Additional mental health difficulties increase harms for older adults with an alcohol problem
As baby boomers enter older adulthood, the number of older adults with alcohol use disorder is projected to double. Improvements in alcohol assessment and treatment efforts can help to address this risk. This study examined the factors in older adults with alcohol problems that place them at greatest risk for harms including hospitalization and mortality.
Hazardous drinking (e.g., drinking at levels that increase risk for greater health harms such as binge drinking and heavy alcohol use) is common among older adults in the U.S. Older adults may experience specific harms from hazardous drinking, such as falling or other unintentional injuries, memory problems, and severe medication interactions or forgetting to take needed medications in the first place, which may result in hospitalizations or death. Despite such risks, many older adults in the U.S. who meet criteria for alcohol use disorder are not receiving treatment for it.
As “baby boomers” (those born between 1946 and 1964) enter into older adulthood, the number of adults aged 50 or older with alcohol or other drug use disorders was projected to double from 2.8 million in 2006 to 5.7 million by 2020. Alcohol use has steadily increased in the population age 60 and above over the past 20 years, placing even further strain on the U.S. healthcare system in terms of services and costs. It is important to identify opportunities for early assessment and intervention on alcohol-related health complications among older adults to reduce preventable hospitalizations and premature mortality.
This retrospective cohort study from 2003-2017 of Swedish adults aged 50 years an older (n = 1741) examined participants’ onset of drinking problems and other clinical characteristics in relation to later hospitalizations and mortality over time.
Addiction treatment services in Sweden are primarily housed within publicly funded, decentralized social services within municipalities. The researchers used a Swedish national data set that includes records from 65 municipalities of all adults assessed for substance use severity in using the Addiction Severity Index from 2003 to 2017. The Addiction Severity Index is used in 90% of social services in Sweden, and is designed as a semi-structured interview to assess potential problem areas commonly affected by unhealthy substance use: physical health, employment and self-support, alcohol use, drug use, legal problems, family and social relationships, and psychiatric health. It also collects information on familial history of substance use and mental health status.
The researchers combined national Swedish data sets of substance use assessment with matched records of all physical and psychiatric-related hospital discharges, and causes of death. Participants were included in this study if they were at least 50 years of age and reported experiencing at least one alcohol problem on one or more days in the 30 days prior to a baseline assessment.
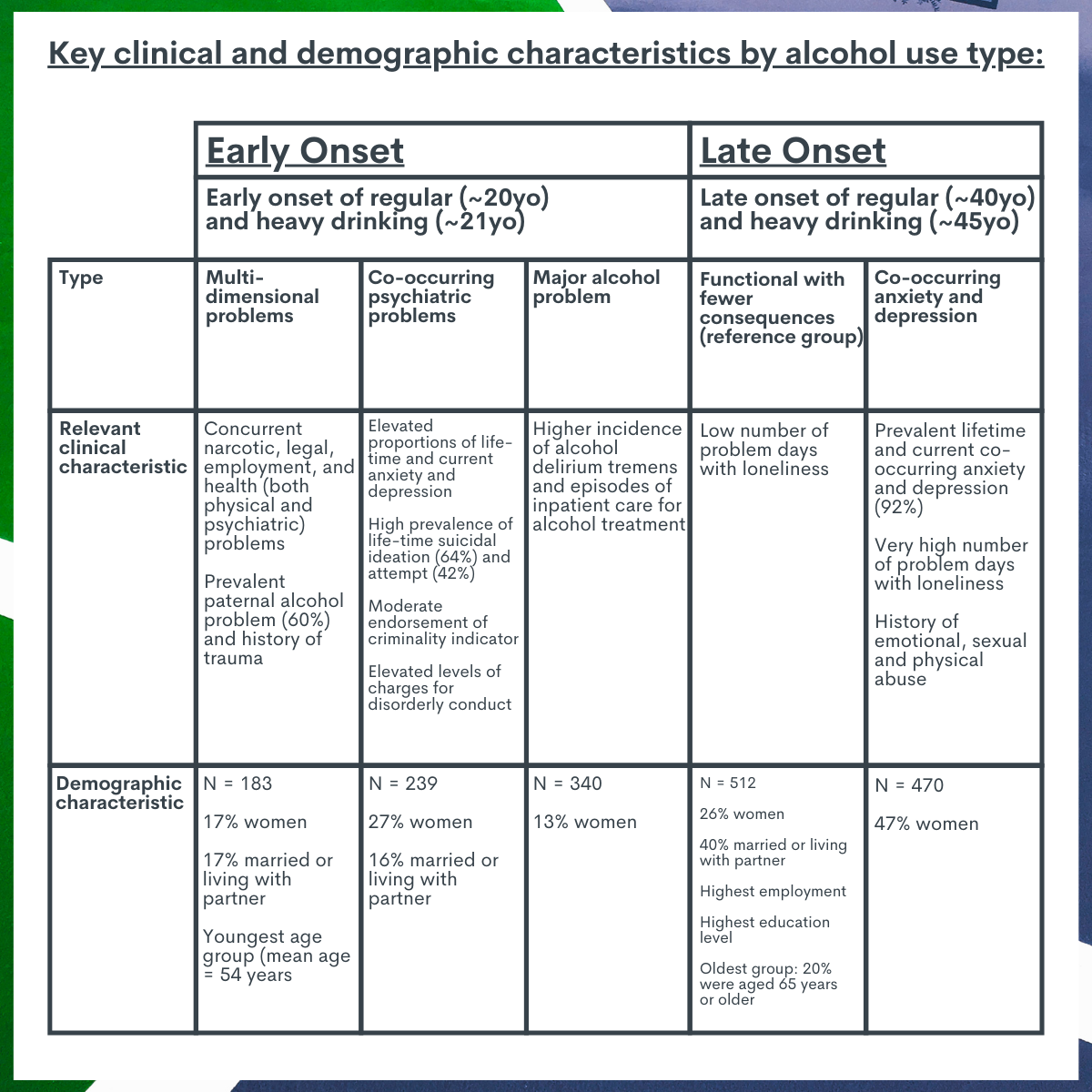
Using information from the interview, participants were categorized into 5 alcohol use types. Identifying specific types of problems is one way to examine clinical characteristics that tend to cluster together and then make predictions about common future health problems. This helps health professionals identify clients who may fit into a particular problem type and intervene on potential problems sooner.
