Many recover from addiction, but how’s their well-being?
Definitions of recovery often extend beyond remission of symptoms to include well-being. At the same time, research in this domain lags behind, with little known about the prevalence or predictors of well-being. This national study explored rates of well-being among people in recovery, making comparisons to individuals with histories of other psychiatric conditions.
Treatment and recovery research on individuals with substance use disorder has broadened beyond changes in substance use and symptoms to include additional outcomes such as quality of life, mental health, physical health, and subjective well-being. In spite of this shift, very little is known about the attainment of general well-being in people in substance use disorder recovery, and other psychiatric conditions that commonly co-occur with addiction. Additionally, many first-line clinical treatments for substance used disorder like cognitive behavioral therapy largely focus on reducing symptoms with much less emphasis on cultivating quality of life and well-being. Greater understanding of recovery outcomes, such as well-being, would help identify targets for improving treatment, recovery supports, and other community-based resources.
In this study, the researchers examined what they termed optimal well-being among Canadians with lifetime history of psychiatric conditions including, substance use disorder, generalized anxiety disorder, major depressive disorder, and bipolar I and II disorders. They also reported rates of different psychiatric conditions in their nationally representative sample, with a breakdown of the frequency of lifetime diagnosis, current psychiatric diagnosis (i.e., a psychiatric condition active in the past 12 months), and diagnostic recovery (i.e., not currently or recently meeting diagnostic criteria for a psychiatric condition) for each psychiatric condition. Those without a history of psychiatric illness were also included in the study sample as a comparison group. The researchers defined optimal well-being as full recovery from any psychiatric conditions accompanied by high levels of psychological well-being and low levels of physical disability.
The researchers created a binary classification of optimal well-being (i.e., yes/no), which included three elements: 1) The absence of mental-health conditions in the past 12 months (i.e., substance use disorders, depressive disorder, anxiety disorders, bipolar disorders, and suicidal ideation or attempts), 2) the presence of psychological well-being, defined as being in the top 25% of the optimal sample, as assessed by the Mental Health Continuum–Short Form, and 3) low disability, defined as being in the bottom 25% of the optimal sample, as assessed from the World Health Organization Disability Assessment Schedule 2.0. They had to meet all 3 of these criteria to be considered as having “optimal well-being”.
The researchers reported the rate of optimal well-being for individuals with a lifetime history of each specific disorder. They also explored demographic and clinical correlates of optimal well-being.
In their nationally representative sample, lifetime mental-health condition rates were: Depression, 11.3%; substance use disorder, 8.7%; generalized anxiety disorder, 8.7%; bipolar I disorder, 0.9%: bipolar II disorder, 0.6%: and “any disorder,” 33.1%. Also, a substantial number of individuals also endorsed lifetime suicidal ideation, 8.2%.
WHAT DID THIS STUDY FIND?
Many were in remission, though only a sub-group had optimal well-being.
Of those who had a lifetime diagnosis of substance use disorder, 68.4% had achieved remission. This remission rate was much higher compared to bipolar I (34.9%), bipolar II (27.7%), and major depressive disorder (49.7%), but similar to generalized anxiety disorder (63.8%).
