Alcohol, tobacco, and co-occurring psychiatric disorders in a national U.S. sample: differences by sex, sexual identity, and stress
National studies show disproportionately high rates of psychological distress and alcohol and other drug use disorders among lesbian, gay, and bisexual individuals. This health inequity is thought to be due to sexual minority stress caused by sexual orientation stigma and discrimination. This study reports U.S. population prevalence rates of alcohol and tobacco use disorder and co-occurring psychiatric disorders among lesbian, gay, bisexual, and heterosexual adults, and associations with different types of stress.
LGBTQ+ populations such as lesbian, gay, and bisexual people report higher rates of alcohol use disorder and co-occurring mood and anxiety disorders compared to heterosexual individuals, with the highest rates among bisexual individuals. In general, bisexual people tend to seek help for alcohol use disorder more frequently than heterosexual people, and more commonly attend Alcoholics Anonymous. At the same time, they also report more barriers to seeking treatment such as fear of judgement from others or not being able to pay for treatment. A large proportion of U.S. adults in recovery from an alcohol or other drug problem are lesbian, gay, or bisexual, who also report higher rates of lifetime co-occurring psychiatric diagnoses, lower quality of life, happiness, self-esteem, and recovery capital compared to heterosexual adults in recovery, independent of how long they have been in recovery. Research can help determine why LGBTQ+ face these greater substance use and mental health challenges, to inform policies and practices tailored to help these at-risk groups.
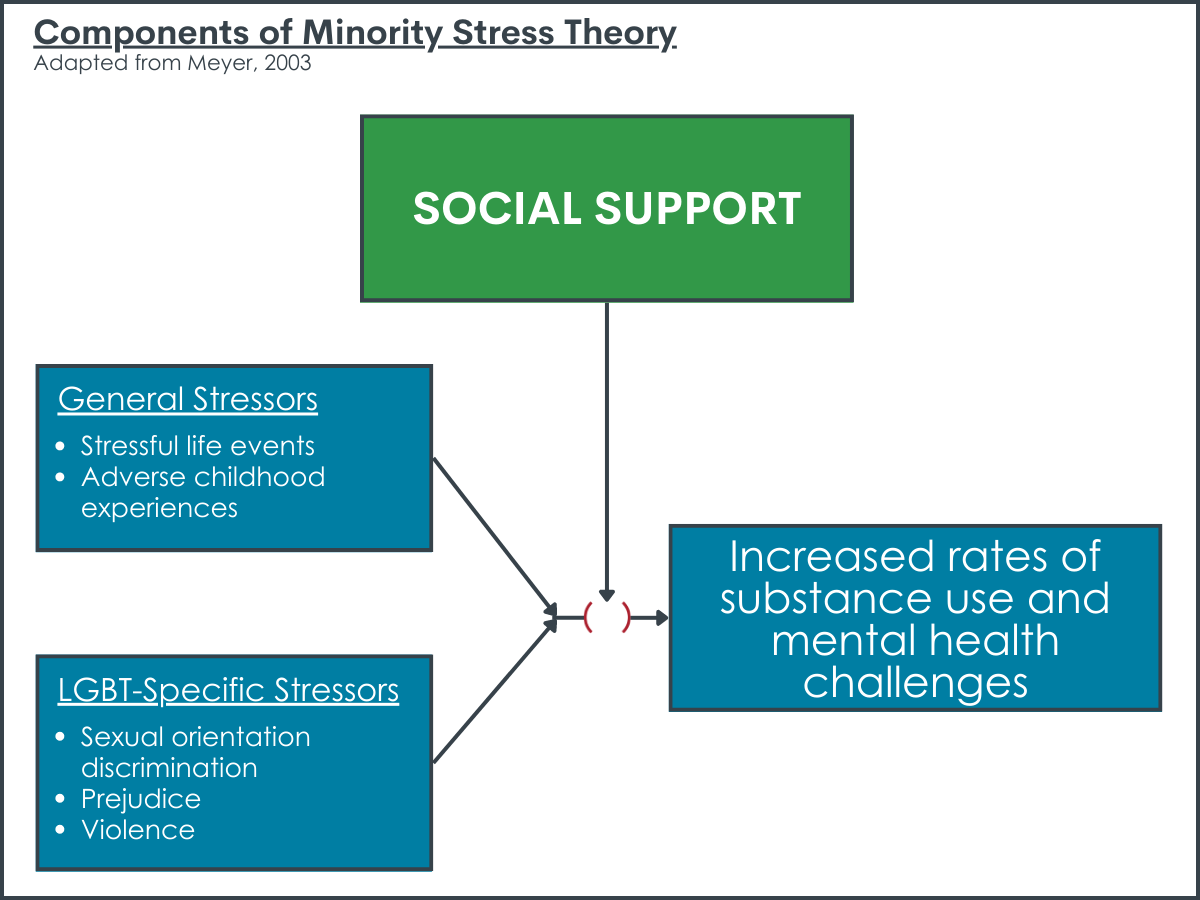
Minority Stress Theory suggests that LGBTQ+ individuals bear a disproportionate burden of worse mental and physical health outcomes due to the stigmatization of any sexual attraction, gender expression, identity or behavior that does not conform to a heterosexual “norm” and the subsequent stigma-related stressors (so called “minority stress”) LGBTQ+ people face. This “minority stress” includes: a) chronic and accumulating stressors that can be experienced by all individuals, but have documented higher prevalence rates among LGBTQ+ populations, such as adverse childhood experiences and stressful life events; and b) specific discrimination and marginalization society imposes because of LGBTQ+ individual’s sexual orientation and/or gender identity – creating an increased risk or burden of worse mental and physical health outcomes compared to heterosexual peers.
Although research on the prevalence of substance use and mental health disorders among LGBTQ+ populations is growing, few studies have examined the co-occurrence of substance use disorders and psychiatric disorders among LGBTQ+ populations in a nationally representative sample, nor tested associations with stress. For example, another study found that sexually diverse participants had higher rates of alcohol and tobacco use disorders, and more severe disorder symptoms, with the highest rates among bisexual adults. The current study adds to this work by examining the prevalence of co-occurring alcohol and tobacco use disorders with mood and anxiety disorders, by sex and sexual identity, and how general (recent stressful life events, adverse childhood experiences) and specific (recent sexual orientation discrimination) stressors are related to the prevalence of these co-occurring disorders. Examining the prevalence of co-occurring substance use and psychiatric disorders among gay, lesbian, and bisexual men and women compared to heterosexual men and women, and associations with stress, can provide further support for Minority Stress Theory, highlighting potential areas for intervention to reduce risks of substance use and psychiatric disorder.
This study uses U.S. national survey data from 2012-2013 to examine three research questions: 1. What are the prevalence rates of alcohol and tobacco use disorder with co-occurring psychiatric disorder among sexually diverse men and women compared to heterosexual men and women? 2. What kinds of stressors and support are associated with such rates of co-occurring substance use and psychiatric disorders among men and women generally? 3. What kinds of stressors and support are associated with rates of co-occurring substance use and psychiatric disorders among sexually diverse men and women specifically? Focusing on experiences of LGBTQ+ individuals with substance use disorder that can be addressed therapeutically, such as co-occurring disorders, can help inform comprehensive strategies to improve the lives of these at-risk groups.
HOW WAS THIS STUDY CONDUCTED?
This study used the U.S. National Epidemiologic Survey on Alcohol and Related Conditions (NESARC)-III data from 2012-2013 to examine: (1) the prevalence of co-occurring psychiatric, alcohol, and tobacco use disorders among adults (N = 36,309) stratified by sexual orientation (gay or lesbian, bisexual, heterosexual) and sex (women and men); (2) general stressors and support associated with co-occurring substance use and psychiatric disorders among men and women, including stressful life events, adverse childhood experiences, and social support; (3) general and specific stressors and support associated with co-occurring substance use and psychiatric disorders among sexually diverse men and women.
Participants in this study included noninstitutionalized civilian adults in the U.S. ages 18 and older surveyed via in-person interviews who had available sexual identity data. Past-year alcohol use disorder, tobacco use disorder, and co-occurring psychiatric disorders were assessed using DSM-5 diagnostic criteria with a commonly used, well-validated structured interview. Co-occurring psychiatric disorders included: past-year mood disorder (i.e., major depressive disorder, bipolar I and II disorder, and dysthymia); past-year anxiety disorder (i.e., generalized anxiety disorder, specific phobia, social anxiety disorder, panic disorder, and agoraphobia); and past-year post-traumatic stress disorder (PTSD). Participants were also asked about past-year stressors that included 16 life events (e.g., moved, lost employment, divorced), adverse childhood experiences that included 18 question items (e.g., physical, sexual, and emotional abuse; exposure to family violence; parental incarceration), and social support using 12 questions. Sexually diverse participants were also asked about 6 different types of sexual orientation discrimination (e.g., discrimination in health care settings, public settings, and obtaining a job). Actual questionnaire items from the NESARC-III study can be found here.
