
How many tries does it take to resolve a substance use problem? Lessons from a national study of recovering adults in the U.S.
Substance use problems are often described as “chronic relapsing” conditions, where those who are affected and trying to stop are going to “fail” several times before they achieve remission or long-term recovery. Despite this depiction, very little is known about the actual number of serious recovery attempts people make before successfully resolving a significant substance problem, nor do we know what factors are associated with needing less or more attempts. To date, almost all of our knowledge about recovery attempt patterns come from follow-up studies of addiction treatment which are usually focused on those with the most severe problems. However, substance use problems are on a spectrum of severity with highly variable causes, characteristics, courses, and approaches to problem resolution. Thus, it is critical to know about problem resolution in a variety of circumstances that better reflects the broad array of substance-related involvement and impairment. In this study of a representative sample of U.S. adults who resolved a drug or alcohol problem, the typical participant surprisingly needed only a small number of serious recovery attempts to resolve their problem. The range, however, was very broad, with many reporting just one or two, and others reporting dozens or more attempts. The upwardly–skewed nature of this distribution of reported recovery attempts – with a much smaller number of individuals requiring many more attempts – has implications for over– or under-treating a large number of individuals suffering from substance-related problems. This highlights the need for a variety of interventions to be available and greater personalization in clinical and public health approaches.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Substance use disorders (SUDs) have long been thought of as chronic diseases that are characterized by multiple serious recovery attempts before a person is able to achieve long-term recovery or remission. This description is supported by accounts from clinicians and those in recovery alike, as well as clinical and epidemiological study data from those seeking treatment for SUDs. However, despite this, we still do not know how many attempts, on average, it takes to resolve a substance problem in a way that accurately reflects the diversity seen across substance-related conditions, and, by extension, we do not know what factors lead to one person needing more or less recovery attempts than another person. This is crucial information for health care providers to aid intervention, policy makers to inform resource allocation, as well as for those interested in resolving a substance problem. To address this, Kelly and colleagues used a national sample of U.S. adults who have successfully resolved a significant substance problem to 1) determine the average number of attempts prior to problem resolution; 2) identify the demographic and clinical factors associated with the number of recovery attempts needed prior to successfully achieving long-term recovery; and 3) characterize the relationship between the number of attempts and indices of quality of life/psychological well-being after substance problem resolution.
HOW WAS THIS STUDY CONDUCTED?
This study used data from the National Recovery Study, a large nationally–representative sample of 2,002 U.S. adults who indicated that they used to have a substance use problem, but no longer do. As part of the survey, participants answered the question, “Approximately how many serious attempts did you make to resolve your alcohol/drug problem before you overcame it?” Participants also self-reported demographic information, as well as primary substance, clinical histories, and measures of psychological distress/well-being.
In this particular study, authors calculated the mean and median of the number of recovery attempts and examined if the number of recovery attempts varied as a function of key demographic (e.g., sex, race, income, and marital status) and clinical factors (e.g., primary substance, psychiatric diagnoses, outpatient treatment history, inpatient treatment history, mutual-help attendance, and utilization of any treatment or recovery support services). Importantly, some of the sample are likely to experience a future recurrence of substance problems, particularly those in the early phases of recovery (e.g., <5 years), which would likely add to their current tally of prior serious recovery attempts. To account for this, the authors conducted a separate analysis that restricted the sample to those who had 5 or more years in recovery in order to see whether the estimate of prior serious recovery attempts differed in this subset of more stable remitters compared to those in the earlier stages of recovery (0-5 years). Additionally, they went on to establish the relationship between the number of recovery attempts and quality of life after a substance problem was resolved.
As detailed in previous publications from this sample, eligible participants (i.e., endorsed having resolved a significant substance problem) were 44 years old on average, 40% female, and 39% identified as a racial/ethnic minority. At the time of the survey, it had been several years since many individuals resolved their substance problem, with roughly 35% resolving their problem 5–15 years ago, and 29% more than 15 years ago.
WHAT DID THIS STUDY FIND?
