Can a mindfulness intervention help people quit smoking while also reducing harmful drinking?
Binge drinking and tobacco use both independently pose serious health risks, but in combination they can be particularly harmful. Heavy alcohol use can also interfere with smoking cessation attempts. In this study, researchers compared a mindfulness-based intervention to standard Cognitive Behavioral Therapy (CBT) to help adult smokers who binge drink to quit smoking and reduce their drinking.
Binge drinking and tobacco use both pose serious health risks, increasing the chance of disease as well as premature death, and together they have additive harmful effects. Additionally, alcohol use—especially binge drinking—can undermine people’s efforts to quit smoking, making this behavioral combination especially problematic.
Mindfulness Based Relapse Prevention is an 8-week intervention developed to treat substance use disorder that has also been used to support smoking cessation. Previous clinical trials have produced promising results suggesting this intervention can prevent substance use disorder relapse as well as standard relapse prevention approaches, and also help individuals quit smoking. Mechanism studies have shown that mindfulness might support addiction recovery and smoking cessation by reducing negative affect like stress and anxiety and disrupting the link between negative affect and craving.
Previous clinical trials have suggested mindfulness-based interventions might support smoking cessation while also reducing high-risk drinking behaviors in individuals engaging in high-risk drinking, but not yet experiencing alcohol addiction (i.e., severe alcohol use disorder). In this study, the researchers compared Mindfulness Based Relapse Prevention with minor modifications to also address nicotine cravings, to standard Cognitive Behavioral Therapy (CBT) in a sample of smokers who endorsed regular binge drinking, who were motivated to quit smoking and reduce their alcohol intake. Due to the COVID-19, the study was conducted remotely.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized trial with 67 adults who reported binge drinking and were motivated to both quit smoking and reduce their alcohol use. Participants received either 8 sessions of Mindfulness Based Relapse Prevention or CBT. Both interventions were delivered over Zoom consistent with COVID-19 physical distancing guidelines.
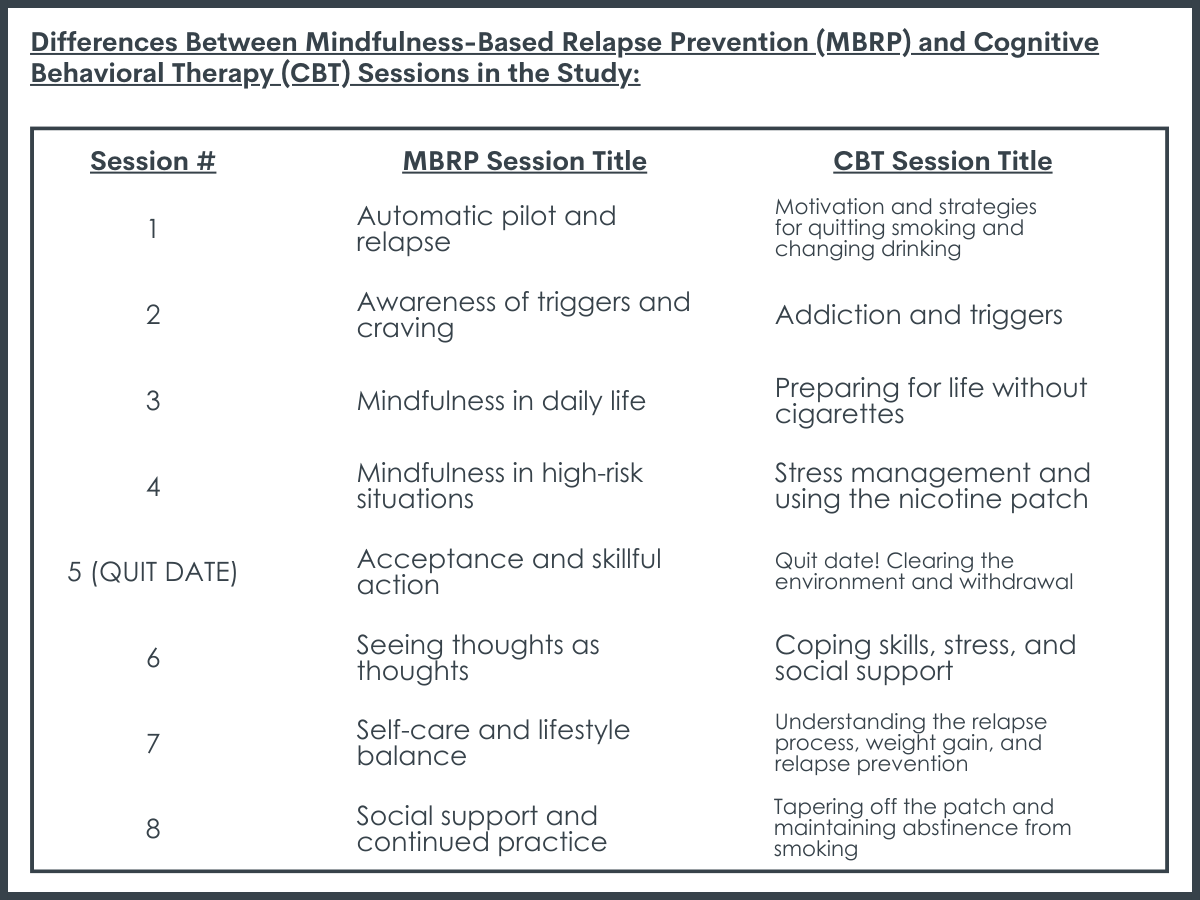
The researchers’ modified Mindfulness Based Relapse Prevention intervention retained the main features of classic Mindfulness Based Relapse Prevention, while adding content specific to smoking cessation, the co-use of cigarettes and alcohol, and reducing drinking (versus abstinence). Sessions 1–4 prepared participants for quitting smoking and changing their drinking by the ‘quit date’, which occurred at session 5. Sessions 5–8 built on the skills learned in sessions 1–4, while helping participants develop a mindfulness practice to continue once treatment ended. At the end of each session, homework was assigned that included daily mindfulness meditations.