The researchers identified 5 alcohol use types using an analysis that estimates a) the number of groups or types that exist within the data set, and b) the liklihood a participant has a certain clinical characteristic (e.g., history of depression) based on their predicted group or type. Although clinicians and researchers have already developed several systems and theories classifying the biopsychosocial factors that influence the varied clinical presentations of people with alcohol use disorder, called “typologies,” these typologies often have not considered or included older adults. Given the lack of knowledge about alcohol typologies among older adults, the researchers in this study developed their own typologies using a statistical approach with the goal of differentiating heterogeneous subtypes. The 5 types were:
The analysis examined the association between alcohol use type and all causes of hospitalization and death, controlling for relevant demographic and clinical characteristics (included age, sex, migration status, legal problems, marital status, employment, education, residential town population size, housing status, physical comorbidities, and number of hospitalizations in the 1 year prior to baseline assessment). This helps to isolate the effect of alcohol use type on hospitalizations and mortality from other factors that are also highly associated with hospitalizations and death. All analyses compared the effect of different alcohol use types to the Late-onset Fewer Consequences type.
A majority of participants were between ages 50-64 (88%) at baseline assessment, male (72%), and separated or widowed (63.5%). A little less than half of participants were full- or part-time employed (41%), had between 9-12 years education (45%), and lived in a highly populated area (Town population >100,000 people; 46%). Over the 14-year period that was the study’s focus, there were a total of 11,455 hospital admissions and 346 deaths