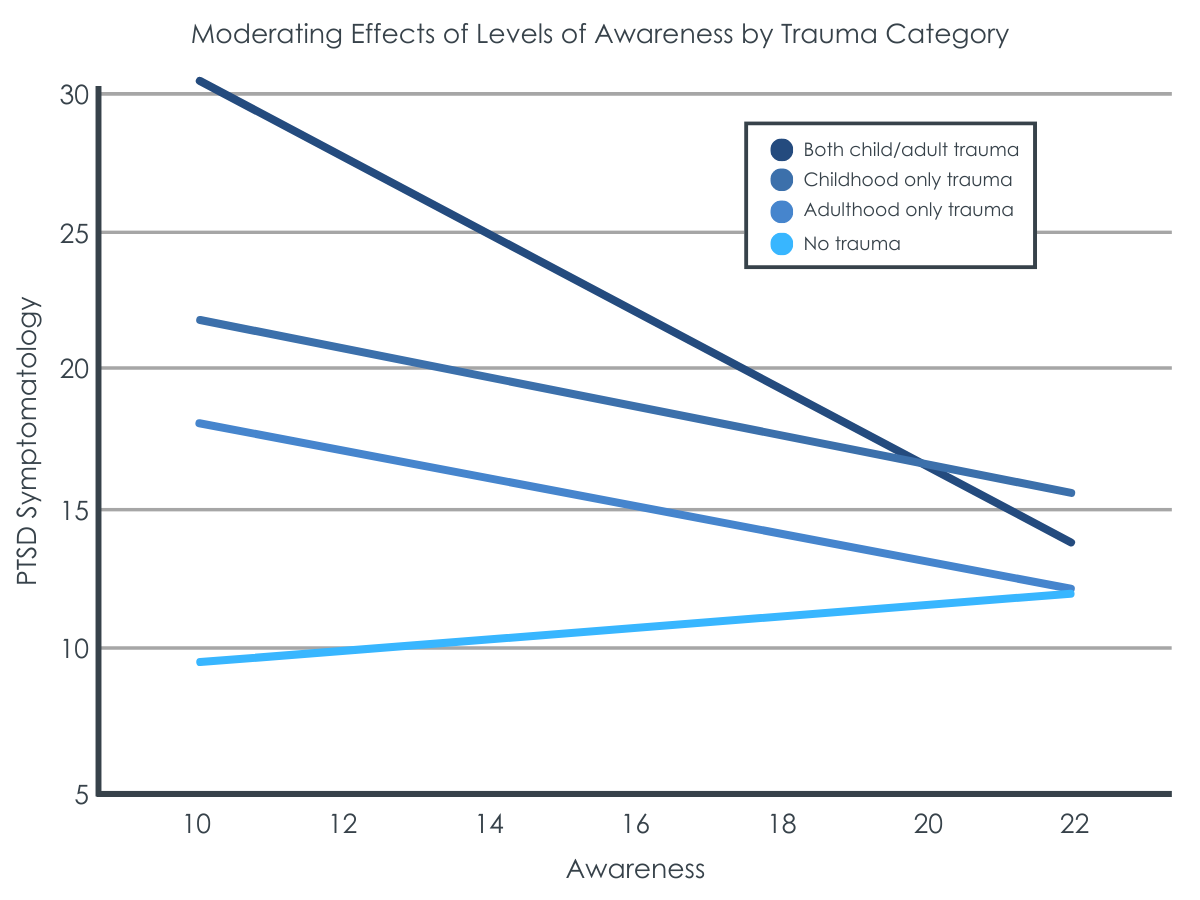
Women who reported trauma exposure during childhood as well as in adulthood reported worse trauma symptoms compared to those that reported no trauma or trauma only in adulthood. Women who reported trauma incident(s) in both childhood and adulthood and those who reported trauma incident(s) only in childhood reported similar trauma symptom severity. The average trauma symptom severity score for women who reported trauma incidents) in both childhood and adulthood was 21.01. Yet, those who reported no trauma only had an average of 10.13, and those with trauma incident(s) only in adulthood had an average of 12.07. Women with only childhood trauma incident(s) had an average severity score of 18.63, which was considerably more than no trauma and adulthood only but not meaningfully different from those with both childhood and adulthood trauma.
Trauma symptomology was directly associated with higher levels of craving. Furthermore, compared to women experiencing traumatic incidents during both childhood and adulthood, those with no experiences and experiences in adulthood only had lower levels of substance use craving, associated with their lower trauma symptom severity.
Acting with awareness buffered the negative effect of trauma and craving.
In this study, mindfulness was considered to have five different components, with acting with awareness as one of them. Although overall trait mindfulness was not linked with changes in the relationship between time of trauma exposure and trauma symptom severity, acting with awareness was associated with that relationship. Acting with awareness was related with a weaker relationship between trauma symptoms and craving. At low levels of awareness, women with trauma exposure in both childhood and adulthood reported more trauma symptomology compared to childhood only, adulthood only, and no exposure. As awareness level increased, this relationship diminished. At high levels of awareness, there were no differences in trauma symptom severity across the developmental groups.