CBT sessions utilized a mix of traditional CBT skills like identification of triggers, cultivation of relapse prevention coping skills, strategies to identify and change faulty beliefs and attitudes, as well as standard smoking cessation strategies. Homework was assigned each week, which involved practicing the skills learned that week.
All participants also received nicotine patches to support their smoking cessation efforts beginning with session 5, which represented their cigarette “quit day.”
Outcome measures included frequency and quantity of tobacco and alcohol use, assessed using a timeline follow-back calendar-based method. Feasibility and acceptability of the intervention were assessed based on recruitment and retention rates, number of sessions completed, and homework completion. Acceptability of the intervention was measured with the Client Satisfaction Questionnaire.
Participants completed follow-ups 5- and 8-weeks post-treatment. At 5-week follow-up, participants completed questionnaires online as well as a phone-based timeline follow-back interview of alcohol and tobacco use since the end of treatment. At 8-week follow-up, participants completed a phone-based timeline follow-back interview of alcohol and tobacco use since the last assessment, and if endorsing tobacco abstinence, a saliva cotinine test was mailed to confirm nicotine abstinence.
Because this was a pilot study, the researchers did not compare groups on study outcomes, but rather explored study outcomes like treatment retention and engagement, alcohol use, and tobacco use change within each group.
Participants were on average 41 years old. The sample was 69% female, 30% male, and 1% transgender. Racially, the sample was 64% White, 20% Black/African American, and 9% Other. In terms of ethnically, 12% of the sample identified as Hispanic/Latino. 55% of the Mindfulness Based Relapse Prevention group and 28% of the CBT group had alcohol use disorder, though degree of disorder severity was not specified.
WHAT DID THIS STUDY FIND?
Treatment retention and engagement were worse than anticipated.
Retention of participants in the study was quite low compared to other randomized trials, with 57% in the Mindfulness Based Relapse Prevention group and 50% in the CBT group retained in the study through to the end of treatment. In the Mindfulness Based Relapse Prevention group 43% completed all 8 sessions, while 34% in the CBT group completed all 8 sessions.
At the same time, as one might guess, participants who completed the end of treatment assessment endorsed high satisfaction with both treatments, and most of these participants planned to continue using the skills they had learned in treatment.
Participants indicated that the skills and tools learned in the respective interventions were most helpful parts of the treatment, along with the accountability and support of the group, and the nicotine patches. They also indicated that having groups over Zoom was convenient, while also highlighting some challenges with Zoom connectivity and having distractions in the home.
Both groups had notable reductions in drinking.
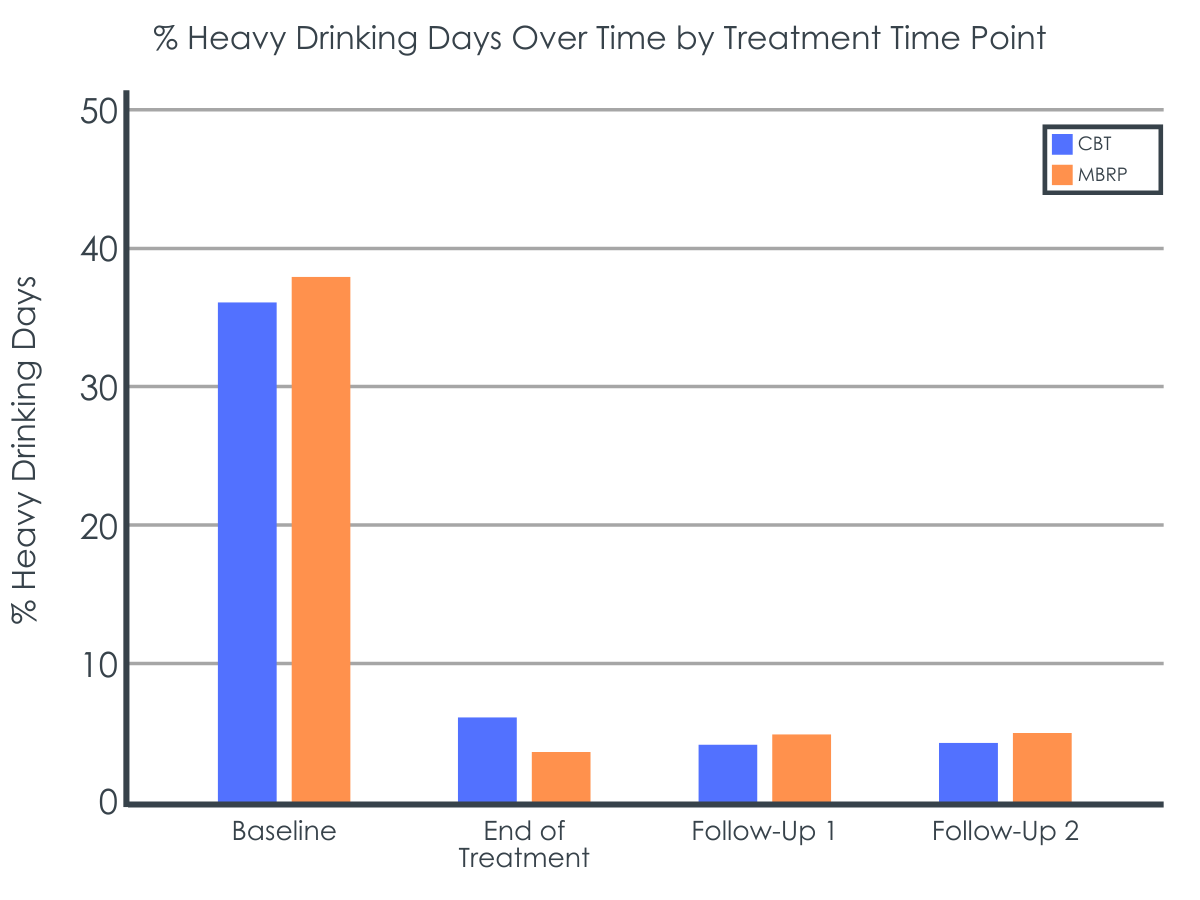
From baseline to the end of treatment, both groups had notable reductions in binge drinking days (defined as days with ≥4 drinks for women and ≥5 for men), with the Mindfulness Based Relapse Prevention group showing a 27% reduction and the CBT group reducing by 35%. Additionally, both groups had major reductions in average number of drinks per day from baseline to end of treatment with the Mindfulness Based Relapse Prevention group reducing by 72% and the CBT group reducing by 85%. Also, in both groups, most participants who consumed alcohol at moderate to very high levels at study baseline were either abstinent or drinking at low risk levels at end of treatment.
