Trauma and emotion regulation effects on cocaine use and depression in treatment-seeking adults
Emotion regulation difficulties and experiencing trauma add complications in addiction treatment. To help inform treatment approaches for individuals with cocaine use disorder, this study examined how trauma experiences and emotion regulation were associated with cocaine use and depressive symptoms.
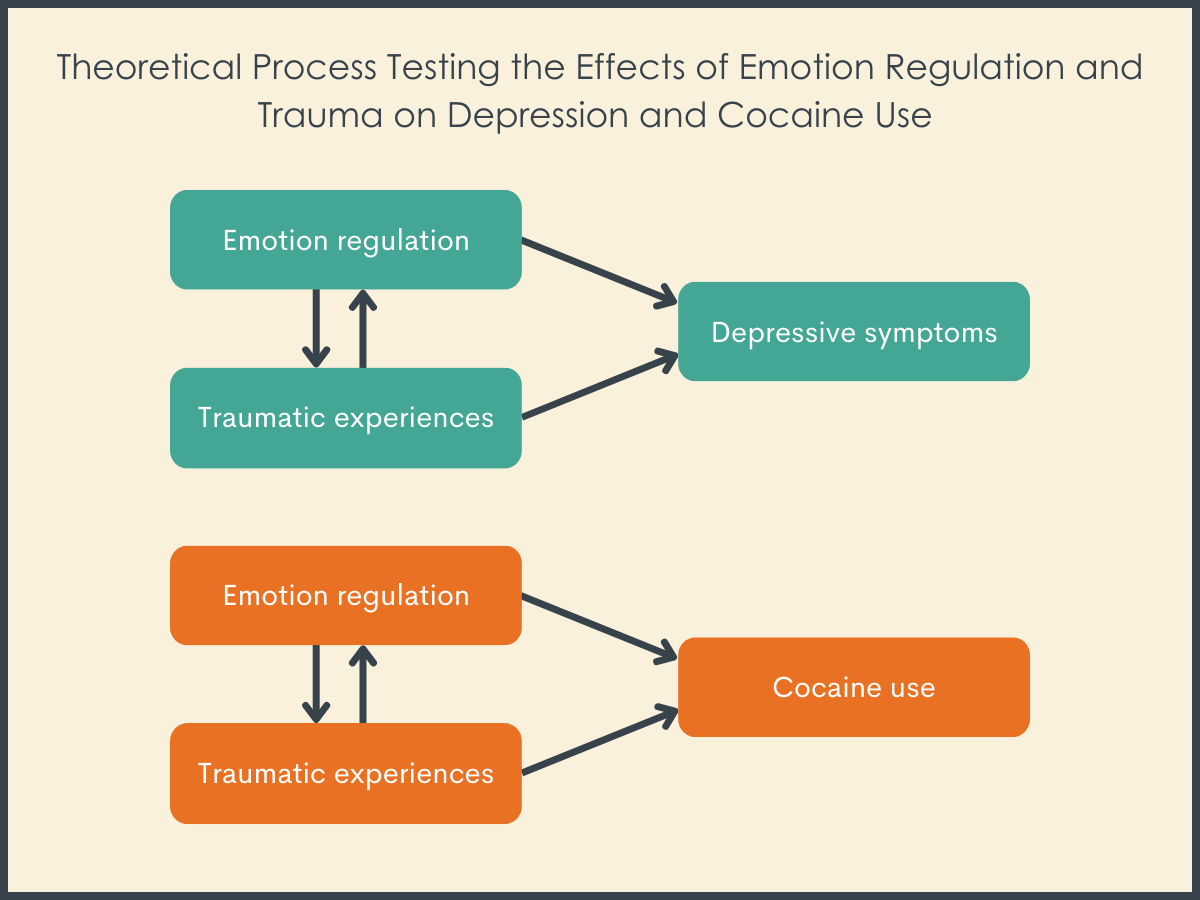
There is also evidence that these factors interact to influence behavior. Problems with emotion regulation have been found to impact depressive symptoms among trauma-exposed people. Additional evidence suggests that depressive symptoms may mediate – or explain – the relationship between emotion regulation and experiencing trauma among people who currently use cocaine. This together suggests that experiencing trauma, emotion regulation difficulties, and depression, may all work in combination to influence cocaine use.
