Can pharmacists improve medication stability for individuals moving across levels of addiction care?
The majority of individuals who initiate substance use disorder treatment do not complete it, with retention rates being particularly low for medication treatments. Staying engaged in medication treatment reduces substance use-related harms, including overdose. Removing barriers to accessing continuing medication care may be key. This study evaluated the effects of a U.S. Veteran’s Affairs pharmacist-led telephone clinic program on retention in medication treatment among individuals transitioning from inpatient to outpatient care.
Recent data suggest that only about 40% of veterans with opioid use disorder utilize medication treatments like buprenorphine, methadone, or extended-release naltrexone. Similarly, about 7% – 11% of veterans with alcohol use disorder use FDA-approved medications like naltrexone in the Veterans Health Administration (VHA). To address these issues, the VA has recently implemented initiatives to increase the use of these medication services within their healthcare system.
While initiation can be critically important, retention in medication treatment can be equally so. Unpublished pilot data from this research team suggest that only 10% of veterans in VA inpatient psychiatric care were initiated on medication treatments for opioid use disorder and all of these patients had discontinued medication treatment within 6 months. Though inpatient treatment is an opportune time to engage and start individuals on a medication, continuation when a patient leaves inpatient treatment can be difficult and many programs fail to help patients transition to community-based care. To improve post-discharge outcomes and enhance continuity of care among patients, the VA recently developed a pharmacist-led telephone clinic to help individuals with their medication treatment and care transitions (e.g., from inpatient to outpatient). This study examined the pharmacist’s role in this new pharmacist-led program, as well as its effect on helping veterans continue on the medication over time among those who started medication treatment for alcohol and opioid use disorders during inpatient care.
HOW WAS THIS STUDY CONDUCTED?
The researchers conducted a retrospective observational cohort study of a pharmacist-led telephone clinic program on medication treatment retention among individuals discharged from Veterans Affairs (VA) inpatient psychiatric hospitalization. All participants started taking either buprenorphine (i.e., for opioid use disorder; often prescribed with naloxone and known by the brand name, Suboxone) or extended-release injectable naltrexone (i.e., for alcohol or opioid use disorder; also known by the brand name, Vivitrol) to help treat their opioid or alcohol use disorder at the start of their inpatient stay, and continued medication treatment up until the time of discharge.
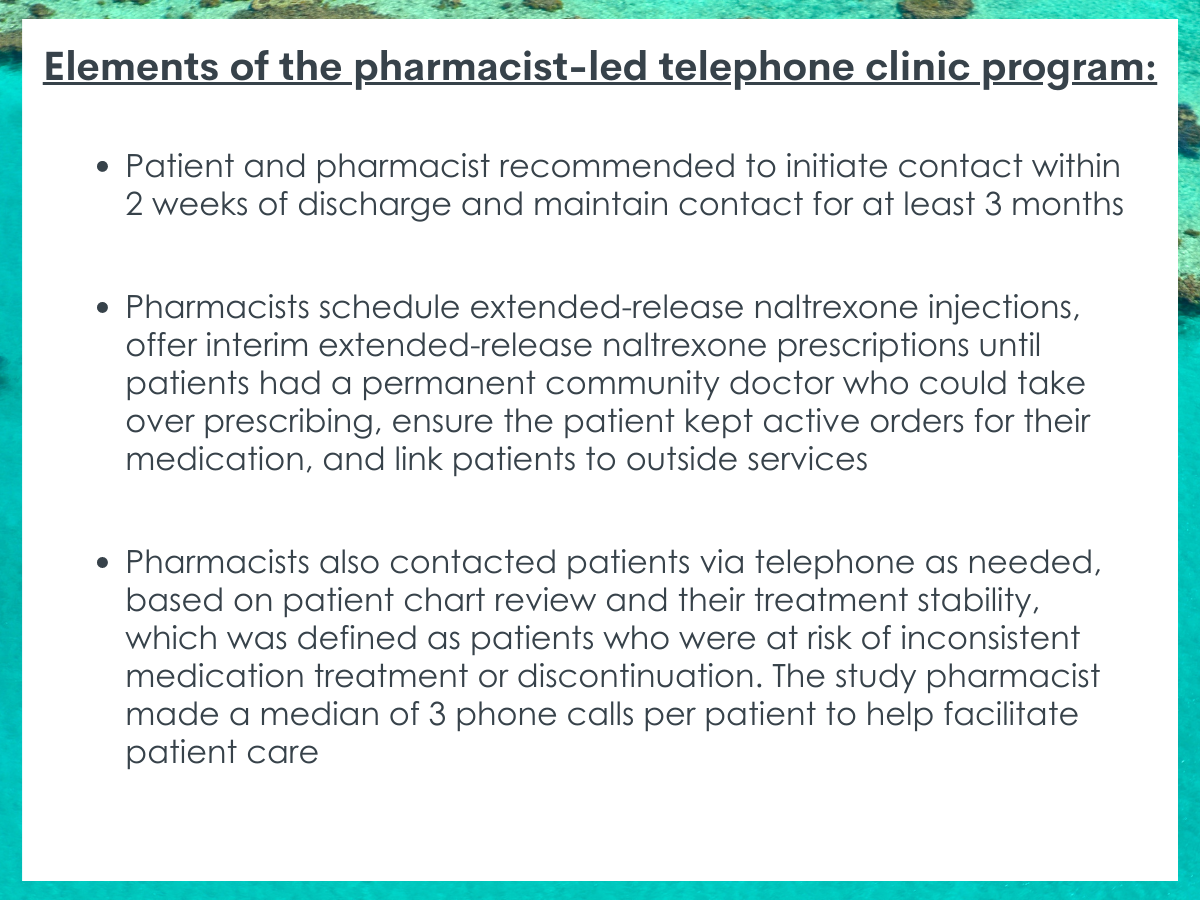
Fifty-four individuals enrolled in the pharmacist-led telephone clinic program, which was intended to help patients continue taking their medication after discharge. Medical staff at the inpatient hospital referred patients to this clinic and subsequently contacted a team of psychiatric pharmacy residents at the time of discharge to enroll the patient in the program. The patient and the pharmacist were recommended to initiate contact within 2 weeks of discharge and to maintain contact as needed for a total of at least 3 months. As part of their role in the program, pharmacists scheduled extended-release naltrexone injections, offered interim extended-release naltrexone prescriptions until patients had a permanent community doctor who could take over prescribing, ensured the patient kept active orders for their medication, and linked patients to outside services (e.g., primary care, specialty clinics, social support services). The pharmacist also contacted patients via telephone as needed, based on patient chart review and their treatment stability, which was defined as patients who were at risk of inconsistent medication treatment or discontinuation (e.g., missed appointments). The study pharmacist made a median of 3 (range 0–4) phone calls per patient to help facilitate patient care. The patients in this active intervention group were compared to a control group of ninety-six individuals who were discharged from inpatient hospitalization but were not identified as clinic candidates by the inpatient medical staff and, therefore, did not enroll in the transitional care program.
