
Recovery community centers: Is participation in these newer recovery support services associated with better functioning and quality of life?
Recovery Community Centers are a new type of organization which provide a range of services centered on the belief that people with addiction histories need access to resources beyond clinical stabilization, such as linkages to social recovery supports, housing, employment, and educational resources. This study provides a first look at the relationships between Recovery Community Center participation, members’ recovery resources (“recovery capital”), and their overall well-being. The authors found that centers may be particularly helpful for those with highest levels of clinical pathology and the lowest recovery capital. Participation in these recovery support services is associated with obtaining higher levels of recovery capital and quality of life and decreased levels of psychological distress.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Professional medical and psychological treatments and non-professional mutual-help organizations have long served as the primary supports for individuals seeking recovery from substance use disorder (SUD). However, the broader psychosocial supports, including personal, social, environmental, and cultural resources, which many find necessary for sustaining long term recovery are often missed by these resources. Recently, a new wave of organizations has emerged to fill this gap. Recovery Community Centers are non-profit, peer-led organizations which provide a range of services to support these broader psychosocial needs and are guided by the belief that there are many pathways to recovery.
Figure 1.
The “many pathways” of recovery philosophy within Recovery Community Centers means that they do not endorse any one recovery model, such as the medical model or Alcoholics Anonymous or Narcotics Anonymous. This allows these centers to serve and support members who may not align with one or more of the traditional philosophies of recovery. All Recovery Meetings, for example, which are “non-denominational” mutual help groups, support the many different pathways to SUD recovery, are a cornerstone of this approach.
Recovery capital is an umbrella term which is used to describe the broader psychosocial resources supported and provided by Recovery Community Centers. While there is evidence from multiple studies that access to recovery capital in the form of housing, employment, a supportive interpersonal network, and related resources are helpful for building and maintaining recovery, traditional forms of recovery support rarely provide such “one-stop” shopping to support these aspects of daily life. Therefore, while there is a theoretical reason to believe that Recovery Community Centers would be extremely valuable for recovery, until recently they were too new to have any empirical evidence supporting them. The authors of this study set out to begin the work of evaluating these centers systematically, examining whether Recovery Community Center participation is related to recovery capital, social support, and markers of well-being in this pilot investigation.
HOW WAS THIS STUDY CONDUCTED?
This was an online, cross-sectional survey study with 336 participants who were asked to provide information about their background, use of their Recovery Community Center, and their SUD recovery and well-being, in order to take a first look at how center participation is associated with recovery indices. The authors recruited volunteers from most (95%) of the Recovery Community Centers in New England and New York state. Staff at the 31 Recovery Community Centers posted flyers and told members about the study, and research study staff facilitated recruitment through visits to the centers and regular conference calls with center staff. Interested members participated using an open link to the online survey.
The survey asked participants to provide demographic, substance use history, and other background information, in order to describe the centers’ overall membership. It also included questions about the frequency and duration of members’ visits to Recovery Community Centers, which resources they used, and how helpful they found them. Finally, the survey included questionnaires on areas theorized to be impacted by Recovery Community Center membership and attendance. Specifically, the authors examined whether greater center participation – years attending the center, percent days attended in the past 90 days, and hours per visit, were associated with higher levels of recovery capital and social support. They also examined whether higher recovery capital and social support were, in turn, associated with higher overall quality of life, greater self-esteem, and less psychological distress.
The participants in this study were 41 years old on average, most (79%) identified as white, non-Hispanic, and half were female. More details on participants’ background are provided in the next section (What Did This Study Find?), since describing the background of Recovery Community Center members was one of the goals of this study.
WHAT DID THIS STUDY FIND?