The current research investigated how difficulties with emotion regulation and trauma experiences both individually and interactively impacted depressive symptoms and cocaine use.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional observational study. Participants in the study (N=135) were treatment-seeking adults living in a large Southern US metropolitan area. Participants were recruited via community-based and online advertising strategies (e.g., newspaper ads, Craigslist) – that is, while recruited from the community, the study targeted those seeking treatment specifically for cocaine use disorder.
Participants were included in the study if they were 1) between 18 and 65 years old, 2) proficient in English, 3) and met criteria for current (i.e., past month) cocaine dependence based on DSM-IV. Participants were excluded from the participating if they a) endorsed current dependence on a substance other than cocaine (except nicotine) for which withdrawal symptoms were a concern (e.g., alcohol), b) had a current or past history of bipolar I disorder, schizophrenia, or any psychotic symptoms in the 6 months prior to screening, c) had a major unstable medical condition(s), d) active suicidal ideation in the 4 weeks prior to screening, d) used any medication which made participation in the study unsafe (e.g., psychotropics), and/or e) were pregnant or nursing at the time of screening.
The primary outcome of this research was cocaine use, which was measured in 2 ways. An objective urine drug screening (via Reditest 6 Cassette tests) measured cocaine use within 96 hours prior to participating in the study. Additionally, the Addiction Severity Index-Lite was used to gather self-report data on past month cocaine use. The study examined both number of days of cocaine use, a continuous outcome, and any cocaine use on the drug screen, a binary outcome. To examine how cocaine use was impacted by emotion regulation, trauma experiences, and depression these factors were operationalized using standardized measures. Problems with emotion regulation was measured using the Difficulties in Emotion Regulation Scale. This 36-item self-report scale is summed across measures resulting in a score from 36 (almost never experienced any problems regulating emotions) to 180 (experienced problems regulating emotions in almost every situation). Experiences of trauma was measured via the Life Events Checklist for the DSM-5. This self-report questionnaire asks participants to indicate if they experienced or witnessed each of 16 potentially traumatic experiences (e.g., sexual assault) during their lifetime. The number of endorsed events were summed together. Depression was operationalized as scores via the Beck Depression Inventory-II. This measure consists of 21 scale items (ranging from 0–3; with a max score of 63) to assess the severity of depressive symptoms in the past fortnight.
The researchers used statistical modeling to determine associations between emotion regulation, trauma experiences, depression, and cocaine use. Multiple regression analyses were run with depressive symptom scores and number of self-reported cocaine use days in the last month. Variables for emotion regulation and trauma experience were examined in separate blocks to determine how much of the unique variance they each account for in depression and cocaine use. These models adjusted for demographic variables (e.g., age and gender) known to be associated with depression and cocaine use. The researchers also controlled for recent concurrent alcohol and other drug use (e.g., cannabis) which are also associated with cocaine use, as well as total years of cocaine use.
Most participants for this study (N=135) identified as African American (n =100, 74.1%), followed by white/Caucasian (n = 16, 11.9%), then by Hispanic or Latino (n = 14, 10.4%), then Native American (n = 1, .7%), and the more than one race/ethnicity (n = 3, 2.2%). One person did not disclose their race/ethnicity (n = 1, .7%). Most participants had never been married (n =55, 40.7%), followed by divorced/separated (n = 51, 37.8%), married (n = 21, 15.6%), and widowed (n = 8, 5.9%). The vast majority of participants (86.7%) reported having completed ≥12 years of education. Around 43% of participants were not working at the time of participation. Nearly 60% of participants reported being treated for substance use ≥1 times during their life.
WHAT DID THIS STUDY FIND?
Gender was the strongest demographic correlate of cocaine use
Across multiple analyses, male gender was significantly associated with recent cocaine use. Age also significantly contributed to models, indicating that older participants were more likely to engage in recent cocaine use at time of participation.
Difficulties in emotion regulation and trauma experiences were associated with depressive symptoms
Measures of both difficulties in emotion regulation and trauma experiences were associated with worse depression for participants. However, emotion regulation and trauma experiences did not interact to influence reported depressive symptoms.
Difficulties in emotion regulation and trauma experiences were not associated with cocaine use
Neither emotion regulation nor trauma experiences had an impact on either self-reported cocaine use days or drug test verified binary cocaine use among participants. Furthermore, there was no evidence that the interaction of emotion regulation and trauma experiences were associated with either cocaine use outcome among this sample.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that emotion regulation and trauma experiences are associated with depressive symptoms, but not recent cocaine use, among cocaine-using adults. However, the mechanisms by which this occurs is unclear.
