
Detox & Medication: Do the Odds of Completing & Staying in Treatment Get Better or Worse With Repeated Attempts?
Due to the chronic course of opioid use disorders, it is not uncommon for people to require repeated attempts at detoxification and medication treatments before consistent, sustained remission is attained.
How do these repeated attempts change someone’s odds of completing detoxification treatment and the duration of medication assisted treatment retention?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
California treats the largest population of individuals with opioid use disorder in the entire USA which makes it an ideal location to understand better what is associated with successful completion of detoxification and agonist medication treatment (i.e., methadone or buprenorphine) for opioid use disorder with longitudinal population level data. Prolonged retention in methadone treatment has resulted in decreased illicit drug use, HIV risk behaviors, and crime.
When out of treatment, individuals with opioid use disorder are at elevated risk for mortality that is 24 times greater than when in treatment. Elevated risk for mortality can be due to a lowered tolerance following detoxification which leaves the body vulnerable to overdose if a relapse occurs. Given the well-documented chronic course of substance use disorders, this study by Nosyk and colleagues sought to identify determinants of successful completion of detoxification and medication treatment retention in repeated attempts.
HOW WAS THIS STUDY CONDUCTED?
This study performed secondary data analysis on state-wide administrative data (i.e., California Outcome Measurement System) collected from publically funded drug treatment centers during the years 1991-2012. The sample consisted of all patients presenting for detoxification treatment and medication treatment (mostly methadone) which resulted in 237,709 unique individuals accounting for 885,971 treatment episodes (30.2% or 192,252 individuals were detoxification only).
Three primary outcomes were examined:
- probability of successful detoxification (i.e., defined by the staff as completion or left treatment early with satisfactory progress)
- duration of medication assisted treatment
- estimated time-to-treatment following successful and unsuccessful detoxification
Many variables were controlled for in the analysis including age, gender, ethnicity, primary drug disorder (heroin versus prescribed opioids), primary drug use frequency, presence of secondary drug use disorder (i.e., none; other opioid; stimulant; alcohol or marijuana), education, labor force status, referral source (individual choice or otherwise), volume of treatment episodes per facility, and county level unemployment rate.
WHAT DID THIS STUDY FIND?
Notably, in 1994, 83.7% of the treatment episodes were detoxification compared to only 40.5% in 2010. Among individuals who never accessed medication assisted treatment, the probability of successful detoxification decreased with each successive attempt.
The odds of success were lowest among younger (under 30) and Hispanic individuals. Primary users of prescription opioids were nearly 85% more likely to have a successful detoxification than heroin users.
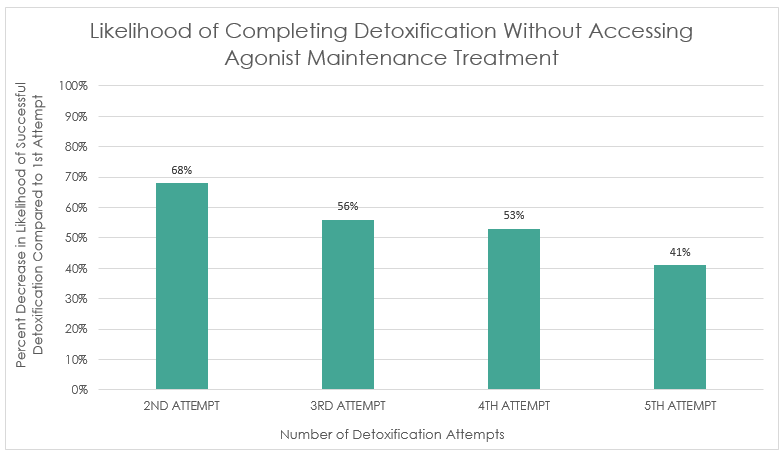
From the graph below: Individuals’ second detoxification attempt was 32% less likely to be successful than the first, the third was 44% less likely to be successful than the first, the fourth was 47% less likely to be successful than the first, and the fifth was 59% less likely to be successful than the first.
The duration of medication assisted treatment retention increased with each attempt.
