Many achieve recovery from alcohol use disorder despite continued use, but how do they compare to those who abstain?
Increasingly, researchers have identified the benefits of supporting recovery goals that include substance use reductions in addition to goals of total abstinence. Questions remain however, about the respective risks and benefits of this approach in comparison with abstinence. This study examines if individuals receiving treatment for alcohol use disorder and co-occurring anxiety disorders have better outcomes depending on their alcohol use status following residential treatment.
Historically, the vast majority of substance use disorder treatment programs in the United States have adhered to an abstinence-based model of recovery. In other words, they espoused recovery through complete abstinence from alcohol and other drugs regardless of patients’ primary substance/s. The rationale behind this approach is that relapse can be so devastating and sometimes fatal, especially for the more severe cases that use residential treatment, that any use of any psychoactive substance—even one that a patient has not used or used very much previously—might impair cognitive functioning including appraisal and judgement, thus increasing the risk for a bad decision that could in turn increase risk for relapse to their primary substance, or even result in an addiction to the new drug. In recent years however, some studies have begun to show that a subset of individuals can achieve remission from substance use disorder by reducing their use of one or more substances, rather than completely abstaining, especially those patients with less severe forms of alcohol or other drug use disorder.
While a growing body of research indicates many can and do achieve remission in this way, questions remain about who can reasonably expect to recover through a non-abstinent pathway, and how continued substance use (versus total abstinence) potentially helps or hinders gains in psychological well-being and general functioning in the recovery process. Such research will be important for informing clinical and public health recommendations.
Using cross-sectional data from the National Recovery Study conducted by the Recovery Research Institute, researchers previously found that lower-risk substance use status (i.e., abstinence or continued use of only a secondary substance, versus use of a primary substance or a primary and secondary substance) across all recovery stages was associated with greater self-esteem, happiness, quality of life and functioning, as well as less psychological distress. In other words, the closer a participant was to the abstinent end of the substance use spectrum, the better off they were in terms of quality of life and well-being.
That study focused on a broad sample of people in the US population self-identifying as having resolved a prior problem with alcohol or other drugs. This study extended this research by asking the same questions but with a sample of individuals with diagnosed alcohol use disorder, and co-occurring anxiety disorders, who may, on average, have had more severe addiction severity than the National Recovery Study sample.
HOW WAS THIS STUDY CONDUCTED?
This was an observational study that included 327 individuals with alcohol use disorder and co-occurring anxiety disorders who were assessed for alcohol use as well as psychological well-being and general functioning at treatment baseline, and then at 1, 4, and 12 months following residential treatment.
Participants were assessed at the start of residential treatment (i.e., baseline), and again at 1, 4, and 12 months on a range of measures gauging psychological well-being and functioning. These included, 1) addiction severity measured with the Addiction Severity Index, 2) quality of life measured by the Quality of Life Enjoyment and Satisfaction Questionnaire, 3) depressive symptoms measured by the Beck Depression Inventory, and 4) trait anxiety measured using the State-Trait Anxiety Inventory. Functional measures included, 1) number of days working, 2) number of days with interpersonal conflicts, 3) legal problems, and 4) total income.
Participants daily alcohol use was assessed for the 30 days prior to entering residential treatment, 30 days following discharge from residential treatment (called the 1-month assessment), and 30 days prior the 4-month, and 12-month assessments, with participants classified as ‘abstinent’, ‘reduced’, or ‘non-reduced’ in terms of their alcohol consumption over each follow-up period, based on the change in their alcohol use from pre-treatment baseline.
Individuals with current suicidality or a lifetime diagnosis of bipolar disorder or schizophrenia were excluded from the study.
The researchers tested for between-group differences (abstinent vs. reduced vs. non-reduced) on their psychological and functional measures at 4- and 12-month follow-up, controlling for age, sex, baseline alcohol dependence severity, and alcohol consumed over the 30-day baseline assessment period.
Of the initial 327 participants who completed baseline assessment, 241 (73.7%) completed the 4-month follow-up assessment, and 222 (67.9%) completed the 12-month assessment. To check how this high attrition rate may have influenced study outcomes, the researchers used a statistical imputation method to assess how replacing missing data caused by study drop-out may have influenced results. They found no major difference in findings whether they used this imputation approach or not, so presented results with only the 241 study participants who completed at least the 4-month assessment.
The study sample was on average 59 years old and 40% female. The majority of participants identified as White (73%), with 10% of the sample identifying as Black, 7% as American Indian/Alaska Native, 1% as Hispanic, 1% as Asian/Pacific Islander, and 1% as Other, with the remainder not indicating their racial identity.
WHAT DID THIS STUDY FIND?
