Historically Asian Americans have been viewed as the “model minority”– an overgeneralized belief that Asian Americans overcome social, economic, and political barriers through hard work and diligence unlike other minority groups. Such beliefs, in part, may lead healthcare providers to assume Asian American patients may not be susceptible to alcohol use disorder, reducing their need to be screened for harmful and hazardous drinking. This may explain why Asian Americans with alcohol use disorder are less likely than members of other racial/ethnic backgrounds to receive AUD treatment. This is troubling since research suggests that Asian Americans may be even more vulnerable to alcohol-related health problems than other racial/ethnic groups. Research on screening disparities between Asian Americans and other racial/ethnic minorities could help contextualize this disparity and present a potential point of intervention for public health administrators and healthcare professionals.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis of the 2015-2019 National Survey on Drug Use and Health, a cross-sectional nationally representative survey conducted in the USA each year. The sample used for the current analyses (n=123,002) consisted of adults who reported any past year drinking and at least one healthcare visit or interaction (e.g., a primary care office visit, emergency room interaction, etc.).
For the current sample, alcohol use was measured in multiple ways. For instance, the authors used number of days participants used alcohol in the past year (range: 1–365 days) and in the past month (range: 0–30 days). Past month binge drinking (i.e., 4+/5+ drinks on one occasion for females or males, respectively) frequency (range: 0–30 days) was also measured. The authors also created categorical alcohol use frequency measures for past year and month drinking (i.e., 0, 1, 2, 3+ days in the past year/month). Past year alcohol use disorder symptomology was defined by DSM-IV criteria for past-year alcohol abuse and/or alcohol dependence.
As part of the national survey, participants were asked a series of questions pertaining to their interactions with healthcare providers (e.g., “During the past 12 months, did any doctor or other healthcare professional ask, either in person or on a form if you drink alcohol?”). Sampled participants were also asked to describe any discussions they had in person with a doctor or other health professional regarding their alcohol use. Participants were reported content details of said discussions (e.g., if the healthcare worker asked them about the amount of alcohol they use, how often they used alcohol, any alcohol-related problems they experienced, etc.). Participants were also asked to describe if their provider offered to give them information about alcohol use treatment. The authors than created a three-level alcohol screening/discussions indicator distinguishing (1) any alcohol discussion with a provider (e.g. reported discussing alcohol use frequency with a provider); (2) any alcohol screening without discussion (e.g. reported being asked about alcohol on an intake form, but was not asked about alcohol by their provider) and (3) no alcohol screening or discussion (i.e., not being asked about alcohol use at any stage of the healthcare interaction).
Once all of the data were collected, the authors utilized data weighting (a statistical technique to adjust data to make it more representative of the overall US population). Next the authors created statistical models estimating associations between the three-level screening/discussions outcome (i.e., any alcohol discussion, alcohol screening without discussions, or no alcohol screening/discussions with providers) across racial/ethnic groups. Finally, the authors created a separate statistical model to estimate the odds of alcohol use disorder treatment utilization across all participants with alcohol use disorder symptomology. All models took individual variations in demographics into account (e.g., age, gender, income, etc.).
Sampled participants were majority White (70.4%) with the remaining race/ethnicities being Hispanic (12.9%), Black (10.2%), and Asian American (4.4%). The sample was roughly equal parts female (53.3%) and male (47.7%). Most participants were 50 years of age or older (44.4%). Most participants earned at least $75,000 a year (45.7%) and had some form of health insurance (93.3%).
WHAT DID THIS STUDY FIND?
Asian Americans were less likely to be screened for alcohol use.
For individuals with any drinking and at least one healthcare visit in the past year, Asian Americans were less likely than all other racial/ethnic groups to receive alcohol use screening. Specifically, about a quarter of Asian American participants reported any screening for alcohol use with their doctors. In contrast, about 30% of Black Americans reported being screened for alcohol use by their doctors at healthcare visits – 1.5 times more likely than Asian Americans. This was independent of other factors such as age and income as well as the presence of alcohol use disorder.
