
Can specially trained community and recovery support specialists improve linkage to post-detoxification care?
Inpatient detoxification (“detox”) provides medical stabilization but is not considered treatment for substance use disorder. Initiating recovery often requires follow up treatment after a detoxification episode; however, the majority of patients leaving detox do not pursue recommended care, thus increasing risk for future detox readmissions, poorer recovery outcomes, and death. To help overcome this, researchers developed, implemented, and evaluated a recovery support navigation intervention designed to link individuals to care following discharge from inpatient detox.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Inpatient detox provides medical stabilization and withdrawal management to help initiate recovery among patients with substance use disorder and may be an important access point for linkage to ongoing treatment. Treatment after detox is recommended and has been shown to improve long term recovery outcomes, particularly among patients who engage in treatment within two weeks of discharge. Unfortunately, the majority of patients who receive detox services do not attend follow up treatment, which increases rates of costly and ineffective detox readmissions. To address this “revolving door” issue, the authors of this study used “recovery support navigators”, who were individuals trained and tasked with facilitating follow up care for patients following discharge from inpatient detox.
Figure 1.
HOW WAS THIS STUDY CONDUCTED?
This quasi-experimental study used Massachusetts Behavioral Health Partnership and MassHealth general medical care administrative data to examine whether individuals receiving a novel, recovery support navigation intervention were more likely to receive treatment within 14 days of detox charge relative to those who receives detox services as usual.
For this study, recovery support navigators at select sites were used and outcomes of patients at these sites were compared to outcomes of patients at other sites that offered services as usual. Recovery support navigators included a collection of new staff or existing staff from the Community Support Program (CSP). Recovery support navigators, some of which were identified as “peers” but not all, received training in Motivational Interviewing, received monthly coaching and quarterly education regarding substance use disorder, and received training in Brief Negotiated Interview and Active Referral to Treatment. Some, but not all, of the Recovery Support Navigators had lived addiction experience, were in recovery, but this was not required.
Patients in the dataset who received detox services between March 29, 2013 and March 31, 2015, were between 18 and 64, and had at least 1 prior detox admission in the 12 months before the index detox episode were included in analyses. For this study, all detox providers in the state of Massachusetts were included, with the 4 largest sites assigned to the recovery support navigator condition, in order to focus intervention and resources on fewer sites albeit high volume sites (approx. half of total patients included), and to ensure intervention fidelity. The other 9 sites were designated to provide services as usual. Patients in sites offering services as usual were provided support and referrals from community support program staff on a fee-for-service basis (i.e., case management, community resources including food, housing, transportation, self-help groups). Community support program staff in the recovery support navigator condition were trained in Motivational Interviewing and other specialized aspects of substance use disorder care. They also provided continuous wrap-around support to facilitate post-detox link to care and provided Medicaid-billable services on a daily case rate, rather than as fee-for-service, to provide care as needed based on patient needs.
The primary outcome was whether or not patients received any substance use disorder (SUD) treatment with 14 days of discharge from inpatient detox. Eligible SUD services for a successful linkage included inpatient hospitalization, residential treatment, intensive outpatient treatment, or outpatient care. When comparing the intervention to services as usual, authors statistically controlled for a number of individual variables (e.g., age, gender, psychiatric diagnosis) as well as program variables (e.g., percentage of patients in the clinic who were women, nondisabled, on Medicaid Basic, enrolled in Medicaid for less than a year, and who had a psychiatric diagnosis), to try and isolate any independent effect of adding the navigator intervention approach to services as usual.
Patients included were between 18 and 64 who were enrolled in the Massachusetts’ Medicaid Programs’ (MassHealth) Primary Care Clinician plan. The authors included 4,236 complete cases for analysis (i.e., 2,520 in the recovery support navigator condition and 1,716 in the services as usual condition), for whom information regarding post-detox treatment data within the first 14 days post-detox was available. Participants were predominantly male (67.8%), 30 years of age or older (70.5%), had a co-occurring psychiatric diagnosis, based on Medicaid claims data (78.9%), and had completed another detox episode prior to the current, index detox episode (52.1%).
