Who is most likely to follow through with a prescription for extended-release buprenorphine?
Naturalistic research on extended-release buprenorphine for opioid use disorder can provide meaningful information regarding the real-world effectiveness of this medication. Studies like these build on rigorous clinical trials showing they outperform placebo and do as well as more commonly prescribed daily buprenorphine. In an addiction medicine specialty clinic, this study compared patients who were prescribed the medication and received it versus those who were prescribed it but did not receive it.
Approximately 6 million people in the United States met criteria for an opioid use disorder in 2022, and there have been persistent year over year increases in opioid-related mortality. Compared to other primary substances, having a primary opioid problem is associated with a similar number of attempts needed to initiate recovery compared to other primary substances but more psychosocial challenges after initiating recovery. Currently, medications for opioid use disorder are first-line, empirically-supported approaches for reducing opioid mortality and increasing likelihood of remission from opioid use disorder. Medications such as buprenorphine are agonists that bind to opioid receptor sites in the brain but act more slowly and with less potency than other opioids. As a result, they reduce cravings and symptoms of withdrawal while blocking other opioids (e.g., heroin), yet without producing opioid-related euphoric effects when used as prescribed. Despite the fact that these medications are helpful, in 2022 only an estimated 18% of people diagnosed with opioid use disorder have used a medication for opioid use disorder that they were prescribed. Even among those who receive an opioid use disorder medication, the challenges accompanying opioid use disorder recovery (e.g., housing instability, mental health difficulties, environmental cues/triggers, etc.) make daily medication regiments difficult for some. In 2017, the U.S. Food and Drug Administration approved a once monthly injectable dose of buprenorphine to help address these potential issues. Data shows this extended-release buprenorphine formulation outperforms placebo injections and does as well as daily sublingual buprenorphine. Yet approximately half of individuals prescribed extended-release buprenorphine discontinue within 1 year. There is a critical need for naturalistic research to understand factors associated with initiation of extended-release buprenorphine and factors that predict ongoing engagement with this injectable medication.
This study examined patient characteristics associated with taking at least one dose of extended-release buprenorphine among those who were prescribed this medication in a low-barrier addiction medicine specialty clinic. The study also examined predictors of the number of doses taken, and treatment retention after 6 months.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of cross-sectional data extracted from the electronic health record (EHR) of an outpatient addiction medicine clinic at an academic medical center examining factors associated with initiating buprenorphine (baseline) and retention (6-month follow-up). The researchers identified all participants who were prescribed extended-release buprenorphine in this addiction medicine clinic between December 2018 and December 2020. Data was extracted via manual free text chart review. Variables extracted from patient charts included gender, race, primary opioid type and route of administration prior to remission, housing status, presence of a co-occurring mental health diagnosis, presence of co-occurring substance use disorder apart from opioid (e.g., stimulant use disorder), reason for prescribing extended-release buprenorphine (“unstable” remission, patient preference, or other), insurance type (public or private), and whether patients were prescribed a supplemental daily dose of buprenorphine at any point during the data extraction period. Notably, the study could not account for services received outside the addiction medicine clinic where the study took place or community-based recovery support services. Whether patients were prescribed extended-release buprenorphine prior to the FDA’s recommended 7-day stabilization period on daily buprenorphine, number of doses received over 6 months, and treatment retention at 6 months (any addiction medicine visit within 6 months of the index buprenorphine injection) were each obtained from patient charts.
Researchers first examined the likelihood of initiating extended-release buprenorphine among those receiving a prescription and factors associated with initiation. Next, they examined factors associated with treatment retention and urine drug test results 6 months after receiving the prescription. All models controlled statistically for the documented demographic and clinical characteristics noted above.