The analyses first examined the prevalence of alcohol use disorder, tobacco use disorder, mood disorders, anxiety disorders, and PTSD using the full sample, separated by sex (men and women) and sexual identity (gay or lesbian, bisexual, or heterosexual) to show differences in the prevalence rates across groups. Then the analyses estimated the prevalence of co-occurring mood, anxiety, or PTSD among those participants in the sample who met criteria for past-year alcohol use disorder (N=5,042) and past-year tobacco use disorder (N=7,188), by sex (men and women) and sexual identity (gay or lesbian, bisexual, or heterosexual) to show differences in the prevalence rates of co-occurring disorders across groups. Finally, they examined the associations between general stressors (stressful life events, adverse childhood experiences), social support, and co-occurring disorders in the full sample. Then they examined the associations between both general (stressful life events, adverse childhood experiences) and specific stressors (sexual orientation discrimination) and social support only among sexually diverse participants. These analyses also examined whether social support might buffer any effects of stressors or adverse childhood experiences on substance use and mental health disorders. They did not test whether social support might buffer risks from stressors and adverse childhood experiences in the sample of only sexually diverse participants compared to heterosexual participants in the sample, as there were too few sexually diverse participants to perform this analysis. Nor could they test whether any buffering conferred by social support was different for sexual minority versus heterosexual participants.
Sexually diverse participants included those who identified as gay or lesbian, bisexual, or individuals who identified as heterosexual but reported same sex attraction or behavior (N=3,203). All analyses controlled for demographic variables that could also influence the prevalence of co-occurring substance use and psychiatric disorders in order to estimate the specific effect of stress and social support on the prevalence of such co-occurring disorders among sexually diverse and heterosexual men and women: race/ethnicity (White non-Hispanic, Black non-Hispanic, American Indian/Alaska Native non-Hispanic, Asian/Native Hawaiian/Other Pacific Islander non-Hispanic, and Hispanic), education (high school diploma or more, or less than a high school diploma), annual income (<$25,000, $25,000–$59,999, >$60,000), urbanicity (urban or rural), and region (Northeast, Midwest, South, and West).
WHAT DID THIS STUDY FIND?
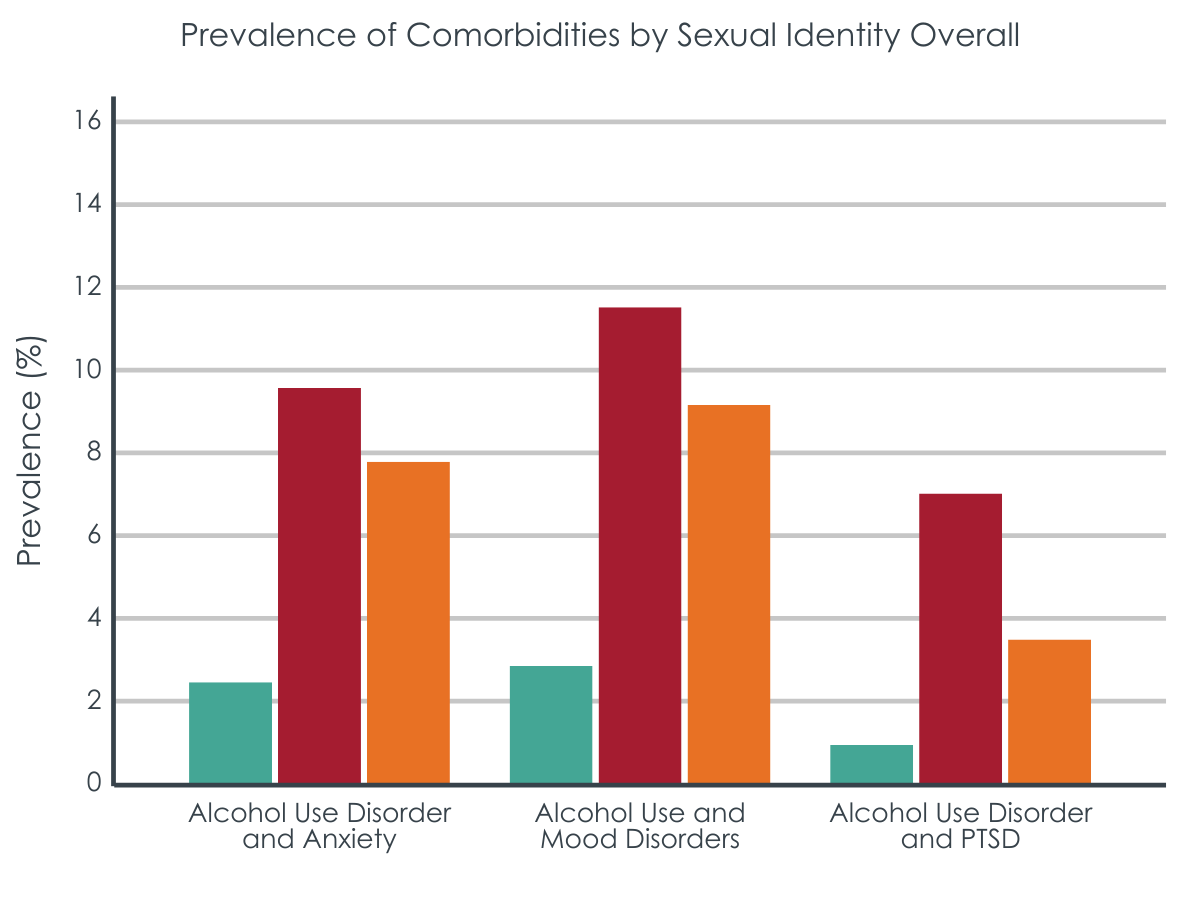
Sexually diverse participants had the highest rates of alcohol and tobacco use disorders, mood and anxiety disorders, and PTSD.
Among the full sample, when examining disorders independently, sexually diverse participants had higher rates of past-year alcohol use disorder, tobacco use disorder, anxiety disorders, mood disorders, and PTSD, compared to heterosexual participants. Bisexual individuals had a fourfold greater prevalence of PTSD (17.9%) compared to heterosexual individuals (4.4%).
Men
Among men, gay men had a higher prevalence of past-year alcohol use disorder (31.4%) and tobacco use disorder (40.8%) compared with the overall sample (13.8%, 12%, respectively). Both gay men and bisexual men had a significantly higher prevalence of all disorders compared with heterosexual men.
Women
Among women, gay or lesbian women had a higher prevalence of alcohol use disorder (25%), tobacco use disorder (27%), and mood disorders (24%) compared with heterosexual women (10%, 16%, 15%, respectively). Bisexual women had a particularly high prevalence of anxiety disorders (32.5%), mood disorders (34.9%), and PTSD (21.0%), compared with the overall sample (13%, 12.8%, and 5.6%, respectively), and a significantly higher prevalence of alcohol (30%) and tobacco use disorders (36%), compared with heterosexual women (10%, 16%, respectively).
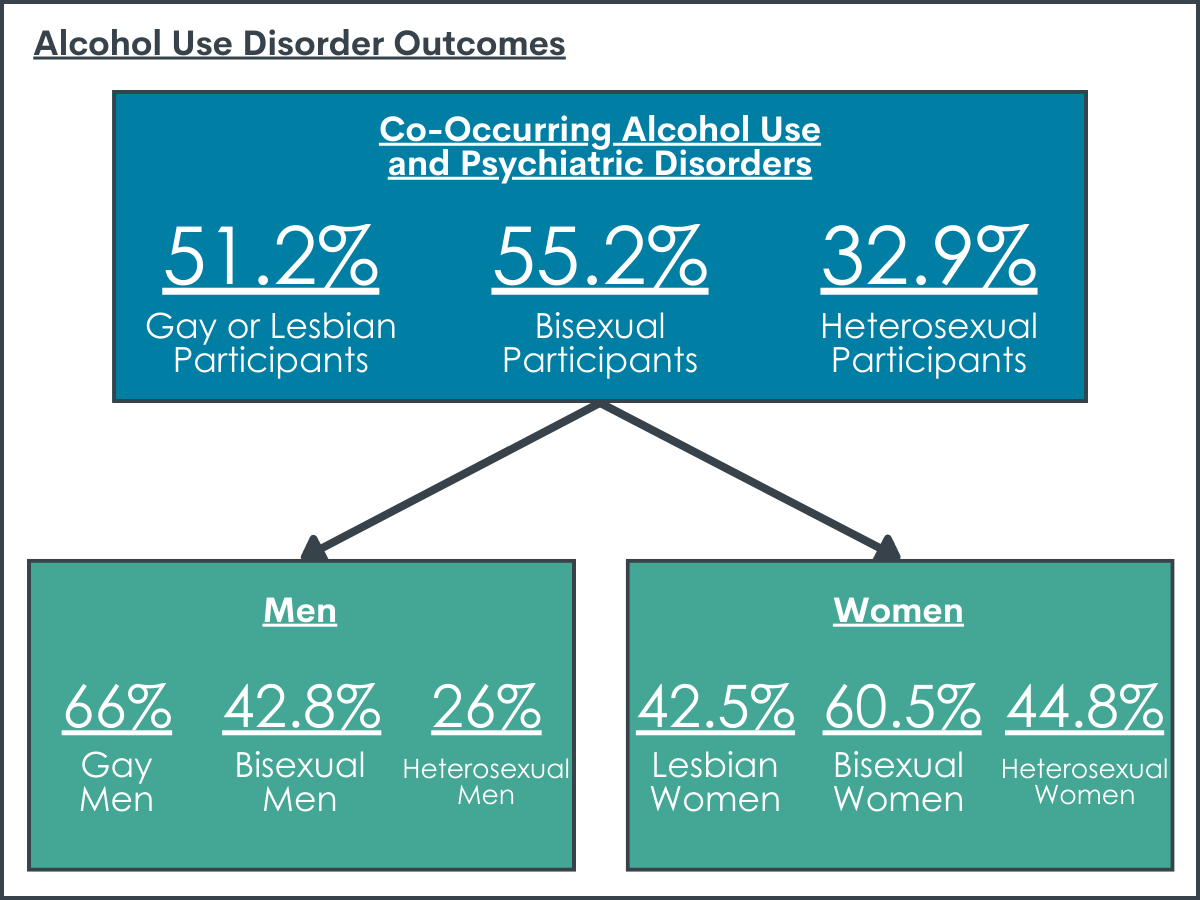
Among those with past-year alcohol or tobacco use disorder, sexually diverse participants had the highest rates of co-occurring psychiatric disorders, with the highest co-occurrence rates among bisexual women.