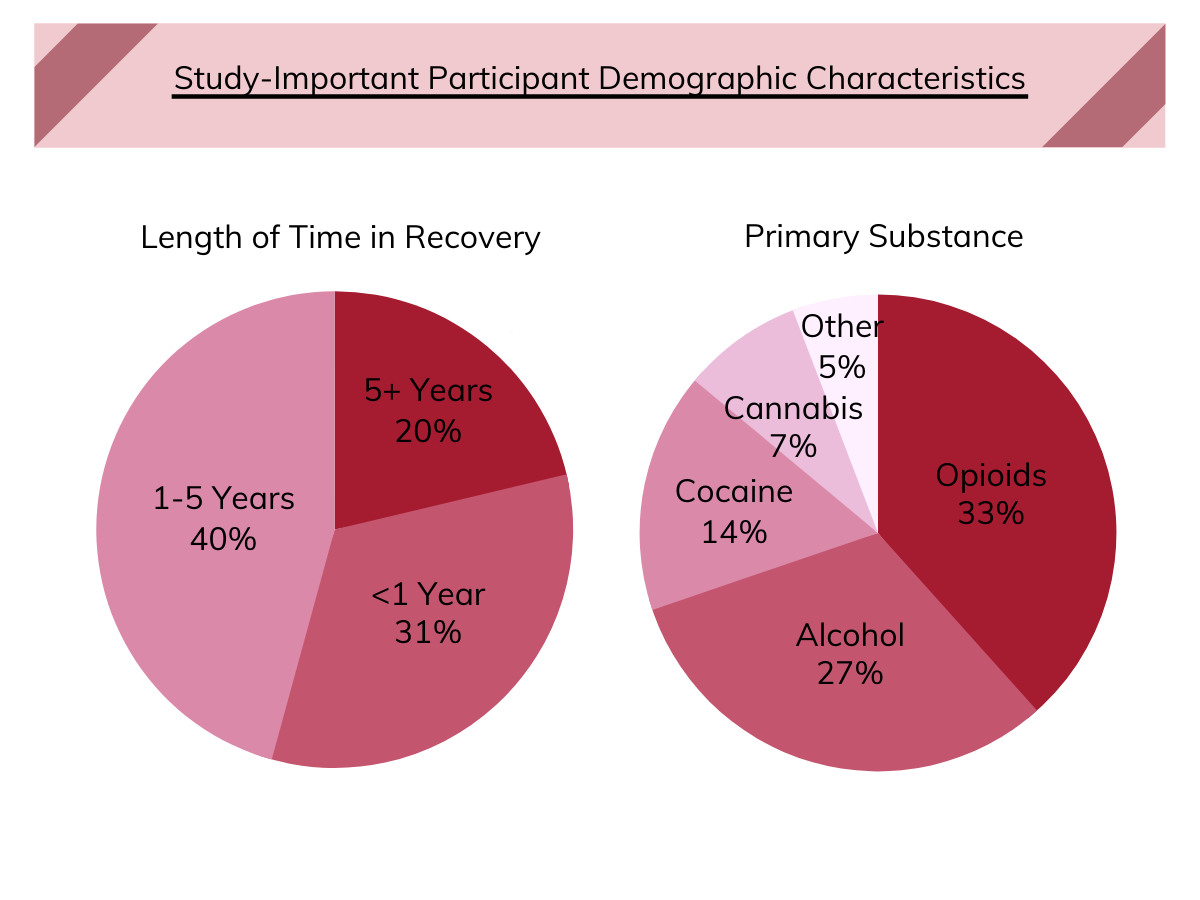
Figure 2.
Recovery Community Center members reported significant substance use disorder histories and limited financial and psychosocial resources.
Most participants described themselves as in recovery, with about 30% reporting duration under a year, a little over 40% in the one to five-year range, and about 20% more than five years in recovery. Participants had four years in recovery, on average. Opioids were the most common primary substance reported by participants (33%), followed by alcohol (27%), and cocaine (14%). History of using more than one substance was the rule rather than the exception (73%). Participants reported limited financial resources, with most (88%) reporting household incomes below $50,000 per year and 45% under $10,000. Only a minority of participants were employed full time (20%), and nearly half (46%) were currently unemployed. Nearly half (49%) reported a history of at least one mental health disorder diagnosis, and one-quarter (24%) reported current criminal justice involvement.