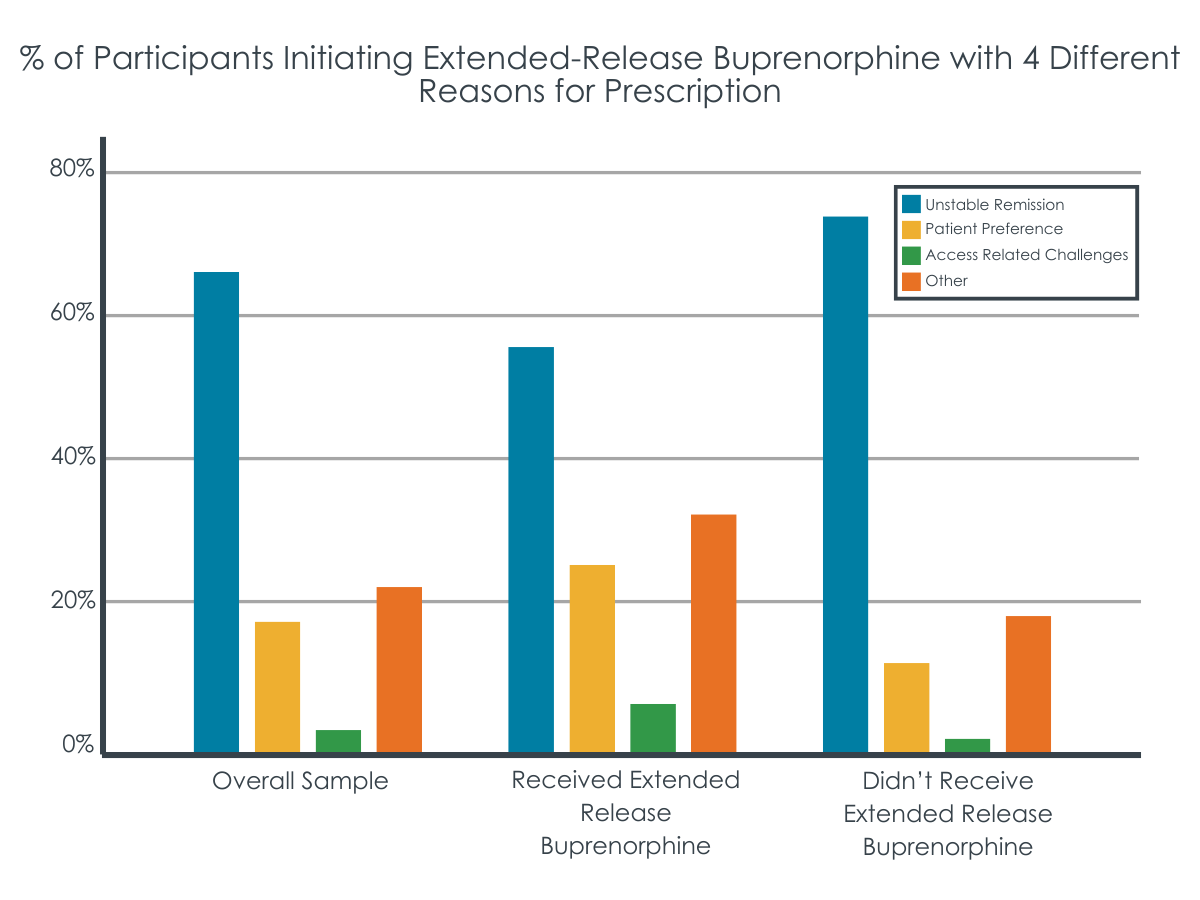
The sample of 233 adults were 39 years old on average, more likely to be male (62.2%), non-Hispanic White (63.8%), use public insurance (93.6%), have stable housing (79%). Almost two-thirds (62.2%) had co-occurring opioid and another substance use disorder, 58.4% had a current co-occurring mental health condition, and 65.2% were prescribed extended-release buprenorphine due to unstable remission for opioid use disorder.
WHAT DID THIS STUDY FIND?
Clinical stability associated with receiving a buprenorphine injection.
Among the full sample, 56% initiated extended-release buprenorphine after receiving a prescription. Initiation took a median time of 28 days to first dose. On average, patients received 3.7 extended-release buprenorphine injections during the 6-month period. Approximately one-third received all 6 doses.
Having a co-occurring substance use disorder (e.g., stimulant) and being prescribed extended-release buprenorphine for a reason other than unstable course of remission for opioid use disorder (e.g., patient preference) was associated with a much greater likelihood of initiating extended-release buprenorphine.
Among those receiving at least one dose of extended-release buprenorphine, those initiating extended-release buprenorphine prior to the recommended 7-day daily dose stabilization phase were less likely to receive all 6 maintenance doses (0 %) compared to 2–5 doses (13.2 %) or 1 dose (4.2 %). Those prescribed a supplemental daily dose of buprenorphine were more likely to receive more than one injection compared to receiving a single dose.
More clinical and psychosocial challenges associated with lower treatment retention.
Those with private insurance, relative to public, were more likely to remain in treatment at 6-month follow-up. Further, those with a mental health diagnosis were more likely to remain in treatment at 6-month follow-up relative to those without co-occurring mental health conditions. Those prescribed extended-release buprenorphine due to having an unstable course of remission were less likely to be retained in treatment. Independent of these and other demographic and clinical factors, those initiating extended-release buprenorphine were 4.8 times more likely to be retained in treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The current study replicated previous studies by demonstrating that half of those prescribed extended-release buprenorphine actually took at least one dose, with only 1/3 of those who received a single dose completing all 6 doses during the study period. These findings highlight the importance of understanding full cascades of care and may demonstrate that enhanced access and availability are “necessary, but not sufficient” to receiving extended-release opioid use disorder medications. Though increasing availability of such a treatment may be effective in reducing overdose and increasing rates of opioid use disorder remission, other important factors may also need to be addressed in order to maximize real world impact of these FDA-approved medications.