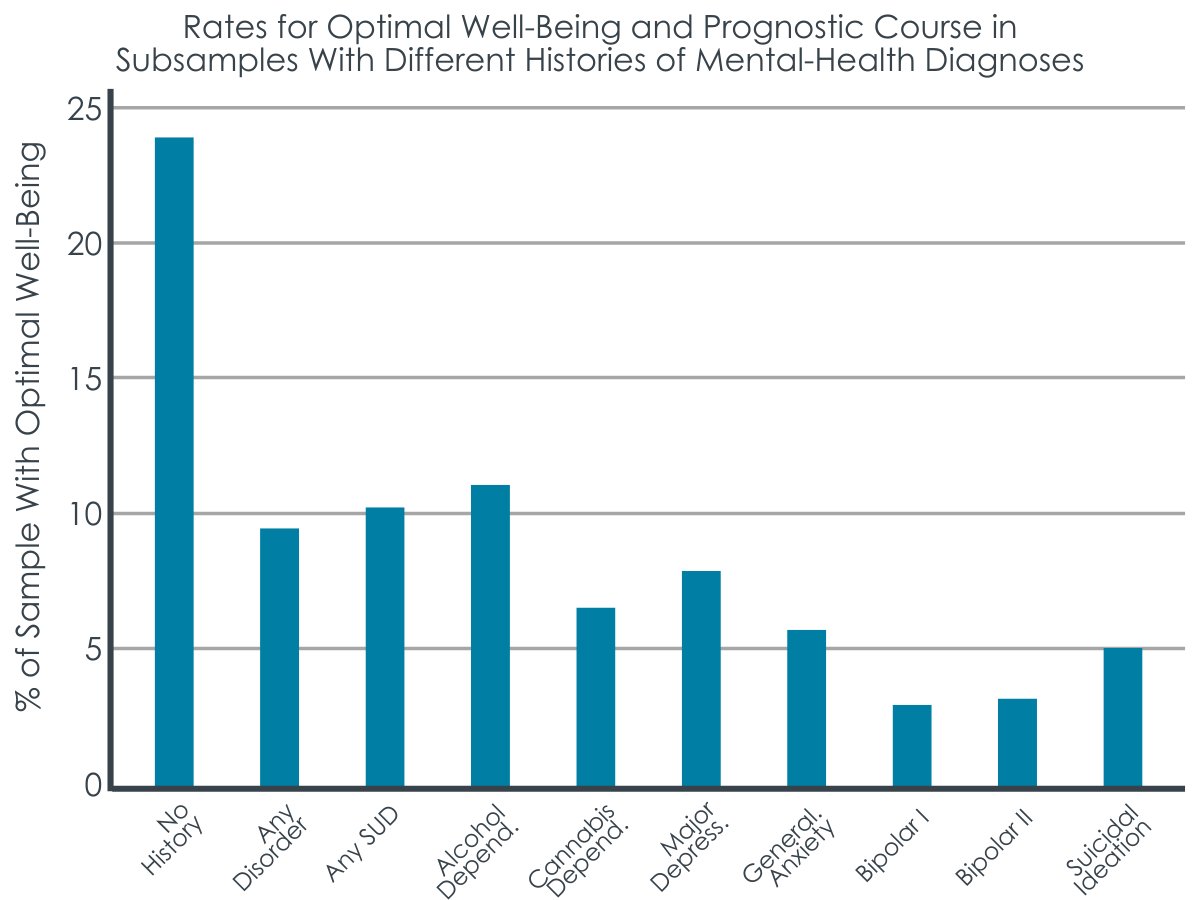
Only 9.8% of participants with any lifetime psychiatric disorder met the researchers’ criteria for optimal well-being, compared to 24.1% of participants with no history of psychiatric illness. Broken down by disorder, those with substance use disorder (10.2%) and depression (7.1%) had the highest rates of optimal well-being, followed by generalized anxiety (5.7%), suicidal ideation (5.0%), bipolar I (3.3%), and bipolar II (3.2%).
While the rate of optimal well-being for participants with a history of substance use disorder was 10.2%, when considering specific types of substance use disorders independently, rates differed. Those with alcohol use disorder had a slightly higher rate of optimal well-being (10.9%), while those with cannabis use disorder fared more poorly (6.3%), as did those with any drug use disorder (excluding alcohol and cannabis, 4.3%). The researchers also found that the absence of a history of cannabis use disorder and any drug use disorder (excluding alcohol and cannabis) was associated with an 89% and 95% greater probability respectively of having optimal well-being. Conversely, having alcohol use disorder was not associated with a clinically significant difference in probability of having optimal well-being.
A history of multiple psychiatric conditions was associated with lower odds of having optimal well-being.
Having two or more psychiatric conditions (including substance use disorder) was associated with much lower odds of having optimal well-being, even after statistically controlling for demographic differences among groups. Specifically, participants with only one lifetime mental-health condition had 4.2 times the odds of endorsing optimal well-being compared to participants with multiple lifetime conditions. Moreover, participants without a lifetime psychiatric condition had 6.0 times the odds of having optimal well-being compared with participants with multiple lifetime psychiatric conditions.
For those with a lifetime history of substance use disorder, demographic predictors of optimal well-being included older age, higher income, male gender, and identifying as non-White.
Having optimal well-being was associated with better health and life satisfaction.
