Are racial and ethnic minorities less likely to achieve remission?
Racial and ethnic minorities face barriers to recovery that can hinder remission. Identifying disparities in remission rates can help determine whether additional supports are needed for particular racial and ethnic groups. This study examined racial and ethnic differences in rates of remission in a national U.S. sample.
Although the risk of developing a substance use disorder is generally similar across individuals of various races and ethnicities, racial and ethnic minorities face barriers to recovery, including less access to addiction treatmentrelative to White individuals. Less is known about the role of race and ethnicity in recovery. In the broader population of individuals with substance use disorders, about halfto three quarters achieve full remission, meaning they no longer meet diagnostic criteria for a formal substance use disorder within the past year.Among the few studies that have examined the role of race and ethnicity, outcomes are mixed with different studies showing racial/ethnic minorities have higher, lower, and equivalent remission rates relative to White individuals. Clarifying whether or not disparities exist in remission status can ultimately inform whether new approaches to treatment and recovery support are needed to ensure all races and ethnicities have equal opportunity for achieving remission.This study examined differences in remission rates between racial/ethnic minorities and White individuals in a nationally representative sample of adults with a lifetime diagnosis of substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from a cross-sectional national survey conducted in the United States between 2012 and 2013 (i.e. the National Epidemiologic Survey on Alcohol and Related Conditions-III (NESARC-III)). Individuals who identified as Black, Hispanic, and Asian were oversampled to ensure an adequate representation of these races and ethnicities, and data was ultimately weighted to represent the U.S. noninstitutionalized population.
All participants included in this study were adults ages 18 or older, with a lifetime substance use disorder (alcohol or other drug use disorder) according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Among all participants, 92% had a lifetime alcohol use disorder and 32% had a lifetime drug use disorder. The researchers grouped the 10,916 participants into 4 racial/ethnic categories: 1) Black (10%), 2) Hispanic (12%), 3) White (73%), 4) Other race/ethnicity (5%; i.e. Asian, Native Hawaiian, other Pacific Islander, American Indian or Alaska Native, and those identifying with more than one racial category).
The researchers investigated differences in demographic and clinical information among participants who were in full remission (i.e., met lifetime criteria but had no past-year symptoms when interviewed for the survey), compared to individuals who met criteria for a past year substance use disorder (i.e., not in remission). Thus, participants were asked to think about their substance use disorder symptoms before the prior year to determine lifetime diagnosis. They were also asked at the same time to think about their symptoms during the prior year to determine current diagnosis or remission. Among demographic and clinical characteristics investigated, mental and physical health were evaluated with the Short Form Health Survey for which scores range from 0 to 100 (average score = 50; higher scores indicate better health), and frequency of experiencing lifetime racial discrimination was examined via Likert scale responses where ‘1’ = ‘almost never’, ‘2’ = ‘sometimes’, ‘3’ = ‘fairly often’, ‘4’ = ‘very often’.