Alcohol Use Disorder
Co-occurring alcohol use and psychiatric disorders were more prevalent among bisexual (55.2%) and gay or lesbian (51.2%) participants compared with heterosexuals (32.9%).
Men
Gay men (66%) and bisexual men (42.8%) had double the estimated prevalence of co-occurring alcohol and psychiatric disorder compared to heterosexual men (26%).
Women
A majority of bisexual women had a co-occurring alcohol and psychiatric disorder (60.5%), and almost half of heterosexual women (44.6%) and gay or lesbian women (42.5%) had a co-occurring alcohol and psychiatric disorder. More than one-quarter (28.3%) of bisexual women had co-occurring alcohol use disorder and PTSD.
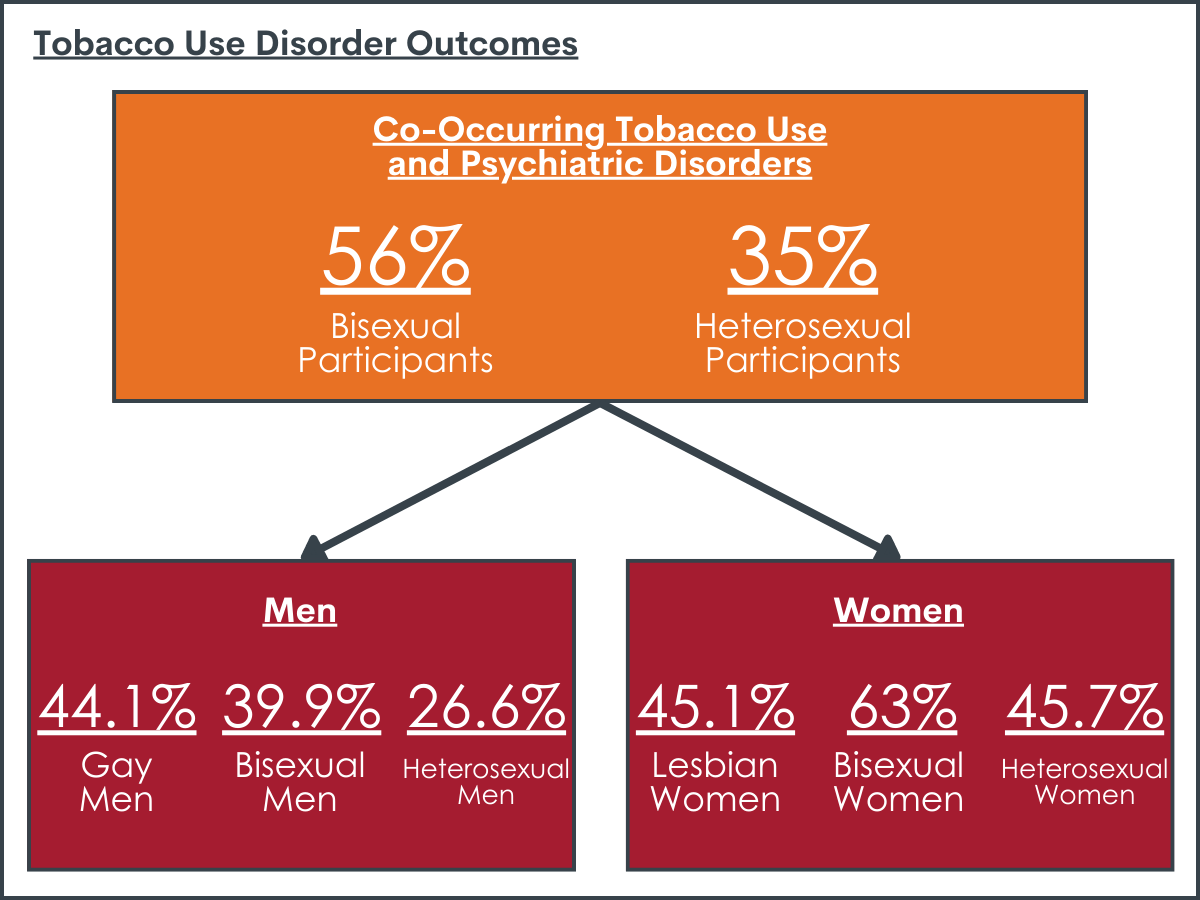
Tobacco Use Disorder
Co-occurring tobacco use and psychiatric disorders were more prevalent among bisexual (56%) participants compared with heterosexuals (35%). Co-occurring tobacco use and anxiety disorders were more prevalent among gay or lesbian (28.3%) participants than among heterosexuals (20.4%).
Men
Bisexual men (39.9%) and gay men (44.1%) had higher rates of co-occurring tobacco use and psychiatric disorder, compared to heterosexual men (26.6%).
Women
A majority of bisexual women (63%) had a co-occurring tobacco use and psychiatric disorder, and almost half of heterosexual women (45.7%) and gay or lesbian women (45.1%) had co-occurring tobacco use and psychiatric disorder.
Greater general- and sexual orientation specific-stress was related to increased rates of past-year co-occurring substance use and psychiatric disorders.
Every additional stressful life event in the past year was associated with a 30-43% increased rate of co-occurring substance use and psychiatric disorder in the overall sample and was associated with a 25-43% increased rate when examining the group of sexually diverse participants. Every additional adverse childhood experience that was reported was associated with an 8-19% increased rate of co-occurring substance use and psychiatric disorder in the overall sample and was associated with a 4-18% increased rate among sexually diverse participants. Finally, every additional event of sexual orientation discrimination experienced in the past year was associated with an 8-10% increased rate of co-occurring substance use and psychiatric disorder.
Social support may help reduce effect of stress on substance use and mental health disorders but only for those with lower levels of stress.
In the overall sample, greater social support was associated with a 2-4% reduced rate of most co-occurring psychiatric disorders. For participants with a greater number of stressful life events, social support was less protective than for those with fewer stressful life events. Among sexually diverse participants, greater social support was associated with a 3-4% reduced rate for only tobacco use and co-occurring anxiety or mood disorder, but not for participants with alcohol use disorder for any of the co-occurring disorder groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Consistent with prior research, this study showed that among adults in the U.S. that met criteria for past-year alcohol or tobacco use disorder, sexually diverse individuals (i.e., gay, lesbian, and bisexual) showed disproportionately high rates of co-occurring psychiatric disorders (i.e., depression, anxiety, and PTSD), compared to heterosexual adults. Bisexual women showed the highest rates of co-occurring psychiatric disorders among the entire sample. In fact, well over half of bisexual women who met criteria for an alcohol or tobacco use disorder had a co-occurring psychiatric disorder.
The current study found that higher rates of co-occurring substance use and psychiatric disorder was associated with greater overall stress. Additionally, sexual orientation specific stress (i.e., sexual orientation discrimination) was associated with higher rates of co-occurring alcohol use disorder and PTSD, as well as tobacco use disorder and mood disorder, over and above the effect of general stress. These findings are consistent with Minority Stress Theory that posits sexually diverse individuals experience societal stigma and discrimination that create more frequent and disproportionate stressors relative to heterosexual individuals, potentially increasing sexually diverse individual’s risk for poor physical and mental health outcomes. However, the nature of these secondary analyses did not allow researchers to empirically test this theory because measures of stress, support, and diagnoses all corresponded to the past year without delineation of which occurred when. That said, these findings highlight the potential importance of structural change (e.g., laws and social norms) that is needed to reduce discrimination, reduce overall stress, and create an environment where stressors are not systematically distributed in a way that overburdens a particular group. Minority Stress Theory also posits that community connection may be a resource that buffers against the negative effects of stigma on poor health outcomes. This study did find an overall reduced rate of co-occurring psychiatric disorder associated with greater social support, but only among individuals with lower levels of stress. While the same caveats for these social support analyses apply like those for the stress analyses, these findings might suggest that social support is indeed helpful, but it cannot fully mitigate the negative effects of stress on psychiatric co-occurrence, and may not help all that much, on average, when stress is very high. It is not clear if social support was more or less helpful for the sexually diverse participants compared to heterosexual participants in the sample, as there were too few sexually diverse participants to perform this level of analysis. However, we may predict that among communities resisting stigma and discrimination, community connection may be particularly helpful in buffering some of the stress caused by such discrimination.
