Globally methamphetamine use disorder is a major public health issue. Methamphetamine use has multiple health consequences including elevated risk of HIV infection. Generally, men are more likely to use drugs than women, but the gender gap in methamphetamine use is narrower between women and men comparedto other substances. This is of concern given women may be more susceptible to methamphetamine addiction than men. It is unclear why these differences in addiction susceptibility occur, but it may be associated with greater risk for psychiatric comorbidity and other gender-specific life stress for women (e.g., childcare; cultural pressure and desire among women to be thin which stimulants can facilitate through suppressing appetite).
Furthermore, women who use methamphetamine face different barriers to recovery than men. For example, women who use methamphetamine are at elevated risk of intimate partner violence, and have more limited resources on average (e.g., low economic status). It is unclear, however, how methamphetamine use disorder treatment may need to be tailored to better serve women. To address this, the present study sought to identify gender differences in demographic and psychiatric comorbidity characteristics of a sample of treatment seeking methamphetamine use disorder patients.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis using data from the Crystal Project. The Crystal Project was a comparative study of 2 inpatient treatment methods employed by 2 different clinics in Germany. One clinic offered treatment as usual for substance use disorder. The other clinic offered the same treatment with additional amphetamine focused therapy (e.g., psychoeducation about stimulant use). The goal of the original study was to compare the efficacy of a stimulant specific treatment program and usual substance use disorder treatment in a cohort of methamphetamine using patients. The study that these data were derived from was conducted between 2016-2020. For these analyses, patients from both clinics were pooled and measured at baseline and follow-up (24 weeks post-baseline).
Study participants (N=108) met these inclusion criteria: 1) provided informed consent, 2) had a diagnosis of methamphetamine use disorder (according to ICD-10 diagnosis F15.2, mental and behavioral disorders are due to use of stimulants), and 3) were at least 18 years old. Participants were excluded from the study if a) they had concurrent “severe symptoms and severe [mental health] disorders” that could disrupt study participation (e.g., mania, or psychosis), b) engaged in substance use of any kind during the study (verified via urine tests), or c) were unable to read or understand the study tests.
Most variables for the present study were derived via self-report measures. Data were collected at baseline (~2 weeks post clinic admission) and at a follow-up assessment (~24 weeks post-baseline). At baseline, demographic data were collected according to the Documentation Standards III for the Evaluation of the Treatment of Dependents. Mental illness diagnoses were measured in several ways. First study staff conducted clinical interviews with participants to assess current and previous mental illness diagnoses. Additionally psychiatric diagnosis data were culled from participants medical records. Psychiatric symptoms data were obtained at both the baseline and follow-up assessment via the Symptom Checklist-90-Revised. This measure includes 90 items assessing nine subscales of mental health issues (e.g., depression and anxiety. Severity of psychological distress is also captured with this measure via global scales (e.g., the Global Severity Index).
WHAT DID THIS STUDY FIND?
Women were more likely to be diagnosed with mental health disorders then men.
Female participants were more likely to report co-occurring mental health disorder diagnoses (e.g., PTSD) than men at both study assessments. In addition, when examining the number of symptoms for each disorder, women also reported higher severity of these symptoms than men (e.g., via the global severity index).