At low levels of awareness, women with exposure to trauma during both childhood and adulthood reported more craving resulting from worse trauma symptom severity compared to all other groups. At average awareness, women with no trauma and adulthood only trauma reported more craving as their trauma symptom severity increased. At high levels of awareness, there were no differences in the relationships between craving and trauma symptom severity across groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Overall, this study found that women experiencing trauma during both childhood and adulthood report more post-traumatic stress disorder (PTSD) symptoms, which is also associated with greater craving. Also, the relationship between trauma symptoms and substance use craving appeared to be buffered by mindfulness abilities. Studies like this help us understand mechanisms that could benefit from further research and that may be targeted to improve treatment outcomes and the chances of recovery, particularly for vulnerable populations such as women who have experienced trauma.
This study identified a potential causal chain of events—trauma exposure to trauma symptoms to craving—that possibly may be interrupted to improve treatment for women in substance use disorder treatment. However, given the cross-sectional nature of the study (i.e., questions only asked at one point in time) more research is needed to clarify these causal connections. Also, overall trait mindfulness did not alter the relationship between trauma symptoms and craving.
Trauma can alter a person’s ability to cope with stressors and thus increases the likelihood of seeking substances to alleviate stress. The past year prevalence of PTSD for women is more than double that of men (5.2% vs. 1.8%). Thus, pinpointing a mechanism to target that involves trauma may be especially important for women. Furthermore, this study highlighted that when trauma occurs may be important. Women who experienced trauma during both childhood and adulthood appeared to fare worse than those who experienced trauma only during adulthood or not at all. This finding suggests that screening for when the exposure to the traumatic incident(s) occurred in addition to if it/they occurred may help identify women who may be at increased risk for relapse.
One aspect of mindfulness—acting with awareness—was found to mitigate the relationship between trauma and craving regardless of when trauma was experienced. Acting with awareness is focusing on one’s activities in the moment instead of operating on autopilot. Women reporting high levels of mindful awareness, and who were exposed to traumatic incidents during childhood or adulthood and those not exposed to trauma reported no more craving than those exposed to traumatic incidents during both childhood and adulthood.
Mindfulness-based trainings, specifically those targeting acting with awareness, warrant future study to explore if it can help buffer the negative effects of trauma and improve recovery chances. Mindfulness-based relapse prevention is one type of therapy that aims to do this. Although some findings suggest mindfulness-based relapse prevention is more beneficial long-term compared to traditional relapse prevention and treatment as usual, one meta-analysis (i.e., a study of studies) found mindfulness-based relapse prevention to only have a small effect on withdrawal and craving compared to comparator treatments (e.g., relapse prevention education, cognitive behavioral therapy, 12-step groups). However, the same study found no differences between mindfulness-based relapse prevention and comparators on relapse, frequency of use, treatment dropout, or mindfulness. Additional work should explore when and for whom mindfulness-based relapse prevention works and if there are characteristics of the intervention that could be enhanced for improved effect. The present study identified one group, women exposed to traumatic incidents, who might benefit from mindfulness training. Future work should explore if interventions targeting acting with awareness do help buffer the negative effects of trauma on craving for women exposed to such incidents and whether any related reductions in craving help reduce relapse risk.
The saying, “An ounce of prevention is worth a pound of cure,” aptly highlights the need to preempt exposure to traumatic incidents. Although modifiable characteristics (e.g., mindfulness, acting with awareness) may help reduce the negative experiences of trauma, a more sustainable and robust solution would be preventing the trauma before it happens. Addressing structural and generational inequities that increase the likelihood of stress and trauma could reduce trauma perpetuation before it happens. Preventing trauma would have compound benefits, including reduced craving. For example, addressing social determinants of health (e.g., healthcare access and quality, education access and quality, housing access and quality) may reduce significant life stressors and result in a range of health benefits, including less trauma.
The study was cross-sectional and did not consider the frequency, duration, or intensity of traumatic incident exposure. Thus, the findings may overly simplify a complex experience, and the findings should be considered exploratory.
The study relied on individuals to recall past experiences, which has possible response bias. Participants may respond in ways that are perceived to be socially desirable. Additionally, recall is imperfect and may result in inaccuracies.
Women in this study were enrolled in treatment. Thus, the findings may not generalize to women not in treatment or other gender identities.
BOTTOM LINE
Women in substance use disorder treatment with exposure to traumatic incidents during childhood and adulthood may be at an increased risk of posttraumatic stress disorder symptoms and greater craving; however, acting with awareness may alleviate the negative association between trauma and craving. Future research is warranted to confirm results from this cross-sectional study and explore why overall mindfulness is not associated with craving via trauma symptoms yet acting with awareness is. Screening women in substance use disorder treatment to find out if and when trauma occurred would likely help identify those at increased risk for craving and thus relapse. Furthermore, mindfulness-based therapies or other interventions that promote acting with awareness (e.g., cognitive behavioral therapy; CBT) may be an effective way to reduce the negative effects of trauma symptoms on craving for women exposed to traumatic incidents.