The continuation of the medication treatment was examined for buprenorphine and extended-release naltrexone combined, and independently for each medication type. Retention was evaluated at 1- and 3-months after starting the medication. Medication retention was defined as continuous acquisition of a patient’s medication at the time of prescription refill. The researchers also examined activities performed by the pharmacist as part of the intervention.
All participants were adults within the VA system who had not engaged in buprenorphine or extended-release naltrexone treatment in the 3 months prior to hospitalization and, after starting one of these treatments at inpatient treatment, had not switched to a different medication during the study period. Of note, the study did not account for pre-existing differences on alcohol and opioid diagnoses between the intervention and comparison patient groups when testing whether the pharmacist-led intervention was more helpful or not. Importantly, a greater percentage of individuals in the intervention group had opioid use disorder alone, whereas more patients in the control group had co-occurring alcohol and opioid use disorders. Accordingly, a greater percentage of patients in the active intervention group received buprenorphine (86% vs. 57%) or extended-release naltrexone (18% vs. 0%) for opioid use disorder, compared to patients in the control group. Groups were statistically similar, however, on other measured variables, including demographic characteristics and referral source. Overall, the majority of patients in both groups were prescribed extended-release injectable naltrexone (~60%). The majority of participants were White (78%) men (95%) and 48 years old, on average.
WHAT DID THIS STUDY FIND?
The pharmacist most commonly helped the intervention group patients by facilitating scheduling and prescribing medications.
Across all 54 participants enrolled in the telephone clinic program, the pharmacist most commonly scheduled extended-release naltrexone injections (20 times in total across all of the patients in that group), prescribed or prompted medication treatment orders (19 times), and recommended or ordered patient labs (15 times). The pharmacist less frequently provided oral naloxone to patients (1 time) or coordinated care with outside facilities (3 times).
Retention was better among patients who enrolled in the pharmacist-led telephone clinic program.
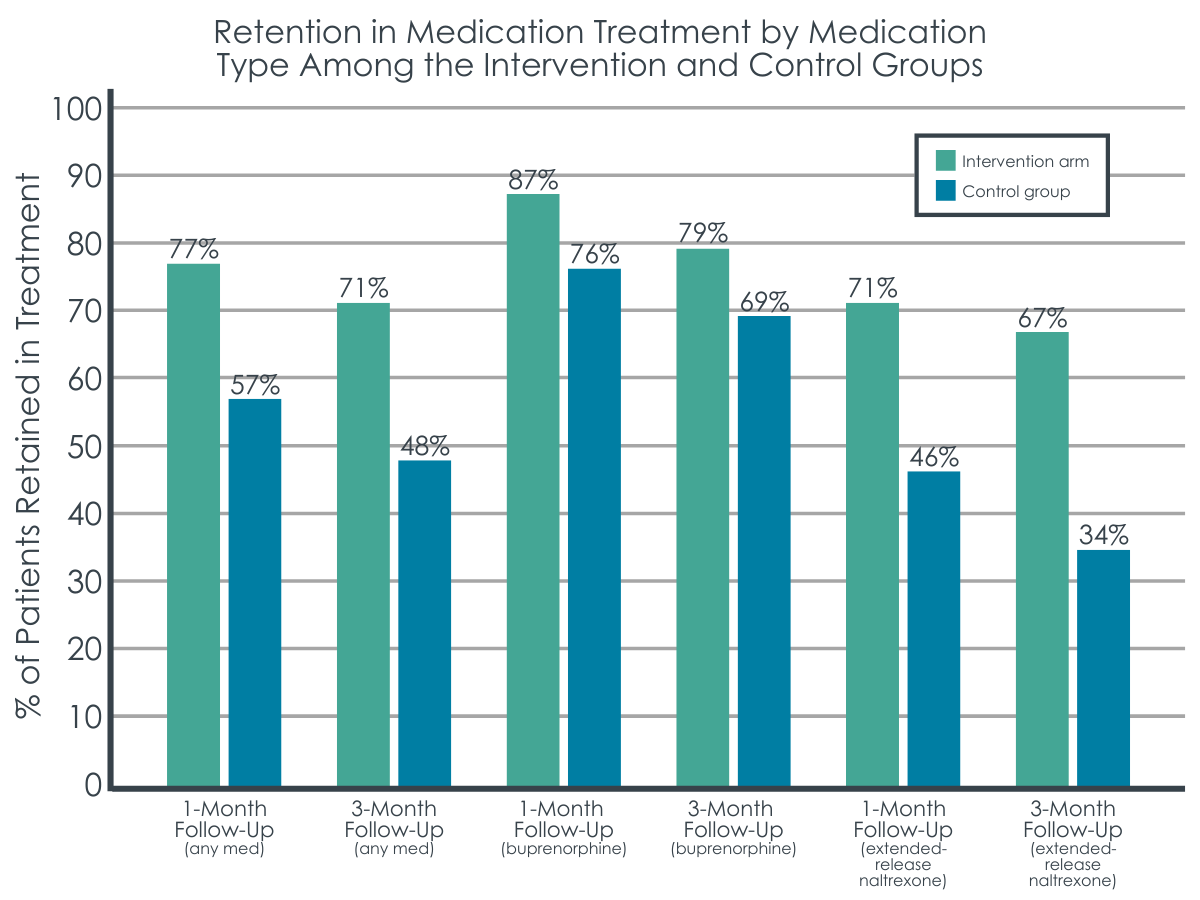
Compared to the control group, a greater percentage of individuals in the intervention group continued their medication treatment for alcohol or opioid use disorder after 1 month and 3 months of starting it. This was largely accounted for by retention rates among those who received extended-release injectable naltrexone, given that a larger proportion of these patients discontinued treatment at both follow-up periods when they did not receive the pharmacist-led intervention. No significant differences between the intervention and control groups were seen in buprenorphine retention rates at 1- or 3-month follow-up.