The presence of a co-occurring substance use disorder was associated with a greater likelihood of initiation. This particular variable may serve as a marker for generally higher levels of severity, and those with higher severity may have greater incentive to engage in treatment. However, this is somewhat counterintuitive given the finding that those prescribed extended-release buprenorphine in response to an unstable course of treatment — indicative of greater severity – were less likely to initiate the treatment. Since severe opioid use was essentially a constant in this study – where 89% had heroin/fentanyl as their primary substance and injection was the primary route of administration for 69% – unstable course of remission may be a marker of other risk factors, such as lower motivation for treatment. Unstable remission may also be indicative of socioeconomic characteristics that interfere with treatment engagement, such as transportation difficulties or work requirements. Importantly, another study showed that patient interest in extended-release buprenorphine is associated with an abstinence (vs. reduction) goal, though this study did not measure treatment goal. Thus, the treatment group who received extended-release buprenorphine may have had a greater proportion of individuals with abstinence goals which would indicate greater motivation and likelihood of remaining in care. Given that the very factors that would make someone less likely to initiate extended-release buprenorphine like housing instability are the same factors that make someone a good candidate for this monthly injection, more research is needed to understand whether there may be additional factors beyond substance use severity driving initiation to inform future medication linkage and adherence strategies.
Those prescribed with extended-release buprenorphine prior to the 7-day stabilization period recommended by the FDA were less likely to receive more than a single dose compared to those prescribed extended-release buprenorphine after this initial period. These findings support the FDA guidance and suggest that initial stabilization may reduce dropout. While it is possible that higher levels of functioning and/or motivation may explain both completing the 7-day stabilization and treatment engagement, notably analyses accounted for unstable remission and co-occurring disorders. Thus, benefits from the 7-day stabilization itself may indeed explain this greater treatment engagement. It could be that daily dosing reduces cravings and thereby increases motivation for extended-release buprenorphine or the patient’s functioning making them more likely to attend the initial injection appointment. Importantly, those who followed through on the prescription were also more likely to have had a stable course of remission before receiving their first dose. It is possible this greater motivation and stability explained the positive effect rather than the medication itself (i.e., known as a “selection bias”). That said, prior randomized controlled trials where all participants received empirically-supported behavioral treatment show extended-release buprenorphine injections outperform placebo injections and did as well as daily sublingual buprenorphine. It seems probable, therefore, that the buprenorphine injection itself helped explain greater odds of continued participation in the addiction medicine clinic.
The study did not account for services received outside the addiction medicine clinic where the study took place including other behavioral treatment or medication nor did the study account for community-based recovery support services.
Diagnostic profiles were determined by research staff review of patient charts. Given the central role of co-occurring substance use and psychiatric disorders to the study findings, structured clinical interviews may have led to greater diagnostic precision and different outcomes – though with unclear direction of such an impact.
BOTTOM LINE
In this naturalistic study of people receiving a prescription for extended-release buprenorphine in an outpatient specialty addiction clinic, only half actually had at least one dose and only one third of these actually stayed on it for at least 6 months, where most benefits are observed. Also, those with an unstable course of opioid use disorder remission were less likely to follow through on the prescription. While agreeing to be administered at least one dose was associated with greater treatment retention and less opioid use at follow up, more work is needed to understand the exact reasons for the generally low rates of extended-release buprenorphine treatment engagement and even lower retention under perhaps the most ideal clinical conditions (i.e., at a specialty addiction clinic at an academic medical center).
For individuals and families seeking recovery: Extended-release buprenorphine may be a good option to help improve your chances of initiating and sustaining recovery if you are experiencing opioid use disorder. However, it may be important to receive continuous doses for 6 months or more to be most effective. Discuss with your providers any obstacles to receiving treatment in case they can help you problem solve strategies to overcoming them.
For treatment professionals and treatment systems: Studies suggest that extended-release buprenorphine is a useful treatment approach for your patients with opioid use disorder. However, several barriers clearly interfere with initiation and treatment retention. Indeed, even when a once per month “gold standard” injectable formulation is made available that can dramatically decrease the medication compliance concerns seen in daily oral dosing, and is administered under perhaps the most ideal clinical treatment conditions (within a specialty addiction medicine clinical within an academic medical center) only about half actually took a single dose and only one third of those actually remained on it for 6 months. Also, those prescribed extended-release buprenorphine due to unstable course of remission from opioid use disorder in particular may be unlikely to initiate treatment and more likely to drop out. Further, the FDA guidance on delaying prescribing extended-release buprenorphine until after a 7-day oral daily dose stabilization period is associated with better outcomes. Ongoing open communication with patients may help identify individualized factors associated with initiation of extended-release buprenorphine. Program evaluation of systems level initiatives to increase availability of extended-release buprenorphine may uncover additional factors that are relevant.