Evidence-based interventions to address sexual minority stress have been developed, such as LGBTQ-affirmative cognitive behavioral therapy, and focus on reducing stigma as it occurs through discriminatory laws policies and prejudice and bolstering coping resources and strategies to mitigate the effect of sexual minority stressors. These interventions show some promise to improve psychological distress, but only a few have been tested in rigorous randomized controlled trials. Mutual-help facilitation can also help LGBTQ+ individuals find LGBTQ-affirmative mutual-help groups and additional social support, like LGBTQ-focused Alcoholic Anonymous meetings, and recommendations for LGBTQ-affirmative SMART Recovery meetings have been recently published.
It was notable the bisexual individuals, and in particular bisexual women, had the highest rates of co-occurring psychiatric disorders overall, with a strikingly high prevalence of PTSD. The prevalence of PTSD among bisexual women may point to underlying stressful and traumatic life events bisexual women experience being important drivers of higher co-occurrence. This is consistent with prior research showing that bisexual individuals had greater alcohol use disorder symptoms, higher rates of co-occurring mood disorder and other drug use disorder, and were more likely to seek treatment, compared to both their gay/lesbian and heterosexual peers. In the National Recovery Study, lesbian, gay and bisexual individuals had higher psychological distress compared to heterosexual individuals. Why are bisexual women, in particular, experiencing these ongoing, salient challenges? As mentioned above, community connection may buffer against minority stress, and bisexual individuals may feel less community connection because of bisexual-specific stigma (i.e., monosexism – a presumption that everyone is, or should be, attracted to no more than one gender) that permeates both the LGBTQ+ community and society at large. Put another way, bisexual individuals may not feel fully accepted in either the LGBTQ+ community, nor by heterosexual individuals, creating even greater stress. This greater stress may be one possible explanation for the high rates of co-occurring disorders seen among bisexual individuals, even compared to gay/lesbian and heterosexual individuals in the current study.
This study was cross-sectional, meaning the researchers are not able to determine a cause-and-effect relationship between stress and co-occurring psychiatric disorders. Longitudinal data would help further uncover the relationships between stress and the development of substance use and co-occurring psychiatric disorders over time.
The researchers were not able to examine differences in the associations between stress and co-occurring psychiatric disorders by sex or sexual identity because sample sizes among sexually diverse participants were too small. This points to the need for national studies to oversample sexually diverse participants to allow for more detailed analyses examining risk and protective factors among subgroups.
Finally, the NESARC-III data do not include information regarding gender identity, and thus the researchers could not examine or control for this in the analysis. It is important that any research, especially national survey research, does not conflate sex and gender so that we can further our understanding of the biopsychosocial underpinnings of addiction and other mental health outcomes. When sex and gender are conflated, it is difficult or nearly impossible to tease apart biological influences from societal and environmental influences on health outcomes. Learn more about the most up to date ways to measure sex, gender identity, and sexual orientation here.
BOTTOM LINE
This study found that among adults in the U.S. from 2012-2013 meeting a past-year alcohol or tobacco use disorder, sexually diverse individuals (gay, lesbian, bisexual or those reporting same-sex attraction or behavior) had disproportionately high rates of co-occurring psychiatric disorders (mood and anxiety disorder, and PTSD) relative to their heterosexual counterparts, where bisexual women had the highest rates in the sample overall. These higher rates of co-occurring psychiatric disorders were associated with high overall stress in the past year, adverse childhood experiences (which obviously predated past year status), and sexual identity discrimination in the past year, which fits with themes inherent within minority stress theory that suggest that underlying stressful life events may be driving these elevated rates of co-occurrence among sexually diverse individuals in the US. Of note, results here highlight particular population sub-groups with high density levels of challenges who may need greater amounts and more specific types of clinical and recovery support services.
For individuals and families seeking recovery: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. Having a supportive community (e.g., friends, family) may help to reduce overall stress and risk for co-occurring psychiatric disorders. Learn more about LGBTQ-affirming AA and resources for family members of people who are LGBTQ+ here.
For treatment professionals and treatment systems: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. If clinicians are cognizant of the challenges faced by LGBTQ+ patients, they can consider these factors as part of their initial assessment and treatment. Learn more about evidence-based LGBTQ-Affirmative therapies to address sexual minority stress here and here. LGBTQ-affirmative mutual-help (e.g., AA, SMART) may another resource for social support.
For scientists:Findings from this secondary analysis of NESARC-III data from 2012-2013 found that sexually diverse participants had significantly higher alcohol and tobacco use disorders with co-occurring psychiatric disorders (mood and anxiety disorders, and PTSD) compared to their heterosexual counterparts, independent of race/ethnicity, education, annual income, urbanicity, and region. Analyses stratified by sex and sexual identity showed particularly high co-occurring disorders for bisexual women. Higher odds of co-occurring psychiatric disorders were significantly associated with greater frequency of past-year stressful life events, adverse childhood experience, and among sexually diverse participants, past-year sexual orientation discrimination. Greater social support was associated with a reduced risk of co-occurring psychiatric disorders, but only for participants with fewer past-year stressful life events. No other interaction analyses were significant. Low sample sizes precluded testing interaction effects by sex or sexual identity. Future national studies should over sample for sexually diverse participants and examine associations among stress and co-occurring psychiatric disorders longitudinally to allow causal inferences to be tested empirically. At the same time, research should focus on developing and testing clinical and public health approaches to remedy both mental health and substance use disorder inequities. While evidence-based psychotherapeutic interventions to address sexual minority stress have been developed with promising results for depression and anxiety, effects on substance use outcomes are minimal. More research is needed to address the effect of sexual minority stress on the development of substance use disorders.
For policy makers: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. Evidence shows that LGBTQ+ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. In fact, research shows that at the state-level, LGBTQ protective policy is associated with better health outcomes for LGBTQ+ people. Policy can support structural interventions to reduce stigma, such as legal protections for LGBTQ+ people in workplace settings, health care, and in schools.
LGBTQ+ populations such as lesbian, gay, and bisexual people report higher rates of alcohol use disorder and co-occurring mood and anxiety disorders compared to heterosexual individuals, with the highest rates among bisexual individuals. In general, bisexual people tend to seek help for alcohol use disorder more frequently than heterosexual people, and more commonly attend Alcoholics Anonymous. At the same time, they also report more barriers to seeking treatment such as fear of judgement from others or not being able to pay for treatment. A large proportion of U.S. adults in recovery from an alcohol or other drug problem are lesbian, gay, or bisexual, who also report higher rates of lifetime co-occurring psychiatric diagnoses, lower quality of life, happiness, self-esteem, and recovery capital compared to heterosexual adults in recovery, independent of how long they have been in recovery. Research can help determine why LGBTQ+ face these greater substance use and mental health challenges, to inform policies and practices tailored to help these at-risk groups.
Minority Stress Theory suggests that LGBTQ+ individuals bear a disproportionate burden of worse mental and physical health outcomes due to the stigmatization of any sexual attraction, gender expression, identity or behavior that does not conform to a heterosexual “norm” and the subsequent stigma-related stressors (so called “minority stress”) LGBTQ+ people face. This “minority stress” includes: a) chronic and accumulating stressors that can be experienced by all individuals, but have documented higher prevalence rates among LGBTQ+ populations, such as adverse childhood experiences and stressful life events; and b) specific discrimination and marginalization society imposes because of LGBTQ+ individual’s sexual orientation and/or gender identity – creating an increased risk or burden of worse mental and physical health outcomes compared to heterosexual peers.
Although research on the prevalence of substance use and mental health disorders among LGBTQ+ populations is growing, few studies have examined the co-occurrence of substance use disorders and psychiatric disorders among LGBTQ+ populations in a nationally representative sample, nor tested associations with stress. For example, another study found that sexually diverse participants had higher rates of alcohol and tobacco use disorders, and more severe disorder symptoms, with the highest rates among bisexual adults. The current study adds to this work by examining the prevalence of co-occurring alcohol and tobacco use disorders with mood and anxiety disorders, by sex and sexual identity, and how general (recent stressful life events, adverse childhood experiences) and specific (recent sexual orientation discrimination) stressors are related to the prevalence of these co-occurring disorders. Examining the prevalence of co-occurring substance use and psychiatric disorders among gay, lesbian, and bisexual men and women compared to heterosexual men and women, and associations with stress, can provide further support for Minority Stress Theory, highlighting potential areas for intervention to reduce risks of substance use and psychiatric disorder.