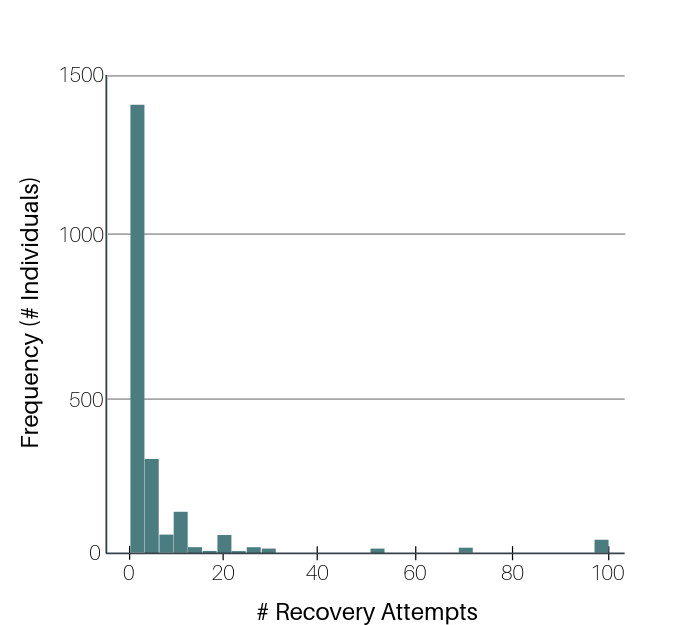
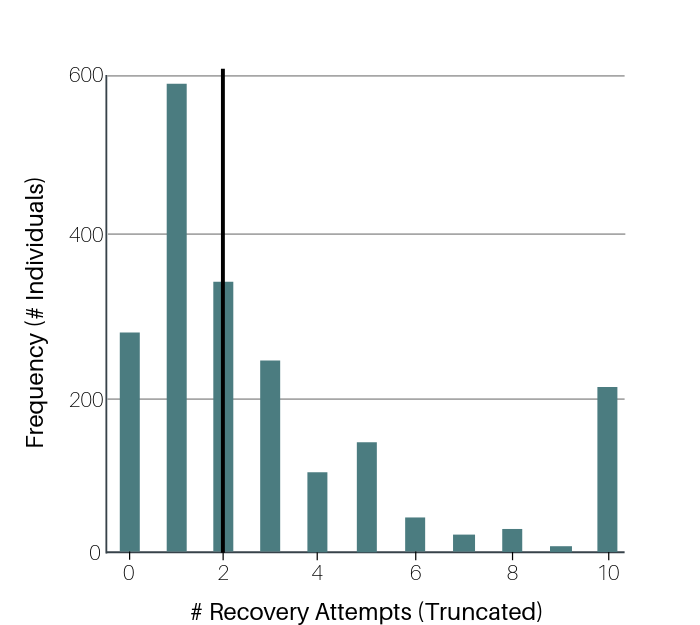
The number of serious recovery attempts ranged from 0-100, with 50% of people (median) needing only 2, and an average of 5.
Approximately 13% of the sample reported not making any “serious” recovery attempts. Importantly, those with 5+ years of recovery reported the same pattern of serious recovery attempts (e.g., average = 5, median = 2) to that of the full sample. Number of recovery attempts did not vary by age, sex, education, or household income. Individuals who were non-Hispanic Black and not married reported a greater number of recovery attempts (Black average = 4.6, median = 3; not married average = 6.1, median = 2). Those with a diagnosis of depression or anxiety or who had received recovery support services (i.e., inpatient, outpatient, mutual–help, or any support service), reported a greater number of recovery attempts (depression disorder average = 5.8, median = 3; anxiety disorder average = 6.1, median = 3; previous recovery support services use average = 6.4, median = 3). Interestingly, age of problem onset and primary substance were not associated with differences in the number of recovery attempts before problem resolution.
Greater number of recovery attempts was related to higher psychological distress.
Greater number of recovery attempts was associated with lower quality of life, happiness, self-esteem, and higher psychological distress after problem resolution. However, when the authors controlled for the number of years since problem resolution, the association between number of recovery attempts and lowered happiness and self-esteem was no longer present. Furthermore, with the addition of key clinical predictors (depression, anxiety, and utilization of any treatment/recovery services), only the relationship between more recovery attempts and higher distress remained. This suggests that a greater number of recovery attempts was still associated with greater current psychological distress regardless of how long one has been in recovery, if they have history of mood and anxiety disorders, and/or if they have utilized treatment services before.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Findings highlight the broad variability in the reported number of recovery attempts prior to resolving a substance problem and perhaps a surprisingly low average number (median = 2), in general, with certain subgroups needing substantially more attempts. This low median held true even when examining the more stably remitted subsample (i.e., those with 5+ years of recovery), who are statistically much less likely to add to their future tally of serious recovery attempts given they are much less likely to relapse. Those with other mental health conditions or a history of using recovery services needed more attempts to resolve their problem. Both can be interpreted as markers of increased severity and/or impairment making recovery more difficult to achieve. Taken together, a few lessons become clear, first that the best estimate for the number of attempts needed for most people to resolve a significant substance problem is two, and that increased severity and/or co-occurring mental health concerns add additional complications that potentially necessitate more attempts. In a practical sense, this means the number of serious recovery attempts an individual needs varies depending on how severe their circumstances are (e.g., depression, lack of social support, addiction severity). Accordingly, some people need many attempts, but most people need 2 or less.