Overall, alcohol use reductions observed in both groups at the end of treatment were sustained at 5- and 8-week follow up.
Both groups also had notable reductions in smoking.
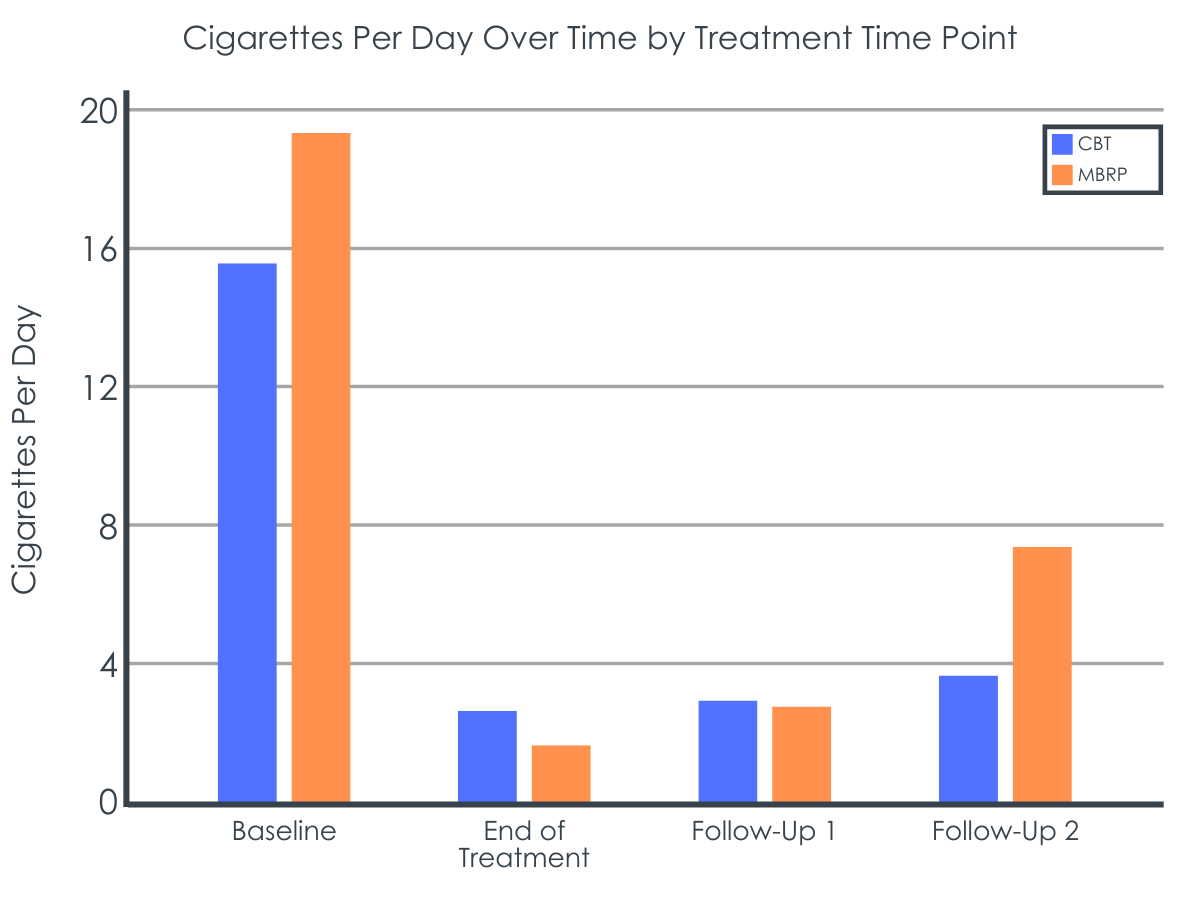
At end of treatment, 34% of participants in the Mindfulness Based Relapse Prevention group and 31% of participants in the CBT group self-reported abstinence from tobacco. Both groups also had noteworthy reductions in average number of cigarettes per day from baseline to end of treatment, with a 91% reduction in the Mindfulness Based Relapse Prevention group and a 79% reduction in the CBT group.
At the 8-week follow-up, after assuming study non-completers had continued to smoke, biochemically confirmed abstinence for treatment completers indicated 14% of participants in the Mindfulness Based Relapse Prevention group were tobacco abstinent, versus 3% in the CBT group.
Most participants who reduced or stopped drinking also reported reductions in smoking.
Smoking and alcohol use reductions were related. Of participants who reduced their average number of cigarettes per day, 88% also reported a reduction in their average number of drinks per day, with the remainder of participants reporting no change. This effect was consistent between experimental groups. Notably, no participants reported an increase in average number of drinks per day from the beginning to end of treatment.