The researchers also found that individuals with optimal well-being reported better overall health, higher life satisfaction, less need for mental-health care, and less psychological distress, compared with individuals not endorsing optimal well-being.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Notably, 68% of Canadians with a lifetime substance use disorder were in remission, which is a higher rate of remission than recently reported for the United States (47%). While this finding offers hope, it is tempered by the fact that only around 10% of this sample endorsed optimal well-being. This is in contrast to those without a history of psychiatric conditions, of whom 24% were considered to be experiencing optimal well-being.That said, those with a lifetime history of substance use disorder were much more likely to be experiencing optimal well-being compared to those with bipolar I and II disorders, and generalized anxiety disorder, suggesting relative to other conditions, substance use disorder is prognostically good, at least in terms of achieving well-being.
At the same time, these findings should be considered in the context of how the researchers’ defined optimal well-being. To be classified as experiencing optimal well-being participants needed to be in the top 25% of psychological well-being and bottom 25% of physical disability, after accounting for their gender and age. This equates to doing very well psychologically and physically. Many people in the sample with a lifetime history of substance use disorder may have been doing quite well psychologically and physically but not have made the researchers’ cutoff for optimal well-being. It’s possible that individuals with a lifetime history of substance use disorder are doing better in terms of well-being than these data suggest.
The researchers’ findings were also notable for highlighting the cumulative detrimental effects of experiencing multiple psychiatric disorders on optimal well-being. Participants with two or more psychiatric diagnoses were around four times less likely to be experiencing optimal well-being compared to those with one diagnosis, and six times less likely to be experiencing optimal well-being compared to those with no diagnosis. This is particularly important in the context of understanding the substance use disorder/well-being relationship because substance use disorder often co-occurs with other psychiatric conditions. This study did not tease out differences in well-being among individuals with lifetime substance use disorder history, with and without co-occurring psychiatric conditions, but this ideally will be addressed in future studies. The study also did not examine time in remission to see how longer durations of remission might be associated with greater well-being.
Though not directly assessed, this study also highlighted how recovery capital—the social, physical, human, cultural, and financial resources that support recovery—can influence well-being. For instance, the researchers’ observed a strong, positive relationship between income and well-being among participants with a history of substance use disorder. Specifically, those in the $80,000+ income bracket were almost four times more likely to be experiencing optimal well-being compared to those earning less than $20,000.
For those with a lifetime history of substance use disorder, demographic predictors of optimal well-being included identifying as non-White. This is surprising as a large body of public health literature indicates people who identify as White generally have greater resources and as a result, greater well-being. Future studies will need to more deeply explore this intriguing finding.
This study was cross-sectional, meaning participants were assessed at one point in time and only on past year remission. By its nature, this design does not allow for analyses of predictors and changes in well-being and psychiatric illness over time.
The data for this study was collected using retrospective self-report. It is possible that during their assessment, less severe disorders may not be recalled by participants, which may have led to underestimation of lifetime disorders.
Relatedly, it is possible that lifetime diagnoses of psychiatric conditions could be undercounted leading to an overrepresentation of severe mental health problems.
Well-being is experienced across a continuum. Although the focus by the researchers in optimal well-being has value, it will be helpful for future research to assess different levels of well-being in people in substance use disorder recovery.
Most studies like this have been done in Western countries like Canada and the US. It will be important for future research to investigate optimal well-being rates in non-Western nations and cultures, especially because the relationship between substance use disorder and well-being may differ in other nations and cultures.
This study did not tease out differences in well-being among individuals with lifetime substance use disorder, with and without other psychiatric conditions. Given the high cooccurrence of other psychiatric conditions with substance use disorder, this will be an important target for future research.
It is likely that individual’s recovery capital greatly influenced well-being in this study. This is an important factor that will be important to explore in future studies exploring the relationship between substance use disorder recovery and well-being.
BOTTOM LINE
This study is consistent with prior work showing that substance use disorder is a good prognosis condition; the majority of participants achieved remission, and a sub-group was thriving. Also, individuals with substance use disorder were on the whole more likely to be experiencing optimal well-being compared to individuals with other psychiatric disorders. Also, among those with substance use disorder, older individuals with more income had a greater likelihood of optimal well-being. For those who were not thriving, however, multiple psychiatric conditions greatly reduced the likelihood of experiencing optimal well-being. Taken together, results speak to the benefit of taking a broader perspective in addictions treatment that goes beyond symptom remission to include the accrual of psychological and physical well-being.