recorded, and approximately 70% of those events were alcohol related. Drug use disorder-related diagnoses (i.e., where the medical record stated the principal diagnosis or contributing causes for hospitalization or death was a substance use disorder other than alcohol) were recorded in 2.5% of cases (288 admissions and 4 deaths). Approximately 8% of hospital admissions during the study period were related to psychiatric diagnoses. More than 75% of participants were hospitalized at least once or died during the study period. Approximately two-thirds (57.3%) were hospitalized once or more related to alcohol disorders, 8.5% due to drug use disorders and 18.5% due to psychiatric-related diagnoses.
WHAT DID THIS STUDY FIND?
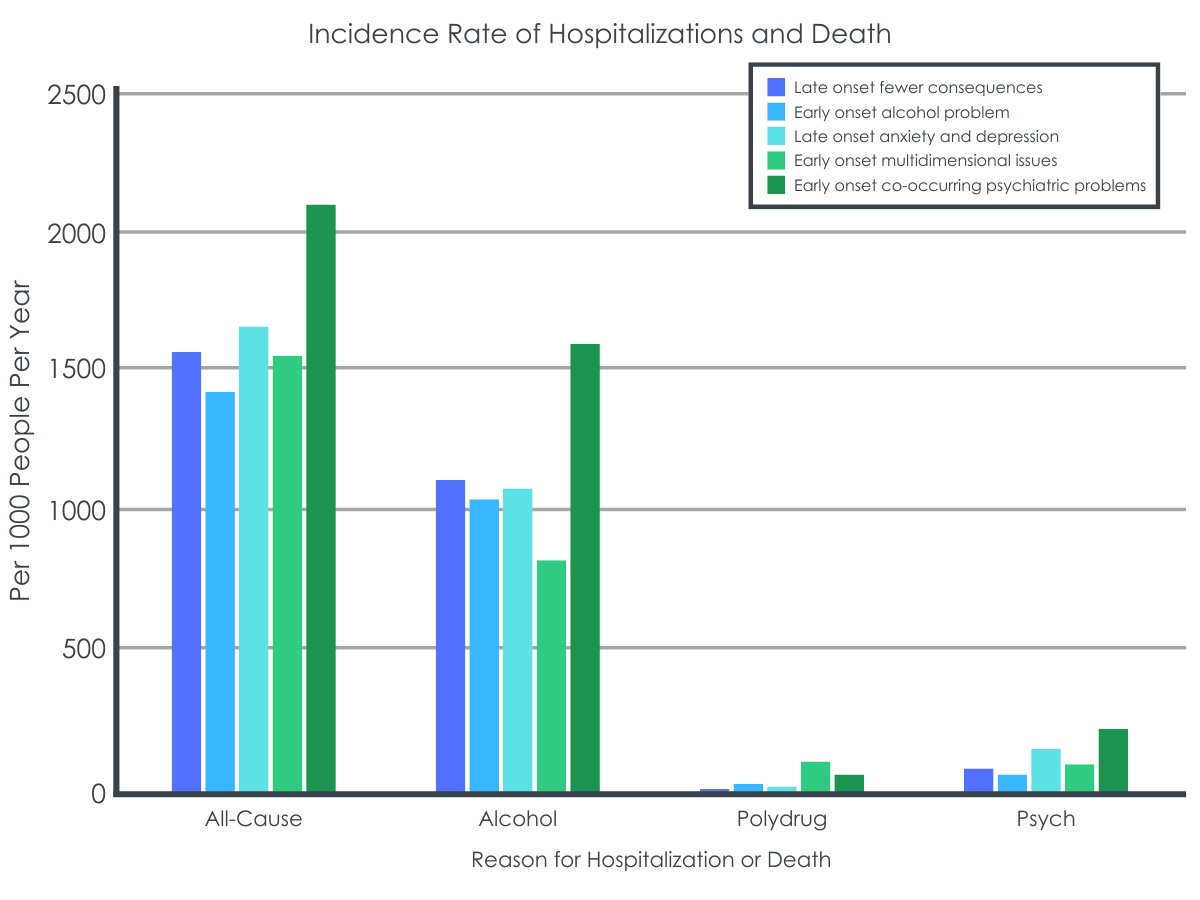
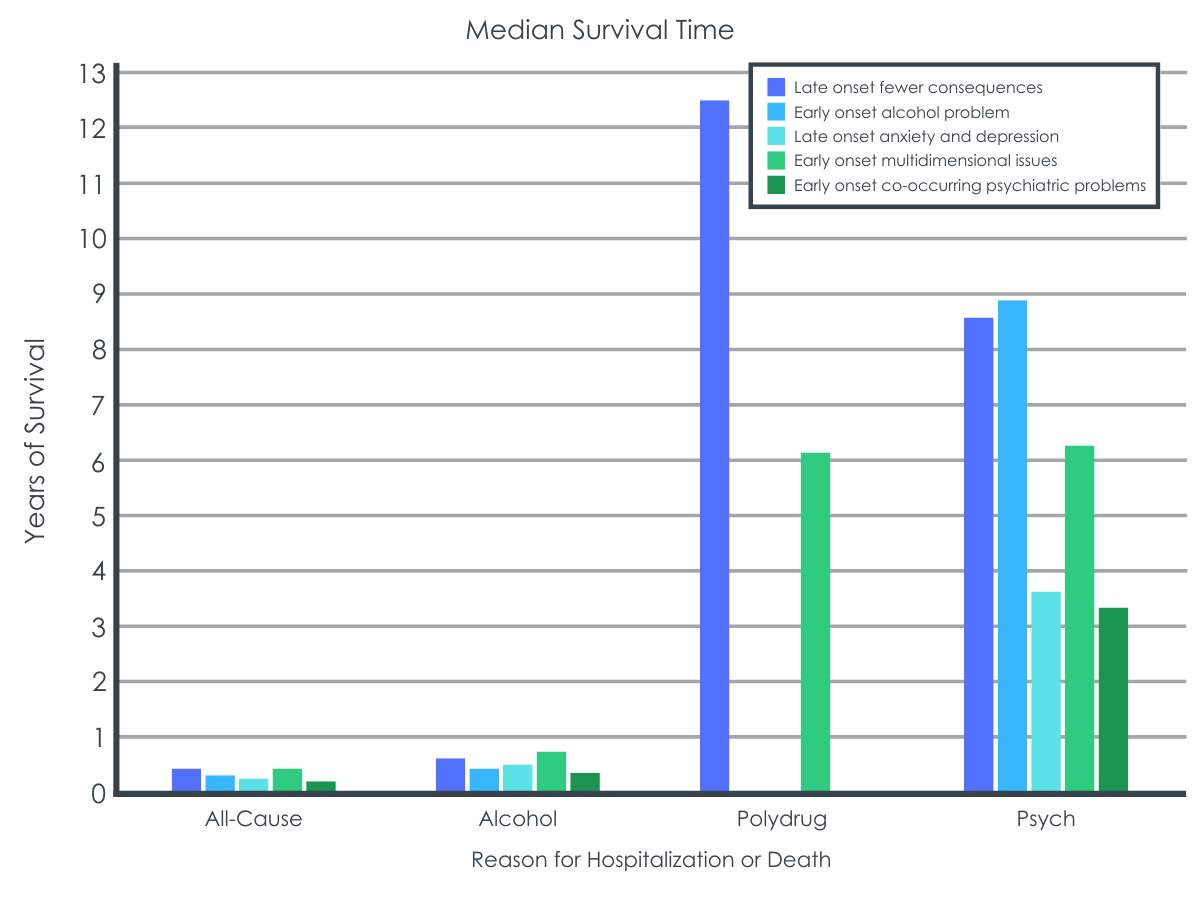
Risks for hospitalization or death were highest among older adults with early onset alcohol use and additional health difficulties compared to older adults with later onset of alcohol use and fewer consequences.
Compared to the Late-onset Fewer Consequences type, Early-onset Co-occurring Psychiatric Problems type had a:
• 27% increased risk of recurrent episode of all-cause hospitalization or death
• 34% increased risk of alcohol-related hospitalization or death
• 162% increased risk of for polydrug use-related hospitalization or death
Compared to the Late-onset Fewer Consequences type, Early-onset Multidimensional Issues type had a:
• 32% reduced risk of alcohol-related hospitalizations or death
• 155% increased risk of poly-drug use disorder-related hospitalizations or death
Compared to the Late-onset Fewer Consequences type, the risk of recurrent psychiatric hospitalization was:
•78% greater in the Late-onset with Co-occurring Anxiety and Depression type
•103% greater in the Early-onset Co-occurring Psychiatric Problems type
Risks were lowest among the Late-onset Fewer Consequences type and the Early-onset Major Alcohol Problems type.