In terms of alcohol use outcomes, although only about half of study participants completed the study, among those that did, Mindfulness Based Relapse Prevention produced comparable results to gold-standard CBT. Both interventions were associated with notable reductions in binge drinking and fairly large reductions in overall alcohol use (as measured by percentage of days abstinent and average drinks per day). Based on number of participants with alcohol use disorder, the Mindfulness Based Relapse Prevention group may have had more alcohol problem severity at study baseline, but because alcohol use disorder and drinking problem severity were not reported by the researchers, it is not clear how different the study groups were on this measure.
More importantly, the estimated reported treatment effects on alcohol use may have been inflated in this study because the researchers’ primary analyses of alcohol use outcomes only examined treatment completers who were likely more motivated to change their drinking at baseline, and/or had more resources available to them to help them stay in treatment and modify their drinking.
Regarding tobacco use cessation, results were less positive, but still suggested benefits associated with Mindfulness Based Relapse Prevention comparable to CBT. Overall, about a third of the total study sample had stopped using tobacco by end of treatment, with about 20% reporting abstinence at 5- and 8-week follow-up. Nicotine saliva testing suggested tobacco abstinence rates were lower than the self-reported results at 8-week follow-up, however poor test return rates may have influenced this result in unknown ways.
Participants who completed the end of treatment assessment endorsed high satisfaction with both Mindfulness Based Relapse Prevention and CBT, and most participants endorsed planning to continue using the skills they learned in treatment. This however may not be a great indicator of actual participant satisfaction with these interventions, given only about half the participants in each group completed treatment. It is possible that participants who discontinued study participation had a less favorable view of these interventions.
In fact, a major problem with both interventions was that only about half of the participants in each group completed treatment and with only 34%-43% of participants completing all the treatment sessions. Obviously, a major future endeavor will be to find out why so few completed the treatment, which was designed to be attractive, supportive, and conducive to these types of alcohol and smoking behavior changes in this particular population.
This study was conducted during the COVID-19 pandemic, which may have affected participant alcohol and tobacco use in unknown ways.
Although the researchers considered those who discontinued from the study to have returned to smoking, the large number of participants who did not complete /the study may have biased the results in unknown ways. For instance, people who dropped out of the study may be more likely to rate the treatments unfavorably, versus those who remained in the study, suggesting that the treatment satisfaction scores may be biased upwards.
There was no report of the participant predictors of treatment completion included in the paper so it is difficult to know who may or may not be more likely to benefit from this type of treatment.
The researchers did not conduct between group analyses of treatment response. Future studies will ideally look at this.
Not a limitation per se, however, between group differences in study outcomes were not explored in this pilot study. Future, larger studies will ideally explore between group differences on these study outcomes in this population.
BOTTOM LINE
A number of clinical trials have indicated Mindfulness Based Relapse Prevention can produce comparable results to gold-standard CBT for substance use disorder relapse prevention. This study provides some potential preliminary evidence that this intervention can also reduce drinking and tobacco use among adults seeking to reduce high-risk drinking behaviors and quit smoking who complete the treatment. An important area for future research also is understanding why so many fail to complete the treatments, so that the treatments can be better optimized to help engage people for longer and hopefully have more finish and derive greater benefit from the intended course of treatment. More studies are needed before Mindfulness Based Relapse Prevention can be recommended as a first-line intervention for co-occurring heavy alcohol use and cigarette smoking. At the same time, given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, it may be readily delivered to individuals interested in this type of treatment.
For individuals and families seeking recovery: This study suggests Mindfulness Based Relapse Prevention may help people who complete the treatment to reduce high-risk drinking and quit smoking. More research is needed, however, to know if this intervention can serve as a stand-alone treatment for combined high-risk drinking and smoking. Given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, there is no reason not to pursue this intervention as an adjunct to first-line interventions like CBT.
For treatment professionals and treatment systems: Mindfulness Based Relapse Prevention appears to be as good as CBT in this pilot study to help adults looking to reduce high-risk drinking and quit smoking. Given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, there is no reason not to offer this acceptance-based intervention as a complement to first-line, interventions like CBT. However, there is not yet a sufficient body of evidence to support Mindfulness Based Relapse Prevention as a stand-alone intervention for combined high-risk drinking and smoking.
For scientists: A growing base of evidence supports the notion that Mindfulness Based Relapse Prevention for substance use disorder relapse prevention is as helpful as other, more standard CBT interventions. In this pilot study, Mindfulness Based Relapse Prevention again produced similar results to CBT for helping adults to reduce high-risk drinking and quit smoking. More studies are needed to establish the efficacy of Mindfulness Based Relapse Prevention for managing high-risk drinking in combination with tobacco use to determine if this intervention might have efficacy as a stand-alone intervention. An important area for future research also is understanding why so many fail to complete the treatment so that the treatments can be better optimized to help engage people for longer and hopefully have more finish and derive greater benefit from the intended course of treatment. More mechanism studies are also needed to uncover exactly how Mindfulness Based Relapse Prevention’s may help reduce relapse risk and how these mechanisms may be similar or different than those related to more standard CBT treatment participation.
For policy makers: Mindfulness Based Relapse Prevention is an intervention that may help people reduce high-risk drinking and tobacco use. If future studies show this intervention to be helpful for addressing these co-occurring issues, policies that increase accessibility to this class of interventions will have the potential to improve public health as it may provide another option that may be attractive and engaging for certain types of individuals who may not be otherwise attracted by more standard CBT approaches.
Binge drinking and tobacco use both pose serious health risks, increasing the chance of disease as well as premature death, and together they have additive harmful effects. Additionally, alcohol use—especially binge drinking—can undermine people’s efforts to quit smoking, making this behavioral combination especially problematic.