The researchers first characterized the percentage of individuals within each racial/ethnic group who were in remission from alcohol and other drug use disorders. Thereafter, the odds of remission were investigated by racial/ethnic group, controlling for demographic and clinical factors that differed between participants who were and were not in remission to better isolate the effect of race/ethnicity on remission.
WHAT DID THIS STUDY FIND?
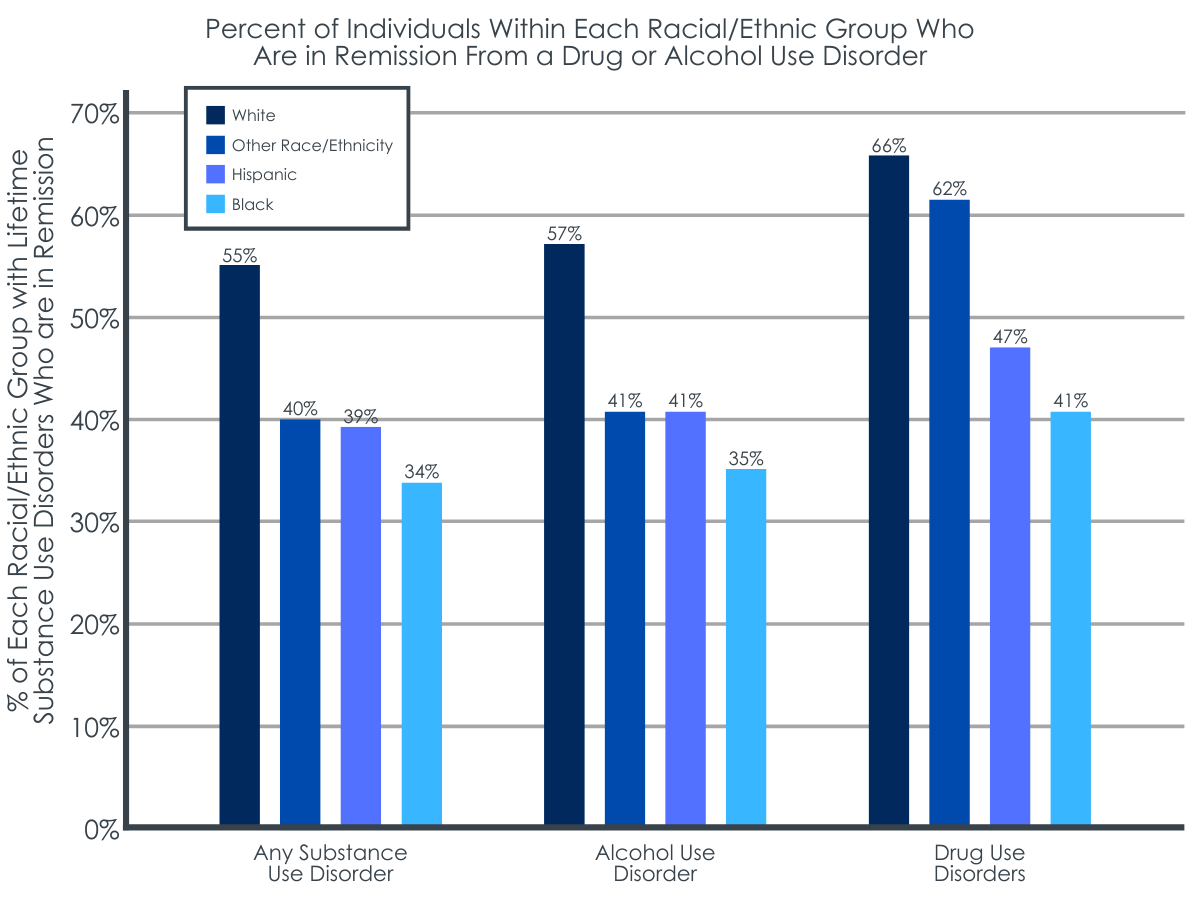
Black individuals had the lowest rates of remission from substance use disorders.
Overall, 47% of participants with a lifetime substance use disorder were in remission. 91% of those in remission had a lifetime alcohol use disorder and 27% of those in remission had a lifetime drug use disorder. When remission rates were assessed within White individuals had the highest rates of remission from alcohol use disorder and drug use disorders, while Black individuals had the lowest rates of remission.
Demographic and clinical factors differed between individuals who were, and who were not, in remission.
Compared to those with a past year substance use disorder, individuals who were in remission were more likely to be older (average age of 47 vs. 37 years), married (65% vs. 43%) or widowed (3% vs. 2%), retired (14% vs. 5%), and military veterans (15% vs. 8%). They were also more likely to have Medicare health insurance (18% vs. 10%), a higher body mass index (average BMI of 29 vs. 27), better mental health (average score of 50 vs. 47 on the Short Form Health Survey), and to attend religious services more frequently (average of ‘a few times a year’ vs. ‘once a year’).
Individuals who had not remitted were more likely than those in remission to be unemployed (13% vs. 7%), never married (40% vs. 16%), to have a past year (2% vs. 1%) or lifetime (4% vs. 2%) psychotic disorder, a yearly income of less than $20,000 (29% vs. 18%), and better physical health (average score of 51 vs. 49 the Short Form Health Survey). They were also more likely to have a lifetime sedative (4% vs. 3%) or opioid (9% vs. 5%) use disorder, to have experienced a past year suicide attempt (0.7% vs. 0.2%), past year trouble with the police (6% vs. 2%), past year houselessness (4% vs. 2%), and more frequent racial discrimination (average score of 1.3 vs. 1.2). This group also had higher rates of lifetime sedative use disorder (4% vs. 3%) and opioid use disorder (9% vs. 5%).
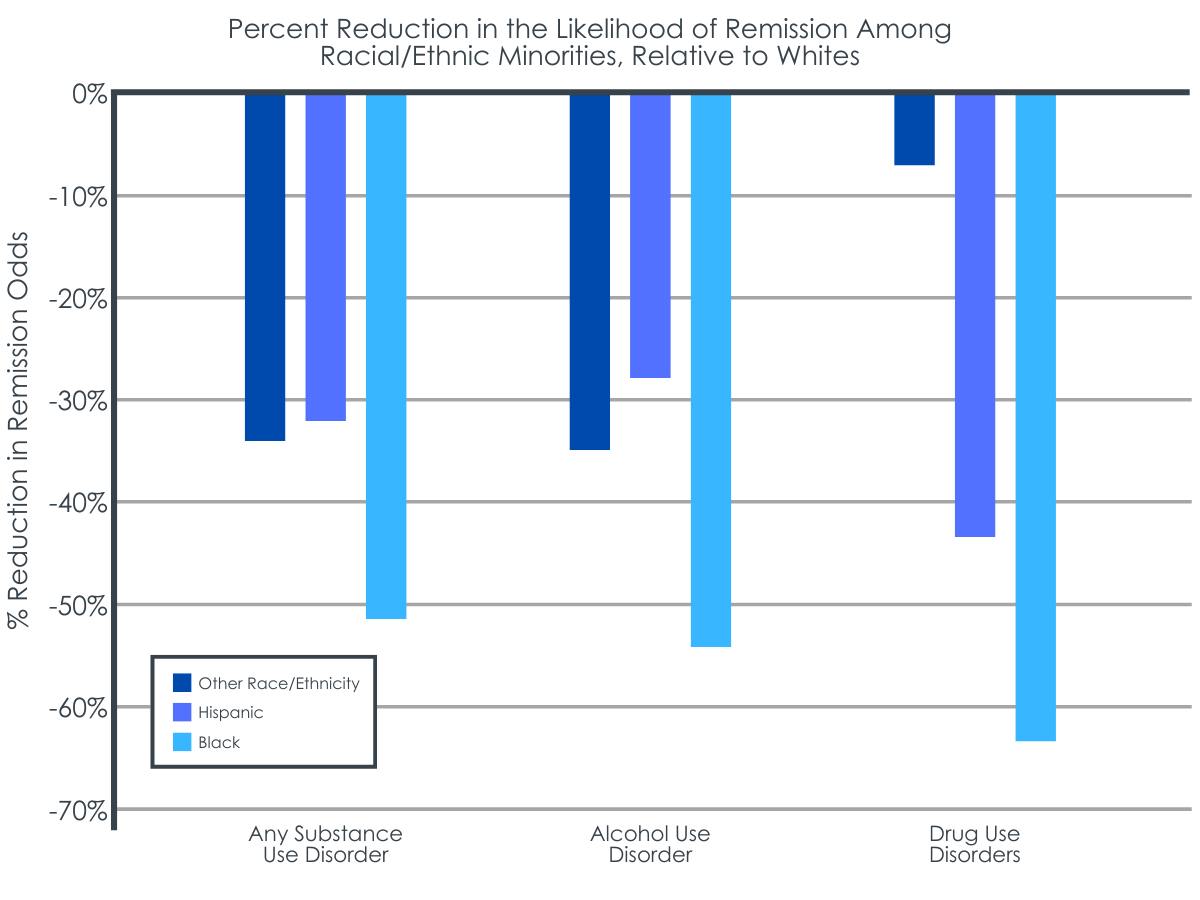
Black, Hispanic, and other races/ethnicities were less likely to be in remission.
Controlling for other demographic and clinical factors associated with remission, the odds of being in remission from a substance use disorder were 51% lower in Blacks, 32% lower in Hispanics, and 34% lower in those of other races/ethnicities, relative to Whites. When the type of use disorder was considered, all minority groups were less likely than Whites to be in remission from both alcohol and drug use disorders except for the other race/ethnicity group, who had a similar likelihood of remission from drug use disorders compared to Whites.
Figure 2. The percent reduction in the odds of remission by race and disorder type, independent of other factors that influenced remission.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the disparities that exist in addiction recovery, which can ultimately inform new treatment and recovery efforts. The researchers found that racial and ethnic minorities, particularly Black individuals, are significantly less likely to achieve remission from substance use disorders relative to Whites.