These findings underscore the notion that alcohol and other drug problems are on a continuum characterized by multiple root causes, diverse clinical profiles, highly variable courses, as well as diverse recovery trajectories and styles of problem resolution. Despite this variability, the most severe get most of the attention in the scientific literature, and for these individuals it often takes more attempts. In practice, most people who report having a substance problem do not even meet criteria for SUD, and of those who do, roughly 30% of individuals have mild cases. Thus, for those on the lower end of the spectrum, substance use is a health behavior that responds well to purposeful efforts to change.
- LIMITATIONS
-
- Although the sample was nationally representative, the study design was cross-sectional, and thus any causal inferences should be made cautiously without future longitudinal investigations.
- The survey methodology relied on participants’ retrospective recall, which could be prone to bias, either over or underestimating recovery attempts.
- The stem question used to inquire into the number of serious recovery attempts was left to participants to decide for themselves regarding what a “serious” attempt was. This could have caused some confusion about how to answer the question. This is somewhat supported by the fact that approximately 13% of the sample reported not making any serious recovery attempts, and one-third of those without a serious attempt had attended treatment or mutual help groups such as AA. Consequently, future estimates may vary depending on how such assessments in this area are made.
BOTTOM LINE
- For individuals and families seeking recovery: This study showed that the number of serious recovery attempts ranged from 0-100, with the average (median) person in the U.S. who once had a problem with alcohol/drugs but no longer does needing only two serious attempts to achieve problem resolution. The median number of recovery attempts prior to successful substance problem resolution may be substantially lower than most people might have guessed. This may come as a surprise to many because, arguably, the cultural portrayal of how substance problems are resolved is infused with the stereotyped notion that such problems constitute “chronically relapsing brain diseases” and thus success in changing substance use is perceived to involve seemingly endless tries. Relatedly, many may believe – again based on cultural stereotype – that changing substance use is so difficult that it inevitably involves going to “rehab” and/or “AA.” Although it is certainly true that some do need that level of care and ongoing recovery support to achieve long-term remission, this stereotype may have the unintended consequence of reducing hope and recovery self-efficacy for many individuals with less severe problems, thus preventing help-seeking because the needed effort for successful change is perceived to be too high. Instead, for most people, the number of serious recovery attempts needed is actually quite low. That said, certain subgroups (i.e., likely those with higher severity/chronicity/other mental health conditions) may require more attempts to achieve success. Yet, it is these more severe subgroups that are perceived as the norm, when in fact the opposite is true.
- For treatment professionals and treatment systems: This study showed that the number of serious recovery attempts ranged from 0-100, with the average (median) person in the U.S. who once had a problem with alcohol/drugs but no longer does needing only two serious attempts to achieve problem resolution. There are important treatment implications from this study. First, the wide range of recovery attempts (0-100) suggests that substance problems are not easily lumped together in a single category. Instead, they appear to reflect a continuum characterized by multiple root causes, diverse clinical profiles, highly variable courses, as well as diverse recovery trajectories and styles of problem resolution. Such diversity requires highly individualized approaches to addressing substance problems. As a result, more time needs to be invested in more accurate assessment of the full nature and impact of substance problems, as well as available supports that can enhance recovery in order to increase the efficiency and effectiveness of treatment efforts.
- For scientists: This study showed that the number of serious recovery attempts ranged from 0-100, with the average (median) person in the U.S. who once had a problem with alcohol/drugs but no longer does needing only two serious attempts to achieve problem resolution. Despite this low number, those who identified as Black, single, and/or reported previous use of recovery support services were more likely to need more serious attempts before resolving their problem. Given the cross-sectional nature of the data, it is currently unclear whether relationship status (e.g., married, living with partner, etc.) at the time of those serious recovery attempts had any bearing on them, as this variable reflected current status rather than historical status. It is unclear also why Black individuals compared to White individuals may have required significantly more recovery attempts. Future research is needed to understand more about such racial/ethnic and relationship differences.
- For policy makers: This study showed that the number of serious recovery attempts ranged from 0-100, with the average (median) person in the U.S. who once had a problem with alcohol/drugs but no longer does needing only two serious attempts to achieve problem resolution. This wide variability was associated with different subgroups that may benefit from unique clinical care that is beyond what a typical person needs, and most likely requires a highly individualized approach to addressing their substance problems. As a result, increased funding for the development of more accurate assessment of substance use and related problems, as well as research on the potential benefits of individualized treatment may improve addiction recovery rates and decrease the public health burden related to hazardous substance use.
CITATIONS
Kelly, J. F., Greene, M. C., Bergman, B. G., White, W. L., & Hoeppner, B. B. (2019). How many recovery attempts does it take to successfully resolve an alcohol or drug problem? Estimates and correlates from a national study of recovering U.S. adults. Alcoholism: Clinical and Experimental Research, 43(7), 1533-1544. doi: 10.1111/acer.14067
