The role of discrimination in alcohol use and mental health for young men identifying as racial and sexual minorities
Young Black and Hispanic men who have sex with men (MSM) report more harmful alcohol use and higher rates of depression compared to young heterosexual men. These health disparities may be linked with experiences of discrimination related both to their sexual and racial/ethnic identities. This study examined how experiences of discrimination were associated with depression and alcohol use over time among a sample of adolescent and young adult MSM.
Men who have sex with men (MSM) engage in more harmful drinking and have higher rates of depression relative to exclusively heterosexual men. Research suggests that being discriminated against is associated with higher rates of alcohol-related health issues among the LGBT community (including MSM).Such results are consistent with the Minority Stress theory, which posits that stress due to social stigma towards minority groups results in poorer health. According to this theory, someone with multiple minority identities (e.g., identifying as Black and gay) would face more stress and subsequently have worse health than those with fewer minoritized identities (e.g., identifying as White and gay).Research supports this theory- holding multiple minority identities has been associated with worse health.To date, however, there has been a lack of research examining how multiple minority stressors impact behavior over time, making it difficult to understand when the best time may beto intervene on these stressors. This research offers insights on how multiple minority stressors are associated with alcohol use and mental healthissues among MSM by assessing MSM as they age from adolescence to young adulthood
HOW WAS THIS STUDY CONDUCTED?
This study used a prospective cohort design (the Healthy Young Men’s Cohort Study) where research participants (N=448) were recruited via social media, and health clinic referrals and followed up over time. Eligible participants had to (1) be between 16-24 years old at baseline; (2) be assigned male sex at birth; (3) identify as gay, bisexual, or uncertain about their sexual identity; (4) report a sexual encounter with a man in the 12 months before screening; (5) self-identify as African American/Black, Hispanic/Latino, or multi-racial/ethnic; and (6) live in the Los Angeles area. Participants were assessed every 6 months post-baseline from 2016-2019 (resulting in a total of 5 assessments). Participant retention in the study over time was high, ranging from 87% to 90% at waves 2–5.
The focus of the research was to examine associations between experiences of racial/sexual identity-based discrimination and internalized homonegativity (i.e., negative attitudes/beliefs about lesbian/gay/bisexual people that have been incorporated into an individual’s belief system) and unhealthy alcohol use and depressive symptoms over time. Statistical models also adjusted for general life stress to account for its influence on alcohol use and depression. At each time point of the study, participants completed questionnaires with measures of these factors. General life stress was assessed via endorsement of 32 stressful life events during the previous 6 months. Item endorsements were summed together resulting in a total stress event score. Discrimination was assessed via 16 (10 for racial/ethnicity and 6 for sexual orientation-based) items ranging from never (0) to many times (3) over the participants’ lifetime. The Revised Internalized Homophobia Scale was used to measure internalized homonegativity. Participants rated their agreement with four items assessing their feelings about sexual attraction and behavior (e.g., ‘‘Sometimes I feel guilty about having sex with men’’), from strongly disagree (1) to strongly agree (4). Participant scale scores were averaged at each wave with higher scores indicating more internalized homonegativity.
The primary outcomes of this research were unhealthy alcohol use and depressive symptoms, both of which were measured at each study assessment. Unhealthy alcohol use was assessed via the Alcohol Use Disorders Identification Test (AUDIT). Items for this continuous measure were summed, with possible values ranging from 0 (never drank in the past 6 months) to 40. An AUDIT score of 8 or more is consistent with harmful (unhealthy) drinking while 16 or greater is consistent with moderate/severe alcohol use disorder. Depressive symptoms were measured by using the 6-item depression subscale from the 18-item Brief Symptom Inventory. Participants reported how often they experienced six depressive symptoms in the past 7 days on a scale ranging from never (0) to always (4). Scores were summed, with higher scores indicating more depressive symptoms.
The participant sample consisted mostly of self-identified Latino (not Black) men (58.9%) with the remainder identifying as Black (not Latino; 21%) and multi-racial/ethnic (20.1%). The average age of participants was 22.3 years. Most participants identified as homosexual/gay (74.6%) and had at least some college education (62.9%). At baseline participants reported average AUDIT scores of 6.58, indicating low odds of alcohol use disorder, but indicative of alcohol use that is approaching harmful levels. Baseline depression scores for participants were relatively low (average of 4.0).
WHAT DID THIS STUDY FIND?