The overall remission rate observed in this study was similar to those of prior studies, with about half of individuals with lifetime substance use disorders achieving full remission. The factors associated with remission status that emerged in this study (e.g., age, opioid use disorder, marital status, psychiatric comorbidities, etc.) were also generally consistent withpreviousresearch. Yet, racial and ethnic differences observed in this study add to a mixed literature on whether or not remission rates vary by minority status. Though this literature is somewhat limited, prior research has generally observed higher rates of remission among Blacks and Hispanics compared to Whites, or equivalent rates of remission across races/ethnicities when controlling for various demographic factors (e.g., age, education, marital status).
Interestingly, racial and ethnic differences in remission status persisted in this study, even when controlling for important demographic and clinical characteristics. It could be that differences in methods across these different studies might account for the different findings. For example, this study examined remission from a lifetime substance use disorder that someone may have initiated either recently or long ago, whereas other studies have largely focused on remission that was achieved over the previous few years. Or it could be due to differences in study design (e.g., cross-sectional/retrospective vs longitudinal) or both. A nationally representative longitudinal study of individuals with alcohol use disorder, for example, showed that Black and Latino individuals were just as likely to be in remission as White individuals 3 years later. Thus, it may be that long-term remission (e.g., being in recovery for 5 years or more) from a lifetime substance use disorder is less prevalent among racial and ethnic minorities. The way substance use disorder is defined and how disorder criteria are evaluated across studies may also contribute to inconsistent outcomes. Additional research is needed to formally study racial/ethnic differences in remission, particularly longitudinal research, given that cross-sectional studies determine lifetime substance use disorder by asking individuals to remember past events and symptoms, which relies on accurate recall.
The factors controlled for in different studies also vary. Race/ethnicity remained the strongest predictor of remission in this study, with the demographic and clinical characteristics assessed here having a less robust effect when race/ethnicity were introduced into the researchers’ statistical models. It may be that other structural and social inequities that were not assessed in this study underlie these racial and ethnic disparities. For example, other social, community, and treatment/recovery support factors that differ by race/ethnicity and influence one’s ability to achieve remission (e.g., access to competent treatment and recovery services, or recovery capital) might produce lower rates of remission among certain racial/ethnic minority groups. With other studies finding higher or equivalent rates of remission among racial and ethnic minorities compared to Whites, additional research can help identify racial and ethnic disparities in short- and long-term recovery and help explain the factors that underlie these disparities.
This study did not include an evaluation of the impact of treatment/recovery service use or a number of other relevant factors that might underlie racial and ethnic disparities in remission rates. Additional research is needed to determine factors that influence these rates to better address inequities.
This study is based on a cross-sectional survey and can’t speak to causal effects, but nevertheless highlights associations between race, ethnicity, sociodemographic factors, and remission. Longitudinal studies that track individuals over long periods of time will help us better understand the role of these factors in the course of remission and recovery. Studies that assess drug use disorders with respect to different drug types will also be useful for informing the development of equitable treatment and recovery efforts.