For scientists: Extended-release buprenorphine can benefit people attempting recovery from opioid use disorder. However, barriers to implementation remain. This study provides some additional real-world data about factors that may be associated with initiation and treatment engagement; additional mixed methods research are needed, however, to help identify relevant factors that have not been previously studied but that may inform interventions or solutions that increase initiation among people prescribed by extended-release buprenorphine.
For policy makers: The current study provides additional information partially explaining high dropout rates among people prescribed extended-release buprenorphine in the real world and in perhaps the most ideal clinical setting. Studies such as this one highlight the many challenges associated with implementing empirically-supported treatments. High drop-out rates do not indicate that extended-release buprenorphine is ineffective; rather, it suggests that there are obstacles to overcome to help maximize initiation among those who receive prescriptions or to the extent that at least some patients do not wish to take such medications, the identification of non-pharmacological alternatives. More research and policy development is needed to address this critical gap in care beyond availability of extended release buprenorphine.
Approximately 6 million people in the United States met criteria for an opioid use disorder in 2022, and there have been persistent year over year increases in opioid-related mortality. Compared to other primary substances, having a primary opioid problem is associated with a similar number of attempts needed to initiate recovery compared to other primary substances but more psychosocial challenges after initiating recovery. Currently, medications for opioid use disorder are first-line, empirically-supported approaches for reducing opioid mortality and increasing likelihood of remission from opioid use disorder. Medications such as buprenorphine are agonists that bind to opioid receptor sites in the brain but act more slowly and with less potency than other opioids. As a result, they reduce cravings and symptoms of withdrawal while blocking other opioids (e.g., heroin), yet without producing opioid-related euphoric effects when used as prescribed. Despite the fact that these medications are helpful, in 2022 only an estimated 18% of people diagnosed with opioid use disorder have used a medication for opioid use disorder that they were prescribed. Even among those who receive an opioid use disorder medication, the challenges accompanying opioid use disorder recovery (e.g., housing instability, mental health difficulties, environmental cues/triggers, etc.) make daily medication regiments difficult for some. In 2017, the U.S. Food and Drug Administration approved a once monthly injectable dose of buprenorphine to help address these potential issues. Data shows this extended-release buprenorphine formulation outperforms placebo injections and does as well as daily sublingual buprenorphine. Yet approximately half of individuals prescribed extended-release buprenorphine discontinue within 1 year. There is a critical need for naturalistic research to understand factors associated with initiation of extended-release buprenorphine and factors that predict ongoing engagement with this injectable medication.
This study examined patient characteristics associated with taking at least one dose of extended-release buprenorphine among those who were prescribed this medication in a low-barrier addiction medicine specialty clinic. The study also examined predictors of the number of doses taken, and treatment retention after 6 months.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of cross-sectional data extracted from the electronic health record (EHR) of an outpatient addiction medicine clinic at an academic medical center examining factors associated with initiating buprenorphine (baseline) and retention (6-month follow-up). The researchers identified all participants who were prescribed extended-release buprenorphine in this addiction medicine clinic between December 2018 and December 2020. Data was extracted via manual free text chart review. Variables extracted from patient charts included gender, race, primary opioid type and route of administration prior to remission, housing status, presence of a co-occurring mental health diagnosis, presence of co-occurring substance use disorder apart from opioid (e.g., stimulant use disorder), reason for prescribing extended-release buprenorphine (“unstable” remission, patient preference, or other), insurance type (public or private), and whether patients were prescribed a supplemental daily dose of buprenorphine at any point during the data extraction period. Notably, the study could not account for services received outside the addiction medicine clinic where the study took place or community-based recovery support services. Whether patients were prescribed extended-release buprenorphine prior to the FDA’s recommended 7-day stabilization period on daily buprenorphine, number of doses received over 6 months, and treatment retention at 6 months (any addiction medicine visit within 6 months of the index buprenorphine injection) were each obtained from patient charts.
Researchers first examined the likelihood of initiating extended-release buprenorphine among those receiving a prescription and factors associated with initiation. Next, they examined factors associated with treatment retention and urine drug test results 6 months after receiving the prescription. All models controlled statistically for the documented demographic and clinical characteristics noted above.
The sample of 233 adults were 39 years old on average, more likely to be male (62.2%), non-Hispanic White (63.8%), use public insurance (93.6%), have stable housing (79%). Almost two-thirds (62.2%) had co-occurring opioid and another substance use disorder, 58.4% had a current co-occurring mental health condition, and 65.2% were prescribed extended-release buprenorphine due to unstable remission for opioid use disorder.
WHAT DID THIS STUDY FIND?