For individuals and families seeking recovery: Every patient that enters treatment has a unique set of needs and challenges but knowing if and when a person has been exposed to traumatic incidents may help signal clinicians to screen for posttraumatic stress disorder symptoms. Additionally, knowing about a person’s trauma history may help clinicians and treatment provides align a person’s needs with an appropriate type of treatment, such as mindfulness-based training that increase acting with awareness. If you or a loved one have been exposed to traumatic incidents and use substances, seeking comprehensive professional assessment is likely to help discover and address current and future symptoms.
For treatment professionals and treatment systems: Treatment systems might benefit from more thorough screening and assessment for if and when a person has been exposed to traumatic incidents in the past. This study found that women exposed to trauma during childhood and adulthood reported more cravings which was also related to greater posttraumatic stress disorder symptom severity compared to those exposed to traumatic incidents during adulthood only or never. More detailed trauma screening would likely help identify individuals at increased risk, which could help facilitate linkage to appropriate resources. Additionally, this study found that for women in substance use disorder treatment, higher levels of acting with awareness helped buffer the negative effects of trauma. Treatment professionals and treatment systems might consider acting with awareness as a potential target in standard, existing treatments for women exposed to trauma.
For scientists:Prospective research is needed to identify causal mechanisms leading to craving and substance use behaviors. Although this study was cross-sectional, the self-reported developmental period of exposure to trauma was found to impact the relationship between trauma symptom severity and craving for women in substance use disorder treatment. Women exposed to traumatic incidents during childhood and adulthood reported worse trauma symptom severity and higher levels craving. Mindfulness was found to buffer these negative effects regardless of when a women experienced trauma. Future studies should explore if mindfulness-based trainings are particularly effective for reducing substance use behaviors among women previously exposed to traumatic incidents. Furthermore, future studies should explore acting with awareness and whether existing interventions (e.g., cognitive behavioral therapy; CBT) mobilize what may be a helpful component of mindfulness. Additional studies may also investigate the relationship between trauma, PTSD symptoms, and craving among other gender identities and non-treatment populations.
For policy makers: Substance use disorder treatment can be a critical first step to addressing substance use behavior and reducing harm. This study found that women in treatment with a history of childhood and adulthood trauma reported more craving due to more severe posttraumatic stress disorder symptoms compared to women with adulthood only or no exposure. However, the study found that acting with awareness buffered the negative effects of trauma. Additional funding to support the investigation of trauma in substance use behavior and treatment could inform clinical care and public health interventions. Interventions that target acting with awareness (e.g., mindfulness-based relapse prevention, cognitive behavioral therapy) may be alternatives particularly effective for women with a trauma history. Increased funding to explore the effectiveness of such interventions for this population would likely help inform treatment and public health interventions.
The researchers in this study hypothesized that the symptoms associated with PTSD, such as intrusive memories and increased arousal to a stressor, may be associated with craving, which in turn can increase the risk of substance use. If an individual is experiencing trauma symptoms, they have less capacity to cope with day-to-day stressors and thus experience more craving. Because women in SUD treatment report higher rates of trauma, determining if trauma exposure is associated with craving could help clinicians and researchers identify a target for future treatments. Furthermore, identifying the effect of when trauma occurs could also help provide appropriate treatment. An intervention that buffers the effect of trauma on craving consequently could increase treatment success and improve health and wellness of women with a substance use disorder who have experienced trauma across the life course.
Although a history of trauma cannot be changed, there may be modifiable traits such as mindfulness that may buffer the negative effects of trauma. Mindfulness is an approach to paying attention that is focused on the present moment with compassion and without judgement or reaction. One meta-analysis, examining the results of many studies at once, found that those with more mindfulness had fewer substance use behaviors (e.g., fewer substance use problems, lower levels of substance use), although the size of this relationship was small. However, the meta-analysis also found that the relationship between mindfulness and substance use behaviors may be stronger for some. For example, the relationship is stronger for more severe inpatients versus outpatients and non-clinical samples. Although mindfulness-based relapse prevention treatments shows some promise to improving treatment outcomes, the time and effort required to train clinicians may limit the cost-benefit ratio of the intervention. Yet, if mindfulness buffers the effects of specific factors of substance use behaviors (i.e., craving) for those with heightened craving (i.e., women with a history of trauma), then mindfulness may be a viable target in specific instances. The relationship between mindfulness and trauma may also depend on when the trauma was experienced (childhood, adulthood, or both). Understanding if and when trauma occurs as well as who may benefit from mindfulness training could improve clinicians’ ability align patient needs and treatments, which could improve treatment effectiveness.
This study aimed to determine if trauma exposure at different times during the life course (i.e., childhood, adulthood, or both) is linked with PTSD symptoms and craving. The study also sought to determine if mindfulness buffered this relationship.
HOW WAS THIS STUDY CONDUCTED?
This cross-sectional study (i.e., where individuals are measured at only one time point) included 245 women receiving treatment for a substance use disorder. Women were eligible to participate if they were 18-65 years old, had a substance use disorder diagnosis, did not have an untreated psychotic disorder or severe chronic mental health condition, had not reported suicidality in the last 30 days, were not more than 6 months pregnant, and were enrolled in the gender-specific residential treatment program.