For individuals and families seeking recovery: People can and do recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse.
For treatment professionals and treatment systems: Most people will recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse. While substance use disorder treatment should of course focus on achieving symptom remission, it is also important that it considers cultivation of well-being. Patients will benefit from treatment approaches that promote well-being.
For scientists:This study provides important epidemiological data on well-being in individuals in substance use disorder remission. Future studies would greatly benefit the field by teasing out differences in well-being among individuals with lifetime substance use disorder, with and without psychiatric comorbidity. It will also be important for future studies in this domain to explore well-being as a continuous measure, and to explore how recovery capital influences well-being. Also given individuals with higher income were more likely to be experiencing optimal well-being, future studies could explore what specific factors are conferring benefits in this groups (e.g., better access to care, more social support, less financial strain and associated stress).
For policy makers: People can and do recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse. Programs that support individuals in recovery from substance use disorder beyond the acute phase of care, and support accrual of recovery capital, are likely to reduce relapse rates, improve public health, and in doing so reduce costs to healthcare systems.
Treatment and recovery research on individuals with substance use disorder has broadened beyond changes in substance use and symptoms to include additional outcomes such as quality of life, mental health, physical health, and subjective well-being. In spite of this shift, very little is known about the attainment of general well-being in people in substance use disorder recovery, and other psychiatric conditions that commonly co-occur with addiction. Additionally, many first-line clinical treatments for substance used disorder like cognitive behavioral therapy largely focus on reducing symptoms with much less emphasis on cultivating quality of life and well-being. Greater understanding of recovery outcomes, such as well-being, would help identify targets for improving treatment, recovery supports, and other community-based resources.
In this study, the researchers examined what they termed optimal well-being among Canadians with lifetime history of psychiatric conditions including, substance use disorder, generalized anxiety disorder, major depressive disorder, and bipolar I and II disorders. They also reported rates of different psychiatric conditions in their nationally representative sample, with a breakdown of the frequency of lifetime diagnosis, current psychiatric diagnosis (i.e., a psychiatric condition active in the past 12 months), and diagnostic recovery (i.e., not currently or recently meeting diagnostic criteria for a psychiatric condition) for each psychiatric condition. Those without a history of psychiatric illness were also included in the study sample as a comparison group. The researchers defined optimal well-being as full recovery from any psychiatric conditions accompanied by high levels of psychological well-being and low levels of physical disability.
The researchers created a binary classification of optimal well-being (i.e., yes/no), which included three elements: 1) The absence of mental-health conditions in the past 12 months (i.e., substance use disorders, depressive disorder, anxiety disorders, bipolar disorders, and suicidal ideation or attempts), 2) the presence of psychological well-being, defined as being in the top 25% of the optimal sample, as assessed by the Mental Health Continuum–Short Form, and 3) low disability, defined as being in the bottom 25% of the optimal sample, as assessed from the World Health Organization Disability Assessment Schedule 2.0. They had to meet all 3 of these criteria to be considered as having “optimal well-being”.
The researchers reported the rate of optimal well-being for individuals with a lifetime history of each specific disorder. They also explored demographic and clinical correlates of optimal well-being.
In their nationally representative sample, lifetime mental-health condition rates were: Depression, 11.3%; substance use disorder, 8.7%; generalized anxiety disorder, 8.7%; bipolar I disorder, 0.9%: bipolar II disorder, 0.6%: and “any disorder,” 33.1%. Also, a substantial number of individuals also endorsed lifetime suicidal ideation, 8.2%.
WHAT DID THIS STUDY FIND?
Many were in remission, though only a sub-group had optimal well-being.
Of those who had a lifetime diagnosis of substance use disorder, 68.4% had achieved remission. This remission rate was much higher compared to bipolar I (34.9%), bipolar II (27.7%), and major depressive disorder (49.7%), but similar to generalized anxiety disorder (63.8%).
Only 9.8% of participants with any lifetime psychiatric disorder met the researchers’ criteria for optimal well-being, compared to 24.1% of participants with no history of psychiatric illness. Broken down by disorder, those with substance use disorder (10.2%) and depression (7.1%) had the highest rates of optimal well-being, followed by generalized anxiety (5.7%), suicidal ideation (5.0%), bipolar I (3.3%), and bipolar II (3.2%).