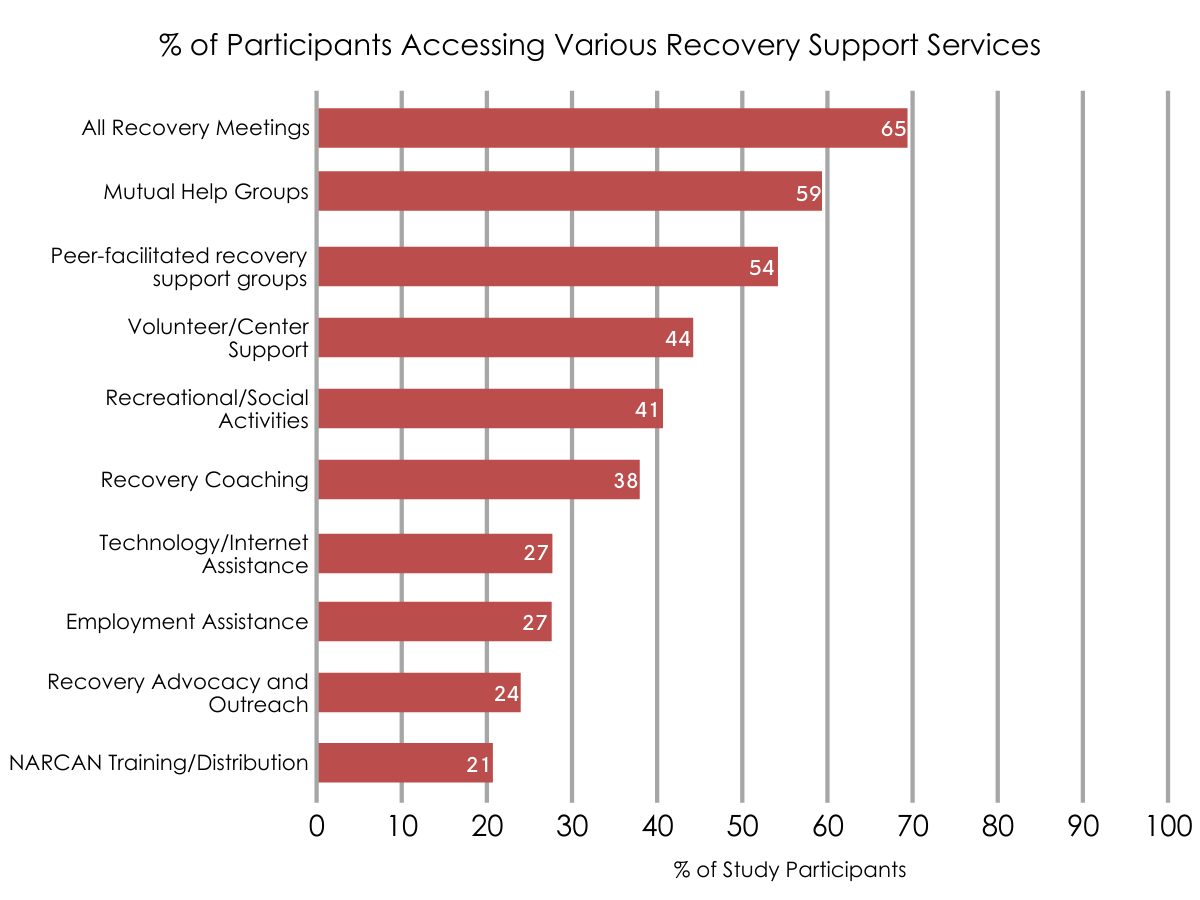
Figure 3.
Members visited their Recovery Community Center frequently, with All Recovery meetings the most commonly accessed service.
Traditional mutual-help and peer-facilitated groups were also attended by more than half of participants. However, members reported using a broad range of services, with recreational, vocational, and volunteer opportunities also among the top 10 most commonly used services. Importantly, members rates all of the 23 different services above a five (out of seven) on helpfulness. Some notable examples of less frequently accessed services included childcare, family support, and basic needs assistance, all of which were rated as extremely helpful by the members who used them. On average, members reported visiting their Recovery Community Center on nearly half (46%) of the last 90 days, staying for about three hours on average per visit.