The risk of all-cause hospitalization and death was:
• 27% lower in the Late-onset Fewer Consequences type, compared to the Co-occurring Psychiatric Problems type
There was no difference in the risk of all-cause hospitalization and death between Late-onset Fewer Consequences type and the Early-onset Major Alcohol Problems type.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of older Swedish adults assessed for alcohol use problems from 2003-2017, alcohol and psychiatric-related hospitalizations were high. Three-fourths of participants were hospitalized at least once during the study period – 70% of hospitalizations and 33% of deaths were alcohol related. Additionally, 18.5% of the cohort were hospitalized at least once with psychiatric-related disorders and 8.5% with drug use disorders. More than 10% were hospitalized at least once with dual alcohol use and psychiatric disorders.
Participants with early onset of regular and heavy drinking with co-occurring psychiatric problems were at highest risk for all-cause, alcohol-related, and psychiatric hospitalizations. This could be due to the fact that alcohol use also can exacerbate and perpetuate depression and anxiety symptoms. Additionally, alcohol interferes with medication efficacy for other psychological disorders on a physiological level, and can also interfere with adherence to taking the medications. Another study of older adults with alcohol use disorder found a similar pattern – participants with co-occurring psychiatric conditions reported more drinks per day when entering treatment compared to those without a co-occurring condition. This alcohol use type is similar to both Babor’s Type B and Cloninger’s Type II descriptions of alcohol use disorder, which also mention early onset of alcohol use, more psychopathology, and a family history of alcohol use.
Participants with late onset of regular and heavy drinking with anxiety and depression also had an elevated risk for psychiatric hospitalization. This group also had the highest proportion of women – nearly half the group were women, compared with a quarter or fewer in the other groups. This is expected as women have a higher prevalence of anxiety and depression compared to men. Historically rates of heavy drinking and alcohol problems have been higher in men than women. While they remain so, this gap is narrowing as rates of drinking are increasing among older women.
After an initial contact with the addiction services, most participants in this study had elevated risk for recurrent hospitalization for alcohol-, drug- and psychiatric-related disorders. Moreover, a significant proportion reported elevated prevalence of lifetime and recent history of depression, anxiety, suicidal ideation, loneliness, and trauma at baseline, suggesting a need for earlier and integrated trauma, addiction, and mental health services.
The absence of coordination between old-age care and addiction services might also be a barrier to detecting problematic alcohol use among older people. Given the high risk of recurrent hospitalization in the current study, older adults who are consuming alcohol and who have complex needs might benefit from efforts to improve substance use assessment in primary care settings, with sensitivity to the multi-dimensionality and consequences of problematic substance use among older people. Mental health services integrated within primary care has shown increased identification of mental health concerns within the VA system in the United States. Furthermore, training old-age care providers on late life substance use could provide social services with an additional point of contact for earlier identification of substance use problems and referral to treatment.
The researchers did not have information on the actual treatment provided to participants after their baseline assessment of alcohol problems. The analysis also did not include data from specialty outpatient or residential addiction treatment services. Given that, this analysis does not reflect how participation in treatment, or the nature of any treatment (substance use focused or integrated), may have impacted hospitalizations during the study period.
Although this analysis included drug use-related hospitalizations other than alcohol, participants were selected for inclusion based on problems with alcohol use at baseline, not problems with other substances. Given that, this analysis may not be representative of older adults with substance use problems other than alcohol.
Finally, participants were included based on being evaluated for alcohol use problems when in contact with social services in Sweden. There could be older adults in Sweden who were experiencing alcohol problems and were not assessed, and thus not included in this analysis.
BOTTOM LINE
This study found that, among 1741 older adults in Sweden who used social services and reported one or more alcohol problems, many experienced repeated hospitalizations over the 14-year study period, and risk varied by distinct clinical characteristics. Some older adults with co-occurring psychiatric problems or multidimensional issues had a greater risk for alcohol-, drug-, and psychiatric-related recurrent hospitalizations. The high rate of substance use and psychiatric-related hospitalizations suggests older people may benefit from integrated mental, addiction and physical health care.
For individuals and families seeking recovery: Older adults may experience alcohol problems that could go left unassessed and untreated. This study showed a high rate of hospitalizations due to alcohol and other drug use and psychiatric disorders among older adults with alcohol problems. Older people may benefit from integrated physical, addiction, and mental health care with age-sensitive components. Learn more about how alcohol affects the body as we age here.
For treatment professionals and treatment systems: As the baby boomer generation in the U.S. reaches older adulthood, the number of people needing addiction related services is expected to double. Rates of alcohol use among older adults in Sweden are similarly high to the U.S. In this study conducted in Sweden, given the high rate of hospitalization due to alcohol and other drug use and psychiatric disorders, and the differential risk throughout risk groups, older people may benefit from integrated mental, addiction and physical health care with age-sensitive components. Learn more about screening older adults for alcohol use disorder here.
For scientists:This retrospective cohort study examined Swedish adults aged 50 years an older (n = 1741) who used social services and were assessed for alcohol problems and from 2003-2017. Participants’ onset of drinking and other clinical characteristics were used in a latent class analysis to develop alcohol use types, then each type was examined in relation to hospitalizations and mortality over time. Older adult service users with early onset and co-occurring psychiatric problems were at highest risk for all-cause, alcohol-, drug-, and psychiatric hospitalizations. The current study did not include data on treatment participation. Because recurrent hospitalization was prevalent at follow-up, future studies should investigate the potential moderating effects of outpatient and residential addiction services between the baseline assessment and hospitalization or death.
For policy makers: As the baby boomer generation reaches older adulthood, the number of people needing addiction related services is expected to double. The high rate of hospitalization due to alcohol as well as other drug use and psychiatric disorders in this study raises concerns about the strain on the healthcare system in terms of services and costs. Early assessment and intervention may be one way to reduce costly hospitalizations in the future. Additional research is needed on how integrated care systems and treatments affect hospitalizations long term.