Longer durations of medication assisted treatment were associated with:
- prior successful detoxification
- two or more immediate prior attempts at detoxification
- older age
- female gender
- full-time employment
- no criminal justice system involvement
- primary prescription opioid use disorder
- poly-opioid use (prescription opioids and heroin) use disorder
Shorter durations of medication assisted treatment were associated with:
- concurrent stimulant use disorder
- primary heroin use disorder
- high daily use
- receiving treatment at higher-volume treatment centers
- receiving treatment in counties with the highest unemployment rates
Time to medication initiation was not connected to detox completion.
However, the proportion of those accessing medication treatment within 14 days of detoxification was lower among successfully detoxified individuals (51.3%) versus unsuccessfully detoxified individuals (55.3%). Furthermore, only 20.2% of the 627,687 detoxification treatment episodes were followed by admission into medication assisted treatment, and only 10.9% were admitted into medication treatment within 14 days.
WHY IS THIS STUDY IMPORTANT
This study found that 237,709 unique individuals accounted for 885,971 treatment episodes in the state of California. This highlights the recurrent course of opioid use disorder and the need to identify determinants of successful detoxification and medication assisted treatment in repeated attempts.
Repeated attempts at detoxification, without subsequent linkage to medication, was associated with continuously decreasing odds of successful completion of detoxification.
Thus, this treatment modality may not contribute as much to the recovery process when used in isolation from medication assisted treatment. Regarding the duration of medication treatment, each subsequent attempt increased in length. Successful detoxification had a positive effect on subsequent duration of medication treatment. Thus, detoxification may support future endeavors at medication treatment by its association with increased medication assisted treatment duration. Opioid treatment guidelines have suggested that success in opioid detoxification should be defined by subsequent linkage to medication, which is supported by this study.
- LIMITATIONS
-
- Clinically important variables that can impact treatment outcomes were not captured in this administrative level database. Medication dosage, adherence to treatment, psychosocial counselling, recovery motivation, and ongoing drug use were not observed and thus the association with treatment outcomes are unknown.
NEXT STEPS
The authors have suggested that future research should seek to quantify the cumulative effects of repeated detoxification, compared to methadone treatment (the standard of care) in terms of morbidity, mortality, and costs to society.
BOTTOM LINE
- For individuals & families seeking recovery: If you or a family member are in need of treatment for alcohol or other drug problems know that detoxification alone is not considered treatment for opioid use disorder but rather a medical intervention. Detoxification should be followed up with long-term medication treatment. This study found that with each successive attempt at medication assisted treatment, the duration increased compared to the first attempt. Finding ways to help you or your family member start and stay on opioid against treatment is important because longer medication treatment durations are related to more positive outcomes.
- For scientists: This study found that only 20.2% of the 627,687 detoxification treatment episodes were followed by admission into medication assisted treatment, and only 10.9% were admitted into medication assisted treatment within 14 days. Unaccounted for in this study is the extent to which individuals transitioned to office-based buprenorphine treatment. Thus, the proportion of individuals who successfully transitioned to agonist treatment may be underestimated, but could still be low overall.
- For policy makers: Detoxification had a positive effect on subsequent medication treatment retention. However, only 20.2% of the 627,687 detoxification treatment episodes were followed by admission into medication assisted treatment, and only 10.9% were admitted into medication assisted treatment within 14 days. Consider adopting policies that encourage, rather than prohibit (e.g., two failed attempts at detox is required to qualify for medication in California) successful and rapid linkage to medications.
- For treatment professionals and treatment systems: People remain on agonist treatment longer and longer with each additional detox episode, suggesting the need for a long-term approach to opioid use disorder recovery and remission. However, shorter durations of medication assisted treatment are associated with concurrent stimulant use disorder and primary heroin use disorder (compared to prescription opioids or both prescription opioids and heroin). This suggest concurrent use of stimulants like cocaine or methamphetamine and those with heroin use disorder are at greater risk for dropout from agonist treatment. Individuals with these clinical characteristics may need greater focus and help to increase the likelihood of treatment retention and more successful outcomes.
CITATIONS
Nosyk, B., Li, L., Evans, E., Urada, D., Huang, D. (2014). Utilization and outcomes of detoxification and maintenance treatment for opioid dependence in publically-funded facilities in California, USA: 1991-2012. Drug and Alcohol Dependence, 143, 149-157.