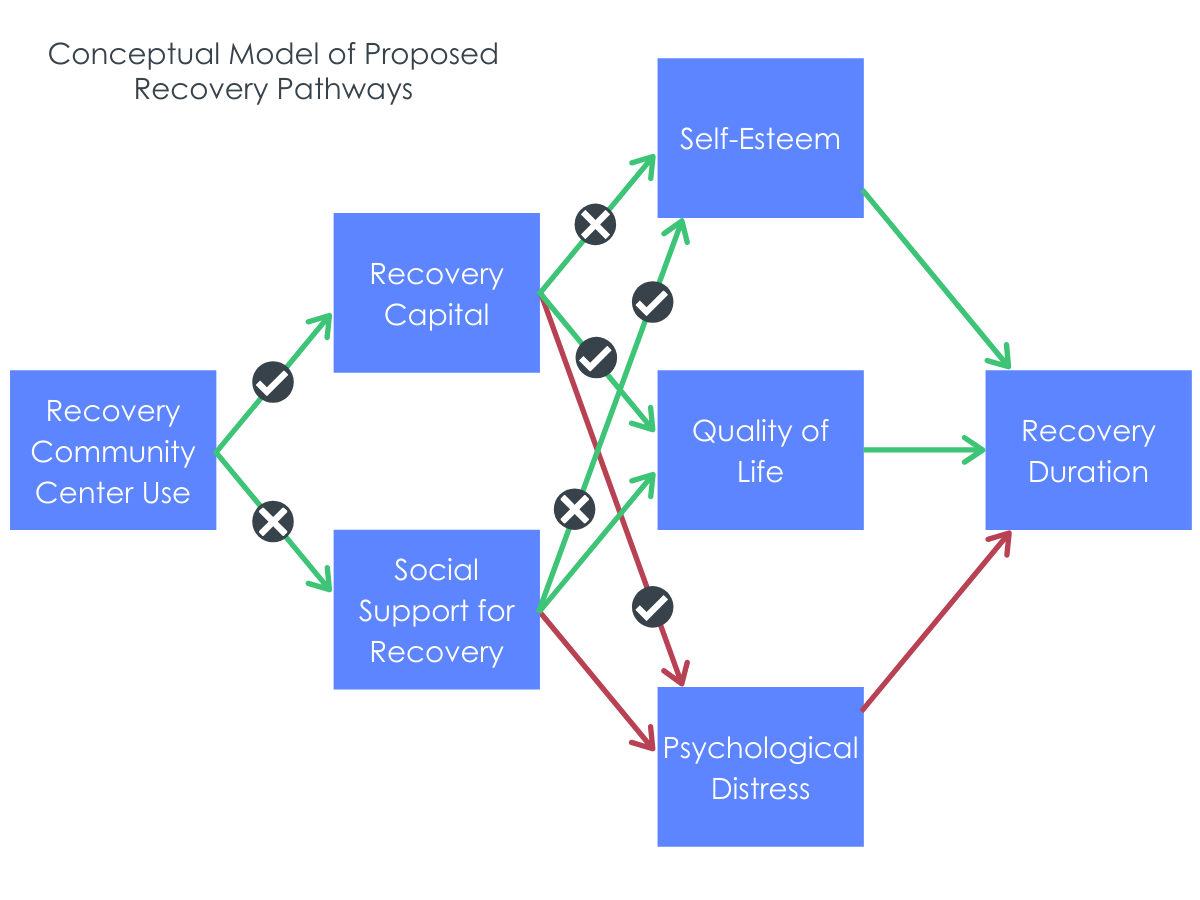
Figure 4. The conceptual model for the current study, which tested several of the proposed paths. Notably, use of RCCs were related to increases in recovery capital but not social support. In turn, recovery capital was associated with increases in self-esteem, quality of life, and decreases in distress.
Attending a Recovery Community Center regularly over time is associated with greater recovery capital, which in turn is associated with positive differences in quality of life and related outcomes.