Hazardous drinking (e.g., drinking at levels that increase risk for greater health harms such as binge drinking and heavy alcohol use) is common among older adults in the U.S. Older adults may experience specific harms from hazardous drinking, such as falling or other unintentional injuries, memory problems, and severe medication interactions or forgetting to take needed medications in the first place, which may result in hospitalizations or death. Despite such risks, many older adults in the U.S. who meet criteria for alcohol use disorder are not receiving treatment for it.
As “baby boomers” (those born between 1946 and 1964) enter into older adulthood, the number of adults aged 50 or older with alcohol or other drug use disorders was projected to double from 2.8 million in 2006 to 5.7 million by 2020. Alcohol use has steadily increased in the population age 60 and above over the past 20 years, placing even further strain on the U.S. healthcare system in terms of services and costs. It is important to identify opportunities for early assessment and intervention on alcohol-related health complications among older adults to reduce preventable hospitalizations and premature mortality.
This retrospective cohort study from 2003-2017 of Swedish adults aged 50 years an older (n = 1741) examined participants’ onset of drinking problems and other clinical characteristics in relation to later hospitalizations and mortality over time.
Addiction treatment services in Sweden are primarily housed within publicly funded, decentralized social services within municipalities. The researchers used a Swedish national data set that includes records from 65 municipalities of all adults assessed for substance use severity in using the Addiction Severity Index from 2003 to 2017. The Addiction Severity Index is used in 90% of social services in Sweden, and is designed as a semi-structured interview to assess potential problem areas commonly affected by unhealthy substance use: physical health, employment and self-support, alcohol use, drug use, legal problems, family and social relationships, and psychiatric health. It also collects information on familial history of substance use and mental health status.
The researchers combined national Swedish data sets of substance use assessment with matched records of all physical and psychiatric-related hospital discharges, and causes of death. Participants were included in this study if they were at least 50 years of age and reported experiencing at least one alcohol problem on one or more days in the 30 days prior to a baseline assessment.
Using information from the interview, participants were categorized into 5 alcohol use types. Identifying specific types of problems is one way to examine clinical characteristics that tend to cluster together and then make predictions about common future health problems. This helps health professionals identify clients who may fit into a particular problem type and intervene on potential problems sooner.
The researchers identified 5 alcohol use types using an analysis that estimates a) the number of groups or types that exist within the data set, and b) the liklihood a participant has a certain clinical characteristic (e.g., history of depression) based on their predicted group or type. Although clinicians and researchers have already developed several systems and theories classifying the biopsychosocial factors that influence the varied clinical presentations of people with alcohol use disorder, called “typologies,” these typologies often have not considered or included older adults. Given the lack of knowledge about alcohol typologies among older adults, the researchers in this study developed their own typologies using a statistical approach with the goal of differentiating heterogeneous subtypes. The 5 types were:
The analysis examined the association between alcohol use type and all causes of hospitalization and death, controlling for relevant demographic and clinical characteristics (included age, sex, migration status, legal problems, marital status, employment, education, residential town population size, housing status, physical comorbidities, and number of hospitalizations in the 1 year prior to baseline assessment). This helps to isolate the effect of alcohol use type on hospitalizations and mortality from other factors that are also highly associated with hospitalizations and death. All analyses compared the effect of different alcohol use types to the Late-onset Fewer Consequences type.
A majority of participants were between ages 50-64 (88%) at baseline assessment, male (72%), and separated or widowed (63.5%). A little less than half of participants were full- or part-time employed (41%), had between 9-12 years education (45%), and lived in a highly populated area (Town population >100,000 people; 46%). Over the 14-year period that was the study’s focus, there were a total of 11,455 hospital admissions and 346 deaths recorded, and approximately 70% of those events were alcohol related. Drug use disorder-related diagnoses (i.e., where the medical record stated the principal diagnosis or contributing causes for hospitalization or death was a substance use disorder other than alcohol) were recorded in 2.5% of cases (288 admissions and 4 deaths). Approximately 8% of hospital admissions during the study period were related to psychiatric diagnoses. More than 75% of participants were hospitalized at least once or died during the study period. Approximately two-thirds (57.3%) were hospitalized once or more related to alcohol disorders, 8.5% due to drug use disorders and 18.5% due to psychiatric-related diagnoses.
WHAT DID THIS STUDY FIND?
Risks for hospitalization or death were highest among older adults with early onset alcohol use and additional health difficulties compared to older adults with later onset of alcohol use and fewer consequences.
Compared to the Late-onset Fewer Consequences type, Early-onset Co-occurring Psychiatric Problems type had a:
• 27% increased risk of recurrent episode of all-cause hospitalization or death
• 34% increased risk of alcohol-related hospitalization or death
• 162% increased risk of for polydrug use-related hospitalization or death
Compared to the Late-onset Fewer Consequences type, Early-onset Multidimensional Issues type had a:
• 32% reduced risk of alcohol-related hospitalizations or death
• 155% increased risk of poly-drug use disorder-related hospitalizations or death
Compared to the Late-onset Fewer Consequences type, the risk of recurrent psychiatric hospitalization was:
•78% greater in the Late-onset with Co-occurring Anxiety and Depression type
•103% greater in the Early-onset Co-occurring Psychiatric Problems type
Risks were lowest among the Late-onset Fewer Consequences type and the Early-onset Major Alcohol Problems type.