BOTTOM LINE
Compared to Whites, racial and ethnic minorities showed a reduced likelihood of achieving remission from substance use disorders in the current study, even when controlling for a number of factors that differed between them and Whites and that were relevant to remission. Findings to date within this limited literature are mixed, however, with some studies showing increased, decreased, or equivalent remission rates between racial/ethnic minorities and Whites. This was a cross-sectional study that evaluated remission from a lifetime substance use disorder and the way remission is defined and observed across studies might account for the mixed findings across different studies that have examined this question. There is a need for additional research to learn more about what factors account for disparities so they can be addressed with culturally competent policies and individualized services. Research to date suggests there are some potential candidates that can be targeted to help address these disparities, such as lower socioeconomic status and unemployment that are often lower among minorities. This study contributes to a growing literature that advances our understanding of racial/ethnic disparities that exist in addiction, treatment, and remission, which may help address the inequities that are often faced by minority populations seeking recovery.
For individuals and families seeking recovery: Individuals who identify as racial or ethnic minorities might face barriers to remission that may be accounted for by sociodemographic characteristics and/or inequities in access to treatment and recovery services. Individuals and families seeking recovery should seek culturally competent care that does not discriminate against race, ethnicity, or those from disadvantaged backgrounds. Many states are developing programs that can help combat barriers to treatment and recovery, such as financial support for treatment, assistance with obtaining education and work skills needed to support recovery, and free local recovery support programs that boost social support for recovery. Interested individuals should check out their state’s websites and local recovery communities to find out more on these novel opportunities in your area that can help combat barriers to treatment and recovery.
For treatment professionals and treatment systems: Individuals who identify as racial or ethnic minorities might face barriers to remission relative to White individuals. Though the literature in this area is limited with mixed outcomes, racial and ethnic disparities are often accounted for by sociodemographic characteristics and/or inequities in access to clinical care and recovery services. Offering culturally competent treatment that considers the many barriers that one might face along their treatment and recovery journey is essential to ensuring equal access and opportunity in the treatment and recovery realm.
For scientists:Additional longitudinal research studies are needed as well as studies that utilize databases from more recent years to examine the role of race, ethnicity, and related factors on remission status. Research examining remission from specific drug use disorders will also enhance our understanding of whether certain patterns emerge for specific substances. Better understanding of the factors that account for these observed racial/ethnic disparities is also needed to develop treatment and recovery initiatives that promote equal access to services and equal opportunity for remission.
For policy makers: Racial and ethnic minorities, particularly Black individuals, may be less likely to achieve remission compared to White individuals. Prior studies have also suggested several potential sociodemographic and clinical risk factors that account for these racial/ethnic disparities. However, inconsistent methods among the few available studies on race, ethnicity, and remission make it hard to form concrete conclusions on racial/ethnic disparities in remission and the factors that account for them (e.g., socioeconomic status, discrimination, community). Additional funding for research will help expand this growing literature to advance our understanding of racial/ethnic disparities that exist in addiction, treatment, and recovery, which will ultimately help address the inequities that are faced by minority populations seeking recovery.
Although the risk of developing a substance use disorder is generally similar across individuals of various races and ethnicities, racial and ethnic minorities face barriers to recovery, including less access to addiction treatmentrelative to White individuals. Less is known about the role of race and ethnicity in recovery. In the broader population of individuals with substance use disorders, about halfto three quarters achieve full remission, meaning they no longer meet diagnostic criteria for a formal substance use disorder within the past year.Among the few studies that have examined the role of race and ethnicity, outcomes are mixed with different studies showing racial/ethnic minorities have higher, lower, and equivalent remission rates relative to White individuals. Clarifying whether or not disparities exist in remission status can ultimately inform whether new approaches to treatment and recovery support are needed to ensure all races and ethnicities have equal opportunity for achieving remission.This study examined differences in remission rates between racial/ethnic minorities and White individuals in a nationally representative sample of adults with a lifetime diagnosis of substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from a cross-sectional national survey conducted in the United States between 2012 and 2013 (i.e. the National Epidemiologic Survey on Alcohol and Related Conditions-III (NESARC-III)). Individuals who identified as Black, Hispanic, and Asian were oversampled to ensure an adequate representation of these races and ethnicities, and data was ultimately weighted to represent the U.S. noninstitutionalized population.
All participants included in this study were adults ages 18 or older, with a lifetime substance use disorder (alcohol or other drug use disorder) according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Among all participants, 92% had a lifetime alcohol use disorder and 32% had a lifetime drug use disorder. The researchers grouped the 10,916 participants into 4 racial/ethnic categories: 1) Black (10%), 2) Hispanic (12%), 3) White (73%), 4) Other race/ethnicity (5%; i.e. Asian, Native Hawaiian, other Pacific Islander, American Indian or Alaska Native, and those identifying with more than one racial category).