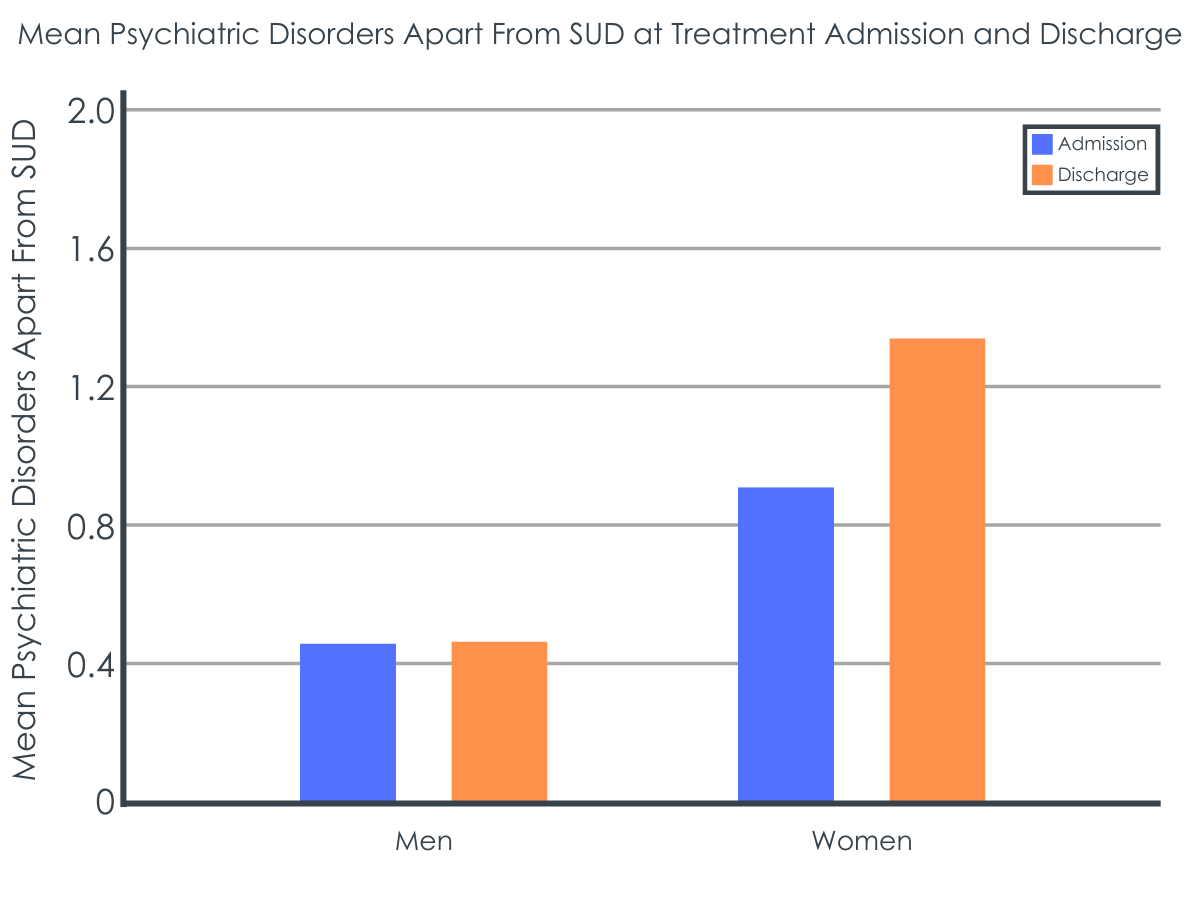
Significant gender differences in psychiatric symptom relief arose at the time of clinic discharge.
At the time they left either clinic, rates of psychiatric symptoms (e.g., depression) improved for men, on average. In contrast, women reported stable levels of psychiatric symptoms, on average, at discharge compared to baseline – their psychiatric symptoms did not improve during treatment. Men and women had similar attrition rates, so that differential dropout was unlikely to account for these differences in treatment response by gender.
Women had more clinical and life contexts which could affect treatment outcomes.
Women in this study were more likely to report having children to care for and of being single parents than men. In addition, women were more likely to report current/lifetime mental stress disorders and specific psychiatric disorders (e.g., posttraumatic stress disorder) known to be associated with poorer treatment outcomes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that on average women seeking treatment for methamphetamine use disorder face more psychiatric and social challenges than men. It is not possible to know from the findings reported in this specific study how these differences may have affected treatment efficacy as they were not reported. However, it is plausible that these factors may inform clinical needs when treating women for methamphetamine use disorder.
The researchers found that women were more likely to report non-addiction-related psychiatric comorbidities compared to men. Women also reported higher levels of psychological distress than men. These results generally align with past research demonstrating women who use methamphetamine suffer from high levels of psychological distress. These results may suggest that psychiatric comorbidities, which constitute substance use treatment barriers, are experienced more by women than men who use methamphetamine.
