Does adding a strengths-based component focused on well-being and self-regulation to residential treatment boost young adult treatment outcomes?
Residential treatment addresses severe substance use disorder by removing a young adult from their high-risk environmental context while helping them begin to build recovery coping skills. Because residential programs primarily focus on substance use, they may lack a broader focus on wellbeing. This study examined whether adding a mindfulness and strengths-based group intervention improved their outcomes.
Recovery from substance use disorders typically involves both a) improvements in substance use either through reductions to non-symptomatic levels or abstinence and b) improvements to other aspects of quality of life, well-being, and overall functioning. For young adults, these recovery processes are occurring also in the context of achieving developmental milestones (for example, completing high school or starting full-time employment or college). For those at the most severe end of the spectrum of substance use disorders, residential treatment can help address an individual’s immediate and long-term needs by removing an individual from their high-risk environmental context, providing detoxification and medical stabilization, and giving them specific forms of treatment to address their substance use disorder. Ideally, this treatment provides an individual with skills that they can use when they exit treatment and return to their home, neighborhood, and place of work or school. Quality residential programs also help assertively link individuals to outpatient treatment and recovery support services in the community.
This study examined if adding a strengths-based group intervention (labeled the Grit Wellbeing and Self-regulation Program) could improve outcomes among young adults who attended residential treatment.
HOW WAS THIS STUDY CONDUCTED?
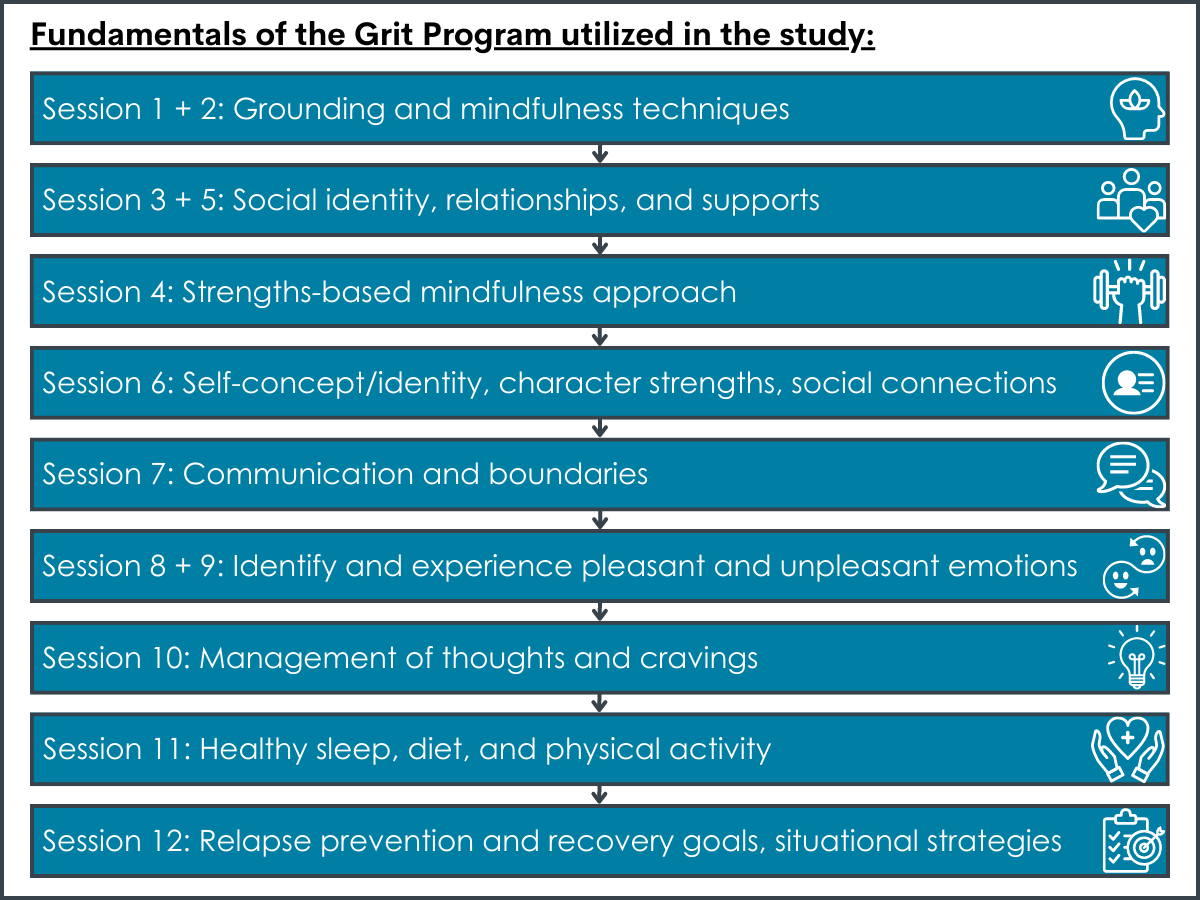
This was a cohort-controlled trial to examine whether among young adults in treatment, an additional group-based intervention produced meaningful recovery-related benefits. There were two participating residential treatment sites; patients attended the treatment site closest to where they lived (i.e., they were not randomized to attend a specific treatment site). Both provided similar standard 6-week residential treatment to adults, although one site served only 18–35-year-olds while the other served adults up to age 65. The site that served the younger adult population also provided an additional intervention, called “Grit,” which was described as a strengths-based, wellbeing and self-regulation program that incorporated some elements of mindfulness-based relapse prevention.