The researchers found that difficulties with emotion regulation and experiencing trauma were independently and strongly associated with more depressive symptoms. However, when the researchers examined how these factors interacted with each other they did not find evidence that emotion regulation interacted with a history of trauma experiences in amplifying and worsening depressive symptoms. The researchers also failed to find associations between emotion regulation and trauma experiences and cocaine use, both when measured using self-report (past 30 days) and urine toxicology screens.
These results suggest that targeting interventions to address problems with emotion regulation and/or trauma experiences may be useful in treating depression, but less so for treating cocaine use among individuals with cocaine use disorder, where other factors may be more important. This work implies that the mechanisms through which emotion regulation and trauma experiences are associated with substance use behavior remain unclear. Prior research suggests there is a link between trauma and substance use, but the pathways through which this association occurs may be indirect. It is possible that mere exposure to a traumatic event is not enough to predict substance use – other factors may better explain drug use. For example, other research suggests that the severity of traumatic experiences may be more predictive of cocaine use than the number of traumatic experiences among people. In a similar vein, difficulties with emotion regulation may impact substance use through a desire to self-medicate. That is, challenges with emotional regulation may lead people to seek out drugs to modulate their negative emotional state. Also, given the cross-sectional nature of this study, it is plausible as well that depression symptoms leads to emotion regulation challenges and not just the other way around; it could also be reciprocal where they influence each other. Future research examining these different hypotheses may help inform substance use prevention and treatment strategies.
Given the cross-sectional research design, the temporality of the relationship between emotion regulation, trauma experiences, depression, and cocaine use cannot be established. That is, it cannot be determined if cocaine use impacted emotion regulation/depression or vice versa. Evidence exists suggesting that early exposure to cocaine may lead issues with emotion regulation. This would mean the authors’ suggestion that intervening on emotion regulation to mitigate cocaine use may be moot.
The demographics of the sample may limit the generalizability of the results. For example, the sample consisted exclusively of adult cocaine users who were seeking drug use disorder treatment. It is unclear if those who were not seeking treatment would show score similarly on measures of emotion regulation, trauma experiences, and depression. Furthermore, the sample consisted mostly of Black African American identified participants. This may impact generalizability of these results since Black Americans experience more trauma yet also have fewer mood disorders than White Americans.
Restricting the primary outcome to cocaine use may have obscured potential relationships between trauma and emotion regulation with other substances. It is possible that these factors may be relevant for other drugs, but it is beyond these data to determine that. In addition, by examining cocaine use alone the researchers may have missed how trauma and emotion regulation may impact poly substance use (e.g., using alcohol and cocaine together, which is very common among adults who use cocaine).
BOTTOM LINE
Difficulties with emotion regulation and experiencing trauma may contribute to depressive symptoms in treatment-seeking cocaine using adults. On the other hand, problems with emotion regulation or experiencing trauma may contribute to cocaine use among this sample. These results suggest that interventions targeting emotion regulation and/or trauma may be a viable way to treat depression among cocaine using adults. Providers working with cocaine using adults may want to consider incorporating such interventions as part of a holistic care plan. Such interventions may not necessarily reduce substance use but may be useful in treating other mental health issues that are part of constellation of symptoms many substance use disorder patients experience. Given the cross-sectional study design here – longitudinal research that examines these associations among emotion regulation, trauma, and substance use over time can help inform substance use prevention and intervention strategies.
For individuals and families seeking recovery: This study did not find an association between trauma and cocaine use. Though it is possible that the consequences of certain traumatic experiences – but not others – may enhance risk for substance use.
For treatment professionals and treatment systems: The present study suggests that depressive symptoms are associated with emotion regulation and trauma experiences among cocaine-using adults. Therefore, it may be important for providers to recognize that those suffering from substance use disorder likely experience multiple mental health problems (e.g., depression) concurrent to their substance use disorder. If mental health treatment is not integrated within your treatment program or protocols, incorporating screening, brief intervention, and referral to treatment (SBIRT) practices may help providers determine what comorbid mental health problems experienced by their patients and offer appropriate referrals. Resources are available for providers to implement SBIRT some of which offer continuing education credit. In addition, new technologies may help automate some SBIRT procedures.