The risk of all-cause hospitalization and death was:
• 27% lower in the Late-onset Fewer Consequences type, compared to the Co-occurring Psychiatric Problems type
There was no difference in the risk of all-cause hospitalization and death between Late-onset Fewer Consequences type and the Early-onset Major Alcohol Problems type.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of older Swedish adults assessed for alcohol use problems from 2003-2017, alcohol and psychiatric-related hospitalizations were high. Three-fourths of participants were hospitalized at least once during the study period – 70% of hospitalizations and 33% of deaths were alcohol related. Additionally, 18.5% of the cohort were hospitalized at least once with psychiatric-related disorders and 8.5% with drug use disorders. More than 10% were hospitalized at least once with dual alcohol use and psychiatric disorders.
Participants with early onset of regular and heavy drinking with co-occurring psychiatric problems were at highest risk for all-cause, alcohol-related, and psychiatric hospitalizations. This could be due to the fact that alcohol use also can exacerbate and perpetuate depression and anxiety symptoms. Additionally, alcohol interferes with medication efficacy for other psychological disorders on a physiological level, and can also interfere with adherence to taking the medications. Another study of older adults with alcohol use disorder found a similar pattern – participants with co-occurring psychiatric conditions reported more drinks per day when entering treatment compared to those without a co-occurring condition. This alcohol use type is similar to both Babor’s Type B and Cloninger’s Type II descriptions of alcohol use disorder, which also mention early onset of alcohol use, more psychopathology, and a family history of alcohol use.
Participants with late onset of regular and heavy drinking with anxiety and depression also had an elevated risk for psychiatric hospitalization. This group also had the highest proportion of women – nearly half the group were women, compared with a quarter or fewer in the other groups. This is expected as women have a higher prevalence of anxiety and depression compared to men. Historically rates of heavy drinking and alcohol problems have been higher in men than women. While they remain so, this gap is narrowing as rates of drinking are increasing among older women.
After an initial contact with the addiction services, most participants in this study had elevated risk for recurrent hospitalization for alcohol-, drug- and psychiatric-related disorders. Moreover, a significant proportion reported elevated prevalence of lifetime and recent history of depression, anxiety, suicidal ideation, loneliness, and trauma at baseline, suggesting a need for earlier and integrated trauma, addiction, and mental health services.
The absence of coordination between old-age care and addiction services might also be a barrier to detecting problematic alcohol use among older people. Given the high risk of recurrent hospitalization in the current study, older adults who are consuming alcohol and who have complex needs might benefit from efforts to improve substance use assessment in primary care settings, with sensitivity to the multi-dimensionality and consequences of problematic substance use among older people. Mental health services integrated within primary care has shown increased identification of mental health concerns within the VA system in the United States. Furthermore, training old-age care providers on late life substance use could provide social services with an additional point of contact for earlier identification of substance use problems and referral to treatment.
The researchers did not have information on the actual treatment provided to participants after their baseline assessment of alcohol problems. The analysis also did not include data from specialty outpatient or residential addiction treatment services. Given that, this analysis does not reflect how participation in treatment, or the nature of any treatment (substance use focused or integrated), may have impacted hospitalizations during the study period.
Although this analysis included drug use-related hospitalizations other than alcohol, participants were selected for inclusion based on problems with alcohol use at baseline, not problems with other substances. Given that, this analysis may not be representative of older adults with substance use problems other than alcohol.
Finally, participants were included based on being evaluated for alcohol use problems when in contact with social services in Sweden. There could be older adults in Sweden who were experiencing alcohol problems and were not assessed, and thus not included in this analysis.
BOTTOM LINE
This study found that, among 1741 older adults in Sweden who used social services and reported one or more alcohol problems, many experienced repeated hospitalizations over the 14-year study period, and risk varied by distinct clinical characteristics. Some older adults with co-occurring psychiatric problems or multidimensional issues had a greater risk for alcohol-, drug-, and psychiatric-related recurrent hospitalizations. The high rate of substance use and psychiatric-related hospitalizations suggests older people may benefit from integrated mental, addiction and physical health care.
For individuals and families seeking recovery: Older adults may experience alcohol problems that could go left unassessed and untreated. This study showed a high rate of hospitalizations due to alcohol and other drug use and psychiatric disorders among older adults with alcohol problems. Older people may benefit from integrated physical, addiction, and mental health care with age-sensitive components. Learn more about how alcohol affects the body as we age here.
For treatment professionals and treatment systems: As the baby boomer generation in the U.S. reaches older adulthood, the number of people needing addiction related services is expected to double. Rates of alcohol use among older adults in Sweden are similarly high to the U.S. In this study conducted in Sweden, given the high rate of hospitalization due to alcohol and other drug use and psychiatric disorders, and the differential risk throughout risk groups, older people may benefit from integrated mental, addiction and physical health care with age-sensitive components. Learn more about screening older adults for alcohol use disorder here.
For scientists:This retrospective cohort study examined Swedish adults aged 50 years an older (n = 1741) who used social services and were assessed for alcohol problems and from 2003-2017. Participants’ onset of drinking and other clinical characteristics were used in a latent class analysis to develop alcohol use types, then each type was examined in relation to hospitalizations and mortality over time. Older adult service users with early onset and co-occurring psychiatric problems were at highest risk for all-cause, alcohol-, drug-, and psychiatric hospitalizations. The current study did not include data on treatment participation. Because recurrent hospitalization was prevalent at follow-up, future studies should investigate the potential moderating effects of outpatient and residential addiction services between the baseline assessment and hospitalization or death.
For policy makers: As the baby boomer generation reaches older adulthood, the number of people needing addiction related services is expected to double. The high rate of hospitalization due to alcohol as well as other drug use and psychiatric disorders in this study raises concerns about the strain on the healthcare system in terms of services and costs. Early assessment and intervention may be one way to reduce costly hospitalizations in the future. Additional research is needed on how integrated care systems and treatments affect hospitalizations long term.