Grit was offered in 60-minute sessions given twice a week for 6 weeks by a clinical researcher and a member of the treatment staff. To be eligible for this study, patients had to be between the ages of 18-35 years old. Participants had assessments at baseline, treatment exit (6 weeks) and 3-, 6-, and 12-months after the baseline assessment.
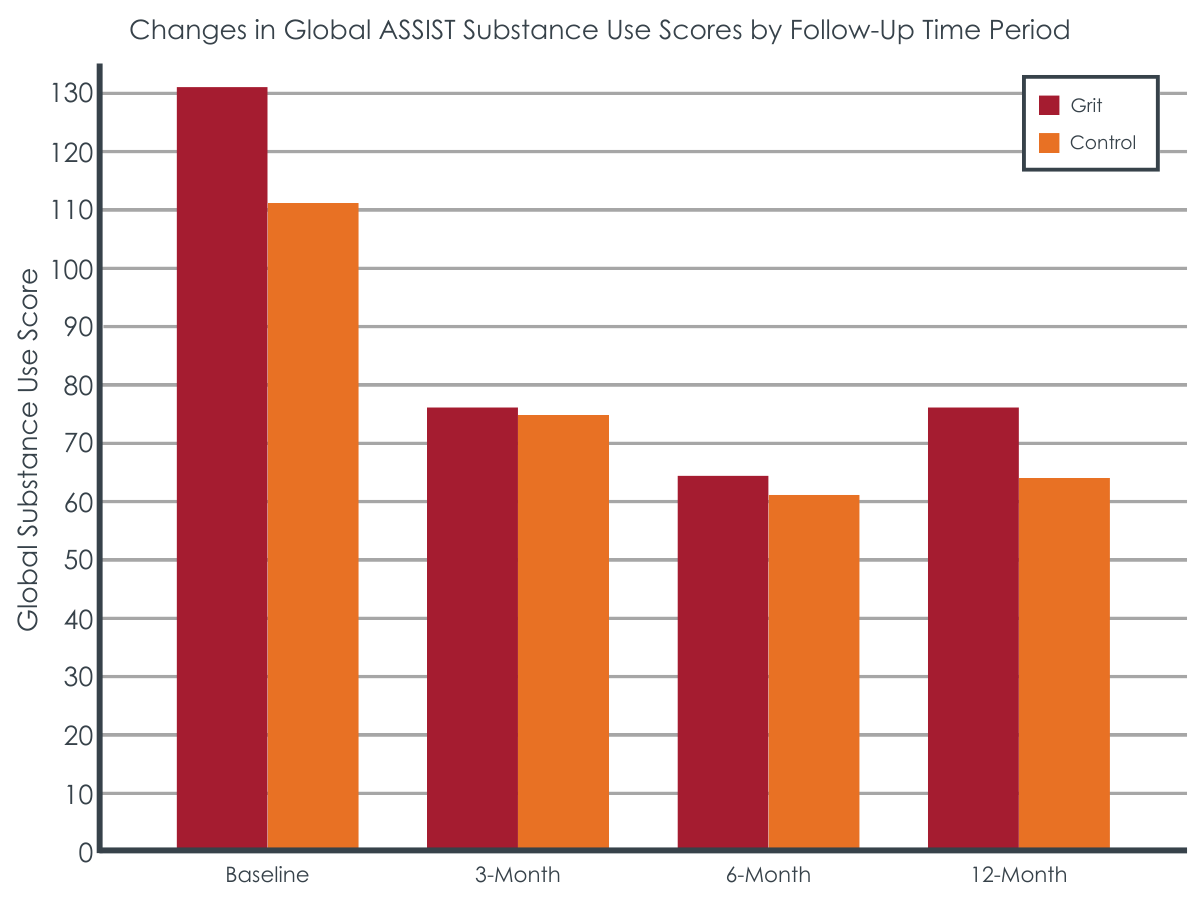
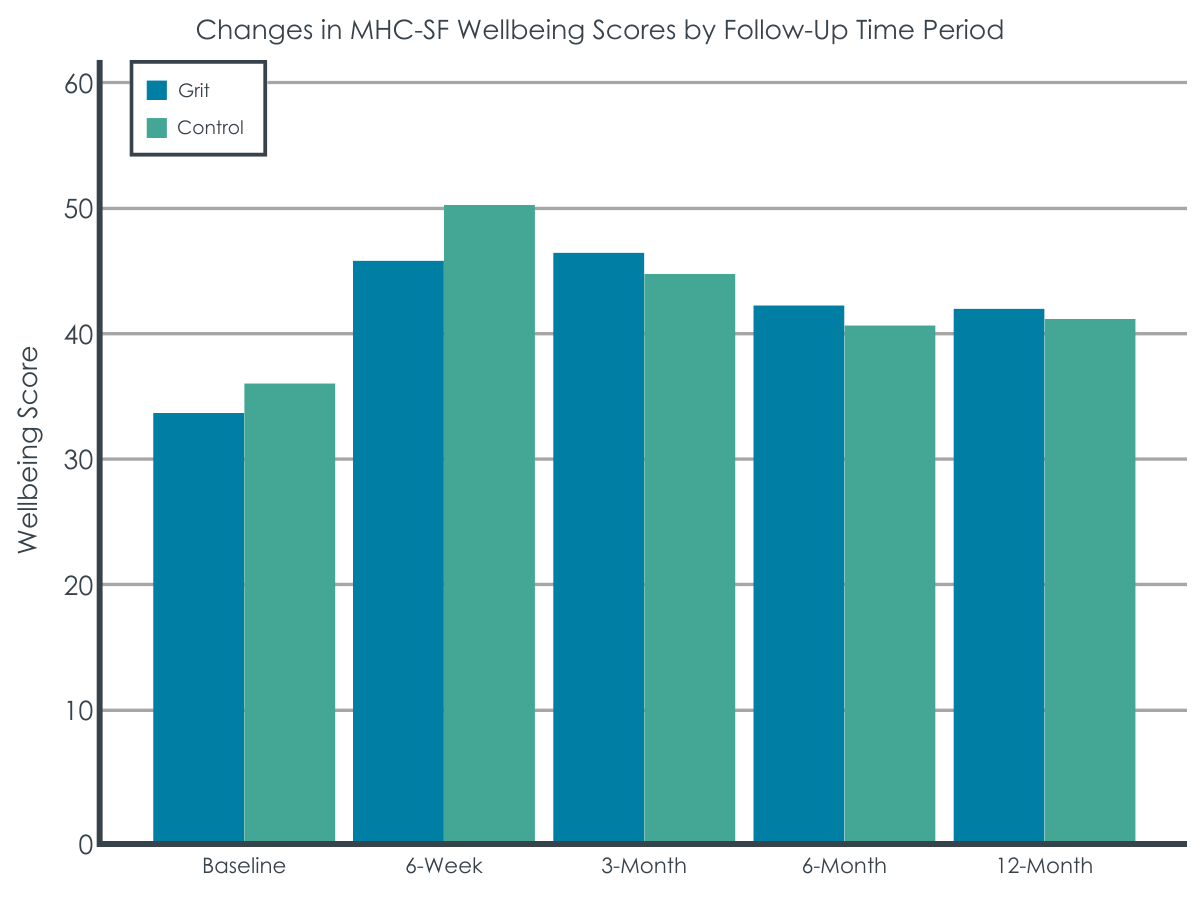
Substance use outcomes were measured by the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (WHO ASSIST) a standardized scale that has been widely validated internationally. The key outcomes were (1) overall substance use score and (2) substance use score of the most common primary drugs of concern at the residential treatment centers (i.e., alcohol, methamphetamine, and cannabis). Secondary outcomes were well-being, mental health (depression and anxiety according to the PHQ-9 and the GAD-7), and past-month vocational engagement (defined as engaging in work or study).
In this analysis, the authors compared (1) baseline and 3-, 6-, and 12-month follow-ups for substance use and vocational engagement between the two conditions and compared (2) baseline to post-treatment (6 weeks) and 3-, 6-, and 12-month follow-ups for wellbeing and mental health between the two groups. All analyses controlled for key participant characteristics that differed between the two sites (i.e., age and having a child) and included all individuals who started the study regardless of whether they participated in follow-up assessments or not. For assessments not completed by a participant, the analytic approach functionally imputed missing scores by testing trajectories of participant outcomes. This approach is taken to decrease the chances that participant dropout will substantially impact the findings.