For scientists: The present study suggests that the relationship between emotion regulation, trauma experienced, depression and cocaine use is complex. The lack of understanding of exactly how these factors interact to influence cocaine use precludes the development of targeted interventions to reduce problematic drug use. To remedy this, scientists would do well to investigate this phenomenon. For example, longitudinal studies which determine how emotion regulation may become dysfunctional over the life course may elucidate how it may impact substance use behavior. Similarly, pinpointing the temporal ordering of varied trauma experiences and cocaine use could offer a better understanding of how trauma influences drugs use (and vice versa)..
For policy makers: The present study implies that emotion regulation and trauma experiences are associated with depression among cocaine using adults. One potential implication of this for policy makers is that there is a need to reduce barriers to mental health and substance use treatment (e.g., through Medicaid). This could include partnering with local foundations to channel funding where cocaine use is especially prevalent. In addition, it may be important for policy makers to devise ways of reducing the impact of trauma on vulnerable populations. That is, if experiencing trauma is a risk factor for mental health issues then reducing its impact may be beneficial in reducing said problems. Such efforts could take the form of outreach programs targeting youth. Providing support to young people may help buffer traumatic experiences and/or reduce exposure to future trauma.
There is also evidence that these factors interact to influence behavior. Problems with emotion regulation have been found to impact depressive symptoms among trauma-exposed people. Additional evidence suggests that depressive symptoms may mediate – or explain – the relationship between emotion regulation and experiencing trauma among people who currently use cocaine. This together suggests that experiencing trauma, emotion regulation difficulties, and depression, may all work in combination to influence cocaine use.
The current research investigated how difficulties with emotion regulation and trauma experiences both individually and interactively impacted depressive symptoms and cocaine use.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional observational study. Participants in the study (N=135) were treatment-seeking adults living in a large Southern US metropolitan area. Participants were recruited via community-based and online advertising strategies (e.g., newspaper ads, Craigslist) – that is, while recruited from the community, the study targeted those seeking treatment specifically for cocaine use disorder.
Participants were included in the study if they were 1) between 18 and 65 years old, 2) proficient in English, 3) and met criteria for current (i.e., past month) cocaine dependence based on DSM-IV. Participants were excluded from the participating if they a) endorsed current dependence on a substance other than cocaine (except nicotine) for which withdrawal symptoms were a concern (e.g., alcohol), b) had a current or past history of bipolar I disorder, schizophrenia, or any psychotic symptoms in the 6 months prior to screening, c) had a major unstable medical condition(s), d) active suicidal ideation in the 4 weeks prior to screening, d) used any medication which made participation in the study unsafe (e.g., psychotropics), and/or e) were pregnant or nursing at the time of screening.
The primary outcome of this research was cocaine use, which was measured in 2 ways. An objective urine drug screening (via Reditest 6 Cassette tests) measured cocaine use within 96 hours prior to participating in the study. Additionally, the Addiction Severity Index-Lite was used to gather self-report data on past month cocaine use. The study examined both number of days of cocaine use, a continuous outcome, and any cocaine use on the drug screen, a binary outcome. To examine how cocaine use was impacted by emotion regulation, trauma experiences, and depression these factors were operationalized using standardized measures. Problems with emotion regulation was measured using the Difficulties in Emotion Regulation Scale. This 36-item self-report scale is summed across measures resulting in a score from 36 (almost never experienced any problems regulating emotions) to 180 (experienced problems regulating emotions in almost every situation). Experiences of trauma was measured via the Life Events Checklist for the DSM-5. This self-report questionnaire asks participants to indicate if they experienced or witnessed each of 16 potentially traumatic experiences (e.g., sexual assault) during their lifetime. The number of endorsed events were summed together. Depression was operationalized as scores via the Beck Depression Inventory-II. This measure consists of 21 scale items (ranging from 0–3; with a max score of 63) to assess the severity of depressive symptoms in the past fortnight.
The researchers used statistical modeling to determine associations between emotion regulation, trauma experiences, depression, and cocaine use. Multiple regression analyses were run with depressive symptom scores and number of self-reported cocaine use days in the last month. Variables for emotion regulation and trauma experience were examined in separate blocks to determine how much of the unique variance they each account for in depression and cocaine use. These models adjusted for demographic variables (e.g., age and gender) known to be associated with depression and cocaine use. The researchers also controlled for recent concurrent alcohol and other drug use (e.g., cannabis) which are also associated with cocaine use, as well as total years of cocaine use.