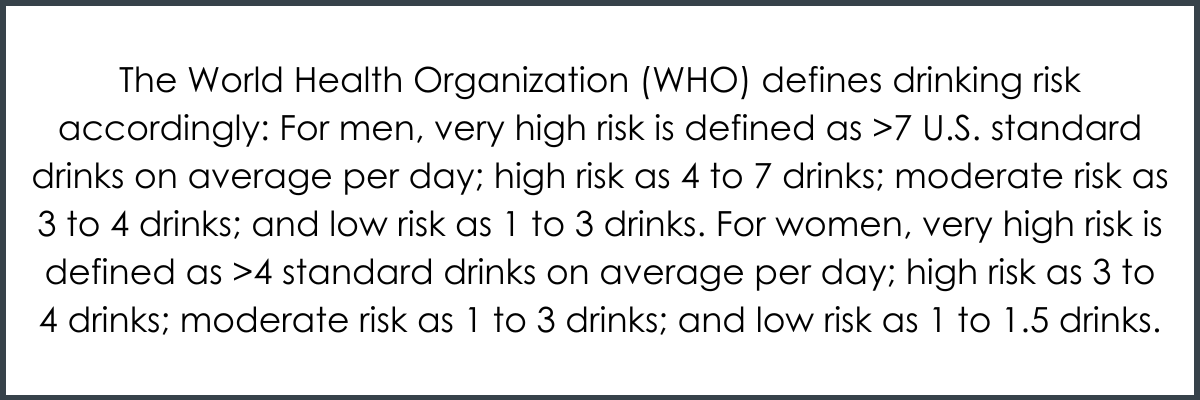
At pre-treatment baseline, on average, about three-quarters (73.7%) of participants were drinking in amounts deemed to be high risk by World Health Organization (WHO) standards, with most having either moderate (62; 24.2%) or severe alcohol dependence (187; 73.1%) according to Diagnostic and Statistical Manual of Mental Disorder IV (commonly referred to as DSM-IV) diagnostic criteria.
Most participants were abstinent early on, though drinking increased for some over the 12-month follow-up period.
Of the 239 individuals who completed their 1-month follow-up assessment interview, 199 (83.3%) reported total alcohol abstinence for the past 30 days, 27 (11.3%) reported reductions in drinking from baseline, and 13 (5.4%) had not reduced their drinking.
Although the majority of participants were totally abstinent at 1-month assessment, many of these participants subsequently resumed drinking, with the rate of abstinence dropping from 83.3% at 1-month assessment, to 62.7% at 4-months. At 4-month assessment, 44 previous abstainers had moved to the reduced drinking group and 18 had returned to their baseline level of alcohol use. This meant that at 4-month follow-up, the number of participants who were non-abstinent but had reduced their drinking from baseline had increased to 60 (i.e., 24.9% of those who completed 4-month follow-up). Further, by 12-month follow-up, this number was 59 (i.e., 26.6% of those who completed 12-month follow-up).
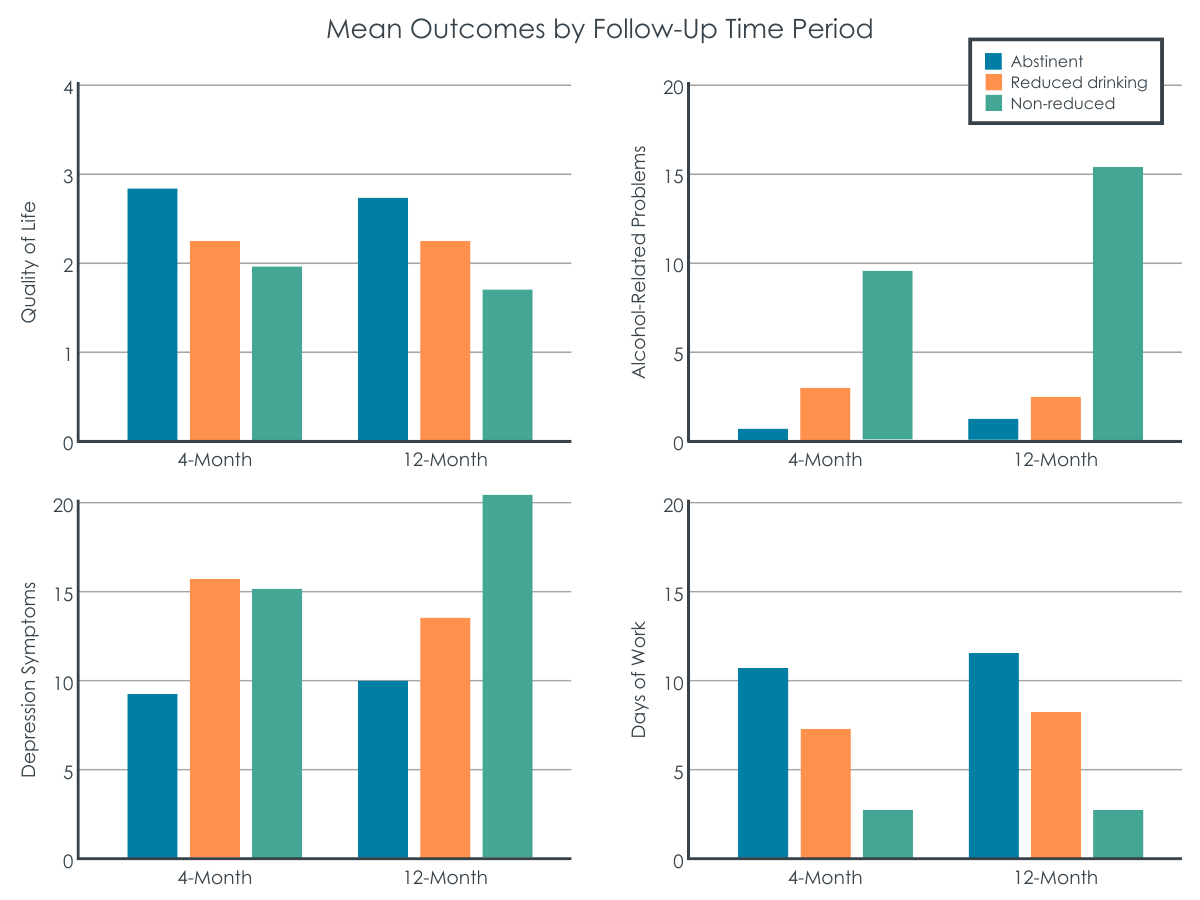
Abstinence was associated with generally better psychological and functional outcomes.