Of the sample of 230 young adults, the average age was 27 years old, 66% were male, 21% had a history of criminal justice involvement, and 35% had at least one child. The primary substances reported were amphetamines (45%: 93% of which was ice/crystal methamphetamine), alcohol (34%), and marijuana (15%). Participants remained in treatment (designed to last 6 weeks) for on average about a month (29 days). Participants who were in the treatment site where Grit was delivered had higher methamphetamine and marijuana use scores at baseline. They were also more likely to be readmitted to treatment following discharge than the standard treatment condition.
WHAT DID THIS STUDY FIND?
Intervention and comparison groups fared equally well on most outcomes.
Both groups reduced their overall and individual substance use scores (alcohol, marijuana, and methamphetamines). These reductions were maintained at the 12-month follow-up. Both groups also improved their well-being, increased their vocational engagement, and reduced symptoms of depression and anxiety.
The Grit group experienced a greater reduction in their methamphetamine use score compared to the standard treatment group from baseline to 3 months and a greater reduction in their marijuana use score compared to the standard treatment group over time, but the Grit group also had higher use scores of these substances at baseline and thus more room to improve. The Grit advantage was not maintained over time for methamphetamine use as both groups had similar reductions in methamphetamine use from baseline to 6- and 12-month follow-ups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this sample of young adults attending residential treatment, individuals experienced improvements in both their substance use as well as well-being, vocational engagement, and mental health. These gains were largely maintained out to 1 year after entering treatment. Yet, an additional intervention, Grit, focused on strengths-based, wellbeing and self-regulation was not linked to improved results on most outcomes. Although the residential program where patients had exposure to the Grit intervention showed some relative improvements on methamphetamine and marijuana scores compared to the standard treatment, this group had higher use scores at baseline on these substances and were also more likely to be readmitted to treatment following discharge. This suggests these participants might have had more severe substance use profiles compared to the participants in the non-Grit, standard treatment condition, with more room to improve their substance use and so the improved results may not be solely due to the Grit program.
As both study conditions involved participants in an intensive 6-week residential program, it is possible that the additional Grit intervention did not address enough unique components necessary or did not address them in the right way or as intensively as needed, to boost recovery compared to the treatment that participants were already receiving. The location of the GRIT intervention also served a younger adult profile (18–35-year-olds) whereas the location of the comparison group served adults up to ages 65, so any differences between the conditions could have been due to the existing programming at each site and its developmental appropriateness for the sample in this study. In addition, there is no information on additional recovery support services that these young adults engaged in following their treatment episode, which could have differed between groups and can strong influences on recovery outcomes over time. Also, while gains made during treatment are largely maintained out to 1 year, 35% were readmitted to the treatment center at 3 months and others had attended another treatment program (14 new admission episodes by the 3-month and 44 new admission episodes by the 12-month follow-ups). The impact of further treatment on outcomes was not examined.
Although the study design of a cohort-controlled trial was used for several logistical reasons, the lack of randomization to study condition introduced potential confounding factors. That is, participants who were in one condition or the other as a result of where they chose (or had access) to attend treatment could also influence their outcomes during and after treatment. There may be other factors, aside from study condition, such as financial or social resources, that influenced both their treatment and their recovery outcomes. As well, the Grit intervention was delivered at the young adult specific residential treatment center where all residents were 18-35 years old. The other center where the control condition was delivered was for adults ages 18 and older. There may have been some key therapeutic aspects related to a young adult program that were part of the standard treatment approach and not unique to Grit leading to differing outcomes.
There was attrition from the study over time indicating there could be differences between those who completed later study visits compared to those who did not: retention ranged from 61% (12 months) to 81% (end of treatment, 6 weeks after baseline). The authors addressed this by conducting analyses where everyone who completed a baseline study visit were included in the analysis whether or not they completed the intervention, but this is still a large rate of study dropout, and it is not clear how the missing data on the outcomes were handled.
The short-term reductions in methamphetamine and marijuana use among the Grit participants could have been due to a statistical artifact known as regression to the mean; that is, over time, high levels of use often return to lower levels and because of the greater severity of use of these substances among the Grit group at baseline compared to the comparison condition, they had a greater likelihood of experiencing a greater reduction in use.