Figure 2. Depicts the percentage of patients who continued medication treatment 1 and 3 months after initiating it. A greater percentage of patients who received the pharmacist-led telephone program continued their medication treatment, relative to those who didn’t receive the program. This difference was largely accounted for by patients who received extended-release naltrexone.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand what may or may not work improving the continuity of medication treatment among patients transitioning to various levels of care. With retention in medication treatmentbeing difficult both within and outside the VA system, and the majority of individuals discontinuing medication treatment within 6 months, it is essential to identify bridge programs or interim services that allow patients the time they need to establish more permanent care with providers in their community to continue their medication treatment.
Continuation of treatment is important because taking these medications for six months or more is often needed for patients to reap their benefits, which include greater engagement in addiction treatment, improved well-being and quality of life, as well as reductions in substance use, risk of overdose and/or all-cause mortality.
Retention is particularly important for opioid agonist treatments like buprenorphine, with studies showing that less than 6 months of treatment significantly increases a patient’s risk of overdose, emergency department visits, and hospitalizations. However, individuals transitioning between levels of care can face long wait times, and delayed transitions can lead to gaps in medication treatment that put a patient at risk of discontinuation. Programs that help patients find more permanent providers and temporarily aid in the management of their treatment during care transitions, like the one investigated in the current study, might help address some of these transition-related barriers to continued medication treatment.
The patients who enrolled in the pharmacist-led telephone clinic program after inpatient hospitalization appeared to benefit compared to those who did not enroll. This was particularly true for extended-release naltrexone, with the intervention group showing a 25 – 33% boost in retention rates compared to the control group. However, it is important to note that the researchers did not control statistically for baseline differences between the intervention and control groups. The control group had a higher prevalence of comorbid alcohol use disorder and opioid use disorder, and this heightened level of clinical severity may have contributed to the increased rates of drop out seen in this group. Indeed, studies show that retention in extended release naltrexone (but not buprenorphine) treatment may be lower in individuals with these comorbid disorders. Buprenorphine did a relatively good job of retaining patients with or without receipt of the pharmacist-led telephone clinic program, with high retention rates seen at 1- and 3- month follow up. Similarly high retention rates have been demonstrated at early follow-up periods in other studies, with some revealing retention rates of 77% – 85% after one month of buprenorphine treatment.
Given the importance of treatment beyond 6 months, additional research is needed to examine longer-follow-up periods after exposure to transitional care programs like this within the VA. Rates of treatment retention at short and long-term follow up in clinical trials show that about 1 in 3 patients drop-out of treatment after receiving 2 to 6 months of extended-release naltrexone for alcohol or opioid use disorders. Similarly, research has shown that 2 out of 3 patients receiving buprenorphine for opioid use disorder discontinue it within 6 months of treatment, with one out of four patients discontinuing in the first month. Dose is also an important consideration in treatment retention that was not assessed here, warranting further study. There are many other important baseline characteristics that may have differed between the intervention and control groups that were not controlled for in this study. This makes it difficult to determine whether the telephone-based continuing care program was directly responsible for the observed benefits or if characteristics of the patients in the intervention group made them more likely to engage after discharge from inpatient treatment. Additional randomized controlled studies with balanced groups will help characterize the causal effects of continuing care programs like the one studied here.
Importantly, the number of intervention activities performed by the pharmacist in this telephone clinic program were limited (ranging from 0–4 activities) and a more intensive or involved program may help to further enhance retention and continuity of care among patients transitioning from controlled inpatient environments to outpatient treatment settings. In particular, there were few referrals to specialty clinics (e.g., addiction treatment services) and few efforts to coordinate medication treatment with other facilities, which may have significantly aided ongoing medication treatment among certain patients. Improving communication between healthcare sectors, departments, and programs might ultimately help to enhance the effects of programs like these, which are important promising approaches to continuing care.
Though this study cannot speak to the direct causal effects of this continuing care intervention on retention, studies of similar interventions with other types of patients and treatment outcomes have revealed the benefits of programs like this one, including recovery management checkups, telemedicine- and telephone-based continuing care.