Mindfulness Based Relapse Prevention is an 8-week intervention developed to treat substance use disorder that has also been used to support smoking cessation. Previous clinical trials have produced promising results suggesting this intervention can prevent substance use disorder relapse as well as standard relapse prevention approaches, and also help individuals quit smoking. Mechanism studies have shown that mindfulness might support addiction recovery and smoking cessation by reducing negative affect like stress and anxiety and disrupting the link between negative affect and craving.
Previous clinical trials have suggested mindfulness-based interventions might support smoking cessation while also reducing high-risk drinking behaviors in individuals engaging in high-risk drinking, but not yet experiencing alcohol addiction (i.e., severe alcohol use disorder). In this study, the researchers compared Mindfulness Based Relapse Prevention with minor modifications to also address nicotine cravings, to standard Cognitive Behavioral Therapy (CBT) in a sample of smokers who endorsed regular binge drinking, who were motivated to quit smoking and reduce their alcohol intake. Due to the COVID-19, the study was conducted remotely.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized trial with 67 adults who reported binge drinking and were motivated to both quit smoking and reduce their alcohol use. Participants received either 8 sessions of Mindfulness Based Relapse Prevention or CBT. Both interventions were delivered over Zoom consistent with COVID-19 physical distancing guidelines.
The researchers’ modified Mindfulness Based Relapse Prevention intervention retained the main features of classic Mindfulness Based Relapse Prevention, while adding content specific to smoking cessation, the co-use of cigarettes and alcohol, and reducing drinking (versus abstinence). Sessions 1–4 prepared participants for quitting smoking and changing their drinking by the ‘quit date’, which occurred at session 5. Sessions 5–8 built on the skills learned in sessions 1–4, while helping participants develop a mindfulness practice to continue once treatment ended. At the end of each session, homework was assigned that included daily mindfulness meditations.
CBT sessions utilized a mix of traditional CBT skills like identification of triggers, cultivation of relapse prevention coping skills, strategies to identify and change faulty beliefs and attitudes, as well as standard smoking cessation strategies. Homework was assigned each week, which involved practicing the skills learned that week.
All participants also received nicotine patches to support their smoking cessation efforts beginning with session 5, which represented their cigarette “quit day.”
Outcome measures included frequency and quantity of tobacco and alcohol use, assessed using a timeline follow-back calendar-based method. Feasibility and acceptability of the intervention were assessed based on recruitment and retention rates, number of sessions completed, and homework completion. Acceptability of the intervention was measured with the Client Satisfaction Questionnaire.
Participants completed follow-ups 5- and 8-weeks post-treatment. At 5-week follow-up, participants completed questionnaires online as well as a phone-based timeline follow-back interview of alcohol and tobacco use since the end of treatment. At 8-week follow-up, participants completed a phone-based timeline follow-back interview of alcohol and tobacco use since the last assessment, and if endorsing tobacco abstinence, a saliva cotinine test was mailed to confirm nicotine abstinence.
Because this was a pilot study, the researchers did not compare groups on study outcomes, but rather explored study outcomes like treatment retention and engagement, alcohol use, and tobacco use change within each group.
Participants were on average 41 years old. The sample was 69% female, 30% male, and 1% transgender. Racially, the sample was 64% White, 20% Black/African American, and 9% Other. In terms of ethnically, 12% of the sample identified as Hispanic/Latino. 55% of the Mindfulness Based Relapse Prevention group and 28% of the CBT group had alcohol use disorder, though degree of disorder severity was not specified.
WHAT DID THIS STUDY FIND?
Treatment retention and engagement were worse than anticipated.
Retention of participants in the study was quite low compared to other randomized trials, with 57% in the Mindfulness Based Relapse Prevention group and 50% in the CBT group retained in the study through to the end of treatment. In the Mindfulness Based Relapse Prevention group 43% completed all 8 sessions, while 34% in the CBT group completed all 8 sessions.
At the same time, as one might guess, participants who completed the end of treatment assessment endorsed high satisfaction with both treatments, and most of these participants planned to continue using the skills they had learned in treatment.
Participants indicated that the skills and tools learned in the respective interventions were most helpful parts of the treatment, along with the accountability and support of the group, and the nicotine patches. They also indicated that having groups over Zoom was convenient, while also highlighting some challenges with Zoom connectivity and having distractions in the home.
Both groups had notable reductions in drinking.
From baseline to the end of treatment, both groups had notable reductions in binge drinking days (defined as days with ≥4 drinks for women and ≥5 for men), with the Mindfulness Based Relapse Prevention group showing a 27% reduction and the CBT group reducing by 35%. Additionally, both groups had major reductions in average number of drinks per day from baseline to end of treatment with the Mindfulness Based Relapse Prevention group reducing by 72% and the CBT group reducing by 85%. Also, in both groups, most participants who consumed alcohol at moderate to very high levels at study baseline were either abstinent or drinking at low risk levels at end of treatment.
Overall, alcohol use reductions observed in both groups at the end of treatment were sustained at 5- and 8-week follow up.
Both groups also had notable reductions in smoking.
At end of treatment, 34% of participants in the Mindfulness Based Relapse Prevention group and 31% of participants in the CBT group self-reported abstinence from tobacco. Both groups also had noteworthy reductions in average number of cigarettes per day from baseline to end of treatment, with a 91% reduction in the Mindfulness Based Relapse Prevention group and a 79% reduction in the CBT group.
At the 8-week follow-up, after assuming study non-completers had continued to smoke, biochemically confirmed abstinence for treatment completers indicated 14% of participants in the Mindfulness Based Relapse Prevention group were tobacco abstinent, versus 3% in the CBT group.
Most participants who reduced or stopped drinking also reported reductions in smoking.
Smoking and alcohol use reductions were related. Of participants who reduced their average number of cigarettes per day, 88% also reported a reduction in their average number of drinks per day, with the remainder of participants reporting no change. This effect was consistent between experimental groups. Notably, no participants reported an increase in average number of drinks per day from the beginning to end of treatment.