BOTTOM LINE
In this sample of young adults, standard residential treatment at both sites was associated with reductions in substance use scores and improvements in well-being, mental health, and vocational engagement that were maintained at the 12-month follow-up, but the addition of the novel Grit group intervention focused on improving well-being and self-regulation in part through mindfulness-based intervention did not, appear to have any meaningful or lasting effects.
For individuals and families seeking recovery: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether receiving continuing care such as through mutual help groups or recovery community organizations, with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research.
For treatment professionals and treatment systems: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average for this sample of young adults, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care such as through mutual help groups or recovery community organizations, with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research.
For scientists:Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research. The use of a cohort-controlled trial in this case made some interpretation of findings difficult. An alternative approach, such as an on-off design within each treatment center could be considered in the future to better understand which outcomes are results of the residential treatment program and which outcomes might be due to new/additional treatment components such as the Grit program examined here. Further work in this area to map and systematically assess the mechanisms of behavior change at work in these interventions is needed.
For policy makers: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average for this group of young adults, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research. Funding to support further research in these areas may help to identify and target key moderators (i.e., who benefits/doesn’t benefit) and mechanisms (i.e., why/why not) of treatment effects and enhance the precision and efficient delivery of interventions in these settings.
Recovery from substance use disorders typically involves both a) improvements in substance use either through reductions to non-symptomatic levels or abstinence and b) improvements to other aspects of quality of life, well-being, and overall functioning. For young adults, these recovery processes are occurring also in the context of achieving developmental milestones (for example, completing high school or starting full-time employment or college). For those at the most severe end of the spectrum of substance use disorders, residential treatment can help address an individual’s immediate and long-term needs by removing an individual from their high-risk environmental context, providing detoxification and medical stabilization, and giving them specific forms of treatment to address their substance use disorder. Ideally, this treatment provides an individual with skills that they can use when they exit treatment and return to their home, neighborhood, and place of work or school. Quality residential programs also help assertively link individuals to outpatient treatment and recovery support services in the community.
This study examined if adding a strengths-based group intervention (labeled the Grit Wellbeing and Self-regulation Program) could improve outcomes among young adults who attended residential treatment.
HOW WAS THIS STUDY CONDUCTED?
This was a cohort-controlled trial to examine whether among young adults in treatment, an additional group-based intervention produced meaningful recovery-related benefits. There were two participating residential treatment sites; patients attended the treatment site closest to where they lived (i.e., they were not randomized to attend a specific treatment site). Both provided similar standard 6-week residential treatment to adults, although one site served only 18–35-year-olds while the other served adults up to age 65. The site that served the younger adult population also provided an additional intervention, called “Grit,” which was described as a strengths-based, wellbeing and self-regulation program that incorporated some elements of mindfulness-based relapse prevention.
Grit was offered in 60-minute sessions given twice a week for 6 weeks by a clinical researcher and a member of the treatment staff. To be eligible for this study, patients had to be between the ages of 18-35 years old. Participants had assessments at baseline, treatment exit (6 weeks) and 3-, 6-, and 12-months after the baseline assessment.
Substance use outcomes were measured by the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (WHO ASSIST) a standardized scale that has been widely validated internationally. The key outcomes were (1) overall substance use score and (2) substance use score of the most common primary drugs of concern at the residential treatment centers (i.e., alcohol, methamphetamine, and cannabis). Secondary outcomes were well-being, mental health (depression and anxiety according to the PHQ-9 and the GAD-7), and past-month vocational engagement (defined as engaging in work or study).
In this analysis, the authors compared (1) baseline and 3-, 6-, and 12-month follow-ups for substance use and vocational engagement between the two conditions and compared (2) baseline to post-treatment (6 weeks) and 3-, 6-, and 12-month follow-ups for wellbeing and mental health between the two groups. All analyses controlled for key participant characteristics that differed between the two sites (i.e., age and having a child) and included all individuals who started the study regardless of whether they participated in follow-up assessments or not. For assessments not completed by a participant, the analytic approach functionally imputed missing scores by testing trajectories of participant outcomes. This approach is taken to decrease the chances that participant dropout will substantially impact the findings.
Of the sample of 230 young adults, the average age was 27 years old, 66% were male, 21% had a history of criminal justice involvement, and 35% had at least one child. The primary substances reported were amphetamines (45%: 93% of which was ice/crystal methamphetamine), alcohol (34%), and marijuana (15%). Participants remained in treatment (designed to last 6 weeks) for on average about a month (29 days). Participants who were in the treatment site where Grit was delivered had higher methamphetamine and marijuana use scores at baseline. They were also more likely to be readmitted to treatment following discharge than the standard treatment condition.