Small sample sizes limited interpretations about the effect of this pharmacist-led clinic program on re-hospitalization and emergency department visits at follow-up. Though trend level differences could be observed, the groups ultimately did not significantly differ. It also limited ability to evaluate sub-groups by intervention, substance use disorder (alcohol, opioid, or both), and medication treatment type.
The pharmacist’s role in the program was variable and patient outreach was on an as-needed basis, making it difficult to quantify the amount of patient exposure to the program and how this might impact outcomes. In addition, the number of intervention activities performed by the pharmacist appeared relatively minimal and it appears that some patients got more attention than others (range of activities per patient = 0 – 4), which could have influenced the overall effect of the program on retention in group analyses.
The control group had more clinical severity (i.e., higher prevalence of dual diagnosis of alcohol and opioid use disorder), hindering the ability to determine whether the intervention was responsible for better outcomes. The dose of extended-release naltrexone and buprenorphine received was not considered, and this deserves additional attention given the role of dose in retention.
BOTTOM LINE
This retrospective observational cohort study found that a pharmacist-led telephone clinic program may help to promote continued medication treatment for veterans with opioid and/or alcohol use disorders who initiate medication in inpatient VA psychiatric treatment and intend to continue after discharged. Such a program may be particularly beneficial for retaining patients in community-based extended-release naltrexone treatment but randomized controlled trials or rigorous quasi-experimental studies are needed to draw conclusions.
For individuals and families seeking recovery: Currently, programs that help individuals transition their medication treatment between different levels of substance use disorder care (e.g., inpatient to outpatient) are not widely available. However, the availability of programs like this are starting to grow. Individuals who are planning to start medication treatment for substance use disorder in one setting and continue it in another should ask their providers about options for a smooth transition without gaps in care.
For treatment professionals and treatment systems: Given the importance of continuity of care to help prevent relapse and recurrence of substance use disorder, particularly in the context of medication treatments for opioid and alcohol use disorders, healthcare professionals might consider developing programs that ensure patient support during care transitions. “Bridge” clinics that provide interim medication treatment for individuals without established providers may help to ensure treatment retention upon transition to various levels of care, which can ultimately enhance patient outcomes and reduce overdose death risk, particularly for individuals with opioid use disorder.
For scientists:Additional research is needed to replicate and extend these findings in various VA settings, and to identify the extent to which such programs are truly helpful with randomized controlled trials and well-designed quasi-experimental studies. Manualizing such interventions and testing them systematically will allow for a more comprehensive and clear understanding of the effects of transitional programs for medication treatment retention. Investigations that allow for the examination of interactions between group assignment, medication type and dose, disorder type, and patient’s level of exposure to program components will also help further our understanding of whether or not these programs are effective for enhancing retention in medication treatment after inpatient care.
For policy makers: Additional programmatic and research funding will help to develop and test programs intended to increase patient retention in empirically-supported medication treatments for opioid and alcohol use disorders. Developing useful programs that prevent gaps in medication treatment during transitions between various types of care (e.g., outpatient, inpatient, residential, etc.) can ultimately help to mitigate adverse events (including premature death) and address the clinical and patient burden of repeat treatment intakes due to relapse and recurrence of symptoms. It also has the potential to help reduce the number of alcohol deaths and opioid overdose deaths that occur due to a discontinuation of medication treatment.
Recent data suggest that only about 40% of veterans with opioid use disorder utilize medication treatments like buprenorphine, methadone, or extended-release naltrexone. Similarly, about 7% – 11% of veterans with alcohol use disorder use FDA-approved medications like naltrexone in the Veterans Health Administration (VHA). To address these issues, the VA has recently implemented initiatives to increase the use of these medication services within their healthcare system.
While initiation can be critically important, retention in medication treatment can be equally so. Unpublished pilot data from this research team suggest that only 10% of veterans in VA inpatient psychiatric care were initiated on medication treatments for opioid use disorder and all of these patients had discontinued medication treatment within 6 months. Though inpatient treatment is an opportune time to engage and start individuals on a medication, continuation when a patient leaves inpatient treatment can be difficult and many programs fail to help patients transition to community-based care. To improve post-discharge outcomes and enhance continuity of care among patients, the VA recently developed a pharmacist-led telephone clinic to help individuals with their medication treatment and care transitions (e.g., from inpatient to outpatient). This study examined the pharmacist’s role in this new pharmacist-led program, as well as its effect on helping veterans continue on the medication over time among those who started medication treatment for alcohol and opioid use disorders during inpatient care.
HOW WAS THIS STUDY CONDUCTED?
The researchers conducted a retrospective observational cohort study of a pharmacist-led telephone clinic program on medication treatment retention among individuals discharged from Veterans Affairs (VA) inpatient psychiatric hospitalization. All participants started taking either buprenorphine (i.e., for opioid use disorder; often prescribed with naloxone and known by the brand name, Suboxone) or extended-release injectable naltrexone (i.e., for alcohol or opioid use disorder; also known by the brand name, Vivitrol) to help treat their opioid or alcohol use disorder at the start of their inpatient stay, and continued medication treatment up until the time of discharge.
Fifty-four individuals enrolled in the pharmacist-led telephone clinic program, which was intended to help patients continue taking their medication after discharge. Medical staff at the inpatient hospital referred patients to this clinic and subsequently contacted a team of psychiatric pharmacy residents at the time of discharge to enroll the patient in the program. The patient and the pharmacist were recommended to initiate contact within 2 weeks of discharge and to maintain contact as needed for a total of at least 3 months. As part of their role in the program, pharmacists scheduled extended-release naltrexone injections, offered interim extended-release naltrexone prescriptions until patients had a permanent community doctor who could take over prescribing, ensured the patient kept active orders for their medication, and linked patients to outside services (e.g., primary care, specialty clinics, social support services). The pharmacist also contacted patients via telephone as needed, based on patient chart review and their treatment stability, which was defined as patients who were at risk of inconsistent medication treatment or discontinuation (e.g., missed appointments). The study pharmacist made a median of 3 (range 0–4) phone calls per patient to help facilitate patient care. The patients in this active intervention group were compared to a control group of ninety-six individuals who were discharged from inpatient hospitalization but were not identified as clinic candidates by the inpatient medical staff and, therefore, did not enroll in the transitional care program.