This study uses U.S. national survey data from 2012-2013 to examine three research questions: 1. What are the prevalence rates of alcohol and tobacco use disorder with co-occurring psychiatric disorder among sexually diverse men and women compared to heterosexual men and women? 2. What kinds of stressors and support are associated with such rates of co-occurring substance use and psychiatric disorders among men and women generally? 3. What kinds of stressors and support are associated with rates of co-occurring substance use and psychiatric disorders among sexually diverse men and women specifically? Focusing on experiences of LGBTQ+ individuals with substance use disorder that can be addressed therapeutically, such as co-occurring disorders, can help inform comprehensive strategies to improve the lives of these at-risk groups.
HOW WAS THIS STUDY CONDUCTED?
This study used the U.S. National Epidemiologic Survey on Alcohol and Related Conditions (NESARC)-III data from 2012-2013 to examine: (1) the prevalence of co-occurring psychiatric, alcohol, and tobacco use disorders among adults (N = 36,309) stratified by sexual orientation (gay or lesbian, bisexual, heterosexual) and sex (women and men); (2) general stressors and support associated with co-occurring substance use and psychiatric disorders among men and women, including stressful life events, adverse childhood experiences, and social support; (3) general and specific stressors and support associated with co-occurring substance use and psychiatric disorders among sexually diverse men and women.
Participants in this study included noninstitutionalized civilian adults in the U.S. ages 18 and older surveyed via in-person interviews who had available sexual identity data. Past-year alcohol use disorder, tobacco use disorder, and co-occurring psychiatric disorders were assessed using DSM-5 diagnostic criteria with a commonly used, well-validated structured interview. Co-occurring psychiatric disorders included: past-year mood disorder (i.e., major depressive disorder, bipolar I and II disorder, and dysthymia); past-year anxiety disorder (i.e., generalized anxiety disorder, specific phobia, social anxiety disorder, panic disorder, and agoraphobia); and past-year post-traumatic stress disorder (PTSD). Participants were also asked about past-year stressors that included 16 life events (e.g., moved, lost employment, divorced), adverse childhood experiences that included 18 question items (e.g., physical, sexual, and emotional abuse; exposure to family violence; parental incarceration), and social support using 12 questions. Sexually diverse participants were also asked about 6 different types of sexual orientation discrimination (e.g., discrimination in health care settings, public settings, and obtaining a job). Actual questionnaire items from the NESARC-III study can be found here.
The analyses first examined the prevalence of alcohol use disorder, tobacco use disorder, mood disorders, anxiety disorders, and PTSD using the full sample, separated by sex (men and women) and sexual identity (gay or lesbian, bisexual, or heterosexual) to show differences in the prevalence rates across groups. Then the analyses estimated the prevalence of co-occurring mood, anxiety, or PTSD among those participants in the sample who met criteria for past-year alcohol use disorder (N=5,042) and past-year tobacco use disorder (N=7,188), by sex (men and women) and sexual identity (gay or lesbian, bisexual, or heterosexual) to show differences in the prevalence rates of co-occurring disorders across groups. Finally, they examined the associations between general stressors (stressful life events, adverse childhood experiences), social support, and co-occurring disorders in the full sample. Then they examined the associations between both general (stressful life events, adverse childhood experiences) and specific stressors (sexual orientation discrimination) and social support only among sexually diverse participants. These analyses also examined whether social support might buffer any effects of stressors or adverse childhood experiences on substance use and mental health disorders. They did not test whether social support might buffer risks from stressors and adverse childhood experiences in the sample of only sexually diverse participants compared to heterosexual participants in the sample, as there were too few sexually diverse participants to perform this analysis. Nor could they test whether any buffering conferred by social support was different for sexual minority versus heterosexual participants.
Sexually diverse participants included those who identified as gay or lesbian, bisexual, or individuals who identified as heterosexual but reported same sex attraction or behavior (N=3,203). All analyses controlled for demographic variables that could also influence the prevalence of co-occurring substance use and psychiatric disorders in order to estimate the specific effect of stress and social support on the prevalence of such co-occurring disorders among sexually diverse and heterosexual men and women: race/ethnicity (White non-Hispanic, Black non-Hispanic, American Indian/Alaska Native non-Hispanic, Asian/Native Hawaiian/Other Pacific Islander non-Hispanic, and Hispanic), education (high school diploma or more, or less than a high school diploma), annual income (<$25,000, $25,000–$59,999, >$60,000), urbanicity (urban or rural), and region (Northeast, Midwest, South, and West).
WHAT DID THIS STUDY FIND?
Sexually diverse participants had the highest rates of alcohol and tobacco use disorders, mood and anxiety disorders, and PTSD.
Among the full sample, when examining disorders independently, sexually diverse participants had higher rates of past-year alcohol use disorder, tobacco use disorder, anxiety disorders, mood disorders, and PTSD, compared to heterosexual participants. Bisexual individuals had a fourfold greater prevalence of PTSD (17.9%) compared to heterosexual individuals (4.4%).
Men
Among men, gay men had a higher prevalence of past-year alcohol use disorder (31.4%) and tobacco use disorder (40.8%) compared with the overall sample (13.8%, 12%, respectively). Both gay men and bisexual men had a significantly higher prevalence of all disorders compared with heterosexual men.
Women
Among women, gay or lesbian women had a higher prevalence of alcohol use disorder (25%), tobacco use disorder (27%), and mood disorders (24%) compared with heterosexual women (10%, 16%, 15%, respectively). Bisexual women had a particularly high prevalence of anxiety disorders (32.5%), mood disorders (34.9%), and PTSD (21.0%), compared with the overall sample (13%, 12.8%, and 5.6%, respectively), and a significantly higher prevalence of alcohol (30%) and tobacco use disorders (36%), compared with heterosexual women (10%, 16%, respectively).
Among those with past-year alcohol or tobacco use disorder, sexually diverse participants had the highest rates of co-occurring psychiatric disorders, with the highest co-occurrence rates among bisexual women.
Alcohol Use Disorder
Co-occurring alcohol use and psychiatric disorders were more prevalent among bisexual (55.2%) and gay or lesbian (51.2%) participants compared with heterosexuals (32.9%).
Men
Gay men (66%) and bisexual men (42.8%) had double the estimated prevalence of co-occurring alcohol and psychiatric disorder compared to heterosexual men (26%).
Women
A majority of bisexual women had a co-occurring alcohol and psychiatric disorder (60.5%), and almost half of heterosexual women (44.6%) and gay or lesbian women (42.5%) had a co-occurring alcohol and psychiatric disorder. More than one-quarter (28.3%) of bisexual women had co-occurring alcohol use disorder and PTSD.
Tobacco Use Disorder
Co-occurring tobacco use and psychiatric disorders were more prevalent among bisexual (56%) participants compared with heterosexuals (35%). Co-occurring tobacco use and anxiety disorders were more prevalent among gay or lesbian (28.3%) participants than among heterosexuals (20.4%).
Men
Bisexual men (39.9%) and gay men (44.1%) had higher rates of co-occurring tobacco use and psychiatric disorder, compared to heterosexual men (26.6%).
Women
A majority of bisexual women (63%) had a co-occurring tobacco use and psychiatric disorder, and almost half of heterosexual women (45.7%) and gay or lesbian women (45.1%) had co-occurring tobacco use and psychiatric disorder.
Greater general- and sexual orientation specific-stress was related to increased rates of past-year co-occurring substance use and psychiatric disorders.
Every additional stressful life event in the past year was associated with a 30-43% increased rate of co-occurring substance use and psychiatric disorder in the overall sample and was associated with a 25-43% increased rate when examining the group of sexually diverse participants. Every additional adverse childhood experience that was reported was associated with an 8-19% increased rate of co-occurring substance use and psychiatric disorder in the overall sample and was associated with a 4-18% increased rate among sexually diverse participants. Finally, every additional event of sexual orientation discrimination experienced in the past year was associated with an 8-10% increased rate of co-occurring substance use and psychiatric disorder.
Social support may help reduce effect of stress on substance use and mental health disorders but only for those with lower levels of stress.
In the overall sample, greater social support was associated with a 2-4% reduced rate of most co-occurring psychiatric disorders. For participants with a greater number of stressful life events, social support was less protective than for those with fewer stressful life events. Among sexually diverse participants, greater social support was associated with a 3-4% reduced rate for only tobacco use and co-occurring anxiety or mood disorder, but not for participants with alcohol use disorder for any of the co-occurring disorder groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Consistent with prior research, this study showed that among adults in the U.S. that met criteria for past-year alcohol or tobacco use disorder, sexually diverse individuals (i.e., gay, lesbian, and bisexual) showed disproportionately high rates of co-occurring psychiatric disorders (i.e., depression, anxiety, and PTSD), compared to heterosexual adults. Bisexual women showed the highest rates of co-occurring psychiatric disorders among the entire sample. In fact, well over half of bisexual women who met criteria for an alcohol or tobacco use disorder had a co-occurring psychiatric disorder.