All women were asked about their exposure to trauma, when the exposure occurred, current PTSD symptoms and their severity, alcohol and drug craving, addiction severity, and mindfulness. Exposure to trauma was classified as yes or no based on responding yes to at least one experience of sexual, physical, and emotional trauma (e.g., “Were you ever abused or physically attacked [not sexually] by someone you knew [for example, a parent, boyfriend, or husband hit, slapped, choked, burned, or beat you up]?). The developmental period of exposure was classified as childhood (17 years old or younger), adulthood (18 years old or older), both, or neither. A post-traumatic stress disorder scale was used to calculate a trauma symptom severity score, and a scale that combined measures of frequency, intensity, and duration of craving for both alcohol and other drugs was also used. The posttraumatic symptom severity score can range from 0-51. The symptom severity ratings are: 0 = none; 1–10 = mild, 11–20 = moderate, 21–35 = moderate to severe, and >35 = severe. The craving scale consisted of five items that each range from 0 to 6, with a higher average score representing higher levels (i.e., more severe) alcohol and drug craving. Mindfulness was measured in a way that featured an overall trait mindfulness score as well as scores across five subscales of mindfulness: observing, describing, acting with awareness, nonjudgmental acceptance, and non-reactivity. Addiction severity, education, race/ethnicity, gender, and housing status was also measured.
A total of 245 women participated in the study. Most identified as Hispanic (58%) with about 21% and 21% identifying as non-Hispanic White and non-Hispanic Black, respectively. Almost half (48%) had not completed high school, and 23% were experiencing homelessness. Although 18% did not have any children, 48% had minor children but did not have custody. Additionally, 74% of the women were never married. Most (76%) of the women had a drug use disorder only, 10% had alcohol use disorder only, and 14% had both. About half (58%) had a mental health diagnosis other than a substance use disorder, with 27% having post-traumatic stress disorder. Methamphetamine was the most common substance used in the 8 months prior to treatment entry, followed by marijuana and alcohol-to-intoxication.
WHAT DID THIS STUDY FIND?
Presence and chronicity of traumatic incidents associated with craving.
Women who reported trauma exposure during childhood as well as in adulthood reported worse trauma symptoms compared to those that reported no trauma or trauma only in adulthood. Women who reported trauma incident(s) in both childhood and adulthood and those who reported trauma incident(s) only in childhood reported similar trauma symptom severity. The average trauma symptom severity score for women who reported trauma incidents) in both childhood and adulthood was 21.01. Yet, those who reported no trauma only had an average of 10.13, and those with trauma incident(s) only in adulthood had an average of 12.07. Women with only childhood trauma incident(s) had an average severity score of 18.63, which was considerably more than no trauma and adulthood only but not meaningfully different from those with both childhood and adulthood trauma.
Trauma symptomology was directly associated with higher levels of craving. Furthermore, compared to women experiencing traumatic incidents during both childhood and adulthood, those with no experiences and experiences in adulthood only had lower levels of substance use craving, associated with their lower trauma symptom severity.
Acting with awareness buffered the negative effect of trauma and craving.
In this study, mindfulness was considered to have five different components, with acting with awareness as one of them. Although overall trait mindfulness was not linked with changes in the relationship between time of trauma exposure and trauma symptom severity, acting with awareness was associated with that relationship. Acting with awareness was related with a weaker relationship between trauma symptoms and craving. At low levels of awareness, women with trauma exposure in both childhood and adulthood reported more trauma symptomology compared to childhood only, adulthood only, and no exposure. As awareness level increased, this relationship diminished. At high levels of awareness, there were no differences in trauma symptom severity across the developmental groups.
At low levels of awareness, women with exposure to trauma during both childhood and adulthood reported more craving resulting from worse trauma symptom severity compared to all other groups. At average awareness, women with no trauma and adulthood only trauma reported more craving as their trauma symptom severity increased. At high levels of awareness, there were no differences in the relationships between craving and trauma symptom severity across groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Overall, this study found that women experiencing trauma during both childhood and adulthood report more post-traumatic stress disorder (PTSD) symptoms, which is also associated with greater craving. Also, the relationship between trauma symptoms and substance use craving appeared to be buffered by mindfulness abilities. Studies like this help us understand mechanisms that could benefit from further research and that may be targeted to improve treatment outcomes and the chances of recovery, particularly for vulnerable populations such as women who have experienced trauma.
This study identified a potential causal chain of events—trauma exposure to trauma symptoms to craving—that possibly may be interrupted to improve treatment for women in substance use disorder treatment. However, given the cross-sectional nature of the study (i.e., questions only asked at one point in time) more research is needed to clarify these causal connections. Also, overall trait mindfulness did not alter the relationship between trauma symptoms and craving.