The continuation of the medication treatment was examined for buprenorphine and extended-release naltrexone combined, and independently for each medication type. Retention was evaluated at 1- and 3-months after starting the medication. Medication retention was defined as continuous acquisition of a patient’s medication at the time of prescription refill. The researchers also examined activities performed by the pharmacist as part of the intervention.
All participants were adults within the VA system who had not engaged in buprenorphine or extended-release naltrexone treatment in the 3 months prior to hospitalization and, after starting one of these treatments at inpatient treatment, had not switched to a different medication during the study period. Of note, the study did not account for pre-existing differences on alcohol and opioid diagnoses between the intervention and comparison patient groups when testing whether the pharmacist-led intervention was more helpful or not. Importantly, a greater percentage of individuals in the intervention group had opioid use disorder alone, whereas more patients in the control group had co-occurring alcohol and opioid use disorders. Accordingly, a greater percentage of patients in the active intervention group received buprenorphine (86% vs. 57%) or extended-release naltrexone (18% vs. 0%) for opioid use disorder, compared to patients in the control group. Groups were statistically similar, however, on other measured variables, including demographic characteristics and referral source. Overall, the majority of patients in both groups were prescribed extended-release injectable naltrexone (~60%). The majority of participants were White (78%) men (95%) and 48 years old, on average.
WHAT DID THIS STUDY FIND?
The pharmacist most commonly helped the intervention group patients by facilitating scheduling and prescribing medications.
Across all 54 participants enrolled in the telephone clinic program, the pharmacist most commonly scheduled extended-release naltrexone injections (20 times in total across all of the patients in that group), prescribed or prompted medication treatment orders (19 times), and recommended or ordered patient labs (15 times). The pharmacist less frequently provided oral naloxone to patients (1 time) or coordinated care with outside facilities (3 times).
Retention was better among patients who enrolled in the pharmacist-led telephone clinic program.
Compared to the control group, a greater percentage of individuals in the intervention group continued their medication treatment for alcohol or opioid use disorder after 1 month and 3 months of starting it. This was largely accounted for by retention rates among those who received extended-release injectable naltrexone, given that a larger proportion of these patients discontinued treatment at both follow-up periods when they did not receive the pharmacist-led intervention. No significant differences between the intervention and control groups were seen in buprenorphine retention rates at 1- or 3-month follow-up.
Figure 2. Depicts the percentage of patients who continued medication treatment 1 and 3 months after initiating it. A greater percentage of patients who received the pharmacist-led telephone program continued their medication treatment, relative to those who didn’t receive the program. This difference was largely accounted for by patients who received extended-release naltrexone.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand what may or may not work improving the continuity of medication treatment among patients transitioning to various levels of care. With retention in medication treatmentbeing difficult both within and outside the VA system, and the majority of individuals discontinuing medication treatment within 6 months, it is essential to identify bridge programs or interim services that allow patients the time they need to establish more permanent care with providers in their community to continue their medication treatment.
Continuation of treatment is important because taking these medications for six months or more is often needed for patients to reap their benefits, which include greater engagement in addiction treatment, improved well-being and quality of life, as well as reductions in substance use, risk of overdose and/or all-cause mortality.
Retention is particularly important for opioid agonist treatments like buprenorphine, with studies showing that less than 6 months of treatment significantly increases a patient’s risk of overdose, emergency department visits, and hospitalizations. However, individuals transitioning between levels of care can face long wait times, and delayed transitions can lead to gaps in medication treatment that put a patient at risk of discontinuation. Programs that help patients find more permanent providers and temporarily aid in the management of their treatment during care transitions, like the one investigated in the current study, might help address some of these transition-related barriers to continued medication treatment.
The patients who enrolled in the pharmacist-led telephone clinic program after inpatient hospitalization appeared to benefit compared to those who did not enroll. This was particularly true for extended-release naltrexone, with the intervention group showing a 25 – 33% boost in retention rates compared to the control group. However, it is important to note that the researchers did not control statistically for baseline differences between the intervention and control groups. The control group had a higher prevalence of comorbid alcohol use disorder and opioid use disorder, and this heightened level of clinical severity may have contributed to the increased rates of drop out seen in this group. Indeed, studies show that retention in extended release naltrexone (but not buprenorphine) treatment may be lower in individuals with these comorbid disorders. Buprenorphine did a relatively good job of retaining patients with or without receipt of the pharmacist-led telephone clinic program, with high retention rates seen at 1- and 3- month follow up. Similarly high retention rates have been demonstrated at early follow-up periods in other studies, with some revealing retention rates of 77% – 85% after one month of buprenorphine treatment.
Given the importance of treatment beyond 6 months, additional research is needed to examine longer-follow-up periods after exposure to transitional care programs like this within the VA. Rates of treatment retention at short and long-term follow up in clinical trials show that about 1 in 3 patients drop-out of treatment after receiving 2 to 6 months of extended-release naltrexone for alcohol or opioid use disorders. Similarly, research has shown that 2 out of 3 patients receiving buprenorphine for opioid use disorder discontinue it within 6 months of treatment, with one out of four patients discontinuing in the first month. Dose is also an important consideration in treatment retention that was not assessed here, warranting further study. There are many other important baseline characteristics that may have differed between the intervention and control groups that were not controlled for in this study. This makes it difficult to determine whether the telephone-based continuing care program was directly responsible for the observed benefits or if characteristics of the patients in the intervention group made them more likely to engage after discharge from inpatient treatment. Additional randomized controlled studies with balanced groups will help characterize the causal effects of continuing care programs like the one studied here.