Most participants for this study (N=135) identified as African American (n =100, 74.1%), followed by white/Caucasian (n = 16, 11.9%), then by Hispanic or Latino (n = 14, 10.4%), then Native American (n = 1, .7%), and the more than one race/ethnicity (n = 3, 2.2%). One person did not disclose their race/ethnicity (n = 1, .7%). Most participants had never been married (n =55, 40.7%), followed by divorced/separated (n = 51, 37.8%), married (n = 21, 15.6%), and widowed (n = 8, 5.9%). The vast majority of participants (86.7%) reported having completed ≥12 years of education. Around 43% of participants were not working at the time of participation. Nearly 60% of participants reported being treated for substance use ≥1 times during their life.
WHAT DID THIS STUDY FIND?
Gender was the strongest demographic correlate of cocaine use
Across multiple analyses, male gender was significantly associated with recent cocaine use. Age also significantly contributed to models, indicating that older participants were more likely to engage in recent cocaine use at time of participation.
Difficulties in emotion regulation and trauma experiences were associated with depressive symptoms
Measures of both difficulties in emotion regulation and trauma experiences were associated with worse depression for participants. However, emotion regulation and trauma experiences did not interact to influence reported depressive symptoms.
Difficulties in emotion regulation and trauma experiences were not associated with cocaine use
Neither emotion regulation nor trauma experiences had an impact on either self-reported cocaine use days or drug test verified binary cocaine use among participants. Furthermore, there was no evidence that the interaction of emotion regulation and trauma experiences were associated with either cocaine use outcome among this sample.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that emotion regulation and trauma experiences are associated with depressive symptoms, but not recent cocaine use, among cocaine-using adults. However, the mechanisms by which this occurs is unclear.
The researchers found that difficulties with emotion regulation and experiencing trauma were independently and strongly associated with more depressive symptoms. However, when the researchers examined how these factors interacted with each other they did not find evidence that emotion regulation interacted with a history of trauma experiences in amplifying and worsening depressive symptoms. The researchers also failed to find associations between emotion regulation and trauma experiences and cocaine use, both when measured using self-report (past 30 days) and urine toxicology screens.
These results suggest that targeting interventions to address problems with emotion regulation and/or trauma experiences may be useful in treating depression, but less so for treating cocaine use among individuals with cocaine use disorder, where other factors may be more important. This work implies that the mechanisms through which emotion regulation and trauma experiences are associated with substance use behavior remain unclear. Prior research suggests there is a link between trauma and substance use, but the pathways through which this association occurs may be indirect. It is possible that mere exposure to a traumatic event is not enough to predict substance use – other factors may better explain drug use. For example, other research suggests that the severity of traumatic experiences may be more predictive of cocaine use than the number of traumatic experiences among people. In a similar vein, difficulties with emotion regulation may impact substance use through a desire to self-medicate. That is, challenges with emotional regulation may lead people to seek out drugs to modulate their negative emotional state. Also, given the cross-sectional nature of this study, it is plausible as well that depression symptoms leads to emotion regulation challenges and not just the other way around; it could also be reciprocal where they influence each other. Future research examining these different hypotheses may help inform substance use prevention and treatment strategies.
Given the cross-sectional research design, the temporality of the relationship between emotion regulation, trauma experiences, depression, and cocaine use cannot be established. That is, it cannot be determined if cocaine use impacted emotion regulation/depression or vice versa. Evidence exists suggesting that early exposure to cocaine may lead issues with emotion regulation. This would mean the authors’ suggestion that intervening on emotion regulation to mitigate cocaine use may be moot.
The demographics of the sample may limit the generalizability of the results. For example, the sample consisted exclusively of adult cocaine users who were seeking drug use disorder treatment. It is unclear if those who were not seeking treatment would show score similarly on measures of emotion regulation, trauma experiences, and depression. Furthermore, the sample consisted mostly of Black African American identified participants. This may impact generalizability of these results since Black Americans experience more trauma yet also have fewer mood disorders than White Americans.
Restricting the primary outcome to cocaine use may have obscured potential relationships between trauma and emotion regulation with other substances. It is possible that these factors may be relevant for other drugs, but it is beyond these data to determine that. In addition, by examining cocaine use alone the researchers may have missed how trauma and emotion regulation may impact poly substance use (e.g., using alcohol and cocaine together, which is very common among adults who use cocaine).