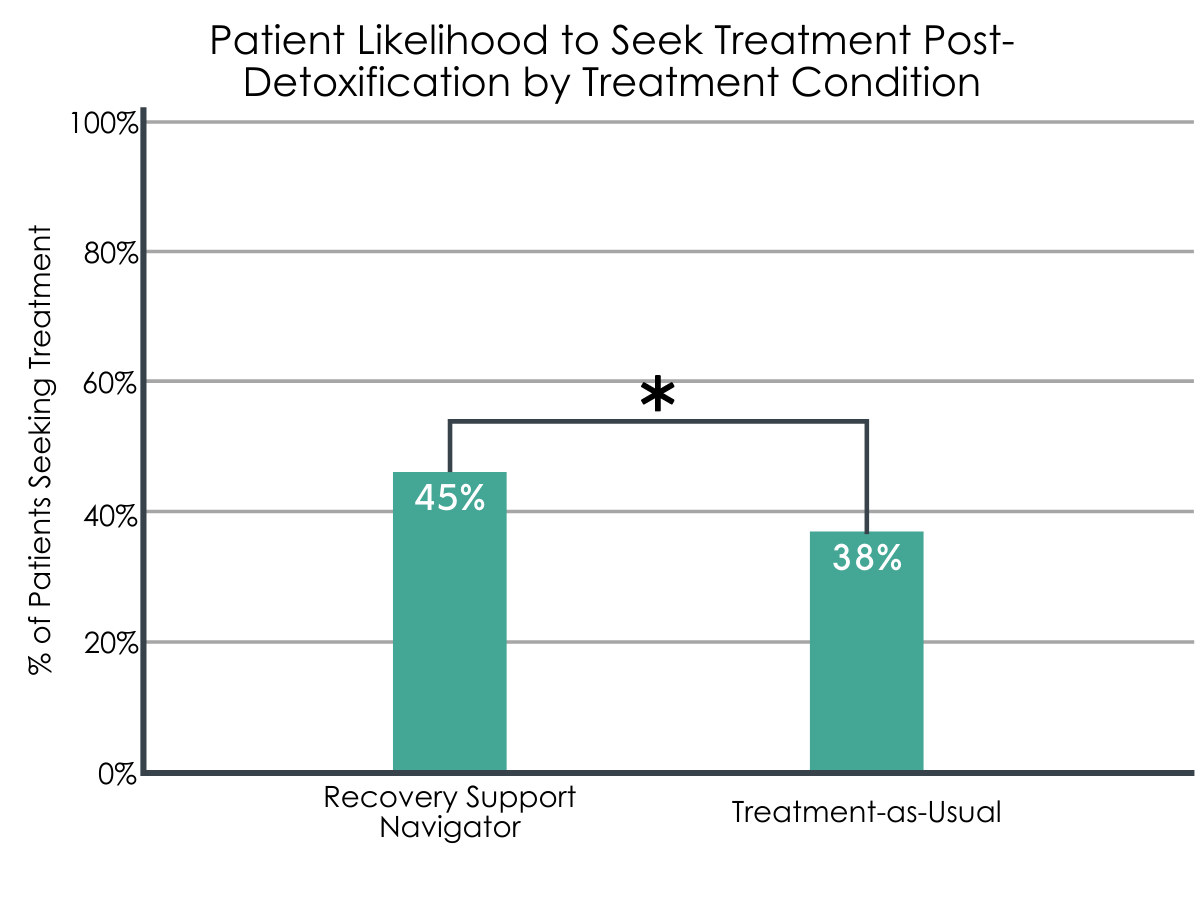
Figure 2. While the difference between conditions was statistically significant, it is worth noting that these particular numbers are raw values and were not statistically controlled for. However, an absolute magnitude difference of 7% translates to a relative advantage of 18.42% in favor of recovery support navigators – a clinically-meaningful added benefit.
WHAT DID THIS STUDY FIND?
Treatment was more likely in the recovery support navigator condition.
A total of 42% of patients attended additional treatment within 14 days of their discharge from inpatient detox. When the authors just compared the number of patients in one condition vs. the other, they found that the proportion of patients who sought additional treatment was significantly higher (45%) among patients who received support from a recovery support navigator compared to patients who received services as usual (38%).
When examined differently, and when taking into account other variables, patients who received support from a recovery support navigator were 23% more likely than patients in the services as usual condition to attend treatment within the first 2 weeks post-detox. In addition, and regardless of treatment condition, attending a prior detox episode recently, having a current psychiatric diagnosis, a documented disability, or who were on Medicaid less than 1 year (compared to more than a year) was associated with a greater likelihood of attending care within 14 days post-detox.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study highlights the ongoing “revolving door” issue of detox and post-detox readmission risk among patients with severe substance use disorders, but also a novel intervention strategy designed to help address it.
The authors developed, implemented, and also evaluated the outcomes of a new and cost-effective intervention designed to link patients to essential treatment post-detox, which used recovery support navigators to facilitate patients’ healthcare transitions. Despite finding that their intervention was associated uniquely with a 23% increase in the likelihood of post-detox treatment engagement, controlling for a host of other variables that might account for the advantage of the intervention (e.g., higher quality services at the programs where the recovery support navigation was implemented), the majority of patients in this large-scale study did not engage in treatment 2 weeks post detox. Individuals who had been in detox recently or who had a psychiatric diagnosis, for instance, were more likely to engage in treatment after detox. Given their higher severity, they might already have connections in the community and treatment resources. As such, recovery support might be less useful to these individuals as they might be to patients with less connection or awareness of treatment options post-detox. It could also be that the types of treatment options available to those who did not engage in treatment post-detox were not appealing or did not meet the needs of these individuals.