Hazardous drinking (e.g., drinking at levels that increase risk for greater health harms such as binge drinking and heavy alcohol use) is common among older adults in the U.S. Older adults may experience specific harms from hazardous drinking, such as falling or other unintentional injuries, memory problems, and severe medication interactions or forgetting to take needed medications in the first place, which may result in hospitalizations or death. Despite such risks, many older adults in the U.S. who meet criteria for alcohol use disorder are not receiving treatment for it.
As “baby boomers” (those born between 1946 and 1964) enter into older adulthood, the number of adults aged 50 or older with alcohol or other drug use disorders was projected to double from 2.8 million in 2006 to 5.7 million by 2020. Alcohol use has steadily increased in the population age 60 and above over the past 20 years, placing even further strain on the U.S. healthcare system in terms of services and costs. It is important to identify opportunities for early assessment and intervention on alcohol-related health complications among older adults to reduce preventable hospitalizations and premature mortality.
This retrospective cohort study from 2003-2017 of Swedish adults aged 50 years an older (n = 1741) examined participants’ onset of drinking problems and other clinical characteristics in relation to later hospitalizations and mortality over time.
Addiction treatment services in Sweden are primarily housed within publicly funded, decentralized social services within municipalities. The researchers used a Swedish national data set that includes records from 65 municipalities of all adults assessed for substance use severity in using the Addiction Severity Index from 2003 to 2017. The Addiction Severity Index is used in 90% of social services in Sweden, and is designed as a semi-structured interview to assess potential problem areas commonly affected by unhealthy substance use: physical health, employment and self-support, alcohol use, drug use, legal problems, family and social relationships, and psychiatric health. It also collects information on familial history of substance use and mental health status.
The researchers combined national Swedish data sets of substance use assessment with matched records of all physical and psychiatric-related hospital discharges, and causes of death. Participants were included in this study if they were at least 50 years of age and reported experiencing at least one alcohol problem on one or more days in the 30 days prior to a baseline assessment.
Using information from the interview, participants were categorized into 5 alcohol use types. Identifying specific types of problems is one way to examine clinical characteristics that tend to cluster together and then make predictions about common future health problems. This helps health professionals identify clients who may fit into a particular problem type and intervene on potential problems sooner.
The researchers identified 5 alcohol use types using an analysis that estimates a) the number of groups or types that exist within the data set, and b) the liklihood a participant has a certain clinical characteristic (e.g., history of depression) based on their predicted group or type. Although clinicians and researchers have already developed several systems and theories classifying the biopsychosocial factors that influence the varied clinical presentations of people with alcohol use disorder, called “typologies,” these typologies often have not considered or included older adults. Given the lack of knowledge about alcohol typologies among older adults, the researchers in this study developed their own typologies using a statistical approach with the goal of differentiating heterogeneous subtypes. The 5 types were:
The analysis examined the association between alcohol use type and all causes of hospitalization and death, controlling for relevant demographic and clinical characteristics (included age, sex, migration status, legal problems, marital status, employment, education, residential town population size, housing status, physical comorbidities, and number of hospitalizations in the 1 year prior to baseline assessment). This helps to isolate the effect of alcohol use type on hospitalizations and mortality from other factors that are also highly associated with hospitalizations and death. All analyses compared the effect of different alcohol use types to the Late-onset Fewer Consequences type.
A majority of participants were between ages 50-64 (88%) at baseline assessment, male (72%), and separated or widowed (63.5%). A little less than half of participants were full- or part-time employed (41%), had between 9-12 years education (45%), and lived in a highly populated area (Town population >100,000 people; 46%). Over the 14-year period that was the study’s focus, there were a total of 11,455 hospital admissions and 346 deaths recorded, and approximately 70% of those events were alcohol related. Drug use disorder-related diagnoses (i.e., where the medical record stated the principal diagnosis or contributing causes for hospitalization or death was a substance use disorder other than alcohol) were recorded in 2.5% of cases (288 admissions and 4 deaths). Approximately 8% of hospital admissions during the study period were related to psychiatric diagnoses. More than 75% of participants were hospitalized at least once or died during the study period. Approximately two-thirds (57.3%) were hospitalized once or more related to alcohol disorders, 8.5% due to drug use disorders and 18.5% due to psychiatric-related diagnoses.
WHAT DID THIS STUDY FIND?
Risks for hospitalization or death were highest among older adults with early onset alcohol use and additional health difficulties compared to older adults with later onset of alcohol use and fewer consequences.
Compared to the Late-onset Fewer Consequences type, Early-onset Co-occurring Psychiatric Problems type had a:
• 27% increased risk of recurrent episode of all-cause hospitalization or death
• 34% increased risk of alcohol-related hospitalization or death
• 162% increased risk of for polydrug use-related hospitalization or death
Compared to the Late-onset Fewer Consequences type, Early-onset Multidimensional Issues type had a:
• 32% reduced risk of alcohol-related hospitalizations or death
• 155% increased risk of poly-drug use disorder-related hospitalizations or death
Compared to the Late-onset Fewer Consequences type, the risk of recurrent psychiatric hospitalization was:
•78% greater in the Late-onset with Co-occurring Anxiety and Depression type
•103% greater in the Early-onset Co-occurring Psychiatric Problems type
Risks were lowest among the Late-onset Fewer Consequences type and the Early-onset Major Alcohol Problems type.