In terms of alcohol use outcomes, although only about half of study participants completed the study, among those that did, Mindfulness Based Relapse Prevention produced comparable results to gold-standard CBT. Both interventions were associated with notable reductions in binge drinking and fairly large reductions in overall alcohol use (as measured by percentage of days abstinent and average drinks per day). Based on number of participants with alcohol use disorder, the Mindfulness Based Relapse Prevention group may have had more alcohol problem severity at study baseline, but because alcohol use disorder and drinking problem severity were not reported by the researchers, it is not clear how different the study groups were on this measure.
More importantly, the estimated reported treatment effects on alcohol use may have been inflated in this study because the researchers’ primary analyses of alcohol use outcomes only examined treatment completers who were likely more motivated to change their drinking at baseline, and/or had more resources available to them to help them stay in treatment and modify their drinking.
Regarding tobacco use cessation, results were less positive, but still suggested benefits associated with Mindfulness Based Relapse Prevention comparable to CBT. Overall, about a third of the total study sample had stopped using tobacco by end of treatment, with about 20% reporting abstinence at 5- and 8-week follow-up. Nicotine saliva testing suggested tobacco abstinence rates were lower than the self-reported results at 8-week follow-up, however poor test return rates may have influenced this result in unknown ways.
Participants who completed the end of treatment assessment endorsed high satisfaction with both Mindfulness Based Relapse Prevention and CBT, and most participants endorsed planning to continue using the skills they learned in treatment. This however may not be a great indicator of actual participant satisfaction with these interventions, given only about half the participants in each group completed treatment. It is possible that participants who discontinued study participation had a less favorable view of these interventions.
In fact, a major problem with both interventions was that only about half of the participants in each group completed treatment and with only 34%-43% of participants completing all the treatment sessions. Obviously, a major future endeavor will be to find out why so few completed the treatment, which was designed to be attractive, supportive, and conducive to these types of alcohol and smoking behavior changes in this particular population.
This study was conducted during the COVID-19 pandemic, which may have affected participant alcohol and tobacco use in unknown ways.
Although the researchers considered those who discontinued from the study to have returned to smoking, the large number of participants who did not complete /the study may have biased the results in unknown ways. For instance, people who dropped out of the study may be more likely to rate the treatments unfavorably, versus those who remained in the study, suggesting that the treatment satisfaction scores may be biased upwards.
There was no report of the participant predictors of treatment completion included in the paper so it is difficult to know who may or may not be more likely to benefit from this type of treatment.
The researchers did not conduct between group analyses of treatment response. Future studies will ideally look at this.
Not a limitation per se, however, between group differences in study outcomes were not explored in this pilot study. Future, larger studies will ideally explore between group differences on these study outcomes in this population.
BOTTOM LINE
A number of clinical trials have indicated Mindfulness Based Relapse Prevention can produce comparable results to gold-standard CBT for substance use disorder relapse prevention. This study provides some potential preliminary evidence that this intervention can also reduce drinking and tobacco use among adults seeking to reduce high-risk drinking behaviors and quit smoking who complete the treatment. An important area for future research also is understanding why so many fail to complete the treatments, so that the treatments can be better optimized to help engage people for longer and hopefully have more finish and derive greater benefit from the intended course of treatment. More studies are needed before Mindfulness Based Relapse Prevention can be recommended as a first-line intervention for co-occurring heavy alcohol use and cigarette smoking. At the same time, given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, it may be readily delivered to individuals interested in this type of treatment.
For individuals and families seeking recovery: This study suggests Mindfulness Based Relapse Prevention may help people who complete the treatment to reduce high-risk drinking and quit smoking. More research is needed, however, to know if this intervention can serve as a stand-alone treatment for combined high-risk drinking and smoking. Given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, there is no reason not to pursue this intervention as an adjunct to first-line interventions like CBT.
For treatment professionals and treatment systems: Mindfulness Based Relapse Prevention appears to be as good as CBT in this pilot study to help adults looking to reduce high-risk drinking and quit smoking. Given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, there is no reason not to offer this acceptance-based intervention as a complement to first-line, interventions like CBT. However, there is not yet a sufficient body of evidence to support Mindfulness Based Relapse Prevention as a stand-alone intervention for combined high-risk drinking and smoking.
For scientists: A growing base of evidence supports the notion that Mindfulness Based Relapse Prevention for substance use disorder relapse prevention is as helpful as other, more standard CBT interventions. In this pilot study, Mindfulness Based Relapse Prevention again produced similar results to CBT for helping adults to reduce high-risk drinking and quit smoking. More studies are needed to establish the efficacy of Mindfulness Based Relapse Prevention for managing high-risk drinking in combination with tobacco use to determine if this intervention might have efficacy as a stand-alone intervention. An important area for future research also is understanding why so many fail to complete the treatment so that the treatments can be better optimized to help engage people for longer and hopefully have more finish and derive greater benefit from the intended course of treatment. More mechanism studies are also needed to uncover exactly how Mindfulness Based Relapse Prevention’s may help reduce relapse risk and how these mechanisms may be similar or different than those related to more standard CBT treatment participation.
For policy makers: Mindfulness Based Relapse Prevention is an intervention that may help people reduce high-risk drinking and tobacco use. If future studies show this intervention to be helpful for addressing these co-occurring issues, policies that increase accessibility to this class of interventions will have the potential to improve public health as it may provide another option that may be attractive and engaging for certain types of individuals who may not be otherwise attracted by more standard CBT approaches.
Binge drinking and tobacco use both pose serious health risks, increasing the chance of disease as well as premature death, and together they have additive harmful effects. Additionally, alcohol use—especially binge drinking—can undermine people’s efforts to quit smoking, making this behavioral combination especially problematic.