While the rate of optimal well-being for participants with a history of substance use disorder was 10.2%, when considering specific types of substance use disorders independently, rates differed. Those with alcohol use disorder had a slightly higher rate of optimal well-being (10.9%), while those with cannabis use disorder fared more poorly (6.3%), as did those with any drug use disorder (excluding alcohol and cannabis, 4.3%). The researchers also found that the absence of a history of cannabis use disorder and any drug use disorder (excluding alcohol and cannabis) was associated with an 89% and 95% greater probability respectively of having optimal well-being. Conversely, having alcohol use disorder was not associated with a clinically significant difference in probability of having optimal well-being.
A history of multiple psychiatric conditions was associated with lower odds of having optimal well-being.
Having two or more psychiatric conditions (including substance use disorder) was associated with much lower odds of having optimal well-being, even after statistically controlling for demographic differences among groups. Specifically, participants with only one lifetime mental-health condition had 4.2 times the odds of endorsing optimal well-being compared to participants with multiple lifetime conditions. Moreover, participants without a lifetime psychiatric condition had 6.0 times the odds of having optimal well-being compared with participants with multiple lifetime psychiatric conditions.
For those with a lifetime history of substance use disorder, demographic predictors of optimal well-being included older age, higher income, male gender, and identifying as non-White.
Having optimal well-being was associated with better health and life satisfaction.
The researchers also found that individuals with optimal well-being reported better overall health, higher life satisfaction, less need for mental-health care, and less psychological distress, compared with individuals not endorsing optimal well-being.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Notably, 68% of Canadians with a lifetime substance use disorder were in remission, which is a higher rate of remission than recently reported for the United States (47%). While this finding offers hope, it is tempered by the fact that only around 10% of this sample endorsed optimal well-being. This is in contrast to those without a history of psychiatric conditions, of whom 24% were considered to be experiencing optimal well-being.That said, those with a lifetime history of substance use disorder were much more likely to be experiencing optimal well-being compared to those with bipolar I and II disorders, and generalized anxiety disorder, suggesting relative to other conditions, substance use disorder is prognostically good, at least in terms of achieving well-being.
At the same time, these findings should be considered in the context of how the researchers’ defined optimal well-being. To be classified as experiencing optimal well-being participants needed to be in the top 25% of psychological well-being and bottom 25% of physical disability, after accounting for their gender and age. This equates to doing very well psychologically and physically. Many people in the sample with a lifetime history of substance use disorder may have been doing quite well psychologically and physically but not have made the researchers’ cutoff for optimal well-being. It’s possible that individuals with a lifetime history of substance use disorder are doing better in terms of well-being than these data suggest.
The researchers’ findings were also notable for highlighting the cumulative detrimental effects of experiencing multiple psychiatric disorders on optimal well-being. Participants with two or more psychiatric diagnoses were around four times less likely to be experiencing optimal well-being compared to those with one diagnosis, and six times less likely to be experiencing optimal well-being compared to those with no diagnosis. This is particularly important in the context of understanding the substance use disorder/well-being relationship because substance use disorder often co-occurs with other psychiatric conditions. This study did not tease out differences in well-being among individuals with lifetime substance use disorder history, with and without co-occurring psychiatric conditions, but this ideally will be addressed in future studies. The study also did not examine time in remission to see how longer durations of remission might be associated with greater well-being.
Though not directly assessed, this study also highlighted how recovery capital—the social, physical, human, cultural, and financial resources that support recovery—can influence well-being. For instance, the researchers’ observed a strong, positive relationship between income and well-being among participants with a history of substance use disorder. Specifically, those in the $80,000+ income bracket were almost four times more likely to be experiencing optimal well-being compared to those earning less than $20,000.
For those with a lifetime history of substance use disorder, demographic predictors of optimal well-being included identifying as non-White. This is surprising as a large body of public health literature indicates people who identify as White generally have greater resources and as a result, greater well-being. Future studies will need to more deeply explore this intriguing finding.
This study was cross-sectional, meaning participants were assessed at one point in time and only on past year remission. By its nature, this design does not allow for analyses of predictors and changes in well-being and psychiatric illness over time.
The data for this study was collected using retrospective self-report. It is possible that during their assessment, less severe disorders may not be recalled by participants, which may have led to underestimation of lifetime disorders.