Asian Americans had lower rates of binge drinking than other groups.
More than half of the Asian Americans sampled reported having at least one drink between 1-36 days in the past year. Roughly 25% of Asian Americans reported binge drinking in the past month. In contrast, 35.2-42.1% of participants from other racial/ethnic groups reported drinking that much in the past month.
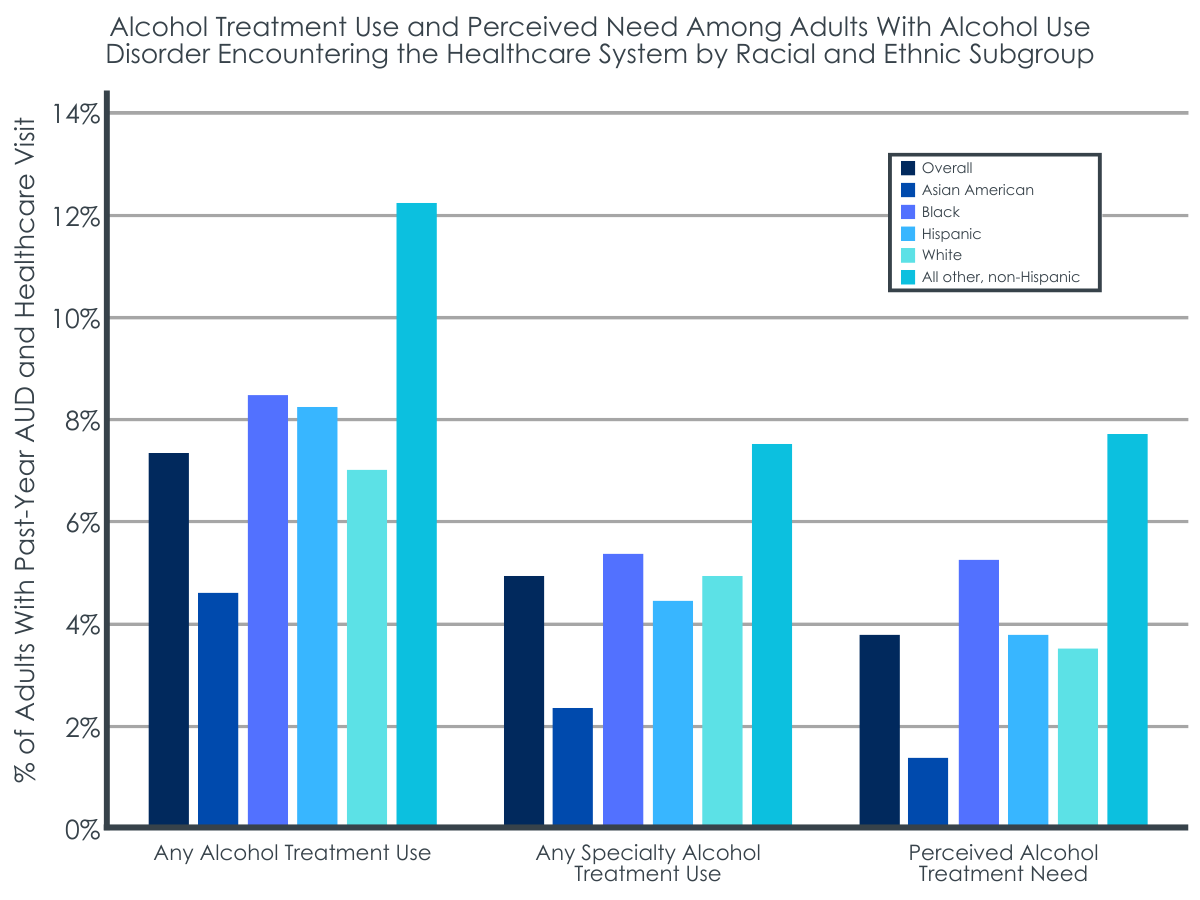
Asian Americans with alcohol use disorder engaged with treatment as much as other groups.