The current study found that higher rates of co-occurring substance use and psychiatric disorder was associated with greater overall stress. Additionally, sexual orientation specific stress (i.e., sexual orientation discrimination) was associated with higher rates of co-occurring alcohol use disorder and PTSD, as well as tobacco use disorder and mood disorder, over and above the effect of general stress. These findings are consistent with Minority Stress Theory that posits sexually diverse individuals experience societal stigma and discrimination that create more frequent and disproportionate stressors relative to heterosexual individuals, potentially increasing sexually diverse individual’s risk for poor physical and mental health outcomes. However, the nature of these secondary analyses did not allow researchers to empirically test this theory because measures of stress, support, and diagnoses all corresponded to the past year without delineation of which occurred when. That said, these findings highlight the potential importance of structural change (e.g., laws and social norms) that is needed to reduce discrimination, reduce overall stress, and create an environment where stressors are not systematically distributed in a way that overburdens a particular group. Minority Stress Theory also posits that community connection may be a resource that buffers against the negative effects of stigma on poor health outcomes. This study did find an overall reduced rate of co-occurring psychiatric disorder associated with greater social support, but only among individuals with lower levels of stress. While the same caveats for these social support analyses apply like those for the stress analyses, these findings might suggest that social support is indeed helpful, but it cannot fully mitigate the negative effects of stress on psychiatric co-occurrence, and may not help all that much, on average, when stress is very high. It is not clear if social support was more or less helpful for the sexually diverse participants compared to heterosexual participants in the sample, as there were too few sexually diverse participants to perform this level of analysis. However, we may predict that among communities resisting stigma and discrimination, community connection may be particularly helpful in buffering some of the stress caused by such discrimination.
Evidence-based interventions to address sexual minority stress have been developed, such as LGBTQ-affirmative cognitive behavioral therapy, and focus on reducing stigma as it occurs through discriminatory laws policies and prejudice and bolstering coping resources and strategies to mitigate the effect of sexual minority stressors. These interventions show some promise to improve psychological distress, but only a few have been tested in rigorous randomized controlled trials. Mutual-help facilitation can also help LGBTQ+ individuals find LGBTQ-affirmative mutual-help groups and additional social support, like LGBTQ-focused Alcoholic Anonymous meetings, and recommendations for LGBTQ-affirmative SMART Recovery meetings have been recently published.
It was notable the bisexual individuals, and in particular bisexual women, had the highest rates of co-occurring psychiatric disorders overall, with a strikingly high prevalence of PTSD. The prevalence of PTSD among bisexual women may point to underlying stressful and traumatic life events bisexual women experience being important drivers of higher co-occurrence. This is consistent with prior research showing that bisexual individuals had greater alcohol use disorder symptoms, higher rates of co-occurring mood disorder and other drug use disorder, and were more likely to seek treatment, compared to both their gay/lesbian and heterosexual peers. In the National Recovery Study, lesbian, gay and bisexual individuals had higher psychological distress compared to heterosexual individuals. Why are bisexual women, in particular, experiencing these ongoing, salient challenges? As mentioned above, community connection may buffer against minority stress, and bisexual individuals may feel less community connection because of bisexual-specific stigma (i.e., monosexism – a presumption that everyone is, or should be, attracted to no more than one gender) that permeates both the LGBTQ+ community and society at large. Put another way, bisexual individuals may not feel fully accepted in either the LGBTQ+ community, nor by heterosexual individuals, creating even greater stress. This greater stress may be one possible explanation for the high rates of co-occurring disorders seen among bisexual individuals, even compared to gay/lesbian and heterosexual individuals in the current study.
This study was cross-sectional, meaning the researchers are not able to determine a cause-and-effect relationship between stress and co-occurring psychiatric disorders. Longitudinal data would help further uncover the relationships between stress and the development of substance use and co-occurring psychiatric disorders over time.
The researchers were not able to examine differences in the associations between stress and co-occurring psychiatric disorders by sex or sexual identity because sample sizes among sexually diverse participants were too small. This points to the need for national studies to oversample sexually diverse participants to allow for more detailed analyses examining risk and protective factors among subgroups.
Finally, the NESARC-III data do not include information regarding gender identity, and thus the researchers could not examine or control for this in the analysis. It is important that any research, especially national survey research, does not conflate sex and gender so that we can further our understanding of the biopsychosocial underpinnings of addiction and other mental health outcomes. When sex and gender are conflated, it is difficult or nearly impossible to tease apart biological influences from societal and environmental influences on health outcomes. Learn more about the most up to date ways to measure sex, gender identity, and sexual orientation here.
BOTTOM LINE
This study found that among adults in the U.S. from 2012-2013 meeting a past-year alcohol or tobacco use disorder, sexually diverse individuals (gay, lesbian, bisexual or those reporting same-sex attraction or behavior) had disproportionately high rates of co-occurring psychiatric disorders (mood and anxiety disorder, and PTSD) relative to their heterosexual counterparts, where bisexual women had the highest rates in the sample overall. These higher rates of co-occurring psychiatric disorders were associated with high overall stress in the past year, adverse childhood experiences (which obviously predated past year status), and sexual identity discrimination in the past year, which fits with themes inherent within minority stress theory that suggest that underlying stressful life events may be driving these elevated rates of co-occurrence among sexually diverse individuals in the US. Of note, results here highlight particular population sub-groups with high density levels of challenges who may need greater amounts and more specific types of clinical and recovery support services.
For individuals and families seeking recovery: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. Having a supportive community (e.g., friends, family) may help to reduce overall stress and risk for co-occurring psychiatric disorders. Learn more about LGBTQ-affirming AA and resources for family members of people who are LGBTQ+ here.
For treatment professionals and treatment systems: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. If clinicians are cognizant of the challenges faced by LGBTQ+ patients, they can consider these factors as part of their initial assessment and treatment. Learn more about evidence-based LGBTQ-Affirmative therapies to address sexual minority stress here and here. LGBTQ-affirmative mutual-help (e.g., AA, SMART) may another resource for social support.
For scientists:Findings from this secondary analysis of NESARC-III data from 2012-2013 found that sexually diverse participants had significantly higher alcohol and tobacco use disorders with co-occurring psychiatric disorders (mood and anxiety disorders, and PTSD) compared to their heterosexual counterparts, independent of race/ethnicity, education, annual income, urbanicity, and region. Analyses stratified by sex and sexual identity showed particularly high co-occurring disorders for bisexual women. Higher odds of co-occurring psychiatric disorders were significantly associated with greater frequency of past-year stressful life events, adverse childhood experience, and among sexually diverse participants, past-year sexual orientation discrimination. Greater social support was associated with a reduced risk of co-occurring psychiatric disorders, but only for participants with fewer past-year stressful life events. No other interaction analyses were significant. Low sample sizes precluded testing interaction effects by sex or sexual identity. Future national studies should over sample for sexually diverse participants and examine associations among stress and co-occurring psychiatric disorders longitudinally to allow causal inferences to be tested empirically. At the same time, research should focus on developing and testing clinical and public health approaches to remedy both mental health and substance use disorder inequities. While evidence-based psychotherapeutic interventions to address sexual minority stress have been developed with promising results for depression and anxiety, effects on substance use outcomes are minimal. More research is needed to address the effect of sexual minority stress on the development of substance use disorders.
For policy makers: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. Evidence shows that LGBTQ+ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. In fact, research shows that at the state-level, LGBTQ protective policy is associated with better health outcomes for LGBTQ+ people. Policy can support structural interventions to reduce stigma, such as legal protections for LGBTQ+ people in workplace settings, health care, and in schools.
LGBTQ+ populations such as lesbian, gay, and bisexual people report higher rates of alcohol use disorder and co-occurring mood and anxiety disorders compared to heterosexual individuals, with the highest rates among bisexual individuals. In general, bisexual people tend to seek help for alcohol use disorder more frequently than heterosexual people, and more commonly attend Alcoholics Anonymous. At the same time, they also report more barriers to seeking treatment such as fear of judgement from others or not being able to pay for treatment. A large proportion of U.S. adults in recovery from an alcohol or other drug problem are lesbian, gay, or bisexual, who also report higher rates of lifetime co-occurring psychiatric diagnoses, lower quality of life, happiness, self-esteem, and recovery capital compared to heterosexual adults in recovery, independent of how long they have been in recovery. Research can help determine why LGBTQ+ face these greater substance use and mental health challenges, to inform policies and practices tailored to help these at-risk groups.
Minority Stress Theory suggests that LGBTQ+ individuals bear a disproportionate burden of worse mental and physical health outcomes due to the stigmatization of any sexual attraction, gender expression, identity or behavior that does not conform to a heterosexual “norm” and the subsequent stigma-related stressors (so called “minority stress”) LGBTQ+ people face. This “minority stress” includes: a) chronic and accumulating stressors that can be experienced by all individuals, but have documented higher prevalence rates among LGBTQ+ populations, such as adverse childhood experiences and stressful life events; and b) specific discrimination and marginalization society imposes because of LGBTQ+ individual’s sexual orientation and/or gender identity – creating an increased risk or burden of worse mental and physical health outcomes compared to heterosexual peers.