Relatedly, it is possible that lifetime diagnoses of psychiatric conditions could be undercounted leading to an overrepresentation of severe mental health problems.
Well-being is experienced across a continuum. Although the focus by the researchers in optimal well-being has value, it will be helpful for future research to assess different levels of well-being in people in substance use disorder recovery.
Most studies like this have been done in Western countries like Canada and the US. It will be important for future research to investigate optimal well-being rates in non-Western nations and cultures, especially because the relationship between substance use disorder and well-being may differ in other nations and cultures.
This study did not tease out differences in well-being among individuals with lifetime substance use disorder, with and without other psychiatric conditions. Given the high cooccurrence of other psychiatric conditions with substance use disorder, this will be an important target for future research.
It is likely that individual’s recovery capital greatly influenced well-being in this study. This is an important factor that will be important to explore in future studies exploring the relationship between substance use disorder recovery and well-being.
BOTTOM LINE
This study is consistent with prior work showing that substance use disorder is a good prognosis condition; the majority of participants achieved remission, and a sub-group was thriving. Also, individuals with substance use disorder were on the whole more likely to be experiencing optimal well-being compared to individuals with other psychiatric disorders. Also, among those with substance use disorder, older individuals with more income had a greater likelihood of optimal well-being. For those who were not thriving, however, multiple psychiatric conditions greatly reduced the likelihood of experiencing optimal well-being. Taken together, results speak to the benefit of taking a broader perspective in addictions treatment that goes beyond symptom remission to include the accrual of psychological and physical well-being.
For individuals and families seeking recovery: People can and do recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse.
For treatment professionals and treatment systems: Most people will recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse. While substance use disorder treatment should of course focus on achieving symptom remission, it is also important that it considers cultivation of well-being. Patients will benefit from treatment approaches that promote well-being.
For scientists:This study provides important epidemiological data on well-being in individuals in substance use disorder remission. Future studies would greatly benefit the field by teasing out differences in well-being among individuals with lifetime substance use disorder, with and without psychiatric comorbidity. It will also be important for future studies in this domain to explore well-being as a continuous measure, and to explore how recovery capital influences well-being. Also given individuals with higher income were more likely to be experiencing optimal well-being, future studies could explore what specific factors are conferring benefits in this groups (e.g., better access to care, more social support, less financial strain and associated stress).
For policy makers: People can and do recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse. Programs that support individuals in recovery from substance use disorder beyond the acute phase of care, and support accrual of recovery capital, are likely to reduce relapse rates, improve public health, and in doing so reduce costs to healthcare systems.
Treatment and recovery research on individuals with substance use disorder has broadened beyond changes in substance use and symptoms to include additional outcomes such as quality of life, mental health, physical health, and subjective well-being. In spite of this shift, very little is known about the attainment of general well-being in people in substance use disorder recovery, and other psychiatric conditions that commonly co-occur with addiction. Additionally, many first-line clinical treatments for substance used disorder like cognitive behavioral therapy largely focus on reducing symptoms with much less emphasis on cultivating quality of life and well-being. Greater understanding of recovery outcomes, such as well-being, would help identify targets for improving treatment, recovery supports, and other community-based resources.
In this study, the researchers examined what they termed optimal well-being among Canadians with lifetime history of psychiatric conditions including, substance use disorder, generalized anxiety disorder, major depressive disorder, and bipolar I and II disorders. They also reported rates of different psychiatric conditions in their nationally representative sample, with a breakdown of the frequency of lifetime diagnosis, current psychiatric diagnosis (i.e., a psychiatric condition active in the past 12 months), and diagnostic recovery (i.e., not currently or recently meeting diagnostic criteria for a psychiatric condition) for each psychiatric condition. Those without a history of psychiatric illness were also included in the study sample as a comparison group. The researchers defined optimal well-being as full recovery from any psychiatric conditions accompanied by high levels of psychological well-being and low levels of physical disability.
The researchers created a binary classification of optimal well-being (i.e., yes/no), which included three elements: 1) The absence of mental-health conditions in the past 12 months (i.e., substance use disorders, depressive disorder, anxiety disorders, bipolar disorders, and suicidal ideation or attempts), 2) the presence of psychological well-being, defined as being in the top 25% of the optimal sample, as assessed by the Mental Health Continuum–Short Form, and 3) low disability, defined as being in the bottom 25% of the optimal sample, as assessed from the World Health Organization Disability Assessment Schedule 2.0. They had to meet all 3 of these criteria to be considered as having “optimal well-being”.