Clinical stability associated with receiving a buprenorphine injection.
Among the full sample, 56% initiated extended-release buprenorphine after receiving a prescription. Initiation took a median time of 28 days to first dose. On average, patients received 3.7 extended-release buprenorphine injections during the 6-month period. Approximately one-third received all 6 doses.
Having a co-occurring substance use disorder (e.g., stimulant) and being prescribed extended-release buprenorphine for a reason other than unstable course of remission for opioid use disorder (e.g., patient preference) was associated with a much greater likelihood of initiating extended-release buprenorphine.
Among those receiving at least one dose of extended-release buprenorphine, those initiating extended-release buprenorphine prior to the recommended 7-day daily dose stabilization phase were less likely to receive all 6 maintenance doses (0 %) compared to 2–5 doses (13.2 %) or 1 dose (4.2 %). Those prescribed a supplemental daily dose of buprenorphine were more likely to receive more than one injection compared to receiving a single dose.
More clinical and psychosocial challenges associated with lower treatment retention.
Those with private insurance, relative to public, were more likely to remain in treatment at 6-month follow-up. Further, those with a mental health diagnosis were more likely to remain in treatment at 6-month follow-up relative to those without co-occurring mental health conditions. Those prescribed extended-release buprenorphine due to having an unstable course of remission were less likely to be retained in treatment. Independent of these and other demographic and clinical factors, those initiating extended-release buprenorphine were 4.8 times more likely to be retained in treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The current study replicated previous studies by demonstrating that half of those prescribed extended-release buprenorphine actually took at least one dose, with only 1/3 of those who received a single dose completing all 6 doses during the study period. These findings highlight the importance of understanding full cascades of care and may demonstrate that enhanced access and availability are “necessary, but not sufficient” to receiving extended-release opioid use disorder medications. Though increasing availability of such a treatment may be effective in reducing overdose and increasing rates of opioid use disorder remission, other important factors may also need to be addressed in order to maximize real world impact of these FDA-approved medications.
The presence of a co-occurring substance use disorder was associated with a greater likelihood of initiation. This particular variable may serve as a marker for generally higher levels of severity, and those with higher severity may have greater incentive to engage in treatment. However, this is somewhat counterintuitive given the finding that those prescribed extended-release buprenorphine in response to an unstable course of treatment — indicative of greater severity – were less likely to initiate the treatment. Since severe opioid use was essentially a constant in this study – where 89% had heroin/fentanyl as their primary substance and injection was the primary route of administration for 69% – unstable course of remission may be a marker of other risk factors, such as lower motivation for treatment. Unstable remission may also be indicative of socioeconomic characteristics that interfere with treatment engagement, such as transportation difficulties or work requirements. Importantly, another study showed that patient interest in extended-release buprenorphine is associated with an abstinence (vs. reduction) goal, though this study did not measure treatment goal. Thus, the treatment group who received extended-release buprenorphine may have had a greater proportion of individuals with abstinence goals which would indicate greater motivation and likelihood of remaining in care. Given that the very factors that would make someone less likely to initiate extended-release buprenorphine like housing instability are the same factors that make someone a good candidate for this monthly injection, more research is needed to understand whether there may be additional factors beyond substance use severity driving initiation to inform future medication linkage and adherence strategies.
Those prescribed with extended-release buprenorphine prior to the 7-day stabilization period recommended by the FDA were less likely to receive more than a single dose compared to those prescribed extended-release buprenorphine after this initial period. These findings support the FDA guidance and suggest that initial stabilization may reduce dropout. While it is possible that higher levels of functioning and/or motivation may explain both completing the 7-day stabilization and treatment engagement, notably analyses accounted for unstable remission and co-occurring disorders. Thus, benefits from the 7-day stabilization itself may indeed explain this greater treatment engagement. It could be that daily dosing reduces cravings and thereby increases motivation for extended-release buprenorphine or the patient’s functioning making them more likely to attend the initial injection appointment. Importantly, those who followed through on the prescription were also more likely to have had a stable course of remission before receiving their first dose. It is possible this greater motivation and stability explained the positive effect rather than the medication itself (i.e., known as a “selection bias”). That said, prior randomized controlled trials where all participants received empirically-supported behavioral treatment show extended-release buprenorphine injections outperform placebo injections and did as well as daily sublingual buprenorphine. It seems probable, therefore, that the buprenorphine injection itself helped explain greater odds of continued participation in the addiction medicine clinic.
The study did not account for services received outside the addiction medicine clinic where the study took place including other behavioral treatment or medication nor did the study account for community-based recovery support services.
Diagnostic profiles were determined by research staff review of patient charts. Given the central role of co-occurring substance use and psychiatric disorders to the study findings, structured clinical interviews may have led to greater diagnostic precision and different outcomes – though with unclear direction of such an impact.