The researchers also found that women who used methamphetamine were more likely to report being a single parent relative to men. This suggests that women seeking methamphetamine use disorder treatment may face different social challenges and barriers to treatment than men. The fact that women were more likely to be the sole caregiver of children corroborates other research suggesting that childcare is a significant barrier to engaging in treatment for women. Offering childcare assistance for women with substance use disorder may therefore help increase women’s ability to engage in care. Other research suggests that women who use methamphetamine encounter high levels of social stigma, which may also lead to lower treatment utilization. Therefore, tailoring methamphetamine treatment to better accommodate the stigma faced by women (e.g., “failing” as a mother due to addiction) may improve the efficacy of treatment.
Of note, the study did not report findings related to post-treatment outcomes (e.g., relapse rates) so we cannot discern how women responded to the provided treatments compared to men. Furthermore, study attrition was very high (41%) – of the total baseline sample (n = 108) only 64 participants completed follow-up (59%). Although men and women had similar attrition rates, it is possible women having persistent elevated co-occurring disorders relative to men may have had different outcomes. For example, women’s co-occurring mental health issues may have affected behavioral change mechanisms through which substance use interventions operate. More research is needed to determine how treatment as usual can be modified to improve engagement and outcomes for women seeking methamphetamine use disorder treatment.
This study design does not allow for causal inferences about treatment effects specifically for women with methamphetamine use disorder. The authors measured psychiatric comorbidities at follow-up as a means of showing how well the inpatient rehabilitation program treated methamphetamine addiction. While psychological problems/symptoms are associated with methamphetamine use, there is no reason to assume that reductions in psychological problems/symptoms immediately following treatment necessarily would indicate recovery from substance use disorder.
The generalizability of this study’s findings is low due to several limitations. First, there was a high study dropout rate and the number of female participants in this study was very small. Only 22 women completed both the baseline and follow-up assessment, severely limiting the power of statistical analyses. Second, the researchers excluded patients with “severe disorders being able to influence (disrupt) measurements” (e.g., symptoms of depression, mania, psychosis, anxiety).” This is a problem as psychosis is a common consequence of methamphetamine use. Finally, the sample was comprised exclusively of those in treatment at an inpatient facility. Conclusions cannot be drawn at all about those with a methamphetamine use disorder not in treatment (e.g., due to incarceration).
BOTTOM LINE
Women with methamphetamine use disorders may have more psychiatric comorbidities and experience worse symptoms of psychological disorders than men. Furthermore, women with methamphetamine use disorders may face unique childcare needs. These factors together may affect women’s ability to receive substance use disorder treatment and achieve recovery. While this study does not directly inform how methamphetamine use treatment can be tailored to improve outcomes for women, it may suggest that addressing specific issues relevant to women who use methamphetamine (e.g., childcare assistance, and mental health problems) may help increase their ability to engage in care. In addition, this work contributes to the growing body of work on gender-specific health care needs of women with methamphetamine use disorder.
For individuals and families seeking recovery: The present study may indicate that women face more barriers to methamphetamine use treatment than men. Therefore, it is important for those seeking treatment for themselves or others to be aware of all available treatment options. For example, if a lack of childcare precludes visiting a substance use treatment center, telemedicine services could be an option. Such services are often covered by insurance including Medicaid.
For treatment professionals and treatment systems: Based on the present study, women who use methamphetamine may suffer from psychiatric problems more than men. As such, it is important for providers to be aware of such comorbidities and try to accommodate for them. This could entail considering how such issues may serve as barriers to treatment and/or impediments to successful recovery. Like past research, it may be important to consider how these issues affect the mechanisms of behavior change. For example, coping skills and self-efficacy related to mental health problems could affect substance use disorder treatment outcomes.
For scientists: The present study offers some clues that women face significant barriers to methamphetamine use disorder treatment and recovery. The inferences that can be drawn about how these factors play a role in treatment efficacy and how interventions can be changed to meet women’s needs are limited. Future research might investigate the ways in which psychiatric symptom severity predicts methamphetamine use disorder recovery among women. In addition, studies examining women’s beliefs about stigma, as well as treatment efficacy, and their associations with substance use and related treatment outcomes, would be useful.