Quality of life
At both 4- and 12-month assessment, the abstinent group, in comparison to the reduced and non-reduced drinking groups, had greater quality of life.
Depressive symptoms
At 4-month assessment the abstinent group endorsed fewer depressive symptoms than the reduced drinking group. Additionally, at 12-month assessment, the abstinent group had fewer depressive symptoms than the non-reduced group.
Alcohol dependence severity, and alcohol-related problems
At 4-month assessment, the abstinent group, in comparison to the reduced and non-reduced drinking groups, had fewer alcohol-related problems, however, these groups were not notably different in terms of alcohol dependence severity. At 12-month assessment, the non-reduced group had higher alcohol dependence severity and alcohol-related problems compared to both the abstinent and reduced drinking groups. The abstinent and reduced drinking groups, however, were not markedly different on these measures at the 12-month assessment.
Anxiety symptoms
At both 4- and 12-month assessments, groups did not differ in terms of their anxiety symptoms.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
There are several individual, clinical, and societal benefits associated with recognizing and supporting non-abstinent substance use disorder recovery pathways. Ultimately, providing treatment options for individuals seeking forms of moderate substance use versus total alcohol and other drug abstinence will lead to engagement of more people in treatment, and better treatment retention.
At the same time, continued substance use, even at less harmful levels is not without risks. Any continued substance use confers some additional medical risk in both the short-term (e.g., greater risk of overdose or accidents), and long-term (e.g., risk of chronic medical conditions like cancer and cirrhosis). Additionally, there is an “opportunity cost” related to the time and effort allocated to continued substance use and its moderation, which might be better spent seeking out and engaging in other meaningful activities that could increase positive emotions, self-confidence, and well-being, without medical risk (e.g., pursuing goals, engaging in hobbies, growing a social support network of pro-recovery peers).
The question remains, however, whether individuals who have achieved substance use disorder remission through abstinence (i.e., they no longer meet diagnostic criteria for substance use disorder) fare better in terms of psychological well-being and functioning than those who achieve remission by reducing their use of one or more substances.
Some recent studies (for example), including this one, suggest individuals may be better off abstinent. This fits with the theory that people who pursue abstinence-based recovery are less encumbered and have more time and cognitive and behavioral resources to devote to building a life worth living inconsistent with high-risk substance use. Abstainers may also reap health benefits associated with not drinking alcohol.
That said, given the advantages of reduced versus non-reduced drinking, there will likely be a net benefit of engaging as many people in treatment as possible by supporting non-abstinent recovery pathways. Even if, on average, individuals don’t experience the same gains in psychological well-being and functioning, not engaging these individuals in treatment at all is worse.
This study experienced significant participant attrition. While this is typically more problematic in studies where the main outcome of interest is substance use lapses or substance use disorder relapse (here the primary outcome of interest was association between drinking over follow-up and measures of psychological well-being and functioning), it nevertheless undermines confidence in the findings. It is likely that many participants lost to follow-up had resumed alcohol use at potentially harmful/hazardous levels, meaning continued drinking rates in the sample were perhaps higher than reported and those who were drinking and doing somewhat better may have been overrepresented, thereby making drinkers appear more similar to abstainers than they actually were.
Notably, groups were not different at 4- or 12-month follow-up in terms of anxiety symptoms. Although baseline anxiety scores were not reported, trait anxiety was fairly high across groups at 4- and 12-month assessment (scores around 40 on the State-Trait Anxiety Inventory indicative of moderate-severe anxiety). This may have been a function of the sample consisting of individuals with co-occurring anxiety disorders, whose anxiety may have been less likely to change in response to drinking versus not drinking.
As noted above, participant attrition over the follow-up period was high in this study. Although checks by the researchers indicated that participants retained in the study, versus those that were lost to follow-up were not notably different in terms of their demographic characteristics and baseline addiction severity, it can’t be truly known how inclusion of these missing data would have affected results. For instance, it is quite possible that on average, those lost to follow-up had resumed problematic drinking but were systematically excluded from the results because they did not complete follow-ups.
The researchers did not assess participants’ alcohol use goal. It is likely that a portion of participants in the reduced-drinking group were drinking by choice rather than as a result of not achieving an abstinence goa (i.e., their drinking goal was moderation, not abstinence). For these individuals, reduced drinking would have been experienced as a success rather than a failure, and may have influenced psychological outcomes in unknown ways.
All study participants were recruited from the same residential treatment program that had an abstinence-based recovery model. As such, participants with moderation-based recovery goals would not have experienced the same level of recovery support. It’s possible individuals in the reduced-drinking group who entered treatment with a goal of moderation versus abstinence, would have had better psychological and functional outcomes had they have received targeted support around reducing rather than stopping alcohol use.
