
The Influence of Life Events on Recovery from Alcohol Use Disorder
It is well known that social factors can be critical to the initiation and maintenance of recovery.
Is this still the case if someone has a strong family history of alcohol use disorder, where their genetics might override any positive (or negative) social influence?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Dozens of studies show that for individuals with substance use disorders, social context has a substantial influence on the chances of initiating and sustaining recovery. For example, the extent to which someone increases the number of people in their social circle who support his/her recovery or are in recovery themselves, can create a foundation for several helpful recovery processes (e.g., social support seeking) and better recovery outcomes.
The question remains, though, whether one’s social environment matters – and to what extent it matters – if the person has a strong family history of substance use disorder. In this case, it could be that someone’s genetic predisposition, for example, plays a much larger role in whether or not they can initiate and sustain recovery, and social context becomes less important.
This study by McCutcheon and colleagues investigated that very question. They sought to uncover whether a series of social factors and treatment services still predict whether or not alcohol use disorder would remit for those with a strong family history of the disorder.
HOW WAS THIS STUDY CONDUCTED?
Authors used data from the Collaborative Study on the Genetics of Alcoholism. This initial multi-site study recruited individuals that met criteria for alcohol dependence beginning in 1989 from substance use disorder treatment. In the current study, authors analyzed data from 686 relatives of these initial recruits who also met criteria for alcohol use disorder based on Diagnostic and Statistical Manual of Mental Disorders, Version 5. As such, the individuals could be assumed to have a positive family history, and perhaps strong genetic loading for alcohol use disorder.
The participants were 80% White, 13% Black, and 5% Hispanic; 86% of them were first degree relatives of the initial recruits (i.e., father, mother, sibling, or offspring).
The primary analyses tested how influential social factors and treatment/recovery support services were in uniquely predicting whether or not the individuals were in remission 5 years later, over and above the effect of each other factor as well as demographic characteristics. Authors attempted, as best they could, to establish a causal relationship between the social factors and alcohol use disorder remission, despite not knowing if the social factors occurred before the onset of remission (see “What are the limitations of the study?” for more on this). Moreover, authors were interested in whether there were different patterns for different types of remission.
Therefore, they investigated changes in social factors and treatment service utilization between baseline and 5-years for four groups:
- Abstinent remission (no alcohol use disorder symptoms and alcohol abstinence)
- Low-risk remission (no alcohol use disorder symptoms and drinking 4 or fewer drinks per day and 13 or fewer per week for men, and 3 or fewer per day and 6 or fewer per week for women)
- High-risk drinkers (drinking outside the low-risk limits mentioned above; authors did not consider these individuals as being in remission despite not meeting any alcohol use disorder criteria)
- Continued alcohol use disorder (1+ symptom within a year of the 5-year follow-up; i.e., not in remission)
In each of these cases the remission outcome pertained to the year before the 5-year follow-up assessment. Authors also investigated differences in remission group by alcohol use disorder severity. In the DSM-5, having 2-3 alcohol (or other drug) use disorder symptoms is considered a “mild” disorder, 4-5 symptoms “moderate”, and 6-11 “severe”. Treatment and recovery support services examined were changes in professional treatment and Alcoholics Anonymous (AA) attendance.
Social factors examined were:
- changes in marital status
- having children
- religious attendance
- employment
- overall level of family and friend support (high versus low)
They also specifically examined whether the effects of marital status and having had a child were different for men and women.
WHAT DID THIS STUDY FIND?
Overall, 31% of participants were in remission at the 5-year follow-up: 9% were in abstinent remission and 22% were in low-risk drinking remission. Also of note, 6% were in the high-risk drinking group and 63% still had alcohol use disorder (i.e., not in remission).
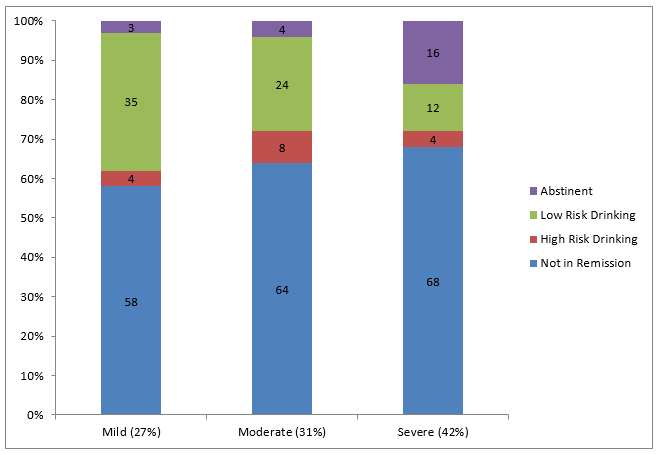
Adapted from McCutcheon et al. (2016).