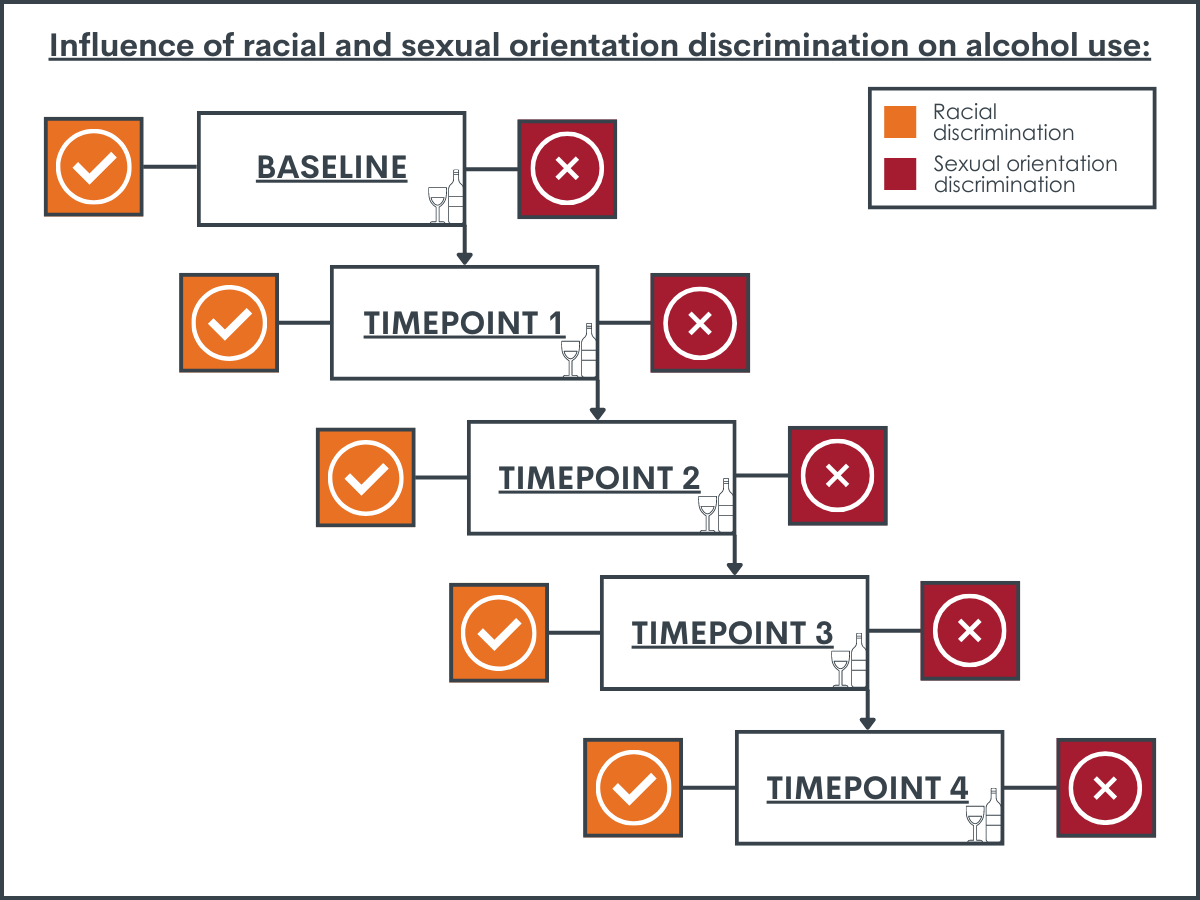
Only racial discrimination was associated with unhealthy alcohol use.
After accounting for general life stress and demographic characteristics, discrimination due to participants’ race was persistently associated with higher levels of unhealthy alcohol use. This was true at all time points of the study. Sexual orientation discrimination was not found to be associated with alcohol use at any time point.
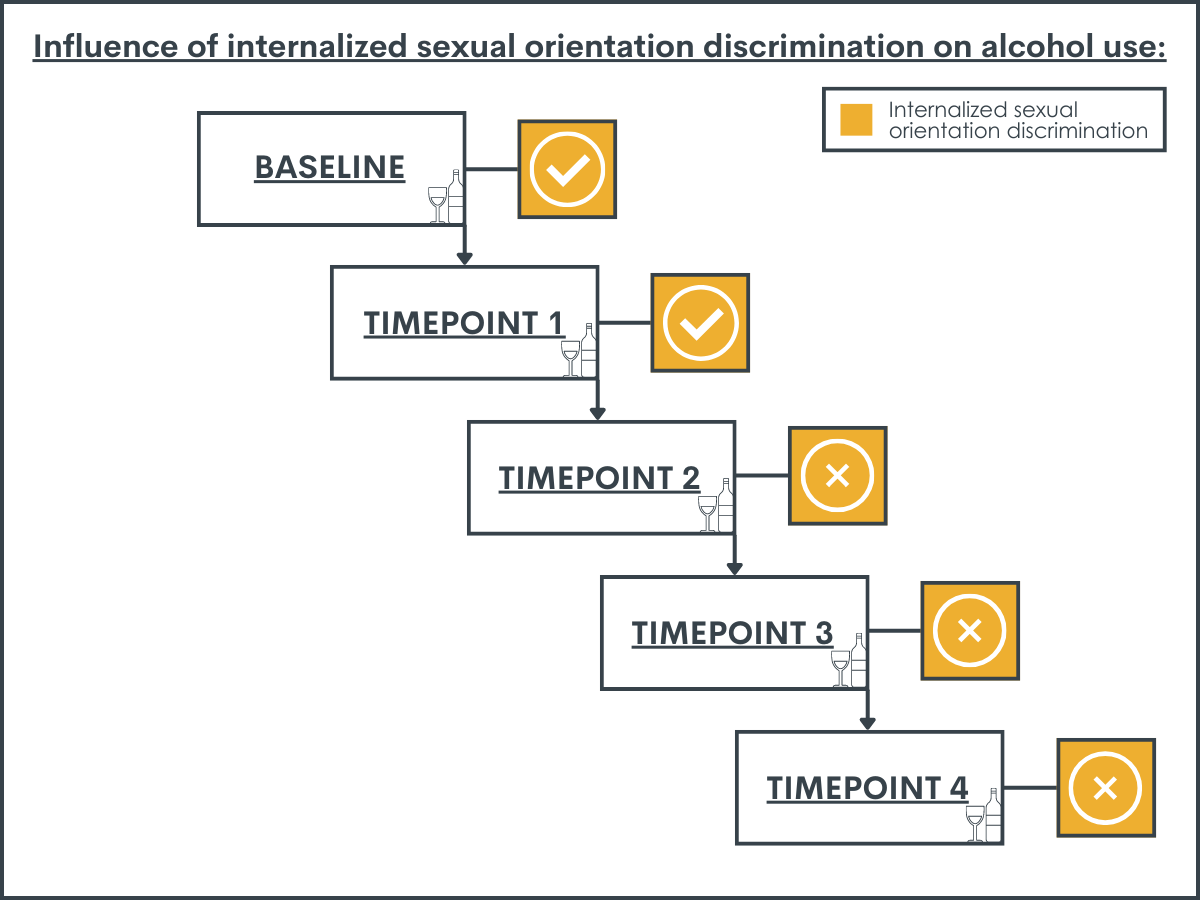
Internalized homonegativity was associated with unhealthy alcohol use initially, but this association faded over time.