The researchers assessed drinking in 30-day windows abutting each assessment time-point. Though this is an acceptable and commonly used approach for assessing alcohol use in longitudinal research like this, drinking episodes can be missed, which could influence results in unknown ways.
BOTTOM LINE
Increasingly the addiction treatment field is recognizing the benefits associated with non-abstinent substance use disorder remission pathways. At this same time, this study, and others like it suggest individuals pursuing abstinence-based recovery may experience more psychological and functional gains.
For individuals and families seeking recovery: Though for most, the safest and most stable path to substance use disorder recovery is total abstinence from alcohol and other drugs, there are some who can achieve substance use disorder remission through reduced substance use. At the same time, this study, and others like it, suggest that on average, individuals pursuing abstinence-based recovery have better psychological and functional outcomes.
For treatment professionals and treatment systems: Though for most, the safest and most stable path to substance use disorder recovery is total abstinence from alcohol and other drugs, there are some who can achieve substance use disorder remission through reduced use of one or more substances. At the same time, this study, and others like it, suggest that on average, individuals pursuing abstinence-based recovery have better psychological and functional outcomes. Although individuals in abstinence-based recovery may have better psychological and functional outcomes, creating more inclusive treatment options for individuals seeking non-abstinence-based recovery will invariably create a net benefit by engaging many individuals in substance use disorder treatment who otherwise may never seek care.
For scientists:Much debate still surrounds moderation-based recovery pathways. More work is needed to determine for whom, and under what conditions moderation-based recovery might be a viable option. Importantly more work is also needed to extend the findings of this and previous studies exploring the psychological and functional sequelae of addiction recovery in these populations.
For policy makers: There is no one path to addiction recovery. Though this study, and others like it suggest individuals may fare better in abstinence-based recovery, much individual and societal benefit will be had by engaging the maximum number of people in substance use disorder treatment by meeting patients “where they’re at” and supporting programs that provide care supporting moderation recovery goals. Encouraging and incentivizing treatment programs to both recommend abstinence but also engage and support patients with non-abstinence goals will have a net benefit on public health.
Historically, the vast majority of substance use disorder treatment programs in the United States have adhered to an abstinence-based model of recovery. In other words, they espoused recovery through complete abstinence from alcohol and other drugs regardless of patients’ primary substance/s. The rationale behind this approach is that relapse can be so devastating and sometimes fatal, especially for the more severe cases that use residential treatment, that any use of any psychoactive substance—even one that a patient has not used or used very much previously—might impair cognitive functioning including appraisal and judgement, thus increasing the risk for a bad decision that could in turn increase risk for relapse to their primary substance, or even result in an addiction to the new drug. In recent years however, some studies have begun to show that a subset of individuals can achieve remission from substance use disorder by reducing their use of one or more substances, rather than completely abstaining, especially those patients with less severe forms of alcohol or other drug use disorder.
While a growing body of research indicates many can and do achieve remission in this way, questions remain about who can reasonably expect to recover through a non-abstinent pathway, and how continued substance use (versus total abstinence) potentially helps or hinders gains in psychological well-being and general functioning in the recovery process. Such research will be important for informing clinical and public health recommendations.
Using cross-sectional data from the National Recovery Study conducted by the Recovery Research Institute, researchers previously found that lower-risk substance use status (i.e., abstinence or continued use of only a secondary substance, versus use of a primary substance or a primary and secondary substance) across all recovery stages was associated with greater self-esteem, happiness, quality of life and functioning, as well as less psychological distress. In other words, the closer a participant was to the abstinent end of the substance use spectrum, the better off they were in terms of quality of life and well-being.
That study focused on a broad sample of people in the US population self-identifying as having resolved a prior problem with alcohol or other drugs. This study extended this research by asking the same questions but with a sample of individuals with diagnosed alcohol use disorder, and co-occurring anxiety disorders, who may, on average, have had more severe addiction severity than the National Recovery Study sample.
HOW WAS THIS STUDY CONDUCTED?
This was an observational study that included 327 individuals with alcohol use disorder and co-occurring anxiety disorders who were assessed for alcohol use as well as psychological well-being and general functioning at treatment baseline, and then at 1, 4, and 12 months following residential treatment.
Participants were assessed at the start of residential treatment (i.e., baseline), and again at 1, 4, and 12 months on a range of measures gauging psychological well-being and functioning. These included, 1) addiction severity measured with the Addiction Severity Index, 2) quality of life measured by the Quality of Life Enjoyment and Satisfaction Questionnaire, 3) depressive symptoms measured by the Beck Depression Inventory, and 4) trait anxiety measured using the State-Trait Anxiety Inventory. Functional measures included, 1) number of days working, 2) number of days with interpersonal conflicts, 3) legal problems, and 4) total income.
Participants daily alcohol use was assessed for the 30 days prior to entering residential treatment, 30 days following discharge from residential treatment (called the 1-month assessment), and 30 days prior the 4-month, and 12-month assessments, with participants classified as ‘abstinent’, ‘reduced’, or ‘non-reduced’ in terms of their alcohol consumption over each follow-up period, based on the change in their alcohol use from pre-treatment baseline.
Individuals with current suicidality or a lifetime diagnosis of bipolar disorder or schizophrenia were excluded from the study.
The researchers tested for between-group differences (abstinent vs. reduced vs. non-reduced) on their psychological and functional measures at 4- and 12-month follow-up, controlling for age, sex, baseline alcohol dependence severity, and alcohol consumed over the 30-day baseline assessment period.