Those with severe alcohol use disorder were more likely to be in abstinent, rather than low-risk drinking, remission, while those with mild and moderate alcohol use disorder were more likely to be in low-risk drinking, rather than abstinent, remission. It is also worth mentioning that the older the participant, the more likely he/she was in abstinent remission; the youngest individuals were more likely to be high-risk drinkers or continued to be diagnosed with alcohol use disorder.
Abstinent women had a greater likelihood of stable separation or divorce for women, a new marriage, high friend support, stable AA attendance, and stable professional treatment. Abstinent women were less likely to have had a first child.
Low-risk drinking women, compared to those with alcohol use disorder, were more likely to have had a first child for women.
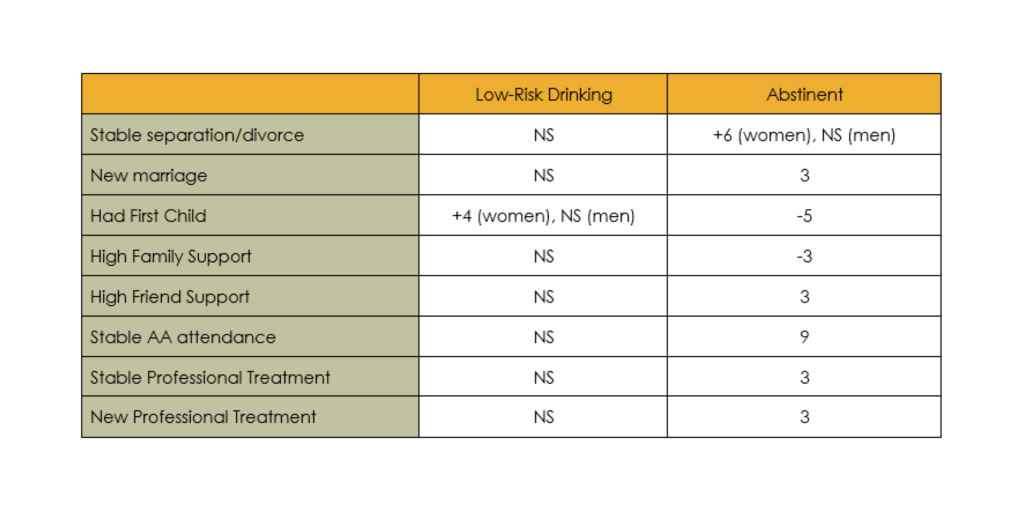
Likelihood of presence or absence of social factors and treatment/recovery support service utilization from baseline to 5-year follow-up by type of alcohol use disorder remission at 5-year follow-up, in comparison to no remission (i.e., persisting alcohol use disorder). Greater likelihood represented by “+”, and lower likelihood by “-“. Factors that were not significantly related to remission are denoted with “NS” for not significant.
Not shown in the table, both groups of individuals in remission had shorter alcohol use disorder “careers” (years living with alcohol use disorder) and were less likely to have used other drugs apart from alcohol in the past year compared to the continued alcohol use disorder group.
WHY IS THIS STUDY IMPORTANT?
In this study, individuals in remission from severe alcohol use disorder were more likely to choose abstinence. It is possible that these individuals chose the safest pathway to recovery due to greater consequences, and perhaps, a history of unsuccessful efforts to change by cutting back.
In a large study of a demographically and geographically representative group of individuals, Dawson and colleagues showed that for individuals with what used to be called alcohol dependence (now moderate or severe alcohol use disorder), those in abstinent remission were four times as likely to still be in remission 3 years later than those in remission but drinking at lower-risk levels, and seven times more likely than those drinking at higher-risk levels.
Social factors that predicted remission in women were stable separation/divorce and having had a first child.