At baseline and the time point 2 assessment, participants’ negative feelings about their sexual orientation were associated with unhealthy alcohol use. However, this association was not observed during the assessments 3-5.
The association between discrimination experiences and depressive symptoms changed as the sample aged.
For assessments 1-3, racial discrimination was a significant predictor of depressive symptoms. After the 3rd time point, however, this association went away. Discrimination due to sexual orientationwas associated with depressive symptoms from time points 3-5. In addition, internalized homonegativity was associated with depressive symptoms from time points 2-5.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the association between discrimination and alcohol/mental health varies over time for racial/ethnic minority MSM.
The researchers found that experiences of racial discrimination were consistently associated with higher levels of unhealthy alcohol use. However, they also found that racial discrimination was associated with depressive symptoms only during the first 3 assessments. In contrast, discrimination due to sexual orientation was not associated with unhealthy alcohol use at any time point. However, sexual orientation-based discrimination experiences and internalized homonegativity were found to be associated with depressive symptoms from assessments 3-5 and 2-5 respectively. Taken together, these latter results suggest that both racial and sexual orientation-based discrimination are associated with depressive symptoms for Black and Latino MSM, but at different times during development.
Reasons for this pattern of results are unclear, but it may suggest that social and psychological forces (e.g., stigma towards racial/ethnic MSM and internalized perceptions of such stigma among MSM) impact behavior differently over the life course. Given the age of the sample (16-24 at baseline) it is likely that these MSM recently became aware of their sexual orientation, and the observed changes in behavior may have reflected participants’ processing this new awareness of their sexual identity. For instance, the effect of internalized homonegativity on alcohol use was initially significant but then dissipated. The effect of internalized homonegativity on depression was not initially present but then emerged later. This may suggest that these MSM were drinking to cope with the burden of integrating their sexual identity. As the sample began to accept their identity, the stress/challenges of identifying as a member of the LGBT community became more salient, resulting in increased levels of depression. Alternatively, the lack of association initially seen between sexual orientation-based discrimination and depression may have been due to participants not having experienced much sexual orientation-based discrimination yet. That is, due to the sample’s youth and that sexual orientation is a more concealable marginalized identity than race/ethnicity it is possible that these MSM had not yet been exposed to harassment due to their sexual orientation.
It is also possible that MSM may need to learn how to utilize different coping strategies when dealing with sexual orientation-based discrimination than those they had previously used when confronting racism. That is, research suggests that coping with negative feelings stemming from discrimination may vary depending on if the discrimination was due to race/ethnicity compared to sexual orientation.For example, MSM may need to create social support networks separate from their same racial/ethnic peers who are also heterosexual (e.g., a chosen family). As such, the present findings suggest that interventions to relieve depressive symptoms will likely be more effective if tailored to the unique needs of MSM of color. Namely, such interventions may do well to attend to the harmful effects of racial and sexual minority-based discrimination and their consequences (e.g., internalized homonegativity) in addition to other life stressors. Mental health practitioners and community advocates may also consider that such interventions may be needed at different times during young adulthood.
The researchers took an additive statistical approach to the impact of social stigma (discrimination) on behavior. Although this is a reasonable research design there has been a shift in theliterature away from this approach as it does not necessarily reflect the experiences of holding multiple minority identities. For example, although a Black identified MSM must contend with social stigma towards racial and sexual minorities their status as a man also confers some social privileges. This unique social positionality is not easily operationalized using traditional additive statistical modeling. That is, these multiple social positions do not shape behavior independent of each other. Therefore, other modeling approaches accounting for the intersections among identities may be more apt when studying the impact of multiple minority identities on behavior.
The measurements used to quantify discrimination may not have been ideal.First, these measures utilized a four-point scale ranging from 0 (never experienced discrimination during life) to 3 (experienced discrimination many times in life). Given the age of participants it is possible that they experienced very little sexual-orientation discrimination. That is, sexual orientation is more concealable than race/ethnicity. This is partially supported by the low internal consistency of the sexual orientation discrimination measure. This may have resulted in anunderestimation of the effects between sexual-orientation discrimination and alcohol use/depressive symptoms. Second, these measures make it difficult to examine the way intersecting identities impact MSM. Measures of discrimination asked participants to indicate how experiences were tied to individual identities (i.e., due to racial/ethnic or sexual identity). These measures cannot capture combined impacts of social stigma associated with these identities and thus have limited use in demonstrating how the social positionality of MSM of color impacts mental health/substance use.