Of the initial 327 participants who completed baseline assessment, 241 (73.7%) completed the 4-month follow-up assessment, and 222 (67.9%) completed the 12-month assessment. To check how this high attrition rate may have influenced study outcomes, the researchers used a statistical imputation method to assess how replacing missing data caused by study drop-out may have influenced results. They found no major difference in findings whether they used this imputation approach or not, so presented results with only the 241 study participants who completed at least the 4-month assessment.
The study sample was on average 59 years old and 40% female. The majority of participants identified as White (73%), with 10% of the sample identifying as Black, 7% as American Indian/Alaska Native, 1% as Hispanic, 1% as Asian/Pacific Islander, and 1% as Other, with the remainder not indicating their racial identity.
WHAT DID THIS STUDY FIND?
At pre-treatment baseline, on average, about three-quarters (73.7%) of participants were drinking in amounts deemed to be high risk by World Health Organization (WHO) standards, with most having either moderate (62; 24.2%) or severe alcohol dependence (187; 73.1%) according to Diagnostic and Statistical Manual of Mental Disorder IV (commonly referred to as DSM-IV) diagnostic criteria.
Most participants were abstinent early on, though drinking increased for some over the 12-month follow-up period.
Of the 239 individuals who completed their 1-month follow-up assessment interview, 199 (83.3%) reported total alcohol abstinence for the past 30 days, 27 (11.3%) reported reductions in drinking from baseline, and 13 (5.4%) had not reduced their drinking.
Although the majority of participants were totally abstinent at 1-month assessment, many of these participants subsequently resumed drinking, with the rate of abstinence dropping from 83.3% at 1-month assessment, to 62.7% at 4-months. At 4-month assessment, 44 previous abstainers had moved to the reduced drinking group and 18 had returned to their baseline level of alcohol use. This meant that at 4-month follow-up, the number of participants who were non-abstinent but had reduced their drinking from baseline had increased to 60 (i.e., 24.9% of those who completed 4-month follow-up). Further, by 12-month follow-up, this number was 59 (i.e., 26.6% of those who completed 12-month follow-up).
Abstinence was associated with generally better psychological and functional outcomes.
Quality of life
At both 4- and 12-month assessment, the abstinent group, in comparison to the reduced and non-reduced drinking groups, had greater quality of life.
Depressive symptoms
At 4-month assessment the abstinent group endorsed fewer depressive symptoms than the reduced drinking group. Additionally, at 12-month assessment, the abstinent group had fewer depressive symptoms than the non-reduced group.
Alcohol dependence severity, and alcohol-related problems
At 4-month assessment, the abstinent group, in comparison to the reduced and non-reduced drinking groups, had fewer alcohol-related problems, however, these groups were not notably different in terms of alcohol dependence severity. At 12-month assessment, the non-reduced group had higher alcohol dependence severity and alcohol-related problems compared to both the abstinent and reduced drinking groups. The abstinent and reduced drinking groups, however, were not markedly different on these measures at the 12-month assessment.
Anxiety symptoms
At both 4- and 12-month assessments, groups did not differ in terms of their anxiety symptoms.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
There are several individual, clinical, and societal benefits associated with recognizing and supporting non-abstinent substance use disorder recovery pathways. Ultimately, providing treatment options for individuals seeking forms of moderate substance use versus total alcohol and other drug abstinence will lead to engagement of more people in treatment, and better treatment retention.
At the same time, continued substance use, even at less harmful levels is not without risks. Any continued substance use confers some additional medical risk in both the short-term (e.g., greater risk of overdose or accidents), and long-term (e.g., risk of chronic medical conditions like cancer and cirrhosis). Additionally, there is an “opportunity cost” related to the time and effort allocated to continued substance use and its moderation, which might be better spent seeking out and engaging in other meaningful activities that could increase positive emotions, self-confidence, and well-being, without medical risk (e.g., pursuing goals, engaging in hobbies, growing a social support network of pro-recovery peers).
The question remains, however, whether individuals who have achieved substance use disorder remission through abstinence (i.e., they no longer meet diagnostic criteria for substance use disorder) fare better in terms of psychological well-being and functioning than those who achieve remission by reducing their use of one or more substances.
Some recent studies (for example), including this one, suggest individuals may be better off abstinent. This fits with the theory that people who pursue abstinence-based recovery are less encumbered and have more time and cognitive and behavioral resources to devote to building a life worth living inconsistent with high-risk substance use. Abstainers may also reap health benefits associated with not drinking alcohol.
That said, given the advantages of reduced versus non-reduced drinking, there will likely be a net benefit of engaging as many people in treatment as possible by supporting non-abstinent recovery pathways. Even if, on average, individuals don’t experience the same gains in psychological well-being and functioning, not engaging these individuals in treatment at all is worse.
This study experienced significant participant attrition. While this is typically more problematic in studies where the main outcome of interest is substance use lapses or substance use disorder relapse (here the primary outcome of interest was association between drinking over follow-up and measures of psychological well-being and functioning), it nevertheless undermines confidence in the findings. It is likely that many participants lost to follow-up had resumed alcohol use at potentially harmful/hazardous levels, meaning continued drinking rates in the sample were perhaps higher than reported and those who were drinking and doing somewhat better may have been overrepresented, thereby making drinkers appear more similar to abstainers than they actually were.