Relative to the rest of the sample, Asian Americans had the lowest rates of past year alcohol use disorder symptoms. However, Asian Americans who did have an alcohol use disorder engaged with treatment at rates similar to White, Black, or Hispanic people when examined as individual groups, though lower rates when compared to all non-Hispanic individuals as a whole (e.g., Non-Hispanic White, Non-Hispanic Black, etc.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests a need to intervene on the differential alcohol screening of patients.
This secondary analysis in a nationally representative sample showed that Asian American individuals may be less likely to be screened for alcohol use at healthcare visits. This may be due to healthcare providers’ racial biases (e.g., assumptions about their Asian American patients’ alcohol use) impacting their bedside manner. Past research somewhat corroborates this claim- Asian Americans have reported poorer patient-provider interactions and difficulties communicating with their providers than other races/ethnicities. Although it was true that the sampled Asian Americans engaged in lower levels of drinking and had fewer alcohol use disorder symptoms relative to other races/ethnicities this does not mean that this population could not still benefit from alcohol screening. That is, Asian Americans did still use alcohol and research suggests that Asian Americans may be even more vulnerable to alcohol-related health problems than other racial/ethnic groups. The study also showed that Asian Americans were just as likely to engage with services if they have alcohol use disorder. This suggests that if Asian Americans are offered alcohol use disorder treatment they may be as likely to utilize such services.
It is important for healthcare professionals to screen for alcohol at healthcare visits for all patients. Although the present analyses focused on racial/ethnic disparities in alcohol use screening, it is important to note that among the overall sample – who drank in the past year and interacted with the healthcare system – roughly 18% reported no alcohol screening whatsoever. This is significant as all participants reported past year alcohol use. Given the long list of health issues and premature deaths associated with alcohol use, it is critical for healthcare providers to know their patient’s alcohol use behavior.
The study also has implications for disparities in alcohol screening across racial/ethnic subgroups. The researchers propose that healthcare providers’ attitudes/beliefs about Asian Americans may have influenced their decision to not screen for alcohol use with their patients. Although the present study did not directly measure this, previous research does support this claim. Therefore, it may be necessary to further research and address racial biases among healthcare providers.
The sample collapsed racial/ethnic subgroups together into a single category. Asia is a huge continent with many countries with distinct cultures. Research suggests that sub populations within Asia have different alcohol risk behavior prevalence. Collapsing participants into a single “Asian” category obfuscates potential behavioral differences between individuals- offering an inaccurate view of public health impact of alcohol on Asian sub-populations.
In a similar vein, the present research did not specify the citizenship status of participants. Studies suggest that having immigrated to the US may play a role in drinking behavior of Asian Americans. It remains unclear why this relationship exists, but it is possible that US-born Asian Americans may have experienced more acculturation to US culture, which contributes to their alcohol use patterns.
The study relied on self-report on measures of screening and discussions with providers which were not verified. It is possible that such data were impacted by recall bias and not completely accurate. It is unclear whether any differential unwillingness to report alcohol use related screening and/or treatment on the survey might be influencing the observed differences on screening rates found in this study.
BOTTOM LINE
Asian Americans were shown to be less likely to be asked about their alcohol use by their doctors relative to all other racial/ethnic groups. The present research implies that there is a need to raise awareness among healthcare providers of the health impact of alcohol use on the Asian American community. In addition, there may be a need to develop culturally tailored alcohol interventions for Asian Americans. The goal of such interventions may be to disseminate information on alcohol use and the unique ways it impacts the Asian American community.
For individuals and families seeking recovery: Given their lower likelihood of alcohol screening experiences during healthcare visits, in may be important for Asian American individuals, to advocate for themselves in healthcare environments if concerned about their alcohol use It is possible that healthcare providers may be unaware of their own biases. To maximize adequate quality care, those seeking treatment may do well to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: Those providing treatment to, and/or work in, healthcare system settings, should be mindful to ask patients (regardless of race/ethnicity) about their alcohol and other drug use. As alcohol can have myriad health impacts, gathering information on drinking is clinically critical. In addition, providers should be aware of resources to support alcohol-related care. The National Institute on Alcohol and Alcoholism has recently published a guide for healthcare professionals outlining available resources for alcohol use problems.