BOTTOM LINE
Results suggest that the association between social stigma and health outcomes are dynamic. Racial discrimination was associated consistently with unhealthy alcohol use among young MSM. The researchers also found that the association between sexual orientation discrimination and depressive symptoms varied as MSM got older. At earlier assessments,racial discrimination was more associated with depressive symptoms than sexual orientation-based discrimination. However, at later time points racial discrimination was not associated with depressive symptoms.Taken together these results indicate that the way social stigma is associated with behavior changes as young MSM develop from adolescence to early stages of young adulthood and from early stages of young adulthood to later ones. This suggests that interventions targeting depressive symptoms and/or alcohol use among young MSM of color need to consider age. For example, intervening on reactions to racial discrimination (e.g., through coping skills training) may be effective at reducing depressive symptoms among younger MSM of colorwhereas MSM who are slightly older may be better served by interventions targeting sexual orientation-based discrimination. More research is needed to corroborate thesefindings and to develop and test potential interventions.
For individuals and families seeking recovery: The present research did not examine treatments for unhealthy alcohol use among MSM of color.This makes it challenging to make recommendations for individuals and families seeking recovery.However, the present research does suggest that different social forces may impact young MSM of color differently depending on their age. Those interested in alcohol use treatment (whether they themselves are a young MSM of color, or seeking treatment for someone who is) may want to seek out providers that are LGBT friendly and have experience working with communities of color.It may also be prudent for those seeking treatment to be aware ofhow substance use may occur after experiences of discrimination. When faced with such experiences, it may be importantto try to find alternative coping strategies.
For treatment professionals and treatment systems: It is unknown why social stigma was associated with race, and that sexual orientation seemed to be associated with behavior differently depending on participants’ age (i.e., developmental stage). One possible explanation could be that young MSM of color are differentially impacted by these forces depending on their previous experiences and developmental stage. Those providing treatment to and/or work in healthcare system settings serving young MSM of color may want to considerthe age of their patientswhen creating treatment plans. For instance, clinicians may find it helpful to ask their adolescent patients about their developing sexual identities and how these may potentially change their healthcare needs. Such providers may also want to consider screening patients for minority stressors (discrimination experiences). If patients are experiencing high levels of discrimination, this may serve as an indicator that more in depth assessment of harmful drinking is warranted (e.g., via SBIRT: Screening, Brief Intervention and Referral to Treatment). It is especially important for providers to link MSM to alcohol use treatment as evidence suggests members of the LGBT community have a more difficult time accessing care than their heterosexual counterparts even though as a group they have more alcohol use disorder symptoms.
For policy makers: Ultimately, researchcan help to inform both broader societal interventions to reduce multiple forms of stigma/oppression,and more specific tailored interventions for sexual minority people of color to mitigate stigma’s downstream effects.This study suggests that the association between social stigma and health outcomes are dynamic over time. This may indicate that social stigma influences behavior differently across the lifespan of young MSM. It may be helpful for policymakers to invest resources in creating, evaluating, and – once shown to be effective – disseminating outreach programs targeting young MSM of color. Such programs may include elements like providing social support and or offering a supportive environment for young MSM of color. By providing support and empowerment to these community members at this critical transitional phase (from adolescence to adulthood) may help them buffer against social marginalizationand could prevent harmful epigenetic effects in turn decreasing furtheran otherwise potentially long-term and costly health burden.
Men who have sex with men (MSM) engage in more harmful drinking and have higher rates of depression relative to exclusively heterosexual men. Research suggests that being discriminated against is associated with higher rates of alcohol-related health issues among the LGBT community (including MSM).Such results are consistent with the Minority Stress theory, which posits that stress due to social stigma towards minority groups results in poorer health. According to this theory, someone with multiple minority identities (e.g., identifying as Black and gay) would face more stress and subsequently have worse health than those with fewer minoritized identities (e.g., identifying as White and gay).Research supports this theory- holding multiple minority identities has been associated with worse health.To date, however, there has been a lack of research examining how multiple minority stressors impact behavior over time, making it difficult to understand when the best time may beto intervene on these stressors. This research offers insights on how multiple minority stressors are associated with alcohol use and mental healthissues among MSM by assessing MSM as they age from adolescence to young adulthood
HOW WAS THIS STUDY CONDUCTED?
This study used a prospective cohort design (the Healthy Young Men’s Cohort Study) where research participants (N=448) were recruited via social media, and health clinic referrals and followed up over time. Eligible participants had to (1) be between 16-24 years old at baseline; (2) be assigned male sex at birth; (3) identify as gay, bisexual, or uncertain about their sexual identity; (4) report a sexual encounter with a man in the 12 months before screening; (5) self-identify as African American/Black, Hispanic/Latino, or multi-racial/ethnic; and (6) live in the Los Angeles area. Participants were assessed every 6 months post-baseline from 2016-2019 (resulting in a total of 5 assessments). Participant retention in the study over time was high, ranging from 87% to 90% at waves 2–5.
The focus of the research was to examine associations between experiences of racial/sexual identity-based discrimination and internalized homonegativity (i.e., negative attitudes/beliefs about lesbian/gay/bisexual people that have been incorporated into an individual’s belief system) and unhealthy alcohol use and depressive symptoms over time. Statistical models also adjusted for general life stress to account for its influence on alcohol use and depression. At each time point of the study, participants completed questionnaires with measures of these factors. General life stress was assessed via endorsement of 32 stressful life events during the previous 6 months. Item endorsements were summed together resulting in a total stress event score. Discrimination was assessed via 16 (10 for racial/ethnicity and 6 for sexual orientation-based) items ranging from never (0) to many times (3) over the participants’ lifetime. The Revised Internalized Homophobia Scale was used to measure internalized homonegativity. Participants rated their agreement with four items assessing their feelings about sexual attraction and behavior (e.g., ‘‘Sometimes I feel guilty about having sex with men’’), from strongly disagree (1) to strongly agree (4). Participant scale scores were averaged at each wave with higher scores indicating more internalized homonegativity.