The researchers reported the rate of optimal well-being for individuals with a lifetime history of each specific disorder. They also explored demographic and clinical correlates of optimal well-being.
In their nationally representative sample, lifetime mental-health condition rates were: Depression, 11.3%; substance use disorder, 8.7%; generalized anxiety disorder, 8.7%; bipolar I disorder, 0.9%: bipolar II disorder, 0.6%: and “any disorder,” 33.1%. Also, a substantial number of individuals also endorsed lifetime suicidal ideation, 8.2%.
WHAT DID THIS STUDY FIND?
Many were in remission, though only a sub-group had optimal well-being.
Of those who had a lifetime diagnosis of substance use disorder, 68.4% had achieved remission. This remission rate was much higher compared to bipolar I (34.9%), bipolar II (27.7%), and major depressive disorder (49.7%), but similar to generalized anxiety disorder (63.8%).
Only 9.8% of participants with any lifetime psychiatric disorder met the researchers’ criteria for optimal well-being, compared to 24.1% of participants with no history of psychiatric illness. Broken down by disorder, those with substance use disorder (10.2%) and depression (7.1%) had the highest rates of optimal well-being, followed by generalized anxiety (5.7%), suicidal ideation (5.0%), bipolar I (3.3%), and bipolar II (3.2%).
While the rate of optimal well-being for participants with a history of substance use disorder was 10.2%, when considering specific types of substance use disorders independently, rates differed. Those with alcohol use disorder had a slightly higher rate of optimal well-being (10.9%), while those with cannabis use disorder fared more poorly (6.3%), as did those with any drug use disorder (excluding alcohol and cannabis, 4.3%). The researchers also found that the absence of a history of cannabis use disorder and any drug use disorder (excluding alcohol and cannabis) was associated with an 89% and 95% greater probability respectively of having optimal well-being. Conversely, having alcohol use disorder was not associated with a clinically significant difference in probability of having optimal well-being.
A history of multiple psychiatric conditions was associated with lower odds of having optimal well-being.
Having two or more psychiatric conditions (including substance use disorder) was associated with much lower odds of having optimal well-being, even after statistically controlling for demographic differences among groups. Specifically, participants with only one lifetime mental-health condition had 4.2 times the odds of endorsing optimal well-being compared to participants with multiple lifetime conditions. Moreover, participants without a lifetime psychiatric condition had 6.0 times the odds of having optimal well-being compared with participants with multiple lifetime psychiatric conditions.
For those with a lifetime history of substance use disorder, demographic predictors of optimal well-being included older age, higher income, male gender, and identifying as non-White.
Having optimal well-being was associated with better health and life satisfaction.
The researchers also found that individuals with optimal well-being reported better overall health, higher life satisfaction, less need for mental-health care, and less psychological distress, compared with individuals not endorsing optimal well-being.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Notably, 68% of Canadians with a lifetime substance use disorder were in remission, which is a higher rate of remission than recently reported for the United States (47%). While this finding offers hope, it is tempered by the fact that only around 10% of this sample endorsed optimal well-being. This is in contrast to those without a history of psychiatric conditions, of whom 24% were considered to be experiencing optimal well-being.That said, those with a lifetime history of substance use disorder were much more likely to be experiencing optimal well-being compared to those with bipolar I and II disorders, and generalized anxiety disorder, suggesting relative to other conditions, substance use disorder is prognostically good, at least in terms of achieving well-being.
At the same time, these findings should be considered in the context of how the researchers’ defined optimal well-being. To be classified as experiencing optimal well-being participants needed to be in the top 25% of psychological well-being and bottom 25% of physical disability, after accounting for their gender and age. This equates to doing very well psychologically and physically. Many people in the sample with a lifetime history of substance use disorder may have been doing quite well psychologically and physically but not have made the researchers’ cutoff for optimal well-being. It’s possible that individuals with a lifetime history of substance use disorder are doing better in terms of well-being than these data suggest.