The researchers investigated differences in demographic and clinical information among participants who were in full remission (i.e., met lifetime criteria but had no past-year symptoms when interviewed for the survey), compared to individuals who met criteria for a past year substance use disorder (i.e., not in remission). Thus, participants were asked to think about their substance use disorder symptoms before the prior year to determine lifetime diagnosis. They were also asked at the same time to think about their symptoms during the prior year to determine current diagnosis or remission. Among demographic and clinical characteristics investigated, mental and physical health were evaluated with the Short Form Health Survey for which scores range from 0 to 100 (average score = 50; higher scores indicate better health), and frequency of experiencing lifetime racial discrimination was examined via Likert scale responses where ‘1’ = ‘almost never’, ‘2’ = ‘sometimes’, ‘3’ = ‘fairly often’, ‘4’ = ‘very often’.
The researchers first characterized the percentage of individuals within each racial/ethnic group who were in remission from alcohol and other drug use disorders. Thereafter, the odds of remission were investigated by racial/ethnic group, controlling for demographic and clinical factors that differed between participants who were and were not in remission to better isolate the effect of race/ethnicity on remission.
WHAT DID THIS STUDY FIND?
Black individuals had the lowest rates of remission from substance use disorders.
Overall, 47% of participants with a lifetime substance use disorder were in remission. 91% of those in remission had a lifetime alcohol use disorder and 27% of those in remission had a lifetime drug use disorder. When remission rates were assessed within White individuals had the highest rates of remission from alcohol use disorder and drug use disorders, while Black individuals had the lowest rates of remission.
Demographic and clinical factors differed between individuals who were, and who were not, in remission.
Compared to those with a past year substance use disorder, individuals who were in remission were more likely to be older (average age of 47 vs. 37 years), married (65% vs. 43%) or widowed (3% vs. 2%), retired (14% vs. 5%), and military veterans (15% vs. 8%). They were also more likely to have Medicare health insurance (18% vs. 10%), a higher body mass index (average BMI of 29 vs. 27), better mental health (average score of 50 vs. 47 on the Short Form Health Survey), and to attend religious services more frequently (average of ‘a few times a year’ vs. ‘once a year’).
Individuals who had not remitted were more likely than those in remission to be unemployed (13% vs. 7%), never married (40% vs. 16%), to have a past year (2% vs. 1%) or lifetime (4% vs. 2%) psychotic disorder, a yearly income of less than $20,000 (29% vs. 18%), and better physical health (average score of 51 vs. 49 the Short Form Health Survey). They were also more likely to have a lifetime sedative (4% vs. 3%) or opioid (9% vs. 5%) use disorder, to have experienced a past year suicide attempt (0.7% vs. 0.2%), past year trouble with the police (6% vs. 2%), past year houselessness (4% vs. 2%), and more frequent racial discrimination (average score of 1.3 vs. 1.2). This group also had higher rates of lifetime sedative use disorder (4% vs. 3%) and opioid use disorder (9% vs. 5%).
Black, Hispanic, and other races/ethnicities were less likely to be in remission.
Controlling for other demographic and clinical factors associated with remission, the odds of being in remission from a substance use disorder were 51% lower in Blacks, 32% lower in Hispanics, and 34% lower in those of other races/ethnicities, relative to Whites. When the type of use disorder was considered, all minority groups were less likely than Whites to be in remission from both alcohol and drug use disorders except for the other race/ethnicity group, who had a similar likelihood of remission from drug use disorders compared to Whites.
Figure 2. The percent reduction in the odds of remission by race and disorder type, independent of other factors that influenced remission.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the disparities that exist in addiction recovery, which can ultimately inform new treatment and recovery efforts. The researchers found that racial and ethnic minorities, particularly Black individuals, are significantly less likely to achieve remission from substance use disorders relative to Whites.
The overall remission rate observed in this study was similar to those of prior studies, with about half of individuals with lifetime substance use disorders achieving full remission. The factors associated with remission status that emerged in this study (e.g., age, opioid use disorder, marital status, psychiatric comorbidities, etc.) were also generally consistent withpreviousresearch. Yet, racial and ethnic differences observed in this study add to a mixed literature on whether or not remission rates vary by minority status. Though this literature is somewhat limited, prior research has generally observed higher rates of remission among Blacks and Hispanics compared to Whites, or equivalent rates of remission across races/ethnicities when controlling for various demographic factors (e.g., age, education, marital status).
Interestingly, racial and ethnic differences in remission status persisted in this study, even when controlling for important demographic and clinical characteristics. It could be that differences in methods across these different studies might account for the different findings. For example, this study examined remission from a lifetime substance use disorder that someone may have initiated either recently or long ago, whereas other studies have largely focused on remission that was achieved over the previous few years. Or it could be due to differences in study design (e.g., cross-sectional/retrospective vs longitudinal) or both. A nationally representative longitudinal study of individuals with alcohol use disorder, for example, showed that Black and Latino individuals were just as likely to be in remission as White individuals 3 years later. Thus, it may be that long-term remission (e.g., being in recovery for 5 years or more) from a lifetime substance use disorder is less prevalent among racial and ethnic minorities. The way substance use disorder is defined and how disorder criteria are evaluated across studies may also contribute to inconsistent outcomes. Additional research is needed to formally study racial/ethnic differences in remission, particularly longitudinal research, given that cross-sectional studies determine lifetime substance use disorder by asking individuals to remember past events and symptoms, which relies on accurate recall.