The primary outcomes of this research were unhealthy alcohol use and depressive symptoms, both of which were measured at each study assessment. Unhealthy alcohol use was assessed via the Alcohol Use Disorders Identification Test (AUDIT). Items for this continuous measure were summed, with possible values ranging from 0 (never drank in the past 6 months) to 40. An AUDIT score of 8 or more is consistent with harmful (unhealthy) drinking while 16 or greater is consistent with moderate/severe alcohol use disorder. Depressive symptoms were measured by using the 6-item depression subscale from the 18-item Brief Symptom Inventory. Participants reported how often they experienced six depressive symptoms in the past 7 days on a scale ranging from never (0) to always (4). Scores were summed, with higher scores indicating more depressive symptoms.
The participant sample consisted mostly of self-identified Latino (not Black) men (58.9%) with the remainder identifying as Black (not Latino; 21%) and multi-racial/ethnic (20.1%). The average age of participants was 22.3 years. Most participants identified as homosexual/gay (74.6%) and had at least some college education (62.9%). At baseline participants reported average AUDIT scores of 6.58, indicating low odds of alcohol use disorder, but indicative of alcohol use that is approaching harmful levels. Baseline depression scores for participants were relatively low (average of 4.0).
WHAT DID THIS STUDY FIND?
Only racial discrimination was associated with unhealthy alcohol use.
After accounting for general life stress and demographic characteristics, discrimination due to participants’ race was persistently associated with higher levels of unhealthy alcohol use. This was true at all time points of the study. Sexual orientation discrimination was not found to be associated with alcohol use at any time point.
Internalized homonegativity was associated with unhealthy alcohol use initially, but this association faded over time.
At baseline and the time point 2 assessment, participants’ negative feelings about their sexual orientation were associated with unhealthy alcohol use. However, this association was not observed during the assessments 3-5.
The association between discrimination experiences and depressive symptoms changed as the sample aged.
For assessments 1-3, racial discrimination was a significant predictor of depressive symptoms. After the 3rd time point, however, this association went away. Discrimination due to sexual orientationwas associated with depressive symptoms from time points 3-5. In addition, internalized homonegativity was associated with depressive symptoms from time points 2-5.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the association between discrimination and alcohol/mental health varies over time for racial/ethnic minority MSM.
The researchers found that experiences of racial discrimination were consistently associated with higher levels of unhealthy alcohol use. However, they also found that racial discrimination was associated with depressive symptoms only during the first 3 assessments. In contrast, discrimination due to sexual orientation was not associated with unhealthy alcohol use at any time point. However, sexual orientation-based discrimination experiences and internalized homonegativity were found to be associated with depressive symptoms from assessments 3-5 and 2-5 respectively. Taken together, these latter results suggest that both racial and sexual orientation-based discrimination are associated with depressive symptoms for Black and Latino MSM, but at different times during development.
Reasons for this pattern of results are unclear, but it may suggest that social and psychological forces (e.g., stigma towards racial/ethnic MSM and internalized perceptions of such stigma among MSM) impact behavior differently over the life course. Given the age of the sample (16-24 at baseline) it is likely that these MSM recently became aware of their sexual orientation, and the observed changes in behavior may have reflected participants’ processing this new awareness of their sexual identity. For instance, the effect of internalized homonegativity on alcohol use was initially significant but then dissipated. The effect of internalized homonegativity on depression was not initially present but then emerged later. This may suggest that these MSM were drinking to cope with the burden of integrating their sexual identity. As the sample began to accept their identity, the stress/challenges of identifying as a member of the LGBT community became more salient, resulting in increased levels of depression. Alternatively, the lack of association initially seen between sexual orientation-based discrimination and depression may have been due to participants not having experienced much sexual orientation-based discrimination yet. That is, due to the sample’s youth and that sexual orientation is a more concealable marginalized identity than race/ethnicity it is possible that these MSM had not yet been exposed to harassment due to their sexual orientation.
It is also possible that MSM may need to learn how to utilize different coping strategies when dealing with sexual orientation-based discrimination than those they had previously used when confronting racism. That is, research suggests that coping with negative feelings stemming from discrimination may vary depending on if the discrimination was due to race/ethnicity compared to sexual orientation.For example, MSM may need to create social support networks separate from their same racial/ethnic peers who are also heterosexual (e.g., a chosen family). As such, the present findings suggest that interventions to relieve depressive symptoms will likely be more effective if tailored to the unique needs of MSM of color. Namely, such interventions may do well to attend to the harmful effects of racial and sexual minority-based discrimination and their consequences (e.g., internalized homonegativity) in addition to other life stressors. Mental health practitioners and community advocates may also consider that such interventions may be needed at different times during young adulthood.
The researchers took an additive statistical approach to the impact of social stigma (discrimination) on behavior. Although this is a reasonable research design there has been a shift in theliterature away from this approach as it does not necessarily reflect the experiences of holding multiple minority identities. For example, although a Black identified MSM must contend with social stigma towards racial and sexual minorities their status as a man also confers some social privileges. This unique social positionality is not easily operationalized using traditional additive statistical modeling. That is, these multiple social positions do not shape behavior independent of each other. Therefore, other modeling approaches accounting for the intersections among identities may be more apt when studying the impact of multiple minority identities on behavior.