BOTTOM LINE
Difficulties with emotion regulation and experiencing trauma may contribute to depressive symptoms in treatment-seeking cocaine using adults. On the other hand, problems with emotion regulation or experiencing trauma may contribute to cocaine use among this sample. These results suggest that interventions targeting emotion regulation and/or trauma may be a viable way to treat depression among cocaine using adults. Providers working with cocaine using adults may want to consider incorporating such interventions as part of a holistic care plan. Such interventions may not necessarily reduce substance use but may be useful in treating other mental health issues that are part of constellation of symptoms many substance use disorder patients experience. Given the cross-sectional study design here – longitudinal research that examines these associations among emotion regulation, trauma, and substance use over time can help inform substance use prevention and intervention strategies.
For individuals and families seeking recovery: This study did not find an association between trauma and cocaine use. Though it is possible that the consequences of certain traumatic experiences – but not others – may enhance risk for substance use.
For treatment professionals and treatment systems: The present study suggests that depressive symptoms are associated with emotion regulation and trauma experiences among cocaine-using adults. Therefore, it may be important for providers to recognize that those suffering from substance use disorder likely experience multiple mental health problems (e.g., depression) concurrent to their substance use disorder. If mental health treatment is not integrated within your treatment program or protocols, incorporating screening, brief intervention, and referral to treatment (SBIRT) practices may help providers determine what comorbid mental health problems experienced by their patients and offer appropriate referrals. Resources are available for providers to implement SBIRT some of which offer continuing education credit. In addition, new technologies may help automate some SBIRT procedures.
For scientists: The present study suggests that the relationship between emotion regulation, trauma experienced, depression and cocaine use is complex. The lack of understanding of exactly how these factors interact to influence cocaine use precludes the development of targeted interventions to reduce problematic drug use. To remedy this, scientists would do well to investigate this phenomenon. For example, longitudinal studies which determine how emotion regulation may become dysfunctional over the life course may elucidate how it may impact substance use behavior. Similarly, pinpointing the temporal ordering of varied trauma experiences and cocaine use could offer a better understanding of how trauma influences drugs use (and vice versa)..
For policy makers: The present study implies that emotion regulation and trauma experiences are associated with depression among cocaine using adults. One potential implication of this for policy makers is that there is a need to reduce barriers to mental health and substance use treatment (e.g., through Medicaid). This could include partnering with local foundations to channel funding where cocaine use is especially prevalent. In addition, it may be important for policy makers to devise ways of reducing the impact of trauma on vulnerable populations. That is, if experiencing trauma is a risk factor for mental health issues then reducing its impact may be beneficial in reducing said problems. Such efforts could take the form of outreach programs targeting youth. Providing support to young people may help buffer traumatic experiences and/or reduce exposure to future trauma.
There is also evidence that these factors interact to influence behavior. Problems with emotion regulation have been found to impact depressive symptoms among trauma-exposed people. Additional evidence suggests that depressive symptoms may mediate – or explain – the relationship between emotion regulation and experiencing trauma among people who currently use cocaine. This together suggests that experiencing trauma, emotion regulation difficulties, and depression, may all work in combination to influence cocaine use.
The current research investigated how difficulties with emotion regulation and trauma experiences both individually and interactively impacted depressive symptoms and cocaine use.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional observational study. Participants in the study (N=135) were treatment-seeking adults living in a large Southern US metropolitan area. Participants were recruited via community-based and online advertising strategies (e.g., newspaper ads, Craigslist) – that is, while recruited from the community, the study targeted those seeking treatment specifically for cocaine use disorder.
Participants were included in the study if they were 1) between 18 and 65 years old, 2) proficient in English, 3) and met criteria for current (i.e., past month) cocaine dependence based on DSM-IV. Participants were excluded from the participating if they a) endorsed current dependence on a substance other than cocaine (except nicotine) for which withdrawal symptoms were a concern (e.g., alcohol), b) had a current or past history of bipolar I disorder, schizophrenia, or any psychotic symptoms in the 6 months prior to screening, c) had a major unstable medical condition(s), d) active suicidal ideation in the 4 weeks prior to screening, d) used any medication which made participation in the study unsafe (e.g., psychotropics), and/or e) were pregnant or nursing at the time of screening.