WHAT DID THIS STUDY FIND?
Intervention and comparison groups fared equally well on most outcomes.
Both groups reduced their overall and individual substance use scores (alcohol, marijuana, and methamphetamines). These reductions were maintained at the 12-month follow-up. Both groups also improved their well-being, increased their vocational engagement, and reduced symptoms of depression and anxiety.
The Grit group experienced a greater reduction in their methamphetamine use score compared to the standard treatment group from baseline to 3 months and a greater reduction in their marijuana use score compared to the standard treatment group over time, but the Grit group also had higher use scores of these substances at baseline and thus more room to improve. The Grit advantage was not maintained over time for methamphetamine use as both groups had similar reductions in methamphetamine use from baseline to 6- and 12-month follow-ups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this sample of young adults attending residential treatment, individuals experienced improvements in both their substance use as well as well-being, vocational engagement, and mental health. These gains were largely maintained out to 1 year after entering treatment. Yet, an additional intervention, Grit, focused on strengths-based, wellbeing and self-regulation was not linked to improved results on most outcomes. Although the residential program where patients had exposure to the Grit intervention showed some relative improvements on methamphetamine and marijuana scores compared to the standard treatment, this group had higher use scores at baseline on these substances and were also more likely to be readmitted to treatment following discharge. This suggests these participants might have had more severe substance use profiles compared to the participants in the non-Grit, standard treatment condition, with more room to improve their substance use and so the improved results may not be solely due to the Grit program.
As both study conditions involved participants in an intensive 6-week residential program, it is possible that the additional Grit intervention did not address enough unique components necessary or did not address them in the right way or as intensively as needed, to boost recovery compared to the treatment that participants were already receiving. The location of the GRIT intervention also served a younger adult profile (18–35-year-olds) whereas the location of the comparison group served adults up to ages 65, so any differences between the conditions could have been due to the existing programming at each site and its developmental appropriateness for the sample in this study. In addition, there is no information on additional recovery support services that these young adults engaged in following their treatment episode, which could have differed between groups and can strong influences on recovery outcomes over time. Also, while gains made during treatment are largely maintained out to 1 year, 35% were readmitted to the treatment center at 3 months and others had attended another treatment program (14 new admission episodes by the 3-month and 44 new admission episodes by the 12-month follow-ups). The impact of further treatment on outcomes was not examined.
Although the study design of a cohort-controlled trial was used for several logistical reasons, the lack of randomization to study condition introduced potential confounding factors. That is, participants who were in one condition or the other as a result of where they chose (or had access) to attend treatment could also influence their outcomes during and after treatment. There may be other factors, aside from study condition, such as financial or social resources, that influenced both their treatment and their recovery outcomes. As well, the Grit intervention was delivered at the young adult specific residential treatment center where all residents were 18-35 years old. The other center where the control condition was delivered was for adults ages 18 and older. There may have been some key therapeutic aspects related to a young adult program that were part of the standard treatment approach and not unique to Grit leading to differing outcomes.
There was attrition from the study over time indicating there could be differences between those who completed later study visits compared to those who did not: retention ranged from 61% (12 months) to 81% (end of treatment, 6 weeks after baseline). The authors addressed this by conducting analyses where everyone who completed a baseline study visit were included in the analysis whether or not they completed the intervention, but this is still a large rate of study dropout, and it is not clear how the missing data on the outcomes were handled.
The short-term reductions in methamphetamine and marijuana use among the Grit participants could have been due to a statistical artifact known as regression to the mean; that is, over time, high levels of use often return to lower levels and because of the greater severity of use of these substances among the Grit group at baseline compared to the comparison condition, they had a greater likelihood of experiencing a greater reduction in use.
BOTTOM LINE
In this sample of young adults, standard residential treatment at both sites was associated with reductions in substance use scores and improvements in well-being, mental health, and vocational engagement that were maintained at the 12-month follow-up, but the addition of the novel Grit group intervention focused on improving well-being and self-regulation in part through mindfulness-based intervention did not, appear to have any meaningful or lasting effects.
For individuals and families seeking recovery: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether receiving continuing care such as through mutual help groups or recovery community organizations, with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research.
For treatment professionals and treatment systems: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average for this sample of young adults, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care such as through mutual help groups or recovery community organizations, with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research.
For scientists:Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research. The use of a cohort-controlled trial in this case made some interpretation of findings difficult. An alternative approach, such as an on-off design within each treatment center could be considered in the future to better understand which outcomes are results of the residential treatment program and which outcomes might be due to new/additional treatment components such as the Grit program examined here. Further work in this area to map and systematically assess the mechanisms of behavior change at work in these interventions is needed.