The measurements used to quantify discrimination may not have been ideal.First, these measures utilized a four-point scale ranging from 0 (never experienced discrimination during life) to 3 (experienced discrimination many times in life). Given the age of participants it is possible that they experienced very little sexual-orientation discrimination. That is, sexual orientation is more concealable than race/ethnicity. This is partially supported by the low internal consistency of the sexual orientation discrimination measure. This may have resulted in anunderestimation of the effects between sexual-orientation discrimination and alcohol use/depressive symptoms. Second, these measures make it difficult to examine the way intersecting identities impact MSM. Measures of discrimination asked participants to indicate how experiences were tied to individual identities (i.e., due to racial/ethnic or sexual identity). These measures cannot capture combined impacts of social stigma associated with these identities and thus have limited use in demonstrating how the social positionality of MSM of color impacts mental health/substance use.
BOTTOM LINE
Results suggest that the association between social stigma and health outcomes are dynamic. Racial discrimination was associated consistently with unhealthy alcohol use among young MSM. The researchers also found that the association between sexual orientation discrimination and depressive symptoms varied as MSM got older. At earlier assessments,racial discrimination was more associated with depressive symptoms than sexual orientation-based discrimination. However, at later time points racial discrimination was not associated with depressive symptoms.Taken together these results indicate that the way social stigma is associated with behavior changes as young MSM develop from adolescence to early stages of young adulthood and from early stages of young adulthood to later ones. This suggests that interventions targeting depressive symptoms and/or alcohol use among young MSM of color need to consider age. For example, intervening on reactions to racial discrimination (e.g., through coping skills training) may be effective at reducing depressive symptoms among younger MSM of colorwhereas MSM who are slightly older may be better served by interventions targeting sexual orientation-based discrimination. More research is needed to corroborate thesefindings and to develop and test potential interventions.
For individuals and families seeking recovery: The present research did not examine treatments for unhealthy alcohol use among MSM of color.This makes it challenging to make recommendations for individuals and families seeking recovery.However, the present research does suggest that different social forces may impact young MSM of color differently depending on their age. Those interested in alcohol use treatment (whether they themselves are a young MSM of color, or seeking treatment for someone who is) may want to seek out providers that are LGBT friendly and have experience working with communities of color.It may also be prudent for those seeking treatment to be aware ofhow substance use may occur after experiences of discrimination. When faced with such experiences, it may be importantto try to find alternative coping strategies.
For treatment professionals and treatment systems: It is unknown why social stigma was associated with race, and that sexual orientation seemed to be associated with behavior differently depending on participants’ age (i.e., developmental stage). One possible explanation could be that young MSM of color are differentially impacted by these forces depending on their previous experiences and developmental stage. Those providing treatment to and/or work in healthcare system settings serving young MSM of color may want to considerthe age of their patientswhen creating treatment plans. For instance, clinicians may find it helpful to ask their adolescent patients about their developing sexual identities and how these may potentially change their healthcare needs. Such providers may also want to consider screening patients for minority stressors (discrimination experiences). If patients are experiencing high levels of discrimination, this may serve as an indicator that more in depth assessment of harmful drinking is warranted (e.g., via SBIRT: Screening, Brief Intervention and Referral to Treatment). It is especially important for providers to link MSM to alcohol use treatment as evidence suggests members of the LGBT community have a more difficult time accessing care than their heterosexual counterparts even though as a group they have more alcohol use disorder symptoms.
For policy makers: Ultimately, researchcan help to inform both broader societal interventions to reduce multiple forms of stigma/oppression,and more specific tailored interventions for sexual minority people of color to mitigate stigma’s downstream effects.This study suggests that the association between social stigma and health outcomes are dynamic over time. This may indicate that social stigma influences behavior differently across the lifespan of young MSM. It may be helpful for policymakers to invest resources in creating, evaluating, and – once shown to be effective – disseminating outreach programs targeting young MSM of color. Such programs may include elements like providing social support and or offering a supportive environment for young MSM of color. By providing support and empowerment to these community members at this critical transitional phase (from adolescence to adulthood) may help them buffer against social marginalizationand could prevent harmful epigenetic effects in turn decreasing furtheran otherwise potentially long-term and costly health burden.
Men who have sex with men (MSM) engage in more harmful drinking and have higher rates of depression relative to exclusively heterosexual men. Research suggests that being discriminated against is associated with higher rates of alcohol-related health issues among the LGBT community (including MSM).Such results are consistent with the Minority Stress theory, which posits that stress due to social stigma towards minority groups results in poorer health. According to this theory, someone with multiple minority identities (e.g., identifying as Black and gay) would face more stress and subsequently have worse health than those with fewer minoritized identities (e.g., identifying as White and gay).Research supports this theory- holding multiple minority identities has been associated with worse health.To date, however, there has been a lack of research examining how multiple minority stressors impact behavior over time, making it difficult to understand when the best time may beto intervene on these stressors. This research offers insights on how multiple minority stressors are associated with alcohol use and mental healthissues among MSM by assessing MSM as they age from adolescence to young adulthood
HOW WAS THIS STUDY CONDUCTED?