Trauma can alter a person’s ability to cope with stressors and thus increases the likelihood of seeking substances to alleviate stress. The past year prevalence of PTSD for women is more than double that of men (5.2% vs. 1.8%). Thus, pinpointing a mechanism to target that involves trauma may be especially important for women. Furthermore, this study highlighted that when trauma occurs may be important. Women who experienced trauma during both childhood and adulthood appeared to fare worse than those who experienced trauma only during adulthood or not at all. This finding suggests that screening for when the exposure to the traumatic incident(s) occurred in addition to if it/they occurred may help identify women who may be at increased risk for relapse.
One aspect of mindfulness—acting with awareness—was found to mitigate the relationship between trauma and craving regardless of when trauma was experienced. Acting with awareness is focusing on one’s activities in the moment instead of operating on autopilot. Women reporting high levels of mindful awareness, and who were exposed to traumatic incidents during childhood or adulthood and those not exposed to trauma reported no more craving than those exposed to traumatic incidents during both childhood and adulthood.
Mindfulness-based trainings, specifically those targeting acting with awareness, warrant future study to explore if it can help buffer the negative effects of trauma and improve recovery chances. Mindfulness-based relapse prevention is one type of therapy that aims to do this. Although some findings suggest mindfulness-based relapse prevention is more beneficial long-term compared to traditional relapse prevention and treatment as usual, one meta-analysis (i.e., a study of studies) found mindfulness-based relapse prevention to only have a small effect on withdrawal and craving compared to comparator treatments (e.g., relapse prevention education, cognitive behavioral therapy, 12-step groups). However, the same study found no differences between mindfulness-based relapse prevention and comparators on relapse, frequency of use, treatment dropout, or mindfulness. Additional work should explore when and for whom mindfulness-based relapse prevention works and if there are characteristics of the intervention that could be enhanced for improved effect. The present study identified one group, women exposed to traumatic incidents, who might benefit from mindfulness training. Future work should explore if interventions targeting acting with awareness do help buffer the negative effects of trauma on craving for women exposed to such incidents and whether any related reductions in craving help reduce relapse risk.
The saying, “An ounce of prevention is worth a pound of cure,” aptly highlights the need to preempt exposure to traumatic incidents. Although modifiable characteristics (e.g., mindfulness, acting with awareness) may help reduce the negative experiences of trauma, a more sustainable and robust solution would be preventing the trauma before it happens. Addressing structural and generational inequities that increase the likelihood of stress and trauma could reduce trauma perpetuation before it happens. Preventing trauma would have compound benefits, including reduced craving. For example, addressing social determinants of health (e.g., healthcare access and quality, education access and quality, housing access and quality) may reduce significant life stressors and result in a range of health benefits, including less trauma.
The study was cross-sectional and did not consider the frequency, duration, or intensity of traumatic incident exposure. Thus, the findings may overly simplify a complex experience, and the findings should be considered exploratory.
The study relied on individuals to recall past experiences, which has possible response bias. Participants may respond in ways that are perceived to be socially desirable. Additionally, recall is imperfect and may result in inaccuracies.
Women in this study were enrolled in treatment. Thus, the findings may not generalize to women not in treatment or other gender identities.
BOTTOM LINE
Women in substance use disorder treatment with exposure to traumatic incidents during childhood and adulthood may be at an increased risk of posttraumatic stress disorder symptoms and greater craving; however, acting with awareness may alleviate the negative association between trauma and craving. Future research is warranted to confirm results from this cross-sectional study and explore why overall mindfulness is not associated with craving via trauma symptoms yet acting with awareness is. Screening women in substance use disorder treatment to find out if and when trauma occurred would likely help identify those at increased risk for craving and thus relapse. Furthermore, mindfulness-based therapies or other interventions that promote acting with awareness (e.g., cognitive behavioral therapy; CBT) may be an effective way to reduce the negative effects of trauma symptoms on craving for women exposed to traumatic incidents.
For individuals and families seeking recovery: Every patient that enters treatment has a unique set of needs and challenges but knowing if and when a person has been exposed to traumatic incidents may help signal clinicians to screen for posttraumatic stress disorder symptoms. Additionally, knowing about a person’s trauma history may help clinicians and treatment provides align a person’s needs with an appropriate type of treatment, such as mindfulness-based training that increase acting with awareness. If you or a loved one have been exposed to traumatic incidents and use substances, seeking comprehensive professional assessment is likely to help discover and address current and future symptoms.
For treatment professionals and treatment systems: Treatment systems might benefit from more thorough screening and assessment for if and when a person has been exposed to traumatic incidents in the past. This study found that women exposed to trauma during childhood and adulthood reported more cravings which was also related to greater posttraumatic stress disorder symptom severity compared to those exposed to traumatic incidents during adulthood only or never. More detailed trauma screening would likely help identify individuals at increased risk, which could help facilitate linkage to appropriate resources. Additionally, this study found that for women in substance use disorder treatment, higher levels of acting with awareness helped buffer the negative effects of trauma. Treatment professionals and treatment systems might consider acting with awareness as a potential target in standard, existing treatments for women exposed to trauma.