For scientists:Scientists may want to investigate the ways in which healthcare professionals’ attitudes/beliefs impact interactions with Asian American patients and also any differential reporting biases that may exist among certain racial/ethnic groups. The extant literature on cultural bias in medicine has already established that care can be impacted by gender and racial/ethnic biases. However little research has specifically examined how different types of clinician and patient reporting biases impact care provided to Asian Americans. There is a need to better understand how biases may be impacting care received by Asian Americans.
For policy makers: The discussed results suggest that Asian Americans may be underserved by the US healthcare system regarding alcohol-related problems and conditions. Policy makers could consider strategies to increase awareness of alcohol use among the Asian American community and its health impacts. This could take the form of public health campaigns tailored to reach the Asian American community and the practitioners who serve them. In addition, medical school administrators could further emphasize the importance of universally applying alcohol use screening at routine health visits to medical students and trainees
Historically Asian Americans have been viewed as the “model minority”– an overgeneralized belief that Asian Americans overcome social, economic, and political barriers through hard work and diligence unlike other minority groups. Such beliefs, in part, may lead healthcare providers to assume Asian American patients may not be susceptible to alcohol use disorder, reducing their need to be screened for harmful and hazardous drinking. This may explain why Asian Americans with alcohol use disorder are less likely than members of other racial/ethnic backgrounds to receive AUD treatment. This is troubling since research suggests that Asian Americans may be even more vulnerable to alcohol-related health problems than other racial/ethnic groups. Research on screening disparities between Asian Americans and other racial/ethnic minorities could help contextualize this disparity and present a potential point of intervention for public health administrators and healthcare professionals.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis of the 2015-2019 National Survey on Drug Use and Health, a cross-sectional nationally representative survey conducted in the USA each year. The sample used for the current analyses (n=123,002) consisted of adults who reported any past year drinking and at least one healthcare visit or interaction (e.g., a primary care office visit, emergency room interaction, etc.).
For the current sample, alcohol use was measured in multiple ways. For instance, the authors used number of days participants used alcohol in the past year (range: 1–365 days) and in the past month (range: 0–30 days). Past month binge drinking (i.e., 4+/5+ drinks on one occasion for females or males, respectively) frequency (range: 0–30 days) was also measured. The authors also created categorical alcohol use frequency measures for past year and month drinking (i.e., 0, 1, 2, 3+ days in the past year/month). Past year alcohol use disorder symptomology was defined by DSM-IV criteria for past-year alcohol abuse and/or alcohol dependence.
As part of the national survey, participants were asked a series of questions pertaining to their interactions with healthcare providers (e.g., “During the past 12 months, did any doctor or other healthcare professional ask, either in person or on a form if you drink alcohol?”). Sampled participants were also asked to describe any discussions they had in person with a doctor or other health professional regarding their alcohol use. Participants were reported content details of said discussions (e.g., if the healthcare worker asked them about the amount of alcohol they use, how often they used alcohol, any alcohol-related problems they experienced, etc.). Participants were also asked to describe if their provider offered to give them information about alcohol use treatment. The authors than created a three-level alcohol screening/discussions indicator distinguishing (1) any alcohol discussion with a provider (e.g. reported discussing alcohol use frequency with a provider); (2) any alcohol screening without discussion (e.g. reported being asked about alcohol on an intake form, but was not asked about alcohol by their provider) and (3) no alcohol screening or discussion (i.e., not being asked about alcohol use at any stage of the healthcare interaction).
Once all of the data were collected, the authors utilized data weighting (a statistical technique to adjust data to make it more representative of the overall US population). Next the authors created statistical models estimating associations between the three-level screening/discussions outcome (i.e., any alcohol discussion, alcohol screening without discussions, or no alcohol screening/discussions with providers) across racial/ethnic groups. Finally, the authors created a separate statistical model to estimate the odds of alcohol use disorder treatment utilization across all participants with alcohol use disorder symptomology. All models took individual variations in demographics into account (e.g., age, gender, income, etc.).