Although research on the prevalence of substance use and mental health disorders among LGBTQ+ populations is growing, few studies have examined the co-occurrence of substance use disorders and psychiatric disorders among LGBTQ+ populations in a nationally representative sample, nor tested associations with stress. For example, another study found that sexually diverse participants had higher rates of alcohol and tobacco use disorders, and more severe disorder symptoms, with the highest rates among bisexual adults. The current study adds to this work by examining the prevalence of co-occurring alcohol and tobacco use disorders with mood and anxiety disorders, by sex and sexual identity, and how general (recent stressful life events, adverse childhood experiences) and specific (recent sexual orientation discrimination) stressors are related to the prevalence of these co-occurring disorders. Examining the prevalence of co-occurring substance use and psychiatric disorders among gay, lesbian, and bisexual men and women compared to heterosexual men and women, and associations with stress, can provide further support for Minority Stress Theory, highlighting potential areas for intervention to reduce risks of substance use and psychiatric disorder.
This study uses U.S. national survey data from 2012-2013 to examine three research questions: 1. What are the prevalence rates of alcohol and tobacco use disorder with co-occurring psychiatric disorder among sexually diverse men and women compared to heterosexual men and women? 2. What kinds of stressors and support are associated with such rates of co-occurring substance use and psychiatric disorders among men and women generally? 3. What kinds of stressors and support are associated with rates of co-occurring substance use and psychiatric disorders among sexually diverse men and women specifically? Focusing on experiences of LGBTQ+ individuals with substance use disorder that can be addressed therapeutically, such as co-occurring disorders, can help inform comprehensive strategies to improve the lives of these at-risk groups.
HOW WAS THIS STUDY CONDUCTED?
This study used the U.S. National Epidemiologic Survey on Alcohol and Related Conditions (NESARC)-III data from 2012-2013 to examine: (1) the prevalence of co-occurring psychiatric, alcohol, and tobacco use disorders among adults (N = 36,309) stratified by sexual orientation (gay or lesbian, bisexual, heterosexual) and sex (women and men); (2) general stressors and support associated with co-occurring substance use and psychiatric disorders among men and women, including stressful life events, adverse childhood experiences, and social support; (3) general and specific stressors and support associated with co-occurring substance use and psychiatric disorders among sexually diverse men and women.
Participants in this study included noninstitutionalized civilian adults in the U.S. ages 18 and older surveyed via in-person interviews who had available sexual identity data. Past-year alcohol use disorder, tobacco use disorder, and co-occurring psychiatric disorders were assessed using DSM-5 diagnostic criteria with a commonly used, well-validated structured interview. Co-occurring psychiatric disorders included: past-year mood disorder (i.e., major depressive disorder, bipolar I and II disorder, and dysthymia); past-year anxiety disorder (i.e., generalized anxiety disorder, specific phobia, social anxiety disorder, panic disorder, and agoraphobia); and past-year post-traumatic stress disorder (PTSD). Participants were also asked about past-year stressors that included 16 life events (e.g., moved, lost employment, divorced), adverse childhood experiences that included 18 question items (e.g., physical, sexual, and emotional abuse; exposure to family violence; parental incarceration), and social support using 12 questions. Sexually diverse participants were also asked about 6 different types of sexual orientation discrimination (e.g., discrimination in health care settings, public settings, and obtaining a job). Actual questionnaire items from the NESARC-III study can be found here.
The analyses first examined the prevalence of alcohol use disorder, tobacco use disorder, mood disorders, anxiety disorders, and PTSD using the full sample, separated by sex (men and women) and sexual identity (gay or lesbian, bisexual, or heterosexual) to show differences in the prevalence rates across groups. Then the analyses estimated the prevalence of co-occurring mood, anxiety, or PTSD among those participants in the sample who met criteria for past-year alcohol use disorder (N=5,042) and past-year tobacco use disorder (N=7,188), by sex (men and women) and sexual identity (gay or lesbian, bisexual, or heterosexual) to show differences in the prevalence rates of co-occurring disorders across groups. Finally, they examined the associations between general stressors (stressful life events, adverse childhood experiences), social support, and co-occurring disorders in the full sample. Then they examined the associations between both general (stressful life events, adverse childhood experiences) and specific stressors (sexual orientation discrimination) and social support only among sexually diverse participants. These analyses also examined whether social support might buffer any effects of stressors or adverse childhood experiences on substance use and mental health disorders. They did not test whether social support might buffer risks from stressors and adverse childhood experiences in the sample of only sexually diverse participants compared to heterosexual participants in the sample, as there were too few sexually diverse participants to perform this analysis. Nor could they test whether any buffering conferred by social support was different for sexual minority versus heterosexual participants.
Sexually diverse participants included those who identified as gay or lesbian, bisexual, or individuals who identified as heterosexual but reported same sex attraction or behavior (N=3,203). All analyses controlled for demographic variables that could also influence the prevalence of co-occurring substance use and psychiatric disorders in order to estimate the specific effect of stress and social support on the prevalence of such co-occurring disorders among sexually diverse and heterosexual men and women: race/ethnicity (White non-Hispanic, Black non-Hispanic, American Indian/Alaska Native non-Hispanic, Asian/Native Hawaiian/Other Pacific Islander non-Hispanic, and Hispanic), education (high school diploma or more, or less than a high school diploma), annual income (<$25,000, $25,000–$59,999, >$60,000), urbanicity (urban or rural), and region (Northeast, Midwest, South, and West).
WHAT DID THIS STUDY FIND?
Sexually diverse participants had the highest rates of alcohol and tobacco use disorders, mood and anxiety disorders, and PTSD.
Among the full sample, when examining disorders independently, sexually diverse participants had higher rates of past-year alcohol use disorder, tobacco use disorder, anxiety disorders, mood disorders, and PTSD, compared to heterosexual participants. Bisexual individuals had a fourfold greater prevalence of PTSD (17.9%) compared to heterosexual individuals (4.4%).
Men
Among men, gay men had a higher prevalence of past-year alcohol use disorder (31.4%) and tobacco use disorder (40.8%) compared with the overall sample (13.8%, 12%, respectively). Both gay men and bisexual men had a significantly higher prevalence of all disorders compared with heterosexual men.
Women
Among women, gay or lesbian women had a higher prevalence of alcohol use disorder (25%), tobacco use disorder (27%), and mood disorders (24%) compared with heterosexual women (10%, 16%, 15%, respectively). Bisexual women had a particularly high prevalence of anxiety disorders (32.5%), mood disorders (34.9%), and PTSD (21.0%), compared with the overall sample (13%, 12.8%, and 5.6%, respectively), and a significantly higher prevalence of alcohol (30%) and tobacco use disorders (36%), compared with heterosexual women (10%, 16%, respectively).
Among those with past-year alcohol or tobacco use disorder, sexually diverse participants had the highest rates of co-occurring psychiatric disorders, with the highest co-occurrence rates among bisexual women.
Alcohol Use Disorder
Co-occurring alcohol use and psychiatric disorders were more prevalent among bisexual (55.2%) and gay or lesbian (51.2%) participants compared with heterosexuals (32.9%).
Men
Gay men (66%) and bisexual men (42.8%) had double the estimated prevalence of co-occurring alcohol and psychiatric disorder compared to heterosexual men (26%).
Women
A majority of bisexual women had a co-occurring alcohol and psychiatric disorder (60.5%), and almost half of heterosexual women (44.6%) and gay or lesbian women (42.5%) had a co-occurring alcohol and psychiatric disorder. More than one-quarter (28.3%) of bisexual women had co-occurring alcohol use disorder and PTSD.
Tobacco Use Disorder
Co-occurring tobacco use and psychiatric disorders were more prevalent among bisexual (56%) participants compared with heterosexuals (35%). Co-occurring tobacco use and anxiety disorders were more prevalent among gay or lesbian (28.3%) participants than among heterosexuals (20.4%).
Men
Bisexual men (39.9%) and gay men (44.1%) had higher rates of co-occurring tobacco use and psychiatric disorder, compared to heterosexual men (26.6%).
Women
A majority of bisexual women (63%) had a co-occurring tobacco use and psychiatric disorder, and almost half of heterosexual women (45.7%) and gay or lesbian women (45.1%) had co-occurring tobacco use and psychiatric disorder.
Greater general- and sexual orientation specific-stress was related to increased rates of past-year co-occurring substance use and psychiatric disorders.
Every additional stressful life event in the past year was associated with a 30-43% increased rate of co-occurring substance use and psychiatric disorder in the overall sample and was associated with a 25-43% increased rate when examining the group of sexually diverse participants. Every additional adverse childhood experience that was reported was associated with an 8-19% increased rate of co-occurring substance use and psychiatric disorder in the overall sample and was associated with a 4-18% increased rate among sexually diverse participants. Finally, every additional event of sexual orientation discrimination experienced in the past year was associated with an 8-10% increased rate of co-occurring substance use and psychiatric disorder.