This study used a prospective cohort design (the Healthy Young Men’s Cohort Study) where research participants (N=448) were recruited via social media, and health clinic referrals and followed up over time. Eligible participants had to (1) be between 16-24 years old at baseline; (2) be assigned male sex at birth; (3) identify as gay, bisexual, or uncertain about their sexual identity; (4) report a sexual encounter with a man in the 12 months before screening; (5) self-identify as African American/Black, Hispanic/Latino, or multi-racial/ethnic; and (6) live in the Los Angeles area. Participants were assessed every 6 months post-baseline from 2016-2019 (resulting in a total of 5 assessments). Participant retention in the study over time was high, ranging from 87% to 90% at waves 2–5.
The focus of the research was to examine associations between experiences of racial/sexual identity-based discrimination and internalized homonegativity (i.e., negative attitudes/beliefs about lesbian/gay/bisexual people that have been incorporated into an individual’s belief system) and unhealthy alcohol use and depressive symptoms over time. Statistical models also adjusted for general life stress to account for its influence on alcohol use and depression. At each time point of the study, participants completed questionnaires with measures of these factors. General life stress was assessed via endorsement of 32 stressful life events during the previous 6 months. Item endorsements were summed together resulting in a total stress event score. Discrimination was assessed via 16 (10 for racial/ethnicity and 6 for sexual orientation-based) items ranging from never (0) to many times (3) over the participants’ lifetime. The Revised Internalized Homophobia Scale was used to measure internalized homonegativity. Participants rated their agreement with four items assessing their feelings about sexual attraction and behavior (e.g., ‘‘Sometimes I feel guilty about having sex with men’’), from strongly disagree (1) to strongly agree (4). Participant scale scores were averaged at each wave with higher scores indicating more internalized homonegativity.
The primary outcomes of this research were unhealthy alcohol use and depressive symptoms, both of which were measured at each study assessment. Unhealthy alcohol use was assessed via the Alcohol Use Disorders Identification Test (AUDIT). Items for this continuous measure were summed, with possible values ranging from 0 (never drank in the past 6 months) to 40. An AUDIT score of 8 or more is consistent with harmful (unhealthy) drinking while 16 or greater is consistent with moderate/severe alcohol use disorder. Depressive symptoms were measured by using the 6-item depression subscale from the 18-item Brief Symptom Inventory. Participants reported how often they experienced six depressive symptoms in the past 7 days on a scale ranging from never (0) to always (4). Scores were summed, with higher scores indicating more depressive symptoms.
The participant sample consisted mostly of self-identified Latino (not Black) men (58.9%) with the remainder identifying as Black (not Latino; 21%) and multi-racial/ethnic (20.1%). The average age of participants was 22.3 years. Most participants identified as homosexual/gay (74.6%) and had at least some college education (62.9%). At baseline participants reported average AUDIT scores of 6.58, indicating low odds of alcohol use disorder, but indicative of alcohol use that is approaching harmful levels. Baseline depression scores for participants were relatively low (average of 4.0).
WHAT DID THIS STUDY FIND?
Only racial discrimination was associated with unhealthy alcohol use.
After accounting for general life stress and demographic characteristics, discrimination due to participants’ race was persistently associated with higher levels of unhealthy alcohol use. This was true at all time points of the study. Sexual orientation discrimination was not found to be associated with alcohol use at any time point.
Internalized homonegativity was associated with unhealthy alcohol use initially, but this association faded over time.
At baseline and the time point 2 assessment, participants’ negative feelings about their sexual orientation were associated with unhealthy alcohol use. However, this association was not observed during the assessments 3-5.
The association between discrimination experiences and depressive symptoms changed as the sample aged.
For assessments 1-3, racial discrimination was a significant predictor of depressive symptoms. After the 3rd time point, however, this association went away. Discrimination due to sexual orientationwas associated with depressive symptoms from time points 3-5. In addition, internalized homonegativity was associated with depressive symptoms from time points 2-5.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the association between discrimination and alcohol/mental health varies over time for racial/ethnic minority MSM.
The researchers found that experiences of racial discrimination were consistently associated with higher levels of unhealthy alcohol use. However, they also found that racial discrimination was associated with depressive symptoms only during the first 3 assessments. In contrast, discrimination due to sexual orientation was not associated with unhealthy alcohol use at any time point. However, sexual orientation-based discrimination experiences and internalized homonegativity were found to be associated with depressive symptoms from assessments 3-5 and 2-5 respectively. Taken together, these latter results suggest that both racial and sexual orientation-based discrimination are associated with depressive symptoms for Black and Latino MSM, but at different times during development.
Reasons for this pattern of results are unclear, but it may suggest that social and psychological forces (e.g., stigma towards racial/ethnic MSM and internalized perceptions of such stigma among MSM) impact behavior differently over the life course. Given the age of the sample (16-24 at baseline) it is likely that these MSM recently became aware of their sexual orientation, and the observed changes in behavior may have reflected participants’ processing this new awareness of their sexual identity. For instance, the effect of internalized homonegativity on alcohol use was initially significant but then dissipated. The effect of internalized homonegativity on depression was not initially present but then emerged later. This may suggest that these MSM were drinking to cope with the burden of integrating their sexual identity. As the sample began to accept their identity, the stress/challenges of identifying as a member of the LGBT community became more salient, resulting in increased levels of depression. Alternatively, the lack of association initially seen between sexual orientation-based discrimination and depression may have been due to participants not having experienced much sexual orientation-based discrimination yet. That is, due to the sample’s youth and that sexual orientation is a more concealable marginalized identity than race/ethnicity it is possible that these MSM had not yet been exposed to harassment due to their sexual orientation.