Sampled participants were majority White (70.4%) with the remaining race/ethnicities being Hispanic (12.9%), Black (10.2%), and Asian American (4.4%). The sample was roughly equal parts female (53.3%) and male (47.7%). Most participants were 50 years of age or older (44.4%). Most participants earned at least $75,000 a year (45.7%) and had some form of health insurance (93.3%).
WHAT DID THIS STUDY FIND?
Asian Americans were less likely to be screened for alcohol use.
For individuals with any drinking and at least one healthcare visit in the past year, Asian Americans were less likely than all other racial/ethnic groups to receive alcohol use screening. Specifically, about a quarter of Asian American participants reported any screening for alcohol use with their doctors. In contrast, about 30% of Black Americans reported being screened for alcohol use by their doctors at healthcare visits – 1.5 times more likely than Asian Americans. This was independent of other factors such as age and income as well as the presence of alcohol use disorder.
Asian Americans had lower rates of binge drinking than other groups.
More than half of the Asian Americans sampled reported having at least one drink between 1-36 days in the past year. Roughly 25% of Asian Americans reported binge drinking in the past month. In contrast, 35.2-42.1% of participants from other racial/ethnic groups reported drinking that much in the past month.
Asian Americans with alcohol use disorder engaged with treatment as much as other groups.
Relative to the rest of the sample, Asian Americans had the lowest rates of past year alcohol use disorder symptoms. However, Asian Americans who did have an alcohol use disorder engaged with treatment at rates similar to White, Black, or Hispanic people when examined as individual groups, though lower rates when compared to all non-Hispanic individuals as a whole (e.g., Non-Hispanic White, Non-Hispanic Black, etc.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests a need to intervene on the differential alcohol screening of patients.
This secondary analysis in a nationally representative sample showed that Asian American individuals may be less likely to be screened for alcohol use at healthcare visits. This may be due to healthcare providers’ racial biases (e.g., assumptions about their Asian American patients’ alcohol use) impacting their bedside manner. Past research somewhat corroborates this claim- Asian Americans have reported poorer patient-provider interactions and difficulties communicating with their providers than other races/ethnicities. Although it was true that the sampled Asian Americans engaged in lower levels of drinking and had fewer alcohol use disorder symptoms relative to other races/ethnicities this does not mean that this population could not still benefit from alcohol screening. That is, Asian Americans did still use alcohol and research suggests that Asian Americans may be even more vulnerable to alcohol-related health problems than other racial/ethnic groups. The study also showed that Asian Americans were just as likely to engage with services if they have alcohol use disorder. This suggests that if Asian Americans are offered alcohol use disorder treatment they may be as likely to utilize such services.
It is important for healthcare professionals to screen for alcohol at healthcare visits for all patients. Although the present analyses focused on racial/ethnic disparities in alcohol use screening, it is important to note that among the overall sample – who drank in the past year and interacted with the healthcare system – roughly 18% reported no alcohol screening whatsoever. This is significant as all participants reported past year alcohol use. Given the long list of health issues and premature deaths associated with alcohol use, it is critical for healthcare providers to know their patient’s alcohol use behavior.
The study also has implications for disparities in alcohol screening across racial/ethnic subgroups. The researchers propose that healthcare providers’ attitudes/beliefs about Asian Americans may have influenced their decision to not screen for alcohol use with their patients. Although the present study did not directly measure this, previous research does support this claim. Therefore, it may be necessary to further research and address racial biases among healthcare providers.
The sample collapsed racial/ethnic subgroups together into a single category. Asia is a huge continent with many countries with distinct cultures. Research suggests that sub populations within Asia have different alcohol risk behavior prevalence. Collapsing participants into a single “Asian” category obfuscates potential behavioral differences between individuals- offering an inaccurate view of public health impact of alcohol on Asian sub-populations.