Importantly, the number of intervention activities performed by the pharmacist in this telephone clinic program were limited (ranging from 0–4 activities) and a more intensive or involved program may help to further enhance retention and continuity of care among patients transitioning from controlled inpatient environments to outpatient treatment settings. In particular, there were few referrals to specialty clinics (e.g., addiction treatment services) and few efforts to coordinate medication treatment with other facilities, which may have significantly aided ongoing medication treatment among certain patients. Improving communication between healthcare sectors, departments, and programs might ultimately help to enhance the effects of programs like these, which are important promising approaches to continuing care.
Though this study cannot speak to the direct causal effects of this continuing care intervention on retention, studies of similar interventions with other types of patients and treatment outcomes have revealed the benefits of programs like this one, including recovery management checkups, telemedicine- and telephone-based continuing care.
Small sample sizes limited interpretations about the effect of this pharmacist-led clinic program on re-hospitalization and emergency department visits at follow-up. Though trend level differences could be observed, the groups ultimately did not significantly differ. It also limited ability to evaluate sub-groups by intervention, substance use disorder (alcohol, opioid, or both), and medication treatment type.
The pharmacist’s role in the program was variable and patient outreach was on an as-needed basis, making it difficult to quantify the amount of patient exposure to the program and how this might impact outcomes. In addition, the number of intervention activities performed by the pharmacist appeared relatively minimal and it appears that some patients got more attention than others (range of activities per patient = 0 – 4), which could have influenced the overall effect of the program on retention in group analyses.
The control group had more clinical severity (i.e., higher prevalence of dual diagnosis of alcohol and opioid use disorder), hindering the ability to determine whether the intervention was responsible for better outcomes. The dose of extended-release naltrexone and buprenorphine received was not considered, and this deserves additional attention given the role of dose in retention.
BOTTOM LINE
This retrospective observational cohort study found that a pharmacist-led telephone clinic program may help to promote continued medication treatment for veterans with opioid and/or alcohol use disorders who initiate medication in inpatient VA psychiatric treatment and intend to continue after discharged. Such a program may be particularly beneficial for retaining patients in community-based extended-release naltrexone treatment but randomized controlled trials or rigorous quasi-experimental studies are needed to draw conclusions.
For individuals and families seeking recovery: Currently, programs that help individuals transition their medication treatment between different levels of substance use disorder care (e.g., inpatient to outpatient) are not widely available. However, the availability of programs like this are starting to grow. Individuals who are planning to start medication treatment for substance use disorder in one setting and continue it in another should ask their providers about options for a smooth transition without gaps in care.
For treatment professionals and treatment systems: Given the importance of continuity of care to help prevent relapse and recurrence of substance use disorder, particularly in the context of medication treatments for opioid and alcohol use disorders, healthcare professionals might consider developing programs that ensure patient support during care transitions. “Bridge” clinics that provide interim medication treatment for individuals without established providers may help to ensure treatment retention upon transition to various levels of care, which can ultimately enhance patient outcomes and reduce overdose death risk, particularly for individuals with opioid use disorder.
For scientists:Additional research is needed to replicate and extend these findings in various VA settings, and to identify the extent to which such programs are truly helpful with randomized controlled trials and well-designed quasi-experimental studies. Manualizing such interventions and testing them systematically will allow for a more comprehensive and clear understanding of the effects of transitional programs for medication treatment retention. Investigations that allow for the examination of interactions between group assignment, medication type and dose, disorder type, and patient’s level of exposure to program components will also help further our understanding of whether or not these programs are effective for enhancing retention in medication treatment after inpatient care.
For policy makers: Additional programmatic and research funding will help to develop and test programs intended to increase patient retention in empirically-supported medication treatments for opioid and alcohol use disorders. Developing useful programs that prevent gaps in medication treatment during transitions between various types of care (e.g., outpatient, inpatient, residential, etc.) can ultimately help to mitigate adverse events (including premature death) and address the clinical and patient burden of repeat treatment intakes due to relapse and recurrence of symptoms. It also has the potential to help reduce the number of alcohol deaths and opioid overdose deaths that occur due to a discontinuation of medication treatment.
Recent data suggest that only about 40% of veterans with opioid use disorder utilize medication treatments like buprenorphine, methadone, or extended-release naltrexone. Similarly, about 7% – 11% of veterans with alcohol use disorder use FDA-approved medications like naltrexone in the Veterans Health Administration (VHA). To address these issues, the VA has recently implemented initiatives to increase the use of these medication services within their healthcare system.
While initiation can be critically important, retention in medication treatment can be equally so. Unpublished pilot data from this research team suggest that only 10% of veterans in VA inpatient psychiatric care were initiated on medication treatments for opioid use disorder and all of these patients had discontinued medication treatment within 6 months. Though inpatient treatment is an opportune time to engage and start individuals on a medication, continuation when a patient leaves inpatient treatment can be difficult and many programs fail to help patients transition to community-based care. To improve post-discharge outcomes and enhance continuity of care among patients, the VA recently developed a pharmacist-led telephone clinic to help individuals with their medication treatment and care transitions (e.g., from inpatient to outpatient). This study examined the pharmacist’s role in this new pharmacist-led program, as well as its effect on helping veterans continue on the medication over time among those who started medication treatment for alcohol and opioid use disorders during inpatient care.
HOW WAS THIS STUDY CONDUCTED?