The researchers’ findings were also notable for highlighting the cumulative detrimental effects of experiencing multiple psychiatric disorders on optimal well-being. Participants with two or more psychiatric diagnoses were around four times less likely to be experiencing optimal well-being compared to those with one diagnosis, and six times less likely to be experiencing optimal well-being compared to those with no diagnosis. This is particularly important in the context of understanding the substance use disorder/well-being relationship because substance use disorder often co-occurs with other psychiatric conditions. This study did not tease out differences in well-being among individuals with lifetime substance use disorder history, with and without co-occurring psychiatric conditions, but this ideally will be addressed in future studies. The study also did not examine time in remission to see how longer durations of remission might be associated with greater well-being.
Though not directly assessed, this study also highlighted how recovery capital—the social, physical, human, cultural, and financial resources that support recovery—can influence well-being. For instance, the researchers’ observed a strong, positive relationship between income and well-being among participants with a history of substance use disorder. Specifically, those in the $80,000+ income bracket were almost four times more likely to be experiencing optimal well-being compared to those earning less than $20,000.
For those with a lifetime history of substance use disorder, demographic predictors of optimal well-being included identifying as non-White. This is surprising as a large body of public health literature indicates people who identify as White generally have greater resources and as a result, greater well-being. Future studies will need to more deeply explore this intriguing finding.
This study was cross-sectional, meaning participants were assessed at one point in time and only on past year remission. By its nature, this design does not allow for analyses of predictors and changes in well-being and psychiatric illness over time.
The data for this study was collected using retrospective self-report. It is possible that during their assessment, less severe disorders may not be recalled by participants, which may have led to underestimation of lifetime disorders.
Relatedly, it is possible that lifetime diagnoses of psychiatric conditions could be undercounted leading to an overrepresentation of severe mental health problems.
Well-being is experienced across a continuum. Although the focus by the researchers in optimal well-being has value, it will be helpful for future research to assess different levels of well-being in people in substance use disorder recovery.
Most studies like this have been done in Western countries like Canada and the US. It will be important for future research to investigate optimal well-being rates in non-Western nations and cultures, especially because the relationship between substance use disorder and well-being may differ in other nations and cultures.
This study did not tease out differences in well-being among individuals with lifetime substance use disorder, with and without other psychiatric conditions. Given the high cooccurrence of other psychiatric conditions with substance use disorder, this will be an important target for future research.
It is likely that individual’s recovery capital greatly influenced well-being in this study. This is an important factor that will be important to explore in future studies exploring the relationship between substance use disorder recovery and well-being.
BOTTOM LINE
This study is consistent with prior work showing that substance use disorder is a good prognosis condition; the majority of participants achieved remission, and a sub-group was thriving. Also, individuals with substance use disorder were on the whole more likely to be experiencing optimal well-being compared to individuals with other psychiatric disorders. Also, among those with substance use disorder, older individuals with more income had a greater likelihood of optimal well-being. For those who were not thriving, however, multiple psychiatric conditions greatly reduced the likelihood of experiencing optimal well-being. Taken together, results speak to the benefit of taking a broader perspective in addictions treatment that goes beyond symptom remission to include the accrual of psychological and physical well-being.
For individuals and families seeking recovery: People can and do recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse.
For treatment professionals and treatment systems: Most people will recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse. While substance use disorder treatment should of course focus on achieving symptom remission, it is also important that it considers cultivation of well-being. Patients will benefit from treatment approaches that promote well-being.
For scientists:This study provides important epidemiological data on well-being in individuals in substance use disorder remission. Future studies would greatly benefit the field by teasing out differences in well-being among individuals with lifetime substance use disorder, with and without psychiatric comorbidity. It will also be important for future studies in this domain to explore well-being as a continuous measure, and to explore how recovery capital influences well-being. Also given individuals with higher income were more likely to be experiencing optimal well-being, future studies could explore what specific factors are conferring benefits in this groups (e.g., better access to care, more social support, less financial strain and associated stress).
For policy makers: People can and do recover from substance use disorder and go on to thrive. Though achieving well-being is contingent on numerous factors—many outside of our control—cultivating well-being in addiction recovery confers numerous benefits including increasing quality of life and buffering against addiction relapse. Programs that support individuals in recovery from substance use disorder beyond the acute phase of care, and support accrual of recovery capital, are likely to reduce relapse rates, improve public health, and in doing so reduce costs to healthcare systems.