BOTTOM LINE
In this naturalistic study of people receiving a prescription for extended-release buprenorphine in an outpatient specialty addiction clinic, only half actually had at least one dose and only one third of these actually stayed on it for at least 6 months, where most benefits are observed. Also, those with an unstable course of opioid use disorder remission were less likely to follow through on the prescription. While agreeing to be administered at least one dose was associated with greater treatment retention and less opioid use at follow up, more work is needed to understand the exact reasons for the generally low rates of extended-release buprenorphine treatment engagement and even lower retention under perhaps the most ideal clinical conditions (i.e., at a specialty addiction clinic at an academic medical center).
For individuals and families seeking recovery: Extended-release buprenorphine may be a good option to help improve your chances of initiating and sustaining recovery if you are experiencing opioid use disorder. However, it may be important to receive continuous doses for 6 months or more to be most effective. Discuss with your providers any obstacles to receiving treatment in case they can help you problem solve strategies to overcoming them.
For treatment professionals and treatment systems: Studies suggest that extended-release buprenorphine is a useful treatment approach for your patients with opioid use disorder. However, several barriers clearly interfere with initiation and treatment retention. Indeed, even when a once per month “gold standard” injectable formulation is made available that can dramatically decrease the medication compliance concerns seen in daily oral dosing, and is administered under perhaps the most ideal clinical treatment conditions (within a specialty addiction medicine clinical within an academic medical center) only about half actually took a single dose and only one third of those actually remained on it for 6 months. Also, those prescribed extended-release buprenorphine due to unstable course of remission from opioid use disorder in particular may be unlikely to initiate treatment and more likely to drop out. Further, the FDA guidance on delaying prescribing extended-release buprenorphine until after a 7-day oral daily dose stabilization period is associated with better outcomes. Ongoing open communication with patients may help identify individualized factors associated with initiation of extended-release buprenorphine. Program evaluation of systems level initiatives to increase availability of extended-release buprenorphine may uncover additional factors that are relevant.
For scientists: Extended-release buprenorphine can benefit people attempting recovery from opioid use disorder. However, barriers to implementation remain. This study provides some additional real-world data about factors that may be associated with initiation and treatment engagement; additional mixed methods research are needed, however, to help identify relevant factors that have not been previously studied but that may inform interventions or solutions that increase initiation among people prescribed by extended-release buprenorphine.
For policy makers: The current study provides additional information partially explaining high dropout rates among people prescribed extended-release buprenorphine in the real world and in perhaps the most ideal clinical setting. Studies such as this one highlight the many challenges associated with implementing empirically-supported treatments. High drop-out rates do not indicate that extended-release buprenorphine is ineffective; rather, it suggests that there are obstacles to overcome to help maximize initiation among those who receive prescriptions or to the extent that at least some patients do not wish to take such medications, the identification of non-pharmacological alternatives. More research and policy development is needed to address this critical gap in care beyond availability of extended release buprenorphine.
Approximately 6 million people in the United States met criteria for an opioid use disorder in 2022, and there have been persistent year over year increases in opioid-related mortality. Compared to other primary substances, having a primary opioid problem is associated with a similar number of attempts needed to initiate recovery compared to other primary substances but more psychosocial challenges after initiating recovery. Currently, medications for opioid use disorder are first-line, empirically-supported approaches for reducing opioid mortality and increasing likelihood of remission from opioid use disorder. Medications such as buprenorphine are agonists that bind to opioid receptor sites in the brain but act more slowly and with less potency than other opioids. As a result, they reduce cravings and symptoms of withdrawal while blocking other opioids (e.g., heroin), yet without producing opioid-related euphoric effects when used as prescribed. Despite the fact that these medications are helpful, in 2022 only an estimated 18% of people diagnosed with opioid use disorder have used a medication for opioid use disorder that they were prescribed. Even among those who receive an opioid use disorder medication, the challenges accompanying opioid use disorder recovery (e.g., housing instability, mental health difficulties, environmental cues/triggers, etc.) make daily medication regiments difficult for some. In 2017, the U.S. Food and Drug Administration approved a once monthly injectable dose of buprenorphine to help address these potential issues. Data shows this extended-release buprenorphine formulation outperforms placebo injections and does as well as daily sublingual buprenorphine. Yet approximately half of individuals prescribed extended-release buprenorphine discontinue within 1 year. There is a critical need for naturalistic research to understand factors associated with initiation of extended-release buprenorphine and factors that predict ongoing engagement with this injectable medication.