It is also possible that MSM may need to learn how to utilize different coping strategies when dealing with sexual orientation-based discrimination than those they had previously used when confronting racism. That is, research suggests that coping with negative feelings stemming from discrimination may vary depending on if the discrimination was due to race/ethnicity compared to sexual orientation.For example, MSM may need to create social support networks separate from their same racial/ethnic peers who are also heterosexual (e.g., a chosen family). As such, the present findings suggest that interventions to relieve depressive symptoms will likely be more effective if tailored to the unique needs of MSM of color. Namely, such interventions may do well to attend to the harmful effects of racial and sexual minority-based discrimination and their consequences (e.g., internalized homonegativity) in addition to other life stressors. Mental health practitioners and community advocates may also consider that such interventions may be needed at different times during young adulthood.
The researchers took an additive statistical approach to the impact of social stigma (discrimination) on behavior. Although this is a reasonable research design there has been a shift in theliterature away from this approach as it does not necessarily reflect the experiences of holding multiple minority identities. For example, although a Black identified MSM must contend with social stigma towards racial and sexual minorities their status as a man also confers some social privileges. This unique social positionality is not easily operationalized using traditional additive statistical modeling. That is, these multiple social positions do not shape behavior independent of each other. Therefore, other modeling approaches accounting for the intersections among identities may be more apt when studying the impact of multiple minority identities on behavior.
The measurements used to quantify discrimination may not have been ideal.First, these measures utilized a four-point scale ranging from 0 (never experienced discrimination during life) to 3 (experienced discrimination many times in life). Given the age of participants it is possible that they experienced very little sexual-orientation discrimination. That is, sexual orientation is more concealable than race/ethnicity. This is partially supported by the low internal consistency of the sexual orientation discrimination measure. This may have resulted in anunderestimation of the effects between sexual-orientation discrimination and alcohol use/depressive symptoms. Second, these measures make it difficult to examine the way intersecting identities impact MSM. Measures of discrimination asked participants to indicate how experiences were tied to individual identities (i.e., due to racial/ethnic or sexual identity). These measures cannot capture combined impacts of social stigma associated with these identities and thus have limited use in demonstrating how the social positionality of MSM of color impacts mental health/substance use.
BOTTOM LINE
Results suggest that the association between social stigma and health outcomes are dynamic. Racial discrimination was associated consistently with unhealthy alcohol use among young MSM. The researchers also found that the association between sexual orientation discrimination and depressive symptoms varied as MSM got older. At earlier assessments,racial discrimination was more associated with depressive symptoms than sexual orientation-based discrimination. However, at later time points racial discrimination was not associated with depressive symptoms.Taken together these results indicate that the way social stigma is associated with behavior changes as young MSM develop from adolescence to early stages of young adulthood and from early stages of young adulthood to later ones. This suggests that interventions targeting depressive symptoms and/or alcohol use among young MSM of color need to consider age. For example, intervening on reactions to racial discrimination (e.g., through coping skills training) may be effective at reducing depressive symptoms among younger MSM of colorwhereas MSM who are slightly older may be better served by interventions targeting sexual orientation-based discrimination. More research is needed to corroborate thesefindings and to develop and test potential interventions.
For individuals and families seeking recovery: The present research did not examine treatments for unhealthy alcohol use among MSM of color.This makes it challenging to make recommendations for individuals and families seeking recovery.However, the present research does suggest that different social forces may impact young MSM of color differently depending on their age. Those interested in alcohol use treatment (whether they themselves are a young MSM of color, or seeking treatment for someone who is) may want to seek out providers that are LGBT friendly and have experience working with communities of color.It may also be prudent for those seeking treatment to be aware ofhow substance use may occur after experiences of discrimination. When faced with such experiences, it may be importantto try to find alternative coping strategies.
For treatment professionals and treatment systems: It is unknown why social stigma was associated with race, and that sexual orientation seemed to be associated with behavior differently depending on participants’ age (i.e., developmental stage). One possible explanation could be that young MSM of color are differentially impacted by these forces depending on their previous experiences and developmental stage. Those providing treatment to and/or work in healthcare system settings serving young MSM of color may want to considerthe age of their patientswhen creating treatment plans. For instance, clinicians may find it helpful to ask their adolescent patients about their developing sexual identities and how these may potentially change their healthcare needs. Such providers may also want to consider screening patients for minority stressors (discrimination experiences). If patients are experiencing high levels of discrimination, this may serve as an indicator that more in depth assessment of harmful drinking is warranted (e.g., via SBIRT: Screening, Brief Intervention and Referral to Treatment). It is especially important for providers to link MSM to alcohol use treatment as evidence suggests members of the LGBT community have a more difficult time accessing care than their heterosexual counterparts even though as a group they have more alcohol use disorder symptoms.
For policy makers: Ultimately, researchcan help to inform both broader societal interventions to reduce multiple forms of stigma/oppression,and more specific tailored interventions for sexual minority people of color to mitigate stigma’s downstream effects.This study suggests that the association between social stigma and health outcomes are dynamic over time. This may indicate that social stigma influences behavior differently across the lifespan of young MSM. It may be helpful for policymakers to invest resources in creating, evaluating, and – once shown to be effective – disseminating outreach programs targeting young MSM of color. Such programs may include elements like providing social support and or offering a supportive environment for young MSM of color. By providing support and empowerment to these community members at this critical transitional phase (from adolescence to adulthood) may help them buffer against social marginalizationand could prevent harmful epigenetic effects in turn decreasing furtheran otherwise potentially long-term and costly health burden.