The researchers conducted a retrospective observational cohort study of a pharmacist-led telephone clinic program on medication treatment retention among individuals discharged from Veterans Affairs (VA) inpatient psychiatric hospitalization. All participants started taking either buprenorphine (i.e., for opioid use disorder; often prescribed with naloxone and known by the brand name, Suboxone) or extended-release injectable naltrexone (i.e., for alcohol or opioid use disorder; also known by the brand name, Vivitrol) to help treat their opioid or alcohol use disorder at the start of their inpatient stay, and continued medication treatment up until the time of discharge.
Fifty-four individuals enrolled in the pharmacist-led telephone clinic program, which was intended to help patients continue taking their medication after discharge. Medical staff at the inpatient hospital referred patients to this clinic and subsequently contacted a team of psychiatric pharmacy residents at the time of discharge to enroll the patient in the program. The patient and the pharmacist were recommended to initiate contact within 2 weeks of discharge and to maintain contact as needed for a total of at least 3 months. As part of their role in the program, pharmacists scheduled extended-release naltrexone injections, offered interim extended-release naltrexone prescriptions until patients had a permanent community doctor who could take over prescribing, ensured the patient kept active orders for their medication, and linked patients to outside services (e.g., primary care, specialty clinics, social support services). The pharmacist also contacted patients via telephone as needed, based on patient chart review and their treatment stability, which was defined as patients who were at risk of inconsistent medication treatment or discontinuation (e.g., missed appointments). The study pharmacist made a median of 3 (range 0–4) phone calls per patient to help facilitate patient care. The patients in this active intervention group were compared to a control group of ninety-six individuals who were discharged from inpatient hospitalization but were not identified as clinic candidates by the inpatient medical staff and, therefore, did not enroll in the transitional care program.
The continuation of the medication treatment was examined for buprenorphine and extended-release naltrexone combined, and independently for each medication type. Retention was evaluated at 1- and 3-months after starting the medication. Medication retention was defined as continuous acquisition of a patient’s medication at the time of prescription refill. The researchers also examined activities performed by the pharmacist as part of the intervention.
All participants were adults within the VA system who had not engaged in buprenorphine or extended-release naltrexone treatment in the 3 months prior to hospitalization and, after starting one of these treatments at inpatient treatment, had not switched to a different medication during the study period. Of note, the study did not account for pre-existing differences on alcohol and opioid diagnoses between the intervention and comparison patient groups when testing whether the pharmacist-led intervention was more helpful or not. Importantly, a greater percentage of individuals in the intervention group had opioid use disorder alone, whereas more patients in the control group had co-occurring alcohol and opioid use disorders. Accordingly, a greater percentage of patients in the active intervention group received buprenorphine (86% vs. 57%) or extended-release naltrexone (18% vs. 0%) for opioid use disorder, compared to patients in the control group. Groups were statistically similar, however, on other measured variables, including demographic characteristics and referral source. Overall, the majority of patients in both groups were prescribed extended-release injectable naltrexone (~60%). The majority of participants were White (78%) men (95%) and 48 years old, on average.
WHAT DID THIS STUDY FIND?
The pharmacist most commonly helped the intervention group patients by facilitating scheduling and prescribing medications.
Across all 54 participants enrolled in the telephone clinic program, the pharmacist most commonly scheduled extended-release naltrexone injections (20 times in total across all of the patients in that group), prescribed or prompted medication treatment orders (19 times), and recommended or ordered patient labs (15 times). The pharmacist less frequently provided oral naloxone to patients (1 time) or coordinated care with outside facilities (3 times).
Retention was better among patients who enrolled in the pharmacist-led telephone clinic program.
Compared to the control group, a greater percentage of individuals in the intervention group continued their medication treatment for alcohol or opioid use disorder after 1 month and 3 months of starting it. This was largely accounted for by retention rates among those who received extended-release injectable naltrexone, given that a larger proportion of these patients discontinued treatment at both follow-up periods when they did not receive the pharmacist-led intervention. No significant differences between the intervention and control groups were seen in buprenorphine retention rates at 1- or 3-month follow-up.
Figure 2. Depicts the percentage of patients who continued medication treatment 1 and 3 months after initiating it. A greater percentage of patients who received the pharmacist-led telephone program continued their medication treatment, relative to those who didn’t receive the program. This difference was largely accounted for by patients who received extended-release naltrexone.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand what may or may not work improving the continuity of medication treatment among patients transitioning to various levels of care. With retention in medication treatmentbeing difficult both within and outside the VA system, and the majority of individuals discontinuing medication treatment within 6 months, it is essential to identify bridge programs or interim services that allow patients the time they need to establish more permanent care with providers in their community to continue their medication treatment.
Continuation of treatment is important because taking these medications for six months or more is often needed for patients to reap their benefits, which include greater engagement in addiction treatment, improved well-being and quality of life, as well as reductions in substance use, risk of overdose and/or all-cause mortality.
Retention is particularly important for opioid agonist treatments like buprenorphine, with studies showing that less than 6 months of treatment significantly increases a patient’s risk of overdose, emergency department visits, and hospitalizations. However, individuals transitioning between levels of care can face long wait times, and delayed transitions can lead to gaps in medication treatment that put a patient at risk of discontinuation. Programs that help patients find more permanent providers and temporarily aid in the management of their treatment during care transitions, like the one investigated in the current study, might help address some of these transition-related barriers to continued medication treatment.