For scientists:Prospective research is needed to identify causal mechanisms leading to craving and substance use behaviors. Although this study was cross-sectional, the self-reported developmental period of exposure to trauma was found to impact the relationship between trauma symptom severity and craving for women in substance use disorder treatment. Women exposed to traumatic incidents during childhood and adulthood reported worse trauma symptom severity and higher levels craving. Mindfulness was found to buffer these negative effects regardless of when a women experienced trauma. Future studies should explore if mindfulness-based trainings are particularly effective for reducing substance use behaviors among women previously exposed to traumatic incidents. Furthermore, future studies should explore acting with awareness and whether existing interventions (e.g., cognitive behavioral therapy; CBT) mobilize what may be a helpful component of mindfulness. Additional studies may also investigate the relationship between trauma, PTSD symptoms, and craving among other gender identities and non-treatment populations.
For policy makers: Substance use disorder treatment can be a critical first step to addressing substance use behavior and reducing harm. This study found that women in treatment with a history of childhood and adulthood trauma reported more craving due to more severe posttraumatic stress disorder symptoms compared to women with adulthood only or no exposure. However, the study found that acting with awareness buffered the negative effects of trauma. Additional funding to support the investigation of trauma in substance use behavior and treatment could inform clinical care and public health interventions. Interventions that target acting with awareness (e.g., mindfulness-based relapse prevention, cognitive behavioral therapy) may be alternatives particularly effective for women with a trauma history. Increased funding to explore the effectiveness of such interventions for this population would likely help inform treatment and public health interventions.
The researchers in this study hypothesized that the symptoms associated with PTSD, such as intrusive memories and increased arousal to a stressor, may be associated with craving, which in turn can increase the risk of substance use. If an individual is experiencing trauma symptoms, they have less capacity to cope with day-to-day stressors and thus experience more craving. Because women in SUD treatment report higher rates of trauma, determining if trauma exposure is associated with craving could help clinicians and researchers identify a target for future treatments. Furthermore, identifying the effect of when trauma occurs could also help provide appropriate treatment. An intervention that buffers the effect of trauma on craving consequently could increase treatment success and improve health and wellness of women with a substance use disorder who have experienced trauma across the life course.
Although a history of trauma cannot be changed, there may be modifiable traits such as mindfulness that may buffer the negative effects of trauma. Mindfulness is an approach to paying attention that is focused on the present moment with compassion and without judgement or reaction. One meta-analysis, examining the results of many studies at once, found that those with more mindfulness had fewer substance use behaviors (e.g., fewer substance use problems, lower levels of substance use), although the size of this relationship was small. However, the meta-analysis also found that the relationship between mindfulness and substance use behaviors may be stronger for some. For example, the relationship is stronger for more severe inpatients versus outpatients and non-clinical samples. Although mindfulness-based relapse prevention treatments shows some promise to improving treatment outcomes, the time and effort required to train clinicians may limit the cost-benefit ratio of the intervention. Yet, if mindfulness buffers the effects of specific factors of substance use behaviors (i.e., craving) for those with heightened craving (i.e., women with a history of trauma), then mindfulness may be a viable target in specific instances. The relationship between mindfulness and trauma may also depend on when the trauma was experienced (childhood, adulthood, or both). Understanding if and when trauma occurs as well as who may benefit from mindfulness training could improve clinicians’ ability align patient needs and treatments, which could improve treatment effectiveness.
This study aimed to determine if trauma exposure at different times during the life course (i.e., childhood, adulthood, or both) is linked with PTSD symptoms and craving. The study also sought to determine if mindfulness buffered this relationship.
HOW WAS THIS STUDY CONDUCTED?
This cross-sectional study (i.e., where individuals are measured at only one time point) included 245 women receiving treatment for a substance use disorder. Women were eligible to participate if they were 18-65 years old, had a substance use disorder diagnosis, did not have an untreated psychotic disorder or severe chronic mental health condition, had not reported suicidality in the last 30 days, were not more than 6 months pregnant, and were enrolled in the gender-specific residential treatment program.
All women were asked about their exposure to trauma, when the exposure occurred, current PTSD symptoms and their severity, alcohol and drug craving, addiction severity, and mindfulness. Exposure to trauma was classified as yes or no based on responding yes to at least one experience of sexual, physical, and emotional trauma (e.g., “Were you ever abused or physically attacked [not sexually] by someone you knew [for example, a parent, boyfriend, or husband hit, slapped, choked, burned, or beat you up]?). The developmental period of exposure was classified as childhood (17 years old or younger), adulthood (18 years old or older), both, or neither. A post-traumatic stress disorder scale was used to calculate a trauma symptom severity score, and a scale that combined measures of frequency, intensity, and duration of craving for both alcohol and other drugs was also used. The posttraumatic symptom severity score can range from 0-51. The symptom severity ratings are: 0 = none; 1–10 = mild, 11–20 = moderate, 21–35 = moderate to severe, and >35 = severe. The craving scale consisted of five items that each range from 0 to 6, with a higher average score representing higher levels (i.e., more severe) alcohol and drug craving. Mindfulness was measured in a way that featured an overall trait mindfulness score as well as scores across five subscales of mindfulness: observing, describing, acting with awareness, nonjudgmental acceptance, and non-reactivity. Addiction severity, education, race/ethnicity, gender, and housing status was also measured.