The factors controlled for in different studies also vary. Race/ethnicity remained the strongest predictor of remission in this study, with the demographic and clinical characteristics assessed here having a less robust effect when race/ethnicity were introduced into the researchers’ statistical models. It may be that other structural and social inequities that were not assessed in this study underlie these racial and ethnic disparities. For example, other social, community, and treatment/recovery support factors that differ by race/ethnicity and influence one’s ability to achieve remission (e.g., access to competent treatment and recovery services, or recovery capital) might produce lower rates of remission among certain racial/ethnic minority groups. With other studies finding higher or equivalent rates of remission among racial and ethnic minorities compared to Whites, additional research can help identify racial and ethnic disparities in short- and long-term recovery and help explain the factors that underlie these disparities.
This study did not include an evaluation of the impact of treatment/recovery service use or a number of other relevant factors that might underlie racial and ethnic disparities in remission rates. Additional research is needed to determine factors that influence these rates to better address inequities.
This study is based on a cross-sectional survey and can’t speak to causal effects, but nevertheless highlights associations between race, ethnicity, sociodemographic factors, and remission. Longitudinal studies that track individuals over long periods of time will help us better understand the role of these factors in the course of remission and recovery. Studies that assess drug use disorders with respect to different drug types will also be useful for informing the development of equitable treatment and recovery efforts.
BOTTOM LINE
Compared to Whites, racial and ethnic minorities showed a reduced likelihood of achieving remission from substance use disorders in the current study, even when controlling for a number of factors that differed between them and Whites and that were relevant to remission. Findings to date within this limited literature are mixed, however, with some studies showing increased, decreased, or equivalent remission rates between racial/ethnic minorities and Whites. This was a cross-sectional study that evaluated remission from a lifetime substance use disorder and the way remission is defined and observed across studies might account for the mixed findings across different studies that have examined this question. There is a need for additional research to learn more about what factors account for disparities so they can be addressed with culturally competent policies and individualized services. Research to date suggests there are some potential candidates that can be targeted to help address these disparities, such as lower socioeconomic status and unemployment that are often lower among minorities. This study contributes to a growing literature that advances our understanding of racial/ethnic disparities that exist in addiction, treatment, and remission, which may help address the inequities that are often faced by minority populations seeking recovery.
For individuals and families seeking recovery: Individuals who identify as racial or ethnic minorities might face barriers to remission that may be accounted for by sociodemographic characteristics and/or inequities in access to treatment and recovery services. Individuals and families seeking recovery should seek culturally competent care that does not discriminate against race, ethnicity, or those from disadvantaged backgrounds. Many states are developing programs that can help combat barriers to treatment and recovery, such as financial support for treatment, assistance with obtaining education and work skills needed to support recovery, and free local recovery support programs that boost social support for recovery. Interested individuals should check out their state’s websites and local recovery communities to find out more on these novel opportunities in your area that can help combat barriers to treatment and recovery.
For treatment professionals and treatment systems: Individuals who identify as racial or ethnic minorities might face barriers to remission relative to White individuals. Though the literature in this area is limited with mixed outcomes, racial and ethnic disparities are often accounted for by sociodemographic characteristics and/or inequities in access to clinical care and recovery services. Offering culturally competent treatment that considers the many barriers that one might face along their treatment and recovery journey is essential to ensuring equal access and opportunity in the treatment and recovery realm.
For scientists:Additional longitudinal research studies are needed as well as studies that utilize databases from more recent years to examine the role of race, ethnicity, and related factors on remission status. Research examining remission from specific drug use disorders will also enhance our understanding of whether certain patterns emerge for specific substances. Better understanding of the factors that account for these observed racial/ethnic disparities is also needed to develop treatment and recovery initiatives that promote equal access to services and equal opportunity for remission.
For policy makers: Racial and ethnic minorities, particularly Black individuals, may be less likely to achieve remission compared to White individuals. Prior studies have also suggested several potential sociodemographic and clinical risk factors that account for these racial/ethnic disparities. However, inconsistent methods among the few available studies on race, ethnicity, and remission make it hard to form concrete conclusions on racial/ethnic disparities in remission and the factors that account for them (e.g., socioeconomic status, discrimination, community). Additional funding for research will help expand this growing literature to advance our understanding of racial/ethnic disparities that exist in addiction, treatment, and recovery, which will ultimately help address the inequities that are faced by minority populations seeking recovery.
Although the risk of developing a substance use disorder is generally similar across individuals of various races and ethnicities, racial and ethnic minorities face barriers to recovery, including less access to addiction treatmentrelative to White individuals. Less is known about the role of race and ethnicity in recovery. In the broader population of individuals with substance use disorders, about halfto three quarters achieve full remission, meaning they no longer meet diagnostic criteria for a formal substance use disorder within the past year.Among the few studies that have examined the role of race and ethnicity, outcomes are mixed with different studies showing racial/ethnic minorities have higher, lower, and equivalent remission rates relative to White individuals. Clarifying whether or not disparities exist in remission status can ultimately inform whether new approaches to treatment and recovery support are needed to ensure all races and ethnicities have equal opportunity for achieving remission.This study examined differences in remission rates between racial/ethnic minorities and White individuals in a nationally representative sample of adults with a lifetime diagnosis of substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis of data from a cross-sectional national survey conducted in the United States between 2012 and 2013 (i.e. the National Epidemiologic Survey on Alcohol and Related Conditions-III (NESARC-III)). Individuals who identified as Black, Hispanic, and Asian were oversampled to ensure an adequate representation of these races and ethnicities, and data was ultimately weighted to represent the U.S. noninstitutionalized population.