The patients who enrolled in the pharmacist-led telephone clinic program after inpatient hospitalization appeared to benefit compared to those who did not enroll. This was particularly true for extended-release naltrexone, with the intervention group showing a 25 – 33% boost in retention rates compared to the control group. However, it is important to note that the researchers did not control statistically for baseline differences between the intervention and control groups. The control group had a higher prevalence of comorbid alcohol use disorder and opioid use disorder, and this heightened level of clinical severity may have contributed to the increased rates of drop out seen in this group. Indeed, studies show that retention in extended release naltrexone (but not buprenorphine) treatment may be lower in individuals with these comorbid disorders. Buprenorphine did a relatively good job of retaining patients with or without receipt of the pharmacist-led telephone clinic program, with high retention rates seen at 1- and 3- month follow up. Similarly high retention rates have been demonstrated at early follow-up periods in other studies, with some revealing retention rates of 77% – 85% after one month of buprenorphine treatment.
Given the importance of treatment beyond 6 months, additional research is needed to examine longer-follow-up periods after exposure to transitional care programs like this within the VA. Rates of treatment retention at short and long-term follow up in clinical trials show that about 1 in 3 patients drop-out of treatment after receiving 2 to 6 months of extended-release naltrexone for alcohol or opioid use disorders. Similarly, research has shown that 2 out of 3 patients receiving buprenorphine for opioid use disorder discontinue it within 6 months of treatment, with one out of four patients discontinuing in the first month. Dose is also an important consideration in treatment retention that was not assessed here, warranting further study. There are many other important baseline characteristics that may have differed between the intervention and control groups that were not controlled for in this study. This makes it difficult to determine whether the telephone-based continuing care program was directly responsible for the observed benefits or if characteristics of the patients in the intervention group made them more likely to engage after discharge from inpatient treatment. Additional randomized controlled studies with balanced groups will help characterize the causal effects of continuing care programs like the one studied here.
Importantly, the number of intervention activities performed by the pharmacist in this telephone clinic program were limited (ranging from 0–4 activities) and a more intensive or involved program may help to further enhance retention and continuity of care among patients transitioning from controlled inpatient environments to outpatient treatment settings. In particular, there were few referrals to specialty clinics (e.g., addiction treatment services) and few efforts to coordinate medication treatment with other facilities, which may have significantly aided ongoing medication treatment among certain patients. Improving communication between healthcare sectors, departments, and programs might ultimately help to enhance the effects of programs like these, which are important promising approaches to continuing care.
Though this study cannot speak to the direct causal effects of this continuing care intervention on retention, studies of similar interventions with other types of patients and treatment outcomes have revealed the benefits of programs like this one, including recovery management checkups, telemedicine- and telephone-based continuing care.
Small sample sizes limited interpretations about the effect of this pharmacist-led clinic program on re-hospitalization and emergency department visits at follow-up. Though trend level differences could be observed, the groups ultimately did not significantly differ. It also limited ability to evaluate sub-groups by intervention, substance use disorder (alcohol, opioid, or both), and medication treatment type.
The pharmacist’s role in the program was variable and patient outreach was on an as-needed basis, making it difficult to quantify the amount of patient exposure to the program and how this might impact outcomes. In addition, the number of intervention activities performed by the pharmacist appeared relatively minimal and it appears that some patients got more attention than others (range of activities per patient = 0 – 4), which could have influenced the overall effect of the program on retention in group analyses.
The control group had more clinical severity (i.e., higher prevalence of dual diagnosis of alcohol and opioid use disorder), hindering the ability to determine whether the intervention was responsible for better outcomes. The dose of extended-release naltrexone and buprenorphine received was not considered, and this deserves additional attention given the role of dose in retention.
BOTTOM LINE
This retrospective observational cohort study found that a pharmacist-led telephone clinic program may help to promote continued medication treatment for veterans with opioid and/or alcohol use disorders who initiate medication in inpatient VA psychiatric treatment and intend to continue after discharged. Such a program may be particularly beneficial for retaining patients in community-based extended-release naltrexone treatment but randomized controlled trials or rigorous quasi-experimental studies are needed to draw conclusions.
For individuals and families seeking recovery: Currently, programs that help individuals transition their medication treatment between different levels of substance use disorder care (e.g., inpatient to outpatient) are not widely available. However, the availability of programs like this are starting to grow. Individuals who are planning to start medication treatment for substance use disorder in one setting and continue it in another should ask their providers about options for a smooth transition without gaps in care.
For treatment professionals and treatment systems: Given the importance of continuity of care to help prevent relapse and recurrence of substance use disorder, particularly in the context of medication treatments for opioid and alcohol use disorders, healthcare professionals might consider developing programs that ensure patient support during care transitions. “Bridge” clinics that provide interim medication treatment for individuals without established providers may help to ensure treatment retention upon transition to various levels of care, which can ultimately enhance patient outcomes and reduce overdose death risk, particularly for individuals with opioid use disorder.
For scientists:Additional research is needed to replicate and extend these findings in various VA settings, and to identify the extent to which such programs are truly helpful with randomized controlled trials and well-designed quasi-experimental studies. Manualizing such interventions and testing them systematically will allow for a more comprehensive and clear understanding of the effects of transitional programs for medication treatment retention. Investigations that allow for the examination of interactions between group assignment, medication type and dose, disorder type, and patient’s level of exposure to program components will also help further our understanding of whether or not these programs are effective for enhancing retention in medication treatment after inpatient care.
For policy makers: Additional programmatic and research funding will help to develop and test programs intended to increase patient retention in empirically-supported medication treatments for opioid and alcohol use disorders. Developing useful programs that prevent gaps in medication treatment during transitions between various types of care (e.g., outpatient, inpatient, residential, etc.) can ultimately help to mitigate adverse events (including premature death) and address the clinical and patient burden of repeat treatment intakes due to relapse and recurrence of symptoms. It also has the potential to help reduce the number of alcohol deaths and opioid overdose deaths that occur due to a discontinuation of medication treatment.