Mindfulness Based Relapse Prevention is an 8-week intervention developed to treat substance use disorder that has also been used to support smoking cessation. Previous clinical trials have produced promising results suggesting this intervention can prevent substance use disorder relapse as well as standard relapse prevention approaches, and also help individuals quit smoking. Mechanism studies have shown that mindfulness might support addiction recovery and smoking cessation by reducing negative affect like stress and anxiety and disrupting the link between negative affect and craving.
Previous clinical trials have suggested mindfulness-based interventions might support smoking cessation while also reducing high-risk drinking behaviors in individuals engaging in high-risk drinking, but not yet experiencing alcohol addiction (i.e., severe alcohol use disorder). In this study, the researchers compared Mindfulness Based Relapse Prevention with minor modifications to also address nicotine cravings, to standard Cognitive Behavioral Therapy (CBT) in a sample of smokers who endorsed regular binge drinking, who were motivated to quit smoking and reduce their alcohol intake. Due to the COVID-19, the study was conducted remotely.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized trial with 67 adults who reported binge drinking and were motivated to both quit smoking and reduce their alcohol use. Participants received either 8 sessions of Mindfulness Based Relapse Prevention or CBT. Both interventions were delivered over Zoom consistent with COVID-19 physical distancing guidelines.
The researchers’ modified Mindfulness Based Relapse Prevention intervention retained the main features of classic Mindfulness Based Relapse Prevention, while adding content specific to smoking cessation, the co-use of cigarettes and alcohol, and reducing drinking (versus abstinence). Sessions 1–4 prepared participants for quitting smoking and changing their drinking by the ‘quit date’, which occurred at session 5. Sessions 5–8 built on the skills learned in sessions 1–4, while helping participants develop a mindfulness practice to continue once treatment ended. At the end of each session, homework was assigned that included daily mindfulness meditations.
CBT sessions utilized a mix of traditional CBT skills like identification of triggers, cultivation of relapse prevention coping skills, strategies to identify and change faulty beliefs and attitudes, as well as standard smoking cessation strategies. Homework was assigned each week, which involved practicing the skills learned that week.
All participants also received nicotine patches to support their smoking cessation efforts beginning with session 5, which represented their cigarette “quit day.”
Outcome measures included frequency and quantity of tobacco and alcohol use, assessed using a timeline follow-back calendar-based method. Feasibility and acceptability of the intervention were assessed based on recruitment and retention rates, number of sessions completed, and homework completion. Acceptability of the intervention was measured with the Client Satisfaction Questionnaire.
Participants completed follow-ups 5- and 8-weeks post-treatment. At 5-week follow-up, participants completed questionnaires online as well as a phone-based timeline follow-back interview of alcohol and tobacco use since the end of treatment. At 8-week follow-up, participants completed a phone-based timeline follow-back interview of alcohol and tobacco use since the last assessment, and if endorsing tobacco abstinence, a saliva cotinine test was mailed to confirm nicotine abstinence.
Because this was a pilot study, the researchers did not compare groups on study outcomes, but rather explored study outcomes like treatment retention and engagement, alcohol use, and tobacco use change within each group.
Participants were on average 41 years old. The sample was 69% female, 30% male, and 1% transgender. Racially, the sample was 64% White, 20% Black/African American, and 9% Other. In terms of ethnically, 12% of the sample identified as Hispanic/Latino. 55% of the Mindfulness Based Relapse Prevention group and 28% of the CBT group had alcohol use disorder, though degree of disorder severity was not specified.
WHAT DID THIS STUDY FIND?
Treatment retention and engagement were worse than anticipated.
Retention of participants in the study was quite low compared to other randomized trials, with 57% in the Mindfulness Based Relapse Prevention group and 50% in the CBT group retained in the study through to the end of treatment. In the Mindfulness Based Relapse Prevention group 43% completed all 8 sessions, while 34% in the CBT group completed all 8 sessions.
At the same time, as one might guess, participants who completed the end of treatment assessment endorsed high satisfaction with both treatments, and most of these participants planned to continue using the skills they had learned in treatment.
Participants indicated that the skills and tools learned in the respective interventions were most helpful parts of the treatment, along with the accountability and support of the group, and the nicotine patches. They also indicated that having groups over Zoom was convenient, while also highlighting some challenges with Zoom connectivity and having distractions in the home.
Both groups had notable reductions in drinking.
From baseline to the end of treatment, both groups had notable reductions in binge drinking days (defined as days with ≥4 drinks for women and ≥5 for men), with the Mindfulness Based Relapse Prevention group showing a 27% reduction and the CBT group reducing by 35%. Additionally, both groups had major reductions in average number of drinks per day from baseline to end of treatment with the Mindfulness Based Relapse Prevention group reducing by 72% and the CBT group reducing by 85%. Also, in both groups, most participants who consumed alcohol at moderate to very high levels at study baseline were either abstinent or drinking at low risk levels at end of treatment.
Overall, alcohol use reductions observed in both groups at the end of treatment were sustained at 5- and 8-week follow up.
Both groups also had notable reductions in smoking.
At end of treatment, 34% of participants in the Mindfulness Based Relapse Prevention group and 31% of participants in the CBT group self-reported abstinence from tobacco. Both groups also had noteworthy reductions in average number of cigarettes per day from baseline to end of treatment, with a 91% reduction in the Mindfulness Based Relapse Prevention group and a 79% reduction in the CBT group.
At the 8-week follow-up, after assuming study non-completers had continued to smoke, biochemically confirmed abstinence for treatment completers indicated 14% of participants in the Mindfulness Based Relapse Prevention group were tobacco abstinent, versus 3% in the CBT group.
Most participants who reduced or stopped drinking also reported reductions in smoking.