This study examined patient characteristics associated with taking at least one dose of extended-release buprenorphine among those who were prescribed this medication in a low-barrier addiction medicine specialty clinic. The study also examined predictors of the number of doses taken, and treatment retention after 6 months.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of cross-sectional data extracted from the electronic health record (EHR) of an outpatient addiction medicine clinic at an academic medical center examining factors associated with initiating buprenorphine (baseline) and retention (6-month follow-up). The researchers identified all participants who were prescribed extended-release buprenorphine in this addiction medicine clinic between December 2018 and December 2020. Data was extracted via manual free text chart review. Variables extracted from patient charts included gender, race, primary opioid type and route of administration prior to remission, housing status, presence of a co-occurring mental health diagnosis, presence of co-occurring substance use disorder apart from opioid (e.g., stimulant use disorder), reason for prescribing extended-release buprenorphine (“unstable” remission, patient preference, or other), insurance type (public or private), and whether patients were prescribed a supplemental daily dose of buprenorphine at any point during the data extraction period. Notably, the study could not account for services received outside the addiction medicine clinic where the study took place or community-based recovery support services. Whether patients were prescribed extended-release buprenorphine prior to the FDA’s recommended 7-day stabilization period on daily buprenorphine, number of doses received over 6 months, and treatment retention at 6 months (any addiction medicine visit within 6 months of the index buprenorphine injection) were each obtained from patient charts.
Researchers first examined the likelihood of initiating extended-release buprenorphine among those receiving a prescription and factors associated with initiation. Next, they examined factors associated with treatment retention and urine drug test results 6 months after receiving the prescription. All models controlled statistically for the documented demographic and clinical characteristics noted above.
The sample of 233 adults were 39 years old on average, more likely to be male (62.2%), non-Hispanic White (63.8%), use public insurance (93.6%), have stable housing (79%). Almost two-thirds (62.2%) had co-occurring opioid and another substance use disorder, 58.4% had a current co-occurring mental health condition, and 65.2% were prescribed extended-release buprenorphine due to unstable remission for opioid use disorder.
WHAT DID THIS STUDY FIND?
Clinical stability associated with receiving a buprenorphine injection.
Among the full sample, 56% initiated extended-release buprenorphine after receiving a prescription. Initiation took a median time of 28 days to first dose. On average, patients received 3.7 extended-release buprenorphine injections during the 6-month period. Approximately one-third received all 6 doses.
Having a co-occurring substance use disorder (e.g., stimulant) and being prescribed extended-release buprenorphine for a reason other than unstable course of remission for opioid use disorder (e.g., patient preference) was associated with a much greater likelihood of initiating extended-release buprenorphine.
Among those receiving at least one dose of extended-release buprenorphine, those initiating extended-release buprenorphine prior to the recommended 7-day daily dose stabilization phase were less likely to receive all 6 maintenance doses (0 %) compared to 2–5 doses (13.2 %) or 1 dose (4.2 %). Those prescribed a supplemental daily dose of buprenorphine were more likely to receive more than one injection compared to receiving a single dose.
More clinical and psychosocial challenges associated with lower treatment retention.
Those with private insurance, relative to public, were more likely to remain in treatment at 6-month follow-up. Further, those with a mental health diagnosis were more likely to remain in treatment at 6-month follow-up relative to those without co-occurring mental health conditions. Those prescribed extended-release buprenorphine due to having an unstable course of remission were less likely to be retained in treatment. Independent of these and other demographic and clinical factors, those initiating extended-release buprenorphine were 4.8 times more likely to be retained in treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The current study replicated previous studies by demonstrating that half of those prescribed extended-release buprenorphine actually took at least one dose, with only 1/3 of those who received a single dose completing all 6 doses during the study period. These findings highlight the importance of understanding full cascades of care and may demonstrate that enhanced access and availability are “necessary, but not sufficient” to receiving extended-release opioid use disorder medications. Though increasing availability of such a treatment may be effective in reducing overdose and increasing rates of opioid use disorder remission, other important factors may also need to be addressed in order to maximize real world impact of these FDA-approved medications.
The presence of a co-occurring substance use disorder was associated with a greater likelihood of initiation. This particular variable may serve as a marker for generally higher levels of severity, and those with higher severity may have greater incentive to engage in treatment. However, this is somewhat counterintuitive given the finding that those prescribed extended-release buprenorphine in response to an unstable course of treatment — indicative of greater severity – were less likely to initiate the treatment. Since severe opioid use was essentially a constant in this study – where 89% had heroin/fentanyl as their primary substance and injection was the primary route of administration for 69% – unstable course of remission may be a marker of other risk factors, such as lower motivation for treatment. Unstable remission may also be indicative of socioeconomic characteristics that interfere with treatment engagement, such as transportation difficulties or work requirements. Importantly, another study showed that patient interest in extended-release buprenorphine is associated with an abstinence (vs. reduction) goal, though this study did not measure treatment goal. Thus, the treatment group who received extended-release buprenorphine may have had a greater proportion of individuals with abstinence goals which would indicate greater motivation and likelihood of remaining in care. Given that the very factors that would make someone less likely to initiate extended-release buprenorphine like housing instability are the same factors that make someone a good candidate for this monthly injection, more research is needed to understand whether there may be additional factors beyond substance use severity driving initiation to inform future medication linkage and adherence strategies.