Studies comparing recovery processes among men and women commonly find differences. In one example, in a study of AA recovery processes, men were more likely to benefit through increased self-efficacy to handle risky social situations whereas women were more likely to benefit through increased self-efficacy to handle difficult feelings. These gender differences in the initiation and maintenance of substance use disorder recovery can inform how clinical and recovery support services address similar and unique needs of each group of individuals.
The primary take-home message of the study is the strong potential role that social factors play in alcohol use disorder remission, even for those who have first degree relatives with substance use disorder.
In fact, in a related study by the research group that conducted this study, they found that environmental factors overall play a substantially larger role in remission than do genetics, for both females and males. That said, far fewer social factors, as well as treatment and recovery support service utilization variables, were predictors of remission for those who were in the low-risk drinking remission group versus the abstinent remission group. Interestingly, also, social factors could work in opposite directions depending on the type of remission.
Having a child was predictive of remission for the low-risk drinking remission group, though not having had a child was predictive of remission for the abstinent remission group. While the reason for these opposite effects is not entirely clear, they illustrate the complex nature of social context in alcohol use disorder remission. It is possible, for example, that birth of a first child can be stressful or spark a major change in priorities. Both increased stress as well as the declining priority of recovery activities (e.g., AA attendance) could be risk factors for relapse.
On the other hand, birth of a child could be protective for those who are drinking at lower-risk levels, sparking enhanced motivation to maintain an overall healthy lifestyle and perhaps garnering positive social support in general from family and friends. Also, because the protective effect of having a child was present only for women in low-risk drinking remission, it could be that they substantially decreased or abstained from alcohol during their pregnancy, which sparked a more lasting change even after they gave birth.
Whatever the case, given that these two remission pathways (low-risk drinking versus abstinence) may very well constitute distinct approaches to alcohol-related behavior change, their similarities and differences are worthy of ongoing investigation.
- LIMITATIONS
-
- The most important limitation of this study is that authors could not tease apart whether the change in social factor (e.g., marriage) came before the onset of remission in time. In other words, temporal precedence could not be established, so the associations between these social factors and alcohol use disorder remission should be treated as being related to one another more generally, rather than the social changes having caused or contributed to remission.
NEXT STEPS
Remission here was only measured in the past year, referred to as sustained remission. Given that the risk for relapse (i.e., return to drinking that leads to re-initiation of alcohol use disorder) remains elevated for 5 years, on average, one important next step would be to examine how well these different forms of remission are sustained over time (i.e., beyond 1 year), and the influence of social and recovery management on “long-term” remission.
BOTTOM LINE
- For individuals & families seeking recovery: There are many life decisions that can affect whether remission is initiated and sustained for individuals with alcohol use disorder. These include, but are certainly not limited to, participation in treatment and other recovery support services like Alcoholics Anonymous. It is recommended that you explore the various social factors in your life, such as romantic relationships, support from friends and family (both support for abstinence and drinking), and decisions to have a child, and how these might affect your chances of making a change in your drinking and other drug use.
- For Scientists: This longitudinal, cohort study of more than 600 individuals with alcohol use disorder that also had a strong family history of alcohol problems highlighted associations between social and service utilization factors and likelihood of remission. Given that different social factors predicted remission depending on the type of remission (abstinent vs. low-risk drinking), future research may investigate similarities and differences between what may be distinct remission pathways.
- For Policy makers: This study examined social and treatment/recovery factors that predict remission among individuals with alcohol use disorder that also have a strong family history of the disorder. Although policies may not necessarily be able to influence social factors identified with remission, both treatment and AA participation predicted abstinent remission versus continued alcohol use disorder. Also different factors were predictive of different forms of remission – abstinent versus low-risk drinking. Consider ongoing funding for research to investigate similarities and differences between these two forms of remission, as well their effects on individuals’ functioning and quality of life.
- For Treatment professionals and treatment systems: It is recommended that treatment providers continue to help patients explore the various social factors in their lives, such as romantic relationships, support from friends and family, and decisions to have a child, and how these might affect their chance of initiating and sustaining remission.
CITATIONS
McCutcheon, V. V., Kramer, J. R., Edenberg, H. J., Nurnberger, J. I., Kuperman, S., Schuckit, M. A., Bucholz, K. K. (2014). Social contexts of remission from DSM-5 alcohol use disorder in a high-risk sample. Alcohol Clin Exp Res, 38(7), 2015-2023. doi: 10.1111/acer.12434