A total of 245 women participated in the study. Most identified as Hispanic (58%) with about 21% and 21% identifying as non-Hispanic White and non-Hispanic Black, respectively. Almost half (48%) had not completed high school, and 23% were experiencing homelessness. Although 18% did not have any children, 48% had minor children but did not have custody. Additionally, 74% of the women were never married. Most (76%) of the women had a drug use disorder only, 10% had alcohol use disorder only, and 14% had both. About half (58%) had a mental health diagnosis other than a substance use disorder, with 27% having post-traumatic stress disorder. Methamphetamine was the most common substance used in the 8 months prior to treatment entry, followed by marijuana and alcohol-to-intoxication.
WHAT DID THIS STUDY FIND?
Presence and chronicity of traumatic incidents associated with craving.
Women who reported trauma exposure during childhood as well as in adulthood reported worse trauma symptoms compared to those that reported no trauma or trauma only in adulthood. Women who reported trauma incident(s) in both childhood and adulthood and those who reported trauma incident(s) only in childhood reported similar trauma symptom severity. The average trauma symptom severity score for women who reported trauma incidents) in both childhood and adulthood was 21.01. Yet, those who reported no trauma only had an average of 10.13, and those with trauma incident(s) only in adulthood had an average of 12.07. Women with only childhood trauma incident(s) had an average severity score of 18.63, which was considerably more than no trauma and adulthood only but not meaningfully different from those with both childhood and adulthood trauma.
Trauma symptomology was directly associated with higher levels of craving. Furthermore, compared to women experiencing traumatic incidents during both childhood and adulthood, those with no experiences and experiences in adulthood only had lower levels of substance use craving, associated with their lower trauma symptom severity.
Acting with awareness buffered the negative effect of trauma and craving.
In this study, mindfulness was considered to have five different components, with acting with awareness as one of them. Although overall trait mindfulness was not linked with changes in the relationship between time of trauma exposure and trauma symptom severity, acting with awareness was associated with that relationship. Acting with awareness was related with a weaker relationship between trauma symptoms and craving. At low levels of awareness, women with trauma exposure in both childhood and adulthood reported more trauma symptomology compared to childhood only, adulthood only, and no exposure. As awareness level increased, this relationship diminished. At high levels of awareness, there were no differences in trauma symptom severity across the developmental groups.
At low levels of awareness, women with exposure to trauma during both childhood and adulthood reported more craving resulting from worse trauma symptom severity compared to all other groups. At average awareness, women with no trauma and adulthood only trauma reported more craving as their trauma symptom severity increased. At high levels of awareness, there were no differences in the relationships between craving and trauma symptom severity across groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Overall, this study found that women experiencing trauma during both childhood and adulthood report more post-traumatic stress disorder (PTSD) symptoms, which is also associated with greater craving. Also, the relationship between trauma symptoms and substance use craving appeared to be buffered by mindfulness abilities. Studies like this help us understand mechanisms that could benefit from further research and that may be targeted to improve treatment outcomes and the chances of recovery, particularly for vulnerable populations such as women who have experienced trauma.
This study identified a potential causal chain of events—trauma exposure to trauma symptoms to craving—that possibly may be interrupted to improve treatment for women in substance use disorder treatment. However, given the cross-sectional nature of the study (i.e., questions only asked at one point in time) more research is needed to clarify these causal connections. Also, overall trait mindfulness did not alter the relationship between trauma symptoms and craving.
Trauma can alter a person’s ability to cope with stressors and thus increases the likelihood of seeking substances to alleviate stress. The past year prevalence of PTSD for women is more than double that of men (5.2% vs. 1.8%). Thus, pinpointing a mechanism to target that involves trauma may be especially important for women. Furthermore, this study highlighted that when trauma occurs may be important. Women who experienced trauma during both childhood and adulthood appeared to fare worse than those who experienced trauma only during adulthood or not at all. This finding suggests that screening for when the exposure to the traumatic incident(s) occurred in addition to if it/they occurred may help identify women who may be at increased risk for relapse.
One aspect of mindfulness—acting with awareness—was found to mitigate the relationship between trauma and craving regardless of when trauma was experienced. Acting with awareness is focusing on one’s activities in the moment instead of operating on autopilot. Women reporting high levels of mindful awareness, and who were exposed to traumatic incidents during childhood or adulthood and those not exposed to trauma reported no more craving than those exposed to traumatic incidents during both childhood and adulthood.
Mindfulness-based trainings, specifically those targeting acting with awareness, warrant future study to explore if it can help buffer the negative effects of trauma and improve recovery chances. Mindfulness-based relapse prevention is one type of therapy that aims to do this. Although some findings suggest mindfulness-based relapse prevention is more beneficial long-term compared to traditional relapse prevention and treatment as usual, one meta-analysis (i.e., a study of studies) found mindfulness-based relapse prevention to only have a small effect on withdrawal and craving compared to comparator treatments (e.g., relapse prevention education, cognitive behavioral therapy, 12-step groups). However, the same study found no differences between mindfulness-based relapse prevention and comparators on relapse, frequency of use, treatment dropout, or mindfulness. Additional work should explore when and for whom mindfulness-based relapse prevention works and if there are characteristics of the intervention that could be enhanced for improved effect. The present study identified one group, women exposed to traumatic incidents, who might benefit from mindfulness training. Future work should explore if interventions targeting acting with awareness do help buffer the negative effects of trauma on craving for women exposed to such incidents and whether any related reductions in craving help reduce relapse risk.