Smoking and alcohol use reductions were related. Of participants who reduced their average number of cigarettes per day, 88% also reported a reduction in their average number of drinks per day, with the remainder of participants reporting no change. This effect was consistent between experimental groups. Notably, no participants reported an increase in average number of drinks per day from the beginning to end of treatment.
In terms of alcohol use outcomes, although only about half of study participants completed the study, among those that did, Mindfulness Based Relapse Prevention produced comparable results to gold-standard CBT. Both interventions were associated with notable reductions in binge drinking and fairly large reductions in overall alcohol use (as measured by percentage of days abstinent and average drinks per day). Based on number of participants with alcohol use disorder, the Mindfulness Based Relapse Prevention group may have had more alcohol problem severity at study baseline, but because alcohol use disorder and drinking problem severity were not reported by the researchers, it is not clear how different the study groups were on this measure.
More importantly, the estimated reported treatment effects on alcohol use may have been inflated in this study because the researchers’ primary analyses of alcohol use outcomes only examined treatment completers who were likely more motivated to change their drinking at baseline, and/or had more resources available to them to help them stay in treatment and modify their drinking.
Regarding tobacco use cessation, results were less positive, but still suggested benefits associated with Mindfulness Based Relapse Prevention comparable to CBT. Overall, about a third of the total study sample had stopped using tobacco by end of treatment, with about 20% reporting abstinence at 5- and 8-week follow-up. Nicotine saliva testing suggested tobacco abstinence rates were lower than the self-reported results at 8-week follow-up, however poor test return rates may have influenced this result in unknown ways.
Participants who completed the end of treatment assessment endorsed high satisfaction with both Mindfulness Based Relapse Prevention and CBT, and most participants endorsed planning to continue using the skills they learned in treatment. This however may not be a great indicator of actual participant satisfaction with these interventions, given only about half the participants in each group completed treatment. It is possible that participants who discontinued study participation had a less favorable view of these interventions.
In fact, a major problem with both interventions was that only about half of the participants in each group completed treatment and with only 34%-43% of participants completing all the treatment sessions. Obviously, a major future endeavor will be to find out why so few completed the treatment, which was designed to be attractive, supportive, and conducive to these types of alcohol and smoking behavior changes in this particular population.
This study was conducted during the COVID-19 pandemic, which may have affected participant alcohol and tobacco use in unknown ways.
Although the researchers considered those who discontinued from the study to have returned to smoking, the large number of participants who did not complete /the study may have biased the results in unknown ways. For instance, people who dropped out of the study may be more likely to rate the treatments unfavorably, versus those who remained in the study, suggesting that the treatment satisfaction scores may be biased upwards.
There was no report of the participant predictors of treatment completion included in the paper so it is difficult to know who may or may not be more likely to benefit from this type of treatment.
The researchers did not conduct between group analyses of treatment response. Future studies will ideally look at this.
Not a limitation per se, however, between group differences in study outcomes were not explored in this pilot study. Future, larger studies will ideally explore between group differences on these study outcomes in this population.
BOTTOM LINE
A number of clinical trials have indicated Mindfulness Based Relapse Prevention can produce comparable results to gold-standard CBT for substance use disorder relapse prevention. This study provides some potential preliminary evidence that this intervention can also reduce drinking and tobacco use among adults seeking to reduce high-risk drinking behaviors and quit smoking who complete the treatment. An important area for future research also is understanding why so many fail to complete the treatments, so that the treatments can be better optimized to help engage people for longer and hopefully have more finish and derive greater benefit from the intended course of treatment. More studies are needed before Mindfulness Based Relapse Prevention can be recommended as a first-line intervention for co-occurring heavy alcohol use and cigarette smoking. At the same time, given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, it may be readily delivered to individuals interested in this type of treatment.
For individuals and families seeking recovery: This study suggests Mindfulness Based Relapse Prevention may help people who complete the treatment to reduce high-risk drinking and quit smoking. More research is needed, however, to know if this intervention can serve as a stand-alone treatment for combined high-risk drinking and smoking. Given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, there is no reason not to pursue this intervention as an adjunct to first-line interventions like CBT.
For treatment professionals and treatment systems: Mindfulness Based Relapse Prevention appears to be as good as CBT in this pilot study to help adults looking to reduce high-risk drinking and quit smoking. Given Mindfulness Based Relapse Prevention has no known adverse side effects and is known to produce side benefits like improved emotion regulation, there is no reason not to offer this acceptance-based intervention as a complement to first-line, interventions like CBT. However, there is not yet a sufficient body of evidence to support Mindfulness Based Relapse Prevention as a stand-alone intervention for combined high-risk drinking and smoking.
For scientists: A growing base of evidence supports the notion that Mindfulness Based Relapse Prevention for substance use disorder relapse prevention is as helpful as other, more standard CBT interventions. In this pilot study, Mindfulness Based Relapse Prevention again produced similar results to CBT for helping adults to reduce high-risk drinking and quit smoking. More studies are needed to establish the efficacy of Mindfulness Based Relapse Prevention for managing high-risk drinking in combination with tobacco use to determine if this intervention might have efficacy as a stand-alone intervention. An important area for future research also is understanding why so many fail to complete the treatment so that the treatments can be better optimized to help engage people for longer and hopefully have more finish and derive greater benefit from the intended course of treatment. More mechanism studies are also needed to uncover exactly how Mindfulness Based Relapse Prevention’s may help reduce relapse risk and how these mechanisms may be similar or different than those related to more standard CBT treatment participation.
For policy makers: Mindfulness Based Relapse Prevention is an intervention that may help people reduce high-risk drinking and tobacco use. If future studies show this intervention to be helpful for addressing these co-occurring issues, policies that increase accessibility to this class of interventions will have the potential to improve public health as it may provide another option that may be attractive and engaging for certain types of individuals who may not be otherwise attracted by more standard CBT approaches.