Notably, groups were not different at 4- or 12-month follow-up in terms of anxiety symptoms. Although baseline anxiety scores were not reported, trait anxiety was fairly high across groups at 4- and 12-month assessment (scores around 40 on the State-Trait Anxiety Inventory indicative of moderate-severe anxiety). This may have been a function of the sample consisting of individuals with co-occurring anxiety disorders, whose anxiety may have been less likely to change in response to drinking versus not drinking.
As noted above, participant attrition over the follow-up period was high in this study. Although checks by the researchers indicated that participants retained in the study, versus those that were lost to follow-up were not notably different in terms of their demographic characteristics and baseline addiction severity, it can’t be truly known how inclusion of these missing data would have affected results. For instance, it is quite possible that on average, those lost to follow-up had resumed problematic drinking but were systematically excluded from the results because they did not complete follow-ups.
The researchers did not assess participants’ alcohol use goal. It is likely that a portion of participants in the reduced-drinking group were drinking by choice rather than as a result of not achieving an abstinence goa (i.e., their drinking goal was moderation, not abstinence). For these individuals, reduced drinking would have been experienced as a success rather than a failure, and may have influenced psychological outcomes in unknown ways.
All study participants were recruited from the same residential treatment program that had an abstinence-based recovery model. As such, participants with moderation-based recovery goals would not have experienced the same level of recovery support. It’s possible individuals in the reduced-drinking group who entered treatment with a goal of moderation versus abstinence, would have had better psychological and functional outcomes had they have received targeted support around reducing rather than stopping alcohol use.
The researchers assessed drinking in 30-day windows abutting each assessment time-point. Though this is an acceptable and commonly used approach for assessing alcohol use in longitudinal research like this, drinking episodes can be missed, which could influence results in unknown ways.
BOTTOM LINE
Increasingly the addiction treatment field is recognizing the benefits associated with non-abstinent substance use disorder remission pathways. At this same time, this study, and others like it suggest individuals pursuing abstinence-based recovery may experience more psychological and functional gains.
For individuals and families seeking recovery: Though for most, the safest and most stable path to substance use disorder recovery is total abstinence from alcohol and other drugs, there are some who can achieve substance use disorder remission through reduced substance use. At the same time, this study, and others like it, suggest that on average, individuals pursuing abstinence-based recovery have better psychological and functional outcomes.
For treatment professionals and treatment systems: Though for most, the safest and most stable path to substance use disorder recovery is total abstinence from alcohol and other drugs, there are some who can achieve substance use disorder remission through reduced use of one or more substances. At the same time, this study, and others like it, suggest that on average, individuals pursuing abstinence-based recovery have better psychological and functional outcomes. Although individuals in abstinence-based recovery may have better psychological and functional outcomes, creating more inclusive treatment options for individuals seeking non-abstinence-based recovery will invariably create a net benefit by engaging many individuals in substance use disorder treatment who otherwise may never seek care.
For scientists:Much debate still surrounds moderation-based recovery pathways. More work is needed to determine for whom, and under what conditions moderation-based recovery might be a viable option. Importantly more work is also needed to extend the findings of this and previous studies exploring the psychological and functional sequelae of addiction recovery in these populations.
For policy makers: There is no one path to addiction recovery. Though this study, and others like it suggest individuals may fare better in abstinence-based recovery, much individual and societal benefit will be had by engaging the maximum number of people in substance use disorder treatment by meeting patients “where they’re at” and supporting programs that provide care supporting moderation recovery goals. Encouraging and incentivizing treatment programs to both recommend abstinence but also engage and support patients with non-abstinence goals will have a net benefit on public health.
Historically, the vast majority of substance use disorder treatment programs in the United States have adhered to an abstinence-based model of recovery. In other words, they espoused recovery through complete abstinence from alcohol and other drugs regardless of patients’ primary substance/s. The rationale behind this approach is that relapse can be so devastating and sometimes fatal, especially for the more severe cases that use residential treatment, that any use of any psychoactive substance—even one that a patient has not used or used very much previously—might impair cognitive functioning including appraisal and judgement, thus increasing the risk for a bad decision that could in turn increase risk for relapse to their primary substance, or even result in an addiction to the new drug. In recent years however, some studies have begun to show that a subset of individuals can achieve remission from substance use disorder by reducing their use of one or more substances, rather than completely abstaining, especially those patients with less severe forms of alcohol or other drug use disorder.
While a growing body of research indicates many can and do achieve remission in this way, questions remain about who can reasonably expect to recover through a non-abstinent pathway, and how continued substance use (versus total abstinence) potentially helps or hinders gains in psychological well-being and general functioning in the recovery process. Such research will be important for informing clinical and public health recommendations.
Using cross-sectional data from the National Recovery Study conducted by the Recovery Research Institute, researchers previously found that lower-risk substance use status (i.e., abstinence or continued use of only a secondary substance, versus use of a primary substance or a primary and secondary substance) across all recovery stages was associated with greater self-esteem, happiness, quality of life and functioning, as well as less psychological distress. In other words, the closer a participant was to the abstinent end of the substance use spectrum, the better off they were in terms of quality of life and well-being.
