
Can Recovery Support Calls From Volunteer Professionals Improve Adolescent Recovery Outcomes?
There is a general consensus among experts from a variety of addiction-related disciplines (e.g., neuroscience, clinical/psychotherapy, epidemiology) that substance use disorders (SUD) are often chronic conditions requiring ongoing maintenance of initial change processes via continuing care.
Research on post-treatment continuing care has provided encouraging, albeit somewhat mixed results, and far less is known about how to help adolescents maintain treatment gains.
Given limited economic resources available to treat substance use disorders (SUD), continuing care researchers are often also interested in the issue of cost containment.
In the current study, Garner et al. examined whether adolescents receiving continuing care in two cost-effective ways – via telephone, and delivered by volunteer pre-professionals – had better outcomes than a matched control group of adolescents. They also examined if any effects of continuing care were accounted for by intermediate changes (mechanisms) in environmental risk (e.g., less 12-step participation) and/or social risk (e.g., spending time with friends that use drugs).
Continuing care participants were 202 adolescents (ages 13-18 years old, mean = 16 years) who received outpatient or inpatient treatment at a Center for Substance Abuse Treatment-funded program, of which 26% were female, and regarding ethnicity, 56% were Caucasian, 23% Latino, 14% Mixed/Other, and 6% were African American. Notably, 80% had lifetime criminal justice involvement.
Using methodologically rigorous propensity score modeling, the authors selected a group of 404 adolescents (ages 13-18) from a larger pool of patients with demographic and baseline characteristics that were similar on aggregate to the intervention group.
All participants were required to have attended at least four outpatient sessions within approximately six weeks of intake or attended 2 weeks of residential treatment. Support call volunteers (n = 60) were 29 years old, on average, and the majority were female (72%) and Caucasian (82%). Half had at least some college education (and a third had a bachelor’s degree). Three-quarters did not report being in recovery. Support call volunteers were guided in their interactions with the adolescents by the Adolescent-Community Reinforcement Approach (ACRA) and Assertive Continuing Care (ACC), evidence-based behavioral interventions that emphasize communication and problem solving skills to engage in healthy and rewarding recovery activities. Calls occurred about weekly (with flexibility to modify frequency depending on adolescent functioning and preference) and lasted about 15 minutes.
Authors found that the continuing care group had decreased environmental risk at the 6-month follow-up, but did not report improved substance use or substance related problems.
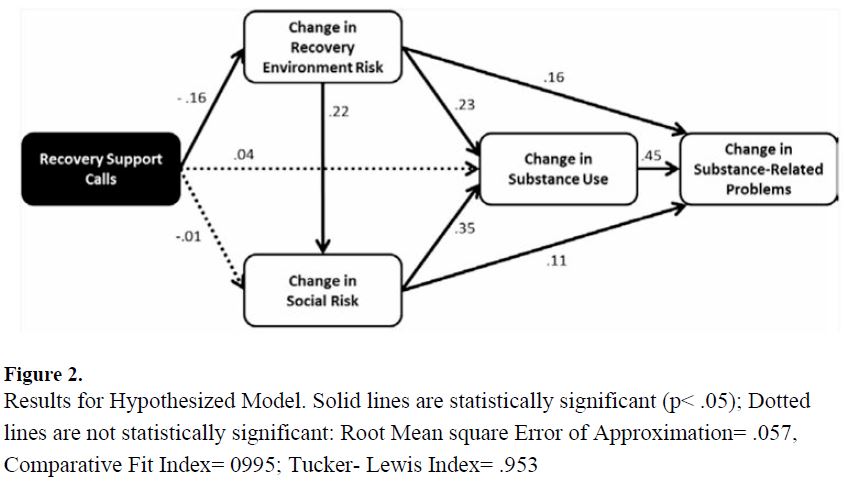
This effect on environmental risk was even more pronounced for adolescents with lower baseline motivation (measured as “treatment readiness”); see illustrative figure below. Results were similar for both males and females. Of note, 46% of the calls were completed as scheduled.
IN CONTEXT
The current study offered both encouraging and discouraging news.
Telephone-based continuing care for adolescents may lead to increased activities and environmental factors known to positively influence recovery rates (e.g., 12-step participation and reduced drinking/drug use in the home). However, at least in this case, the recovery calls were not sufficient to ultimately influence substance use outcomes in a meaningful way.
Adolescents engaged in only 46% of scheduled calls. While authors point out this level of adherence is quite favorable relative to other telephone-based continuing care studies, that degree of engagement may not be an adequate continuing care ‘dose’.
This study was particularly innovative in its use of pre-professional volunteers, reducing the health care costs needed to deliver the recovery support intervention. It remains unclear whether the use of professionals explicitly trained in ACRA and ACC might have led to more favorable outcomes.
BOTTOM LINE
- For individuals & families seeking recovery: Treatment services work differently for different people. For adolescents, participation in post-treatment recovery support calls are unlikely to be harmful, and could be beneficial, as part of continuing care after treatment.
- For scientists: It is unclear why the authors’ mediational model was generally supported, yet they did not find a direct effect of recovery support calls on substance use outcomes. That said, these results are sufficiently encouraging – and the public health significance of adolescent continuing care a great enough need – to warrant a randomized controlled trial of phone-based continuing care. If possible, including two arms of the treatment where one is delivered by professionals and the other by pre-professionals might help elucidate whether professionals could deliver a more potent version of the intervention.
- For policy makers: Policies are needed to provide resources for adolescents’ ongoing engagement in care after they are discharged from SUD treatment. Future research can examine whether less-expensive pre-professionals might be as effective in delivering continuing care interventions as trained professionals.
- For treatment professionals and treatment systems: Consider innovative ways to engage adolescent patients in continuing care after they are discharged from treatment, including recovery support calls grounded in evidence-based therapy approaches, such as the ACRA and ACC.
CITATIONS
Garner, B. R., Godley, M. D., Passetti, L. L., Funk, R. R., & White, W. L. (2014). Recovery Support for Adolescents with Substance use Disorders: The Impact of Recovery Support Telephone Calls Provided by Pre-Professional Volunteers. Journal of substance abuse and alcoholism, 2(2), 1010.