For policy makers: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average for this group of young adults, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research. Funding to support further research in these areas may help to identify and target key moderators (i.e., who benefits/doesn’t benefit) and mechanisms (i.e., why/why not) of treatment effects and enhance the precision and efficient delivery of interventions in these settings.
Recovery from substance use disorders typically involves both a) improvements in substance use either through reductions to non-symptomatic levels or abstinence and b) improvements to other aspects of quality of life, well-being, and overall functioning. For young adults, these recovery processes are occurring also in the context of achieving developmental milestones (for example, completing high school or starting full-time employment or college). For those at the most severe end of the spectrum of substance use disorders, residential treatment can help address an individual’s immediate and long-term needs by removing an individual from their high-risk environmental context, providing detoxification and medical stabilization, and giving them specific forms of treatment to address their substance use disorder. Ideally, this treatment provides an individual with skills that they can use when they exit treatment and return to their home, neighborhood, and place of work or school. Quality residential programs also help assertively link individuals to outpatient treatment and recovery support services in the community.
This study examined if adding a strengths-based group intervention (labeled the Grit Wellbeing and Self-regulation Program) could improve outcomes among young adults who attended residential treatment.
HOW WAS THIS STUDY CONDUCTED?
This was a cohort-controlled trial to examine whether among young adults in treatment, an additional group-based intervention produced meaningful recovery-related benefits. There were two participating residential treatment sites; patients attended the treatment site closest to where they lived (i.e., they were not randomized to attend a specific treatment site). Both provided similar standard 6-week residential treatment to adults, although one site served only 18–35-year-olds while the other served adults up to age 65. The site that served the younger adult population also provided an additional intervention, called “Grit,” which was described as a strengths-based, wellbeing and self-regulation program that incorporated some elements of mindfulness-based relapse prevention.
Grit was offered in 60-minute sessions given twice a week for 6 weeks by a clinical researcher and a member of the treatment staff. To be eligible for this study, patients had to be between the ages of 18-35 years old. Participants had assessments at baseline, treatment exit (6 weeks) and 3-, 6-, and 12-months after the baseline assessment.
Substance use outcomes were measured by the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (WHO ASSIST) a standardized scale that has been widely validated internationally. The key outcomes were (1) overall substance use score and (2) substance use score of the most common primary drugs of concern at the residential treatment centers (i.e., alcohol, methamphetamine, and cannabis). Secondary outcomes were well-being, mental health (depression and anxiety according to the PHQ-9 and the GAD-7), and past-month vocational engagement (defined as engaging in work or study).
In this analysis, the authors compared (1) baseline and 3-, 6-, and 12-month follow-ups for substance use and vocational engagement between the two conditions and compared (2) baseline to post-treatment (6 weeks) and 3-, 6-, and 12-month follow-ups for wellbeing and mental health between the two groups. All analyses controlled for key participant characteristics that differed between the two sites (i.e., age and having a child) and included all individuals who started the study regardless of whether they participated in follow-up assessments or not. For assessments not completed by a participant, the analytic approach functionally imputed missing scores by testing trajectories of participant outcomes. This approach is taken to decrease the chances that participant dropout will substantially impact the findings.
Of the sample of 230 young adults, the average age was 27 years old, 66% were male, 21% had a history of criminal justice involvement, and 35% had at least one child. The primary substances reported were amphetamines (45%: 93% of which was ice/crystal methamphetamine), alcohol (34%), and marijuana (15%). Participants remained in treatment (designed to last 6 weeks) for on average about a month (29 days). Participants who were in the treatment site where Grit was delivered had higher methamphetamine and marijuana use scores at baseline. They were also more likely to be readmitted to treatment following discharge than the standard treatment condition.
WHAT DID THIS STUDY FIND?
Intervention and comparison groups fared equally well on most outcomes.
Both groups reduced their overall and individual substance use scores (alcohol, marijuana, and methamphetamines). These reductions were maintained at the 12-month follow-up. Both groups also improved their well-being, increased their vocational engagement, and reduced symptoms of depression and anxiety.