All participants included in this study were adults ages 18 or older, with a lifetime substance use disorder (alcohol or other drug use disorder) according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Among all participants, 92% had a lifetime alcohol use disorder and 32% had a lifetime drug use disorder. The researchers grouped the 10,916 participants into 4 racial/ethnic categories: 1) Black (10%), 2) Hispanic (12%), 3) White (73%), 4) Other race/ethnicity (5%; i.e. Asian, Native Hawaiian, other Pacific Islander, American Indian or Alaska Native, and those identifying with more than one racial category).
The researchers investigated differences in demographic and clinical information among participants who were in full remission (i.e., met lifetime criteria but had no past-year symptoms when interviewed for the survey), compared to individuals who met criteria for a past year substance use disorder (i.e., not in remission). Thus, participants were asked to think about their substance use disorder symptoms before the prior year to determine lifetime diagnosis. They were also asked at the same time to think about their symptoms during the prior year to determine current diagnosis or remission. Among demographic and clinical characteristics investigated, mental and physical health were evaluated with the Short Form Health Survey for which scores range from 0 to 100 (average score = 50; higher scores indicate better health), and frequency of experiencing lifetime racial discrimination was examined via Likert scale responses where ‘1’ = ‘almost never’, ‘2’ = ‘sometimes’, ‘3’ = ‘fairly often’, ‘4’ = ‘very often’.
The researchers first characterized the percentage of individuals within each racial/ethnic group who were in remission from alcohol and other drug use disorders. Thereafter, the odds of remission were investigated by racial/ethnic group, controlling for demographic and clinical factors that differed between participants who were and were not in remission to better isolate the effect of race/ethnicity on remission.
WHAT DID THIS STUDY FIND?
Black individuals had the lowest rates of remission from substance use disorders.
Overall, 47% of participants with a lifetime substance use disorder were in remission. 91% of those in remission had a lifetime alcohol use disorder and 27% of those in remission had a lifetime drug use disorder. When remission rates were assessed within White individuals had the highest rates of remission from alcohol use disorder and drug use disorders, while Black individuals had the lowest rates of remission.
Demographic and clinical factors differed between individuals who were, and who were not, in remission.
Compared to those with a past year substance use disorder, individuals who were in remission were more likely to be older (average age of 47 vs. 37 years), married (65% vs. 43%) or widowed (3% vs. 2%), retired (14% vs. 5%), and military veterans (15% vs. 8%). They were also more likely to have Medicare health insurance (18% vs. 10%), a higher body mass index (average BMI of 29 vs. 27), better mental health (average score of 50 vs. 47 on the Short Form Health Survey), and to attend religious services more frequently (average of ‘a few times a year’ vs. ‘once a year’).
Individuals who had not remitted were more likely than those in remission to be unemployed (13% vs. 7%), never married (40% vs. 16%), to have a past year (2% vs. 1%) or lifetime (4% vs. 2%) psychotic disorder, a yearly income of less than $20,000 (29% vs. 18%), and better physical health (average score of 51 vs. 49 the Short Form Health Survey). They were also more likely to have a lifetime sedative (4% vs. 3%) or opioid (9% vs. 5%) use disorder, to have experienced a past year suicide attempt (0.7% vs. 0.2%), past year trouble with the police (6% vs. 2%), past year houselessness (4% vs. 2%), and more frequent racial discrimination (average score of 1.3 vs. 1.2). This group also had higher rates of lifetime sedative use disorder (4% vs. 3%) and opioid use disorder (9% vs. 5%).
Black, Hispanic, and other races/ethnicities were less likely to be in remission.
Controlling for other demographic and clinical factors associated with remission, the odds of being in remission from a substance use disorder were 51% lower in Blacks, 32% lower in Hispanics, and 34% lower in those of other races/ethnicities, relative to Whites. When the type of use disorder was considered, all minority groups were less likely than Whites to be in remission from both alcohol and drug use disorders except for the other race/ethnicity group, who had a similar likelihood of remission from drug use disorders compared to Whites.
Figure 2. The percent reduction in the odds of remission by race and disorder type, independent of other factors that influenced remission.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand the disparities that exist in addiction recovery, which can ultimately inform new treatment and recovery efforts. The researchers found that racial and ethnic minorities, particularly Black individuals, are significantly less likely to achieve remission from substance use disorders relative to Whites.
The overall remission rate observed in this study was similar to those of prior studies, with about half of individuals with lifetime substance use disorders achieving full remission. The factors associated with remission status that emerged in this study (e.g., age, opioid use disorder, marital status, psychiatric comorbidities, etc.) were also generally consistent withpreviousresearch. Yet, racial and ethnic differences observed in this study add to a mixed literature on whether or not remission rates vary by minority status. Though this literature is somewhat limited, prior research has generally observed higher rates of remission among Blacks and Hispanics compared to Whites, or equivalent rates of remission across races/ethnicities when controlling for various demographic factors (e.g., age, education, marital status).