In a similar vein, the present research did not specify the citizenship status of participants. Studies suggest that having immigrated to the US may play a role in drinking behavior of Asian Americans. It remains unclear why this relationship exists, but it is possible that US-born Asian Americans may have experienced more acculturation to US culture, which contributes to their alcohol use patterns.
The study relied on self-report on measures of screening and discussions with providers which were not verified. It is possible that such data were impacted by recall bias and not completely accurate. It is unclear whether any differential unwillingness to report alcohol use related screening and/or treatment on the survey might be influencing the observed differences on screening rates found in this study.
BOTTOM LINE
Asian Americans were shown to be less likely to be asked about their alcohol use by their doctors relative to all other racial/ethnic groups. The present research implies that there is a need to raise awareness among healthcare providers of the health impact of alcohol use on the Asian American community. In addition, there may be a need to develop culturally tailored alcohol interventions for Asian Americans. The goal of such interventions may be to disseminate information on alcohol use and the unique ways it impacts the Asian American community.
For individuals and families seeking recovery: Given their lower likelihood of alcohol screening experiences during healthcare visits, in may be important for Asian American individuals, to advocate for themselves in healthcare environments if concerned about their alcohol use It is possible that healthcare providers may be unaware of their own biases. To maximize adequate quality care, those seeking treatment may do well to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: Those providing treatment to, and/or work in, healthcare system settings, should be mindful to ask patients (regardless of race/ethnicity) about their alcohol and other drug use. As alcohol can have myriad health impacts, gathering information on drinking is clinically critical. In addition, providers should be aware of resources to support alcohol-related care. The National Institute on Alcohol and Alcoholism has recently published a guide for healthcare professionals outlining available resources for alcohol use problems.
For scientists:Scientists may want to investigate the ways in which healthcare professionals’ attitudes/beliefs impact interactions with Asian American patients and also any differential reporting biases that may exist among certain racial/ethnic groups. The extant literature on cultural bias in medicine has already established that care can be impacted by gender and racial/ethnic biases. However little research has specifically examined how different types of clinician and patient reporting biases impact care provided to Asian Americans. There is a need to better understand how biases may be impacting care received by Asian Americans.
For policy makers: The discussed results suggest that Asian Americans may be underserved by the US healthcare system regarding alcohol-related problems and conditions. Policy makers could consider strategies to increase awareness of alcohol use among the Asian American community and its health impacts. This could take the form of public health campaigns tailored to reach the Asian American community and the practitioners who serve them. In addition, medical school administrators could further emphasize the importance of universally applying alcohol use screening at routine health visits to medical students and trainees
Historically Asian Americans have been viewed as the “model minority”– an overgeneralized belief that Asian Americans overcome social, economic, and political barriers through hard work and diligence unlike other minority groups. Such beliefs, in part, may lead healthcare providers to assume Asian American patients may not be susceptible to alcohol use disorder, reducing their need to be screened for harmful and hazardous drinking. This may explain why Asian Americans with alcohol use disorder are less likely than members of other racial/ethnic backgrounds to receive AUD treatment. This is troubling since research suggests that Asian Americans may be even more vulnerable to alcohol-related health problems than other racial/ethnic groups. Research on screening disparities between Asian Americans and other racial/ethnic minorities could help contextualize this disparity and present a potential point of intervention for public health administrators and healthcare professionals.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis of the 2015-2019 National Survey on Drug Use and Health, a cross-sectional nationally representative survey conducted in the USA each year. The sample used for the current analyses (n=123,002) consisted of adults who reported any past year drinking and at least one healthcare visit or interaction (e.g., a primary care office visit, emergency room interaction, etc.).
For the current sample, alcohol use was measured in multiple ways. For instance, the authors used number of days participants used alcohol in the past year (range: 1–365 days) and in the past month (range: 0–30 days). Past month binge drinking (i.e., 4+/5+ drinks on one occasion for females or males, respectively) frequency (range: 0–30 days) was also measured. The authors also created categorical alcohol use frequency measures for past year and month drinking (i.e., 0, 1, 2, 3+ days in the past year/month). Past year alcohol use disorder symptomology was defined by DSM-IV criteria for past-year alcohol abuse and/or alcohol dependence.