The Grit group experienced a greater reduction in their methamphetamine use score compared to the standard treatment group from baseline to 3 months and a greater reduction in their marijuana use score compared to the standard treatment group over time, but the Grit group also had higher use scores of these substances at baseline and thus more room to improve. The Grit advantage was not maintained over time for methamphetamine use as both groups had similar reductions in methamphetamine use from baseline to 6- and 12-month follow-ups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this sample of young adults attending residential treatment, individuals experienced improvements in both their substance use as well as well-being, vocational engagement, and mental health. These gains were largely maintained out to 1 year after entering treatment. Yet, an additional intervention, Grit, focused on strengths-based, wellbeing and self-regulation was not linked to improved results on most outcomes. Although the residential program where patients had exposure to the Grit intervention showed some relative improvements on methamphetamine and marijuana scores compared to the standard treatment, this group had higher use scores at baseline on these substances and were also more likely to be readmitted to treatment following discharge. This suggests these participants might have had more severe substance use profiles compared to the participants in the non-Grit, standard treatment condition, with more room to improve their substance use and so the improved results may not be solely due to the Grit program.
As both study conditions involved participants in an intensive 6-week residential program, it is possible that the additional Grit intervention did not address enough unique components necessary or did not address them in the right way or as intensively as needed, to boost recovery compared to the treatment that participants were already receiving. The location of the GRIT intervention also served a younger adult profile (18–35-year-olds) whereas the location of the comparison group served adults up to ages 65, so any differences between the conditions could have been due to the existing programming at each site and its developmental appropriateness for the sample in this study. In addition, there is no information on additional recovery support services that these young adults engaged in following their treatment episode, which could have differed between groups and can strong influences on recovery outcomes over time. Also, while gains made during treatment are largely maintained out to 1 year, 35% were readmitted to the treatment center at 3 months and others had attended another treatment program (14 new admission episodes by the 3-month and 44 new admission episodes by the 12-month follow-ups). The impact of further treatment on outcomes was not examined.
Although the study design of a cohort-controlled trial was used for several logistical reasons, the lack of randomization to study condition introduced potential confounding factors. That is, participants who were in one condition or the other as a result of where they chose (or had access) to attend treatment could also influence their outcomes during and after treatment. There may be other factors, aside from study condition, such as financial or social resources, that influenced both their treatment and their recovery outcomes. As well, the Grit intervention was delivered at the young adult specific residential treatment center where all residents were 18-35 years old. The other center where the control condition was delivered was for adults ages 18 and older. There may have been some key therapeutic aspects related to a young adult program that were part of the standard treatment approach and not unique to Grit leading to differing outcomes.
There was attrition from the study over time indicating there could be differences between those who completed later study visits compared to those who did not: retention ranged from 61% (12 months) to 81% (end of treatment, 6 weeks after baseline). The authors addressed this by conducting analyses where everyone who completed a baseline study visit were included in the analysis whether or not they completed the intervention, but this is still a large rate of study dropout, and it is not clear how the missing data on the outcomes were handled.
The short-term reductions in methamphetamine and marijuana use among the Grit participants could have been due to a statistical artifact known as regression to the mean; that is, over time, high levels of use often return to lower levels and because of the greater severity of use of these substances among the Grit group at baseline compared to the comparison condition, they had a greater likelihood of experiencing a greater reduction in use.
BOTTOM LINE
In this sample of young adults, standard residential treatment at both sites was associated with reductions in substance use scores and improvements in well-being, mental health, and vocational engagement that were maintained at the 12-month follow-up, but the addition of the novel Grit group intervention focused on improving well-being and self-regulation in part through mindfulness-based intervention did not, appear to have any meaningful or lasting effects.
For individuals and families seeking recovery: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether receiving continuing care such as through mutual help groups or recovery community organizations, with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research.
For treatment professionals and treatment systems: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average for this sample of young adults, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care such as through mutual help groups or recovery community organizations, with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research.
For scientists:Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research. The use of a cohort-controlled trial in this case made some interpretation of findings difficult. An alternative approach, such as an on-off design within each treatment center could be considered in the future to better understand which outcomes are results of the residential treatment program and which outcomes might be due to new/additional treatment components such as the Grit program examined here. Further work in this area to map and systematically assess the mechanisms of behavior change at work in these interventions is needed.
For policy makers: Although residential treatment has shown to be helpful in facilitating remission and improvements in functioning and well-being overall, the addition of a twice-weekly hour-long group focused on enhancing well-being and emotion regulation through mindfulness training, did not appear to help. This does not necessarily mean that such approaches cannot be helpful for some people; just that, on average for this group of young adults, it was not associated with strong or lasting improvements. It is unclear whether a different style or intensity of this Grit intervention would have produced better results or whether providing continuing care with this Grit intervention over time during the year following discharge would also have done so. This is a question for future research. Funding to support further research in these areas may help to identify and target key moderators (i.e., who benefits/doesn’t benefit) and mechanisms (i.e., why/why not) of treatment effects and enhance the precision and efficient delivery of interventions in these settings.