Those prescribed with extended-release buprenorphine prior to the 7-day stabilization period recommended by the FDA were less likely to receive more than a single dose compared to those prescribed extended-release buprenorphine after this initial period. These findings support the FDA guidance and suggest that initial stabilization may reduce dropout. While it is possible that higher levels of functioning and/or motivation may explain both completing the 7-day stabilization and treatment engagement, notably analyses accounted for unstable remission and co-occurring disorders. Thus, benefits from the 7-day stabilization itself may indeed explain this greater treatment engagement. It could be that daily dosing reduces cravings and thereby increases motivation for extended-release buprenorphine or the patient’s functioning making them more likely to attend the initial injection appointment. Importantly, those who followed through on the prescription were also more likely to have had a stable course of remission before receiving their first dose. It is possible this greater motivation and stability explained the positive effect rather than the medication itself (i.e., known as a “selection bias”). That said, prior randomized controlled trials where all participants received empirically-supported behavioral treatment show extended-release buprenorphine injections outperform placebo injections and did as well as daily sublingual buprenorphine. It seems probable, therefore, that the buprenorphine injection itself helped explain greater odds of continued participation in the addiction medicine clinic.
The study did not account for services received outside the addiction medicine clinic where the study took place including other behavioral treatment or medication nor did the study account for community-based recovery support services.
Diagnostic profiles were determined by research staff review of patient charts. Given the central role of co-occurring substance use and psychiatric disorders to the study findings, structured clinical interviews may have led to greater diagnostic precision and different outcomes – though with unclear direction of such an impact.
BOTTOM LINE
In this naturalistic study of people receiving a prescription for extended-release buprenorphine in an outpatient specialty addiction clinic, only half actually had at least one dose and only one third of these actually stayed on it for at least 6 months, where most benefits are observed. Also, those with an unstable course of opioid use disorder remission were less likely to follow through on the prescription. While agreeing to be administered at least one dose was associated with greater treatment retention and less opioid use at follow up, more work is needed to understand the exact reasons for the generally low rates of extended-release buprenorphine treatment engagement and even lower retention under perhaps the most ideal clinical conditions (i.e., at a specialty addiction clinic at an academic medical center).
For individuals and families seeking recovery: Extended-release buprenorphine may be a good option to help improve your chances of initiating and sustaining recovery if you are experiencing opioid use disorder. However, it may be important to receive continuous doses for 6 months or more to be most effective. Discuss with your providers any obstacles to receiving treatment in case they can help you problem solve strategies to overcoming them.
For treatment professionals and treatment systems: Studies suggest that extended-release buprenorphine is a useful treatment approach for your patients with opioid use disorder. However, several barriers clearly interfere with initiation and treatment retention. Indeed, even when a once per month “gold standard” injectable formulation is made available that can dramatically decrease the medication compliance concerns seen in daily oral dosing, and is administered under perhaps the most ideal clinical treatment conditions (within a specialty addiction medicine clinical within an academic medical center) only about half actually took a single dose and only one third of those actually remained on it for 6 months. Also, those prescribed extended-release buprenorphine due to unstable course of remission from opioid use disorder in particular may be unlikely to initiate treatment and more likely to drop out. Further, the FDA guidance on delaying prescribing extended-release buprenorphine until after a 7-day oral daily dose stabilization period is associated with better outcomes. Ongoing open communication with patients may help identify individualized factors associated with initiation of extended-release buprenorphine. Program evaluation of systems level initiatives to increase availability of extended-release buprenorphine may uncover additional factors that are relevant.
For scientists: Extended-release buprenorphine can benefit people attempting recovery from opioid use disorder. However, barriers to implementation remain. This study provides some additional real-world data about factors that may be associated with initiation and treatment engagement; additional mixed methods research are needed, however, to help identify relevant factors that have not been previously studied but that may inform interventions or solutions that increase initiation among people prescribed by extended-release buprenorphine.
For policy makers: The current study provides additional information partially explaining high dropout rates among people prescribed extended-release buprenorphine in the real world and in perhaps the most ideal clinical setting. Studies such as this one highlight the many challenges associated with implementing empirically-supported treatments. High drop-out rates do not indicate that extended-release buprenorphine is ineffective; rather, it suggests that there are obstacles to overcome to help maximize initiation among those who receive prescriptions or to the extent that at least some patients do not wish to take such medications, the identification of non-pharmacological alternatives. More research and policy development is needed to address this critical gap in care beyond availability of extended release buprenorphine.