The primary outcome of this research was cocaine use, which was measured in 2 ways. An objective urine drug screening (via Reditest 6 Cassette tests) measured cocaine use within 96 hours prior to participating in the study. Additionally, the Addiction Severity Index-Lite was used to gather self-report data on past month cocaine use. The study examined both number of days of cocaine use, a continuous outcome, and any cocaine use on the drug screen, a binary outcome. To examine how cocaine use was impacted by emotion regulation, trauma experiences, and depression these factors were operationalized using standardized measures. Problems with emotion regulation was measured using the Difficulties in Emotion Regulation Scale. This 36-item self-report scale is summed across measures resulting in a score from 36 (almost never experienced any problems regulating emotions) to 180 (experienced problems regulating emotions in almost every situation). Experiences of trauma was measured via the Life Events Checklist for the DSM-5. This self-report questionnaire asks participants to indicate if they experienced or witnessed each of 16 potentially traumatic experiences (e.g., sexual assault) during their lifetime. The number of endorsed events were summed together. Depression was operationalized as scores via the Beck Depression Inventory-II. This measure consists of 21 scale items (ranging from 0–3; with a max score of 63) to assess the severity of depressive symptoms in the past fortnight.
The researchers used statistical modeling to determine associations between emotion regulation, trauma experiences, depression, and cocaine use. Multiple regression analyses were run with depressive symptom scores and number of self-reported cocaine use days in the last month. Variables for emotion regulation and trauma experience were examined in separate blocks to determine how much of the unique variance they each account for in depression and cocaine use. These models adjusted for demographic variables (e.g., age and gender) known to be associated with depression and cocaine use. The researchers also controlled for recent concurrent alcohol and other drug use (e.g., cannabis) which are also associated with cocaine use, as well as total years of cocaine use.
Most participants for this study (N=135) identified as African American (n =100, 74.1%), followed by white/Caucasian (n = 16, 11.9%), then by Hispanic or Latino (n = 14, 10.4%), then Native American (n = 1, .7%), and the more than one race/ethnicity (n = 3, 2.2%). One person did not disclose their race/ethnicity (n = 1, .7%). Most participants had never been married (n =55, 40.7%), followed by divorced/separated (n = 51, 37.8%), married (n = 21, 15.6%), and widowed (n = 8, 5.9%). The vast majority of participants (86.7%) reported having completed ≥12 years of education. Around 43% of participants were not working at the time of participation. Nearly 60% of participants reported being treated for substance use ≥1 times during their life.
WHAT DID THIS STUDY FIND?
Gender was the strongest demographic correlate of cocaine use
Across multiple analyses, male gender was significantly associated with recent cocaine use. Age also significantly contributed to models, indicating that older participants were more likely to engage in recent cocaine use at time of participation.
Difficulties in emotion regulation and trauma experiences were associated with depressive symptoms
Measures of both difficulties in emotion regulation and trauma experiences were associated with worse depression for participants. However, emotion regulation and trauma experiences did not interact to influence reported depressive symptoms.
Difficulties in emotion regulation and trauma experiences were not associated with cocaine use
Neither emotion regulation nor trauma experiences had an impact on either self-reported cocaine use days or drug test verified binary cocaine use among participants. Furthermore, there was no evidence that the interaction of emotion regulation and trauma experiences were associated with either cocaine use outcome among this sample.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that emotion regulation and trauma experiences are associated with depressive symptoms, but not recent cocaine use, among cocaine-using adults. However, the mechanisms by which this occurs is unclear.
The researchers found that difficulties with emotion regulation and experiencing trauma were independently and strongly associated with more depressive symptoms. However, when the researchers examined how these factors interacted with each other they did not find evidence that emotion regulation interacted with a history of trauma experiences in amplifying and worsening depressive symptoms. The researchers also failed to find associations between emotion regulation and trauma experiences and cocaine use, both when measured using self-report (past 30 days) and urine toxicology screens.
These results suggest that targeting interventions to address problems with emotion regulation and/or trauma experiences may be useful in treating depression, but less so for treating cocaine use among individuals with cocaine use disorder, where other factors may be more important. This work implies that the mechanisms through which emotion regulation and trauma experiences are associated with substance use behavior remain unclear. Prior research suggests there is a link between trauma and substance use, but the pathways through which this association occurs may be indirect. It is possible that mere exposure to a traumatic event is not enough to predict substance use – other factors may better explain drug use. For example, other research suggests that the severity of traumatic experiences may be more predictive of cocaine use than the number of traumatic experiences among people. In a similar vein, difficulties with emotion regulation may impact substance use through a desire to self-medicate. That is, challenges with emotional regulation may lead people to seek out drugs to modulate their negative emotional state. Also, given the cross-sectional nature of this study, it is plausible as well that depression symptoms leads to emotion regulation challenges and not just the other way around; it could also be reciprocal where they influence each other. Future research examining these different hypotheses may help inform substance use prevention and treatment strategies.