As part of the national survey, participants were asked a series of questions pertaining to their interactions with healthcare providers (e.g., “During the past 12 months, did any doctor or other healthcare professional ask, either in person or on a form if you drink alcohol?”). Sampled participants were also asked to describe any discussions they had in person with a doctor or other health professional regarding their alcohol use. Participants were reported content details of said discussions (e.g., if the healthcare worker asked them about the amount of alcohol they use, how often they used alcohol, any alcohol-related problems they experienced, etc.). Participants were also asked to describe if their provider offered to give them information about alcohol use treatment. The authors than created a three-level alcohol screening/discussions indicator distinguishing (1) any alcohol discussion with a provider (e.g. reported discussing alcohol use frequency with a provider); (2) any alcohol screening without discussion (e.g. reported being asked about alcohol on an intake form, but was not asked about alcohol by their provider) and (3) no alcohol screening or discussion (i.e., not being asked about alcohol use at any stage of the healthcare interaction).
Once all of the data were collected, the authors utilized data weighting (a statistical technique to adjust data to make it more representative of the overall US population). Next the authors created statistical models estimating associations between the three-level screening/discussions outcome (i.e., any alcohol discussion, alcohol screening without discussions, or no alcohol screening/discussions with providers) across racial/ethnic groups. Finally, the authors created a separate statistical model to estimate the odds of alcohol use disorder treatment utilization across all participants with alcohol use disorder symptomology. All models took individual variations in demographics into account (e.g., age, gender, income, etc.).
Sampled participants were majority White (70.4%) with the remaining race/ethnicities being Hispanic (12.9%), Black (10.2%), and Asian American (4.4%). The sample was roughly equal parts female (53.3%) and male (47.7%). Most participants were 50 years of age or older (44.4%). Most participants earned at least $75,000 a year (45.7%) and had some form of health insurance (93.3%).
WHAT DID THIS STUDY FIND?
Asian Americans were less likely to be screened for alcohol use.
For individuals with any drinking and at least one healthcare visit in the past year, Asian Americans were less likely than all other racial/ethnic groups to receive alcohol use screening. Specifically, about a quarter of Asian American participants reported any screening for alcohol use with their doctors. In contrast, about 30% of Black Americans reported being screened for alcohol use by their doctors at healthcare visits – 1.5 times more likely than Asian Americans. This was independent of other factors such as age and income as well as the presence of alcohol use disorder.
Asian Americans had lower rates of binge drinking than other groups.
More than half of the Asian Americans sampled reported having at least one drink between 1-36 days in the past year. Roughly 25% of Asian Americans reported binge drinking in the past month. In contrast, 35.2-42.1% of participants from other racial/ethnic groups reported drinking that much in the past month.
Asian Americans with alcohol use disorder engaged with treatment as much as other groups.
Relative to the rest of the sample, Asian Americans had the lowest rates of past year alcohol use disorder symptoms. However, Asian Americans who did have an alcohol use disorder engaged with treatment at rates similar to White, Black, or Hispanic people when examined as individual groups, though lower rates when compared to all non-Hispanic individuals as a whole (e.g., Non-Hispanic White, Non-Hispanic Black, etc.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests a need to intervene on the differential alcohol screening of patients.
This secondary analysis in a nationally representative sample showed that Asian American individuals may be less likely to be screened for alcohol use at healthcare visits. This may be due to healthcare providers’ racial biases (e.g., assumptions about their Asian American patients’ alcohol use) impacting their bedside manner. Past research somewhat corroborates this claim- Asian Americans have reported poorer patient-provider interactions and difficulties communicating with their providers than other races/ethnicities. Although it was true that the sampled Asian Americans engaged in lower levels of drinking and had fewer alcohol use disorder symptoms relative to other races/ethnicities this does not mean that this population could not still benefit from alcohol screening. That is, Asian Americans did still use alcohol and research suggests that Asian Americans may be even more vulnerable to alcohol-related health problems than other racial/ethnic groups. The study also showed that Asian Americans were just as likely to engage with services if they have alcohol use disorder. This suggests that if Asian Americans are offered alcohol use disorder treatment they may be as likely to utilize such services.