The longer someone had attended a Recovery Community Center and the more time they spent there, the higher their recovery capital was. In turn, higher recovery capital among participants was related to higher quality of life and lower psychological distress. Length and amount of time spent attending a Recovery Community Center was unrelated to social support. High levels of social support, however, were associated with higher levels of self-esteem, suggesting that social support is important, but may be driven by other resources such as mutual help meetings, rather than center involvement specifically.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Recovery Community Centers are part of a national effort to provide the broad range of supports that many individuals need in order to build a stable life in recovery. A guiding principle of these centers is the belief that people need access to additional non-clinical resources (e.g., jobs, housing, education) and that there are many different recovery pathways – members need not align with any specific philosophy in order to engage with and benefit from services. The “many pathways” approach is consistent with research evidence, including a recent large, nationally representative study of individuals who resolved a significant substance use problem, which illustrated the range of different approaches to resolving a substance use disorder successfully.
Recovery Community Centers themselves are so new that there has been little direct research on their effects. In one of the first efforts to systematically examine these centers, the authors of this study found that Recovery Community Centers are reaching members with severe SUD histories and psychosocial needs, and that for members who regularly use center services more participation is associated with higher levels of recovery capital and overall well-being.
In fact, centers are so new that there was very little information on who is using their services. The participant characteristics in this study suggest that Recovery Community Centers are reaching those in the community who may need their services most, including individuals with opioid use disorder, who tend to experience severe psychosocial consequences relative to other substance use disorders. However, the majority of members were also white, non-Hispanic, and family and friends were the most common referral source. Thus, there may be room for additional outreach efforts to inform more diverse members of the community of the resources available in Recovery Community Centers. The authors of this study also showed that members make regular use of Recovery Community Center resources and report a very positive impression of them overall. Connection with others in recovery appears to be a critical resource offered by these centers. All Recovery Meetings, which are open to all and align with the unique perspective of the centers themselves, were the most commonly accessed service, closely followed by the other common types of recovery meetings. Importantly, the results of this study suggest that Recovery Community Center membership is associated with members’ recovery capital, which in turn is related to quality of life and psychological distress levels. This is the first evidence indicating that centers may indeed be filling a critical gap in recovery support services. Recovery capital levels were also associated (as expected) with quality of life and psychological distress levels.
Figure 5.
While these results are promising, there are a number of different areas for future research on Recovery Community Centers. For example, since this study was conducted in the densely populated northeast area of the United States, most Recovery Community Centers were likely close geographically to members’ homes. Digital resources, particularly live online video meetings, may be an area where centers can reach more remote community residents, particularly those with limited access to transportation. There are also ongoing efforts to add to the available services in this center. For example, some experts have proposed the provision of medications for opioid use disorder through these centers, and the large proportion of members in this study who reported a history of a primary opioid use disorder provide further support for this potential expansion of services.
- LIMITATIONS
-
- This study was cross sectional, meaning it collected information from participants at a single point in time, rather than following participants across multiple time points. This limits the authors’ ability to fully test their model in which Recovery Community Center use leads to increased recovery capital, which then leads to improvements in well-being, so future work would need to follow members across time to further validate this model.
- The study only included members of Recovery Community Centers located in New England and New York state. Within the U.S., there is significant geographical variation in substances used as well as related issues such as the approach of law enforcement to addressing substance use in the community. Thus, patterns and effects of Recovery Community Center use may vary across the country. New England and New York state also tend to have more financial resources available to fund public health initiatives like Recovery Community Centers.
- Participants were all volunteers and may not be representative of everyone who uses Recovery Community Centers. For example, study participants may have been some of the most invested members of the centers. While compensation for participants helps address the possibility that only the most invested members would participate in the study, the findings may not apply to all Recovery Community Center members even in the Northeast.
BOTTOM LINE
- For individuals and families seeking recovery: This study showed that members of Recovery Community Centers have levels of clinical problems and low levels of resources and those who participate more in these centers show increases in their recovery capital. This increase in recovery capital was in turn, related to increases in members’ quality of life and decrease in psychological distress levels. While this early study cannot determine for certain whether center involvement caused these positive outcomes, it is consistent with their theoretical rationale and purpose and an important first step in the research on these new centers. The study also showed that centers serve a membership who reports a history of severe SUD, and that members regularly use a range of services, which they rate as quite helpful. Recovery Community Centers are a new form of support that are expanding across the United States and have the potential to fill a gap in psychosocial recovery needs not addressed by traditional forms of recovery support. An important feature of these centers is their emphasis on All Recovery meetings, which support the centers’ mission to provide support for all comers and facilitate many different pathways to recovery from SUD. Recovery Community Centers also offer support for a range of challenges that are common in recovery, often including support for basic needs like housing, employment and legal services, as well as opportunities for recreation and volunteer work. For those who are engaged with other recovery support services, membership can serve as a supplement to formal treatment and mutual help involvement. To find a Recovery Community Center in your area, the Association of Recovery Community Organizations provides this helpful map of existing centers.