That study focused on a broad sample of people in the US population self-identifying as having resolved a prior problem with alcohol or other drugs. This study extended this research by asking the same questions but with a sample of individuals with diagnosed alcohol use disorder, and co-occurring anxiety disorders, who may, on average, have had more severe addiction severity than the National Recovery Study sample.
HOW WAS THIS STUDY CONDUCTED?
This was an observational study that included 327 individuals with alcohol use disorder and co-occurring anxiety disorders who were assessed for alcohol use as well as psychological well-being and general functioning at treatment baseline, and then at 1, 4, and 12 months following residential treatment.
Participants were assessed at the start of residential treatment (i.e., baseline), and again at 1, 4, and 12 months on a range of measures gauging psychological well-being and functioning. These included, 1) addiction severity measured with the Addiction Severity Index, 2) quality of life measured by the Quality of Life Enjoyment and Satisfaction Questionnaire, 3) depressive symptoms measured by the Beck Depression Inventory, and 4) trait anxiety measured using the State-Trait Anxiety Inventory. Functional measures included, 1) number of days working, 2) number of days with interpersonal conflicts, 3) legal problems, and 4) total income.
Participants daily alcohol use was assessed for the 30 days prior to entering residential treatment, 30 days following discharge from residential treatment (called the 1-month assessment), and 30 days prior the 4-month, and 12-month assessments, with participants classified as ‘abstinent’, ‘reduced’, or ‘non-reduced’ in terms of their alcohol consumption over each follow-up period, based on the change in their alcohol use from pre-treatment baseline.
Individuals with current suicidality or a lifetime diagnosis of bipolar disorder or schizophrenia were excluded from the study.
The researchers tested for between-group differences (abstinent vs. reduced vs. non-reduced) on their psychological and functional measures at 4- and 12-month follow-up, controlling for age, sex, baseline alcohol dependence severity, and alcohol consumed over the 30-day baseline assessment period.
Of the initial 327 participants who completed baseline assessment, 241 (73.7%) completed the 4-month follow-up assessment, and 222 (67.9%) completed the 12-month assessment. To check how this high attrition rate may have influenced study outcomes, the researchers used a statistical imputation method to assess how replacing missing data caused by study drop-out may have influenced results. They found no major difference in findings whether they used this imputation approach or not, so presented results with only the 241 study participants who completed at least the 4-month assessment.
The study sample was on average 59 years old and 40% female. The majority of participants identified as White (73%), with 10% of the sample identifying as Black, 7% as American Indian/Alaska Native, 1% as Hispanic, 1% as Asian/Pacific Islander, and 1% as Other, with the remainder not indicating their racial identity.
WHAT DID THIS STUDY FIND?
At pre-treatment baseline, on average, about three-quarters (73.7%) of participants were drinking in amounts deemed to be high risk by World Health Organization (WHO) standards, with most having either moderate (62; 24.2%) or severe alcohol dependence (187; 73.1%) according to Diagnostic and Statistical Manual of Mental Disorder IV (commonly referred to as DSM-IV) diagnostic criteria.
Most participants were abstinent early on, though drinking increased for some over the 12-month follow-up period.
Of the 239 individuals who completed their 1-month follow-up assessment interview, 199 (83.3%) reported total alcohol abstinence for the past 30 days, 27 (11.3%) reported reductions in drinking from baseline, and 13 (5.4%) had not reduced their drinking.
Although the majority of participants were totally abstinent at 1-month assessment, many of these participants subsequently resumed drinking, with the rate of abstinence dropping from 83.3% at 1-month assessment, to 62.7% at 4-months. At 4-month assessment, 44 previous abstainers had moved to the reduced drinking group and 18 had returned to their baseline level of alcohol use. This meant that at 4-month follow-up, the number of participants who were non-abstinent but had reduced their drinking from baseline had increased to 60 (i.e., 24.9% of those who completed 4-month follow-up). Further, by 12-month follow-up, this number was 59 (i.e., 26.6% of those who completed 12-month follow-up).
Abstinence was associated with generally better psychological and functional outcomes.
Quality of life
At both 4- and 12-month assessment, the abstinent group, in comparison to the reduced and non-reduced drinking groups, had greater quality of life.
Depressive symptoms
At 4-month assessment the abstinent group endorsed fewer depressive symptoms than the reduced drinking group. Additionally, at 12-month assessment, the abstinent group had fewer depressive symptoms than the non-reduced group.
Alcohol dependence severity, and alcohol-related problems
At 4-month assessment, the abstinent group, in comparison to the reduced and non-reduced drinking groups, had fewer alcohol-related problems, however, these groups were not notably different in terms of alcohol dependence severity. At 12-month assessment, the non-reduced group had higher alcohol dependence severity and alcohol-related problems compared to both the abstinent and reduced drinking groups. The abstinent and reduced drinking groups, however, were not markedly different on these measures at the 12-month assessment.
Anxiety symptoms
At both 4- and 12-month assessments, groups did not differ in terms of their anxiety symptoms.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
There are several individual, clinical, and societal benefits associated with recognizing and supporting non-abstinent substance use disorder recovery pathways. Ultimately, providing treatment options for individuals seeking forms of moderate substance use versus total alcohol and other drug abstinence will lead to engagement of more people in treatment, and better treatment retention.