Given the cross-sectional research design, the temporality of the relationship between emotion regulation, trauma experiences, depression, and cocaine use cannot be established. That is, it cannot be determined if cocaine use impacted emotion regulation/depression or vice versa. Evidence exists suggesting that early exposure to cocaine may lead issues with emotion regulation. This would mean the authors’ suggestion that intervening on emotion regulation to mitigate cocaine use may be moot.
The demographics of the sample may limit the generalizability of the results. For example, the sample consisted exclusively of adult cocaine users who were seeking drug use disorder treatment. It is unclear if those who were not seeking treatment would show score similarly on measures of emotion regulation, trauma experiences, and depression. Furthermore, the sample consisted mostly of Black African American identified participants. This may impact generalizability of these results since Black Americans experience more trauma yet also have fewer mood disorders than White Americans.
Restricting the primary outcome to cocaine use may have obscured potential relationships between trauma and emotion regulation with other substances. It is possible that these factors may be relevant for other drugs, but it is beyond these data to determine that. In addition, by examining cocaine use alone the researchers may have missed how trauma and emotion regulation may impact poly substance use (e.g., using alcohol and cocaine together, which is very common among adults who use cocaine).
BOTTOM LINE
Difficulties with emotion regulation and experiencing trauma may contribute to depressive symptoms in treatment-seeking cocaine using adults. On the other hand, problems with emotion regulation or experiencing trauma may contribute to cocaine use among this sample. These results suggest that interventions targeting emotion regulation and/or trauma may be a viable way to treat depression among cocaine using adults. Providers working with cocaine using adults may want to consider incorporating such interventions as part of a holistic care plan. Such interventions may not necessarily reduce substance use but may be useful in treating other mental health issues that are part of constellation of symptoms many substance use disorder patients experience. Given the cross-sectional study design here – longitudinal research that examines these associations among emotion regulation, trauma, and substance use over time can help inform substance use prevention and intervention strategies.
For individuals and families seeking recovery: This study did not find an association between trauma and cocaine use. Though it is possible that the consequences of certain traumatic experiences – but not others – may enhance risk for substance use.
For treatment professionals and treatment systems: The present study suggests that depressive symptoms are associated with emotion regulation and trauma experiences among cocaine-using adults. Therefore, it may be important for providers to recognize that those suffering from substance use disorder likely experience multiple mental health problems (e.g., depression) concurrent to their substance use disorder. If mental health treatment is not integrated within your treatment program or protocols, incorporating screening, brief intervention, and referral to treatment (SBIRT) practices may help providers determine what comorbid mental health problems experienced by their patients and offer appropriate referrals. Resources are available for providers to implement SBIRT some of which offer continuing education credit. In addition, new technologies may help automate some SBIRT procedures.
For scientists: The present study suggests that the relationship between emotion regulation, trauma experienced, depression and cocaine use is complex. The lack of understanding of exactly how these factors interact to influence cocaine use precludes the development of targeted interventions to reduce problematic drug use. To remedy this, scientists would do well to investigate this phenomenon. For example, longitudinal studies which determine how emotion regulation may become dysfunctional over the life course may elucidate how it may impact substance use behavior. Similarly, pinpointing the temporal ordering of varied trauma experiences and cocaine use could offer a better understanding of how trauma influences drugs use (and vice versa)..
For policy makers: The present study implies that emotion regulation and trauma experiences are associated with depression among cocaine using adults. One potential implication of this for policy makers is that there is a need to reduce barriers to mental health and substance use treatment (e.g., through Medicaid). This could include partnering with local foundations to channel funding where cocaine use is especially prevalent. In addition, it may be important for policy makers to devise ways of reducing the impact of trauma on vulnerable populations. That is, if experiencing trauma is a risk factor for mental health issues then reducing its impact may be beneficial in reducing said problems. Such efforts could take the form of outreach programs targeting youth. Providing support to young people may help buffer traumatic experiences and/or reduce exposure to future trauma.