This lack of treatment engagement post-detox is critical for individuals with opioid use disorder, in particular, since this initial period after detox discharge is the highest risk time for drug overdose. The authors were unable to examine whether patients enrolled in treatment after 2 weeks, which is still possible, but nevertheless provides important insight into a new and cost-effective strategy that clinics can implement to improve short-term patient care, and potentially long-term outcomes as well. The flexibility of the fee-by-case model afforded clinicians the ability to meet with and provide more active and intensive support that may have been of added value to patients, which might also be needed to effectively engage detox patients in after care.
- LIMITATIONS
-
- The authors compared treatment outcomes following assignment of treatment to the 4 highest volume clinics in Massachusetts. This might have influenced results in ways that could have been overcome by randomly assigning clinics, patients, or both to receive the treatment or not.
- While use of administrative data is a strength in many ways, it can also be a limitation to the extent that it cannot be used to examine or control for other unmeasured considerations. Relevant factors might include healthcare sought after 14 days, patient recovery or relapse post-detox, or unmeasured provider-level factors. These factors might include characteristics of the providers in one condition vs. the other, or the extent and duration of services provided by providers across conditions.
- The authors were unable to isolate which active ingredients that were largely responsible for the intervention’s observed effect, such as whether it was the Motivational Interviewing or other recovery support services navigators offered, characteristics of the providers or clinics assigned to the treatment vs. services as usual condition, or the enhanced flexibility of recovery support navigators to provide patient-centered treatment outside the bounds of fee-for-service care, or some combination thereof.
- The authors were not able to take into account factors associated with substance use disorder or types of substance use disorder for which patients received detox services.
- The primary outcome of engagement in treatment did not include engagement in recovery other support services, such as recovery residences, recovery community centers, or mutual help organizations as these were not measured by administrative claims data.
BOTTOM LINE
- For individuals and families seeking recovery: The majority of patients admitted to inpatient detox do not engage in recommended follow up treatment, which is important for long-term recovery but especially within 2 weeks of discharge. The results of this study might indicate that recovery support navigators, trained in strategies of patient treatment engagement and motivation (i.e., Motivational Interviewing), and with the time and flexibility to work closely with patients, may have been successful in linking a higher number of patients with post-detox treatment compared to services as usual. The benefit of this intervention is that it also highlights the importance of individualized and supportive services that facilitate engagement in post-detox treatment among patients. This is also important given the that individuals who link to treatment post-detox are less likely to readmit, and repeated detox readmissions are associated with lower rates of successful detoxification in the future.
- For treatment professionals and treatment systems: The majority of patients who leave detox do not engage in recommended treatment, which is important for many for long-term recovery and is linked to lower risk of patient mortality. Use of recovery support navigators, who in the current study were trained in Motivational Interviewing, substance use disorder treatment, and who had the flexibility to provide active and person-centered care outside the bounds of fee-for-service, were more successful than providers in services as usual settings in connecting detox patients to after care. Results of this study are also supported by research demonstrating that this intervention is cost-effective and associated with net savings per patient. However, while this study was as rigorous as it could be given the nature of the data, given that this was not a randomized study, follow up research is needed to confirm these promising preliminary findings.
- For scientists: Use of recovery support navigators within inpatient detox clinics was associated with a significantly higher rate of referral and engagement in post-detox treatment. Specifically, patients in the treatment condition were 23% more likely to seek additional treatment post-detox within the 2 weeks of discharge, controlling for between-clinic differences in the percentage of patients in the clinic who were women, nondisabled, on Medicaid Basic, enrolled in Medicaid for less than a year, and who had a psychiatric diagnosis. The strengths of this study include use of large and administrative claims data. However, limitations of this design and these data include lack of measurement of important other characteristics of the patients included (e.g., substance use disorder type and severity), or provider characteristics. Another limitation that would inform dissemination and implementation of the intervention if addressed in follow up research is lack of randomization, and disaggregation of intervention components (the active ingredients) to isolate causal attributes of the intervention. While the authors controlled statistically as best they could for factors that were significantly different between included sites, randomization is a more robust method of overcoming any potential systematic differences between sites and treatment conditions.
- For policy makers: Patients who received support from recovery support navigators were 23% more likely to engage in recommended treatment in the 2 weeks following discharge from inpatient detox. Further successful linkage to after care is associated with improved patient outcomes and reduced mortality risk. The provision of these services required training of staff and the ability to bill for services in a flexible manner required for active and personalized patient care. While an investment on the part of providers, clinics, and systems, the results of this study also highlight that this intervention, while potentially effective, was also cost-effective and resulted in a net savings regarding per month patient cost. At the same time, the majority of the patients included in the current study still did not engage in follow up care. Additional intervention development aimed at reducing the “revolving door” issues among detox patients will necessitate further research and policy support to improve patient outcomes but might also result in cost-savings long-term.
CITATIONS
Lee, M. T., Torres, M., Brolin, M., Merrick, E. L., Ritter, G. A., Panas, L., Horgan, C. M., Lane, N., Hopwood, J. C., De Marco, N., & Gewirtz, A. (2020). Impact of recovery support navigators on continuity of care after detoxification. Journal of substance abuse treatment, 112, 10–16. doi: 10.1016/j.jsat.2020.01.019