The risk of all-cause hospitalization and death was:
• 27% lower in the Late-onset Fewer Consequences type, compared to the Co-occurring Psychiatric Problems type
There was no difference in the risk of all-cause hospitalization and death between Late-onset Fewer Consequences type and the Early-onset Major Alcohol Problems type.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of older Swedish adults assessed for alcohol use problems from 2003-2017, alcohol and psychiatric-related hospitalizations were high. Three-fourths of participants were hospitalized at least once during the study period – 70% of hospitalizations and 33% of deaths were alcohol related. Additionally, 18.5% of the cohort were hospitalized at least once with psychiatric-related disorders and 8.5% with drug use disorders. More than 10% were hospitalized at least once with dual alcohol use and psychiatric disorders.
Participants with early onset of regular and heavy drinking with co-occurring psychiatric problems were at highest risk for all-cause, alcohol-related, and psychiatric hospitalizations. This could be due to the fact that alcohol use also can exacerbate and perpetuate depression and anxiety symptoms. Additionally, alcohol interferes with medication efficacy for other psychological disorders on a physiological level, and can also interfere with adherence to taking the medications. Another study of older adults with alcohol use disorder found a similar pattern – participants with co-occurring psychiatric conditions reported more drinks per day when entering treatment compared to those without a co-occurring condition. This alcohol use type is similar to both Babor’s Type B and Cloninger’s Type II descriptions of alcohol use disorder, which also mention early onset of alcohol use, more psychopathology, and a family history of alcohol use.
Participants with late onset of regular and heavy drinking with anxiety and depression also had an elevated risk for psychiatric hospitalization. This group also had the highest proportion of women – nearly half the group were women, compared with a quarter or fewer in the other groups. This is expected as women have a higher prevalence of anxiety and depression compared to men. Historically rates of heavy drinking and alcohol problems have been higher in men than women. While they remain so, this gap is narrowing as rates of drinking are increasing among older women.
After an initial contact with the addiction services, most participants in this study had elevated risk for recurrent hospitalization for alcohol-, drug- and psychiatric-related disorders. Moreover, a significant proportion reported elevated prevalence of lifetime and recent history of depression, anxiety, suicidal ideation, loneliness, and trauma at baseline, suggesting a need for earlier and integrated trauma, addiction, and mental health services.
The absence of coordination between old-age care and addiction services might also be a barrier to detecting problematic alcohol use among older people. Given the high risk of recurrent hospitalization in the current study, older adults who are consuming alcohol and who have complex needs might benefit from efforts to improve substance use assessment in primary care settings, with sensitivity to the multi-dimensionality and consequences of problematic substance use among older people. Mental health services integrated within primary care has shown increased identification of mental health concerns within the VA system in the United States. Furthermore, training old-age care providers on late life substance use could provide social services with an additional point of contact for earlier identification of substance use problems and referral to treatment.
The researchers did not have information on the actual treatment provided to participants after their baseline assessment of alcohol problems. The analysis also did not include data from specialty outpatient or residential addiction treatment services. Given that, this analysis does not reflect how participation in treatment, or the nature of any treatment (substance use focused or integrated), may have impacted hospitalizations during the study period.
Although this analysis included drug use-related hospitalizations other than alcohol, participants were selected for inclusion based on problems with alcohol use at baseline, not problems with other substances. Given that, this analysis may not be representative of older adults with substance use problems other than alcohol.
Finally, participants were included based on being evaluated for alcohol use problems when in contact with social services in Sweden. There could be older adults in Sweden who were experiencing alcohol problems and were not assessed, and thus not included in this analysis.
BOTTOM LINE
This study found that, among 1741 older adults in Sweden who used social services and reported one or more alcohol problems, many experienced repeated hospitalizations over the 14-year study period, and risk varied by distinct clinical characteristics. Some older adults with co-occurring psychiatric problems or multidimensional issues had a greater risk for alcohol-, drug-, and psychiatric-related recurrent hospitalizations. The high rate of substance use and psychiatric-related hospitalizations suggests older people may benefit from integrated mental, addiction and physical health care.
For individuals and families seeking recovery: Older adults may experience alcohol problems that could go left unassessed and untreated. This study showed a high rate of hospitalizations due to alcohol and other drug use and psychiatric disorders among older adults with alcohol problems. Older people may benefit from integrated physical, addiction, and mental health care with age-sensitive components. Learn more about how alcohol affects the body as we age here.
For treatment professionals and treatment systems: As the baby boomer generation in the U.S. reaches older adulthood, the number of people needing addiction related services is expected to double. Rates of alcohol use among older adults in Sweden are similarly high to the U.S. In this study conducted in Sweden, given the high rate of hospitalization due to alcohol and other drug use and psychiatric disorders, and the differential risk throughout risk groups, older people may benefit from integrated mental, addiction and physical health care with age-sensitive components. Learn more about screening older adults for alcohol use disorder here.
For scientists:This retrospective cohort study examined Swedish adults aged 50 years an older (n = 1741) who used social services and were assessed for alcohol problems and from 2003-2017. Participants’ onset of drinking and other clinical characteristics were used in a latent class analysis to develop alcohol use types, then each type was examined in relation to hospitalizations and mortality over time. Older adult service users with early onset and co-occurring psychiatric problems were at highest risk for all-cause, alcohol-, drug-, and psychiatric hospitalizations. The current study did not include data on treatment participation. Because recurrent hospitalization was prevalent at follow-up, future studies should investigate the potential moderating effects of outpatient and residential addiction services between the baseline assessment and hospitalization or death.
For policy makers: As the baby boomer generation reaches older adulthood, the number of people needing addiction related services is expected to double. The high rate of hospitalization due to alcohol as well as other drug use and psychiatric disorders in this study raises concerns about the strain on the healthcare system in terms of services and costs. Early assessment and intervention may be one way to reduce costly hospitalizations in the future. Additional research is needed on how integrated care systems and treatments affect hospitalizations long term.