It is important for healthcare professionals to screen for alcohol at healthcare visits for all patients. Although the present analyses focused on racial/ethnic disparities in alcohol use screening, it is important to note that among the overall sample – who drank in the past year and interacted with the healthcare system – roughly 18% reported no alcohol screening whatsoever. This is significant as all participants reported past year alcohol use. Given the long list of health issues and premature deaths associated with alcohol use, it is critical for healthcare providers to know their patient’s alcohol use behavior.
The study also has implications for disparities in alcohol screening across racial/ethnic subgroups. The researchers propose that healthcare providers’ attitudes/beliefs about Asian Americans may have influenced their decision to not screen for alcohol use with their patients. Although the present study did not directly measure this, previous research does support this claim. Therefore, it may be necessary to further research and address racial biases among healthcare providers.
The sample collapsed racial/ethnic subgroups together into a single category. Asia is a huge continent with many countries with distinct cultures. Research suggests that sub populations within Asia have different alcohol risk behavior prevalence. Collapsing participants into a single “Asian” category obfuscates potential behavioral differences between individuals- offering an inaccurate view of public health impact of alcohol on Asian sub-populations.
In a similar vein, the present research did not specify the citizenship status of participants. Studies suggest that having immigrated to the US may play a role in drinking behavior of Asian Americans. It remains unclear why this relationship exists, but it is possible that US-born Asian Americans may have experienced more acculturation to US culture, which contributes to their alcohol use patterns.
The study relied on self-report on measures of screening and discussions with providers which were not verified. It is possible that such data were impacted by recall bias and not completely accurate. It is unclear whether any differential unwillingness to report alcohol use related screening and/or treatment on the survey might be influencing the observed differences on screening rates found in this study.
BOTTOM LINE
Asian Americans were shown to be less likely to be asked about their alcohol use by their doctors relative to all other racial/ethnic groups. The present research implies that there is a need to raise awareness among healthcare providers of the health impact of alcohol use on the Asian American community. In addition, there may be a need to develop culturally tailored alcohol interventions for Asian Americans. The goal of such interventions may be to disseminate information on alcohol use and the unique ways it impacts the Asian American community.
For individuals and families seeking recovery: Given their lower likelihood of alcohol screening experiences during healthcare visits, in may be important for Asian American individuals, to advocate for themselves in healthcare environments if concerned about their alcohol use It is possible that healthcare providers may be unaware of their own biases. To maximize adequate quality care, those seeking treatment may do well to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: Those providing treatment to, and/or work in, healthcare system settings, should be mindful to ask patients (regardless of race/ethnicity) about their alcohol and other drug use. As alcohol can have myriad health impacts, gathering information on drinking is clinically critical. In addition, providers should be aware of resources to support alcohol-related care. The National Institute on Alcohol and Alcoholism has recently published a guide for healthcare professionals outlining available resources for alcohol use problems.
For scientists:Scientists may want to investigate the ways in which healthcare professionals’ attitudes/beliefs impact interactions with Asian American patients and also any differential reporting biases that may exist among certain racial/ethnic groups. The extant literature on cultural bias in medicine has already established that care can be impacted by gender and racial/ethnic biases. However little research has specifically examined how different types of clinician and patient reporting biases impact care provided to Asian Americans. There is a need to better understand how biases may be impacting care received by Asian Americans.
For policy makers: The discussed results suggest that Asian Americans may be underserved by the US healthcare system regarding alcohol-related problems and conditions. Policy makers could consider strategies to increase awareness of alcohol use among the Asian American community and its health impacts. This could take the form of public health campaigns tailored to reach the Asian American community and the practitioners who serve them. In addition, medical school administrators could further emphasize the importance of universally applying alcohol use screening at routine health visits to medical students and trainees