- For treatment professionals and treatment systems: This study showed that Recovery Community Centers are reaching a membership with histories of severe SUD and high levels of psychosocial need. Members accessed a range of the different services provided and rated these as very helpful. The more that members engaged with their center, the higher their recovery capital, and this was associated with better quality of life and lower psychological distress. While future research will need to determine whether center membership directly cause these positive outcomes, in the meantime membership is unlikely to be harmful and looks like it helps. Recovery Community Centers are a new resource which take a “many pathways to recovery” approach and are a valuable resource for anyone interested in pursuing recovery, regardless of their affiliation with traditional medical and/or mutual help models of recovery. Centers provide a range of services that are generally not offered by traditional treatment or mutual help organizations, including support for basic needs (housing, legal, employment support) and opportunities for recreation and volunteer work. Treatment professionals and systems which are located near existing centers may consider their local Recovery Community Center as an additional resource for supporting individuals in their recovery.
- For scientists: This cross-sectional study illustrates associations between Recovery Community Center membership and recovery capital, and the relationships between recovery capital and potential positive downstream effects on quality of life and psychological distress among members. The authors also provide an initial overview of center membership, services used, and ratings of services overall. Recovery Community Centers are non-profit, peer-led organizations which provide a range of services to support the broader psychosocial needs of many who are seeking recovery from SUD. These resources, known collectively as recovery capital, are generally associated with better long-term outcomes, so there is strong theoretical rationale for the potential effects of these centers for their members. The results from this initial cross-section examination are promising and support the value of further research on the effectiveness of Recovery Community Centers. Such work should examine the models’ proposed effects in a truly longitudinal manner. In other words, the next step will be to determine whether active membership leads to increased recovery capital over time, and whether psychological distress and quality of life improve as the result of this increased recovery capital. There is also potential benefit to examining any barriers to center use, since participants of this study were volunteers who were likely actively engaged in membership activities. Finally, regional variation in membership, service needs and use, and overall effects of centers is likely necessary in a country like the United States, where there is significant variation by region with respect to SUD, services, and general psychosocial supports.
- For policy makers: This study showed that Recovery Community Centers are reaching a membership with histories of severe SUD and high levels of psychosocial need. Members accessed a range of the different services provided and rated these highly in terms of helpfulness. Members who engaged more with their center also reported higher recovery capital, and this was associated with better quality of life and lower psychological distress. While additional research is needed in order to determine whether these relationships are causal in nature, center membership in the meantime is unlikely to cause harm for individuals in recovery from SUD and are likely to be helpful at least to some, and particularly those with the greatest needs. Recovery Community Centers are non-profit, peer-led organizations which provide a range of services to support the broader psychosocial needs of many who are seeking recovery from SUD. These resources, known collectively as recovery capital, are theorized to improve long-term outcomes, but there is limited research on the specific effects of these new centers for their members. The findings from this study, while preliminary in nature, do suggest that providing financial and policy support for local Recovery Community Center efforts may have a positive impact on community well-being. Policy makers may also play a role in helping the public to understand the nature of these centers, and the benefits of having such supports available in one’s home community.
CITATIONS
Kelly, J. F., Stout, R. L., Jason, L. A., Fallah‐Sohy, N., Hoffman, L. A., & Hoeppner, B. B. (2020). One‐stop shopping for recovery: An investigation of participant characteristics and benefits derived From U.S. recovery community centers. Alcoholism: Clinical and Experimental Research, 44(3), 711-721. doi: doi.org/10.1111/acer.14281