Social support may help reduce effect of stress on substance use and mental health disorders but only for those with lower levels of stress.
In the overall sample, greater social support was associated with a 2-4% reduced rate of most co-occurring psychiatric disorders. For participants with a greater number of stressful life events, social support was less protective than for those with fewer stressful life events. Among sexually diverse participants, greater social support was associated with a 3-4% reduced rate for only tobacco use and co-occurring anxiety or mood disorder, but not for participants with alcohol use disorder for any of the co-occurring disorder groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Consistent with prior research, this study showed that among adults in the U.S. that met criteria for past-year alcohol or tobacco use disorder, sexually diverse individuals (i.e., gay, lesbian, and bisexual) showed disproportionately high rates of co-occurring psychiatric disorders (i.e., depression, anxiety, and PTSD), compared to heterosexual adults. Bisexual women showed the highest rates of co-occurring psychiatric disorders among the entire sample. In fact, well over half of bisexual women who met criteria for an alcohol or tobacco use disorder had a co-occurring psychiatric disorder.
The current study found that higher rates of co-occurring substance use and psychiatric disorder was associated with greater overall stress. Additionally, sexual orientation specific stress (i.e., sexual orientation discrimination) was associated with higher rates of co-occurring alcohol use disorder and PTSD, as well as tobacco use disorder and mood disorder, over and above the effect of general stress. These findings are consistent with Minority Stress Theory that posits sexually diverse individuals experience societal stigma and discrimination that create more frequent and disproportionate stressors relative to heterosexual individuals, potentially increasing sexually diverse individual’s risk for poor physical and mental health outcomes. However, the nature of these secondary analyses did not allow researchers to empirically test this theory because measures of stress, support, and diagnoses all corresponded to the past year without delineation of which occurred when. That said, these findings highlight the potential importance of structural change (e.g., laws and social norms) that is needed to reduce discrimination, reduce overall stress, and create an environment where stressors are not systematically distributed in a way that overburdens a particular group. Minority Stress Theory also posits that community connection may be a resource that buffers against the negative effects of stigma on poor health outcomes. This study did find an overall reduced rate of co-occurring psychiatric disorder associated with greater social support, but only among individuals with lower levels of stress. While the same caveats for these social support analyses apply like those for the stress analyses, these findings might suggest that social support is indeed helpful, but it cannot fully mitigate the negative effects of stress on psychiatric co-occurrence, and may not help all that much, on average, when stress is very high. It is not clear if social support was more or less helpful for the sexually diverse participants compared to heterosexual participants in the sample, as there were too few sexually diverse participants to perform this level of analysis. However, we may predict that among communities resisting stigma and discrimination, community connection may be particularly helpful in buffering some of the stress caused by such discrimination.
Evidence-based interventions to address sexual minority stress have been developed, such as LGBTQ-affirmative cognitive behavioral therapy, and focus on reducing stigma as it occurs through discriminatory laws policies and prejudice and bolstering coping resources and strategies to mitigate the effect of sexual minority stressors. These interventions show some promise to improve psychological distress, but only a few have been tested in rigorous randomized controlled trials. Mutual-help facilitation can also help LGBTQ+ individuals find LGBTQ-affirmative mutual-help groups and additional social support, like LGBTQ-focused Alcoholic Anonymous meetings, and recommendations for LGBTQ-affirmative SMART Recovery meetings have been recently published.
It was notable the bisexual individuals, and in particular bisexual women, had the highest rates of co-occurring psychiatric disorders overall, with a strikingly high prevalence of PTSD. The prevalence of PTSD among bisexual women may point to underlying stressful and traumatic life events bisexual women experience being important drivers of higher co-occurrence. This is consistent with prior research showing that bisexual individuals had greater alcohol use disorder symptoms, higher rates of co-occurring mood disorder and other drug use disorder, and were more likely to seek treatment, compared to both their gay/lesbian and heterosexual peers. In the National Recovery Study, lesbian, gay and bisexual individuals had higher psychological distress compared to heterosexual individuals. Why are bisexual women, in particular, experiencing these ongoing, salient challenges? As mentioned above, community connection may buffer against minority stress, and bisexual individuals may feel less community connection because of bisexual-specific stigma (i.e., monosexism – a presumption that everyone is, or should be, attracted to no more than one gender) that permeates both the LGBTQ+ community and society at large. Put another way, bisexual individuals may not feel fully accepted in either the LGBTQ+ community, nor by heterosexual individuals, creating even greater stress. This greater stress may be one possible explanation for the high rates of co-occurring disorders seen among bisexual individuals, even compared to gay/lesbian and heterosexual individuals in the current study.
This study was cross-sectional, meaning the researchers are not able to determine a cause-and-effect relationship between stress and co-occurring psychiatric disorders. Longitudinal data would help further uncover the relationships between stress and the development of substance use and co-occurring psychiatric disorders over time.
The researchers were not able to examine differences in the associations between stress and co-occurring psychiatric disorders by sex or sexual identity because sample sizes among sexually diverse participants were too small. This points to the need for national studies to oversample sexually diverse participants to allow for more detailed analyses examining risk and protective factors among subgroups.
Finally, the NESARC-III data do not include information regarding gender identity, and thus the researchers could not examine or control for this in the analysis. It is important that any research, especially national survey research, does not conflate sex and gender so that we can further our understanding of the biopsychosocial underpinnings of addiction and other mental health outcomes. When sex and gender are conflated, it is difficult or nearly impossible to tease apart biological influences from societal and environmental influences on health outcomes. Learn more about the most up to date ways to measure sex, gender identity, and sexual orientation here.
BOTTOM LINE
This study found that among adults in the U.S. from 2012-2013 meeting a past-year alcohol or tobacco use disorder, sexually diverse individuals (gay, lesbian, bisexual or those reporting same-sex attraction or behavior) had disproportionately high rates of co-occurring psychiatric disorders (mood and anxiety disorder, and PTSD) relative to their heterosexual counterparts, where bisexual women had the highest rates in the sample overall. These higher rates of co-occurring psychiatric disorders were associated with high overall stress in the past year, adverse childhood experiences (which obviously predated past year status), and sexual identity discrimination in the past year, which fits with themes inherent within minority stress theory that suggest that underlying stressful life events may be driving these elevated rates of co-occurrence among sexually diverse individuals in the US. Of note, results here highlight particular population sub-groups with high density levels of challenges who may need greater amounts and more specific types of clinical and recovery support services.
For individuals and families seeking recovery: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. Having a supportive community (e.g., friends, family) may help to reduce overall stress and risk for co-occurring psychiatric disorders. Learn more about LGBTQ-affirming AA and resources for family members of people who are LGBTQ+ here.
For treatment professionals and treatment systems: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. If clinicians are cognizant of the challenges faced by LGBTQ+ patients, they can consider these factors as part of their initial assessment and treatment. Learn more about evidence-based LGBTQ-Affirmative therapies to address sexual minority stress here and here. LGBTQ-affirmative mutual-help (e.g., AA, SMART) may another resource for social support.
For scientists:Findings from this secondary analysis of NESARC-III data from 2012-2013 found that sexually diverse participants had significantly higher alcohol and tobacco use disorders with co-occurring psychiatric disorders (mood and anxiety disorders, and PTSD) compared to their heterosexual counterparts, independent of race/ethnicity, education, annual income, urbanicity, and region. Analyses stratified by sex and sexual identity showed particularly high co-occurring disorders for bisexual women. Higher odds of co-occurring psychiatric disorders were significantly associated with greater frequency of past-year stressful life events, adverse childhood experience, and among sexually diverse participants, past-year sexual orientation discrimination. Greater social support was associated with a reduced risk of co-occurring psychiatric disorders, but only for participants with fewer past-year stressful life events. No other interaction analyses were significant. Low sample sizes precluded testing interaction effects by sex or sexual identity. Future national studies should over sample for sexually diverse participants and examine associations among stress and co-occurring psychiatric disorders longitudinally to allow causal inferences to be tested empirically. At the same time, research should focus on developing and testing clinical and public health approaches to remedy both mental health and substance use disorder inequities. While evidence-based psychotherapeutic interventions to address sexual minority stress have been developed with promising results for depression and anxiety, effects on substance use outcomes are minimal. More research is needed to address the effect of sexual minority stress on the development of substance use disorders.
For policy makers: LGBTQ+ populations experience disproportionate alcohol and other drug use disorders and co-occurring psychiatric disorders, compared to their heterosexual counterparts. This is likely due to the stigma and discrimination LGBTQ+ people face that increases overall stress. Evidence shows that LGBTQ+ people who have access to spaces that affirm their sexual orientation and gender identity report better mental health. In fact, research shows that at the state-level, LGBTQ protective policy is associated with better health outcomes for LGBTQ+ people. Policy can support structural interventions to reduce stigma, such as legal protections for LGBTQ+ people in workplace settings, health care, and in schools.