At the same time, continued substance use, even at less harmful levels is not without risks. Any continued substance use confers some additional medical risk in both the short-term (e.g., greater risk of overdose or accidents), and long-term (e.g., risk of chronic medical conditions like cancer and cirrhosis). Additionally, there is an “opportunity cost” related to the time and effort allocated to continued substance use and its moderation, which might be better spent seeking out and engaging in other meaningful activities that could increase positive emotions, self-confidence, and well-being, without medical risk (e.g., pursuing goals, engaging in hobbies, growing a social support network of pro-recovery peers).
The question remains, however, whether individuals who have achieved substance use disorder remission through abstinence (i.e., they no longer meet diagnostic criteria for substance use disorder) fare better in terms of psychological well-being and functioning than those who achieve remission by reducing their use of one or more substances.
Some recent studies (for example), including this one, suggest individuals may be better off abstinent. This fits with the theory that people who pursue abstinence-based recovery are less encumbered and have more time and cognitive and behavioral resources to devote to building a life worth living inconsistent with high-risk substance use. Abstainers may also reap health benefits associated with not drinking alcohol.
That said, given the advantages of reduced versus non-reduced drinking, there will likely be a net benefit of engaging as many people in treatment as possible by supporting non-abstinent recovery pathways. Even if, on average, individuals don’t experience the same gains in psychological well-being and functioning, not engaging these individuals in treatment at all is worse.
This study experienced significant participant attrition. While this is typically more problematic in studies where the main outcome of interest is substance use lapses or substance use disorder relapse (here the primary outcome of interest was association between drinking over follow-up and measures of psychological well-being and functioning), it nevertheless undermines confidence in the findings. It is likely that many participants lost to follow-up had resumed alcohol use at potentially harmful/hazardous levels, meaning continued drinking rates in the sample were perhaps higher than reported and those who were drinking and doing somewhat better may have been overrepresented, thereby making drinkers appear more similar to abstainers than they actually were.
Notably, groups were not different at 4- or 12-month follow-up in terms of anxiety symptoms. Although baseline anxiety scores were not reported, trait anxiety was fairly high across groups at 4- and 12-month assessment (scores around 40 on the State-Trait Anxiety Inventory indicative of moderate-severe anxiety). This may have been a function of the sample consisting of individuals with co-occurring anxiety disorders, whose anxiety may have been less likely to change in response to drinking versus not drinking.
As noted above, participant attrition over the follow-up period was high in this study. Although checks by the researchers indicated that participants retained in the study, versus those that were lost to follow-up were not notably different in terms of their demographic characteristics and baseline addiction severity, it can’t be truly known how inclusion of these missing data would have affected results. For instance, it is quite possible that on average, those lost to follow-up had resumed problematic drinking but were systematically excluded from the results because they did not complete follow-ups.
The researchers did not assess participants’ alcohol use goal. It is likely that a portion of participants in the reduced-drinking group were drinking by choice rather than as a result of not achieving an abstinence goa (i.e., their drinking goal was moderation, not abstinence). For these individuals, reduced drinking would have been experienced as a success rather than a failure, and may have influenced psychological outcomes in unknown ways.
All study participants were recruited from the same residential treatment program that had an abstinence-based recovery model. As such, participants with moderation-based recovery goals would not have experienced the same level of recovery support. It’s possible individuals in the reduced-drinking group who entered treatment with a goal of moderation versus abstinence, would have had better psychological and functional outcomes had they have received targeted support around reducing rather than stopping alcohol use.
The researchers assessed drinking in 30-day windows abutting each assessment time-point. Though this is an acceptable and commonly used approach for assessing alcohol use in longitudinal research like this, drinking episodes can be missed, which could influence results in unknown ways.
BOTTOM LINE
Increasingly the addiction treatment field is recognizing the benefits associated with non-abstinent substance use disorder remission pathways. At this same time, this study, and others like it suggest individuals pursuing abstinence-based recovery may experience more psychological and functional gains.
For individuals and families seeking recovery: Though for most, the safest and most stable path to substance use disorder recovery is total abstinence from alcohol and other drugs, there are some who can achieve substance use disorder remission through reduced substance use. At the same time, this study, and others like it, suggest that on average, individuals pursuing abstinence-based recovery have better psychological and functional outcomes.
For treatment professionals and treatment systems: Though for most, the safest and most stable path to substance use disorder recovery is total abstinence from alcohol and other drugs, there are some who can achieve substance use disorder remission through reduced use of one or more substances. At the same time, this study, and others like it, suggest that on average, individuals pursuing abstinence-based recovery have better psychological and functional outcomes. Although individuals in abstinence-based recovery may have better psychological and functional outcomes, creating more inclusive treatment options for individuals seeking non-abstinence-based recovery will invariably create a net benefit by engaging many individuals in substance use disorder treatment who otherwise may never seek care.
For scientists:Much debate still surrounds moderation-based recovery pathways. More work is needed to determine for whom, and under what conditions moderation-based recovery might be a viable option. Importantly more work is also needed to extend the findings of this and previous studies exploring the psychological and functional sequelae of addiction recovery in these populations.
For policy makers: There is no one path to addiction recovery. Though this study, and others like it suggest individuals may fare better in abstinence-based recovery, much individual and societal benefit will be had by engaging the maximum number of people in substance use disorder treatment by meeting patients “where they’re at” and supporting programs that provide care supporting moderation recovery goals. Encouraging and incentivizing treatment programs to both recommend abstinence but also engage and support patients with non-abstinence goals will have a net benefit on public health.