The saying, “An ounce of prevention is worth a pound of cure,” aptly highlights the need to preempt exposure to traumatic incidents. Although modifiable characteristics (e.g., mindfulness, acting with awareness) may help reduce the negative experiences of trauma, a more sustainable and robust solution would be preventing the trauma before it happens. Addressing structural and generational inequities that increase the likelihood of stress and trauma could reduce trauma perpetuation before it happens. Preventing trauma would have compound benefits, including reduced craving. For example, addressing social determinants of health (e.g., healthcare access and quality, education access and quality, housing access and quality) may reduce significant life stressors and result in a range of health benefits, including less trauma.
The study was cross-sectional and did not consider the frequency, duration, or intensity of traumatic incident exposure. Thus, the findings may overly simplify a complex experience, and the findings should be considered exploratory.
The study relied on individuals to recall past experiences, which has possible response bias. Participants may respond in ways that are perceived to be socially desirable. Additionally, recall is imperfect and may result in inaccuracies.
Women in this study were enrolled in treatment. Thus, the findings may not generalize to women not in treatment or other gender identities.
BOTTOM LINE
Women in substance use disorder treatment with exposure to traumatic incidents during childhood and adulthood may be at an increased risk of posttraumatic stress disorder symptoms and greater craving; however, acting with awareness may alleviate the negative association between trauma and craving. Future research is warranted to confirm results from this cross-sectional study and explore why overall mindfulness is not associated with craving via trauma symptoms yet acting with awareness is. Screening women in substance use disorder treatment to find out if and when trauma occurred would likely help identify those at increased risk for craving and thus relapse. Furthermore, mindfulness-based therapies or other interventions that promote acting with awareness (e.g., cognitive behavioral therapy; CBT) may be an effective way to reduce the negative effects of trauma symptoms on craving for women exposed to traumatic incidents.
For individuals and families seeking recovery: Every patient that enters treatment has a unique set of needs and challenges but knowing if and when a person has been exposed to traumatic incidents may help signal clinicians to screen for posttraumatic stress disorder symptoms. Additionally, knowing about a person’s trauma history may help clinicians and treatment provides align a person’s needs with an appropriate type of treatment, such as mindfulness-based training that increase acting with awareness. If you or a loved one have been exposed to traumatic incidents and use substances, seeking comprehensive professional assessment is likely to help discover and address current and future symptoms.
For treatment professionals and treatment systems: Treatment systems might benefit from more thorough screening and assessment for if and when a person has been exposed to traumatic incidents in the past. This study found that women exposed to trauma during childhood and adulthood reported more cravings which was also related to greater posttraumatic stress disorder symptom severity compared to those exposed to traumatic incidents during adulthood only or never. More detailed trauma screening would likely help identify individuals at increased risk, which could help facilitate linkage to appropriate resources. Additionally, this study found that for women in substance use disorder treatment, higher levels of acting with awareness helped buffer the negative effects of trauma. Treatment professionals and treatment systems might consider acting with awareness as a potential target in standard, existing treatments for women exposed to trauma.
For scientists:Prospective research is needed to identify causal mechanisms leading to craving and substance use behaviors. Although this study was cross-sectional, the self-reported developmental period of exposure to trauma was found to impact the relationship between trauma symptom severity and craving for women in substance use disorder treatment. Women exposed to traumatic incidents during childhood and adulthood reported worse trauma symptom severity and higher levels craving. Mindfulness was found to buffer these negative effects regardless of when a women experienced trauma. Future studies should explore if mindfulness-based trainings are particularly effective for reducing substance use behaviors among women previously exposed to traumatic incidents. Furthermore, future studies should explore acting with awareness and whether existing interventions (e.g., cognitive behavioral therapy; CBT) mobilize what may be a helpful component of mindfulness. Additional studies may also investigate the relationship between trauma, PTSD symptoms, and craving among other gender identities and non-treatment populations.
For policy makers: Substance use disorder treatment can be a critical first step to addressing substance use behavior and reducing harm. This study found that women in treatment with a history of childhood and adulthood trauma reported more craving due to more severe posttraumatic stress disorder symptoms compared to women with adulthood only or no exposure. However, the study found that acting with awareness buffered the negative effects of trauma. Additional funding to support the investigation of trauma in substance use behavior and treatment could inform clinical care and public health interventions. Interventions that target acting with awareness (e.g., mindfulness-based relapse prevention, cognitive behavioral therapy) may be alternatives particularly effective for women with a trauma history. Increased funding to explore the effectiveness of such interventions for this population would likely help inform treatment and public health interventions.