Interestingly, racial and ethnic differences in remission status persisted in this study, even when controlling for important demographic and clinical characteristics. It could be that differences in methods across these different studies might account for the different findings. For example, this study examined remission from a lifetime substance use disorder that someone may have initiated either recently or long ago, whereas other studies have largely focused on remission that was achieved over the previous few years. Or it could be due to differences in study design (e.g., cross-sectional/retrospective vs longitudinal) or both. A nationally representative longitudinal study of individuals with alcohol use disorder, for example, showed that Black and Latino individuals were just as likely to be in remission as White individuals 3 years later. Thus, it may be that long-term remission (e.g., being in recovery for 5 years or more) from a lifetime substance use disorder is less prevalent among racial and ethnic minorities. The way substance use disorder is defined and how disorder criteria are evaluated across studies may also contribute to inconsistent outcomes. Additional research is needed to formally study racial/ethnic differences in remission, particularly longitudinal research, given that cross-sectional studies determine lifetime substance use disorder by asking individuals to remember past events and symptoms, which relies on accurate recall.
The factors controlled for in different studies also vary. Race/ethnicity remained the strongest predictor of remission in this study, with the demographic and clinical characteristics assessed here having a less robust effect when race/ethnicity were introduced into the researchers’ statistical models. It may be that other structural and social inequities that were not assessed in this study underlie these racial and ethnic disparities. For example, other social, community, and treatment/recovery support factors that differ by race/ethnicity and influence one’s ability to achieve remission (e.g., access to competent treatment and recovery services, or recovery capital) might produce lower rates of remission among certain racial/ethnic minority groups. With other studies finding higher or equivalent rates of remission among racial and ethnic minorities compared to Whites, additional research can help identify racial and ethnic disparities in short- and long-term recovery and help explain the factors that underlie these disparities.
This study did not include an evaluation of the impact of treatment/recovery service use or a number of other relevant factors that might underlie racial and ethnic disparities in remission rates. Additional research is needed to determine factors that influence these rates to better address inequities.
This study is based on a cross-sectional survey and can’t speak to causal effects, but nevertheless highlights associations between race, ethnicity, sociodemographic factors, and remission. Longitudinal studies that track individuals over long periods of time will help us better understand the role of these factors in the course of remission and recovery. Studies that assess drug use disorders with respect to different drug types will also be useful for informing the development of equitable treatment and recovery efforts.
BOTTOM LINE
Compared to Whites, racial and ethnic minorities showed a reduced likelihood of achieving remission from substance use disorders in the current study, even when controlling for a number of factors that differed between them and Whites and that were relevant to remission. Findings to date within this limited literature are mixed, however, with some studies showing increased, decreased, or equivalent remission rates between racial/ethnic minorities and Whites. This was a cross-sectional study that evaluated remission from a lifetime substance use disorder and the way remission is defined and observed across studies might account for the mixed findings across different studies that have examined this question. There is a need for additional research to learn more about what factors account for disparities so they can be addressed with culturally competent policies and individualized services. Research to date suggests there are some potential candidates that can be targeted to help address these disparities, such as lower socioeconomic status and unemployment that are often lower among minorities. This study contributes to a growing literature that advances our understanding of racial/ethnic disparities that exist in addiction, treatment, and remission, which may help address the inequities that are often faced by minority populations seeking recovery.
For individuals and families seeking recovery: Individuals who identify as racial or ethnic minorities might face barriers to remission that may be accounted for by sociodemographic characteristics and/or inequities in access to treatment and recovery services. Individuals and families seeking recovery should seek culturally competent care that does not discriminate against race, ethnicity, or those from disadvantaged backgrounds. Many states are developing programs that can help combat barriers to treatment and recovery, such as financial support for treatment, assistance with obtaining education and work skills needed to support recovery, and free local recovery support programs that boost social support for recovery. Interested individuals should check out their state’s websites and local recovery communities to find out more on these novel opportunities in your area that can help combat barriers to treatment and recovery.
For treatment professionals and treatment systems: Individuals who identify as racial or ethnic minorities might face barriers to remission relative to White individuals. Though the literature in this area is limited with mixed outcomes, racial and ethnic disparities are often accounted for by sociodemographic characteristics and/or inequities in access to clinical care and recovery services. Offering culturally competent treatment that considers the many barriers that one might face along their treatment and recovery journey is essential to ensuring equal access and opportunity in the treatment and recovery realm.
For scientists:Additional longitudinal research studies are needed as well as studies that utilize databases from more recent years to examine the role of race, ethnicity, and related factors on remission status. Research examining remission from specific drug use disorders will also enhance our understanding of whether certain patterns emerge for specific substances. Better understanding of the factors that account for these observed racial/ethnic disparities is also needed to develop treatment and recovery initiatives that promote equal access to services and equal opportunity for remission.
For policy makers: Racial and ethnic minorities, particularly Black individuals, may be less likely to achieve remission compared to White individuals. Prior studies have also suggested several potential sociodemographic and clinical risk factors that account for these racial/ethnic disparities. However, inconsistent methods among the few available studies on race, ethnicity, and remission make it hard to form concrete conclusions on racial/ethnic disparities in remission and the factors that account for them (e.g., socioeconomic status, discrimination, community). Additional funding for research will help expand this growing literature to advance our understanding of racial/ethnic disparities that exist in addiction, treatment, and recovery, which will ultimately help address the inequities that are faced by minority populations seeking recovery.