For policy makers: Women in treatment for methamphetamine use disorder were more likely to have a diagnosis of psychiatric problems and to report severe mental health symptoms. Women who used methamphetamine were also more likely to report being the sole caregiver of a child. This suggests that women may face unique challenges to achieving methamphetamine use disorder recovery. As such, policymakers may want to consider strategies to improve women’s access to mental health and substance use disorder treatment (e.g., through Medicaid). This could include partnering with local foundations to channel funding where methamphetamine use is endemic.
Globally methamphetamine use disorder is a major public health issue. Methamphetamine use has multiple health consequences including elevated risk of HIV infection. Generally, men are more likely to use drugs than women, but the gender gap in methamphetamine use is narrower between women and men comparedto other substances. This is of concern given women may be more susceptible to methamphetamine addiction than men. It is unclear why these differences in addiction susceptibility occur, but it may be associated with greater risk for psychiatric comorbidity and other gender-specific life stress for women (e.g., childcare; cultural pressure and desire among women to be thin which stimulants can facilitate through suppressing appetite).
Furthermore, women who use methamphetamine face different barriers to recovery than men. For example, women who use methamphetamine are at elevated risk of intimate partner violence, and have more limited resources on average (e.g., low economic status). It is unclear, however, how methamphetamine use disorder treatment may need to be tailored to better serve women. To address this, the present study sought to identify gender differences in demographic and psychiatric comorbidity characteristics of a sample of treatment seeking methamphetamine use disorder patients.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis using data from the Crystal Project. The Crystal Project was a comparative study of 2 inpatient treatment methods employed by 2 different clinics in Germany. One clinic offered treatment as usual for substance use disorder. The other clinic offered the same treatment with additional amphetamine focused therapy (e.g., psychoeducation about stimulant use). The goal of the original study was to compare the efficacy of a stimulant specific treatment program and usual substance use disorder treatment in a cohort of methamphetamine using patients. The study that these data were derived from was conducted between 2016-2020. For these analyses, patients from both clinics were pooled and measured at baseline and follow-up (24 weeks post-baseline).
Study participants (N=108) met these inclusion criteria: 1) provided informed consent, 2) had a diagnosis of methamphetamine use disorder (according to ICD-10 diagnosis F15.2, mental and behavioral disorders are due to use of stimulants), and 3) were at least 18 years old. Participants were excluded from the study if a) they had concurrent “severe symptoms and severe [mental health] disorders” that could disrupt study participation (e.g., mania, or psychosis), b) engaged in substance use of any kind during the study (verified via urine tests), or c) were unable to read or understand the study tests.
Most variables for the present study were derived via self-report measures. Data were collected at baseline (~2 weeks post clinic admission) and at a follow-up assessment (~24 weeks post-baseline). At baseline, demographic data were collected according to the Documentation Standards III for the Evaluation of the Treatment of Dependents. Mental illness diagnoses were measured in several ways. First study staff conducted clinical interviews with participants to assess current and previous mental illness diagnoses. Additionally psychiatric diagnosis data were culled from participants medical records. Psychiatric symptoms data were obtained at both the baseline and follow-up assessment via the Symptom Checklist-90-Revised. This measure includes 90 items assessing nine subscales of mental health issues (e.g., depression and anxiety. Severity of psychological distress is also captured with this measure via global scales (e.g., the Global Severity Index).
WHAT DID THIS STUDY FIND?
Women were more likely to be diagnosed with mental health disorders then men.
Female participants were more likely to report co-occurring mental health disorder diagnoses (e.g., PTSD) than men at both study assessments. In addition, when examining the number of symptoms for each disorder, women also reported higher severity of these symptoms than men (e.g., via the global severity index).
Significant gender differences in psychiatric symptom relief arose at the time of clinic discharge.
At the time they left either clinic, rates of psychiatric symptoms (e.g., depression) improved for men, on average. In contrast, women reported stable levels of psychiatric symptoms, on average, at discharge compared to baseline – their psychiatric symptoms did not improve during treatment. Men and women had similar attrition rates, so that differential dropout was unlikely to account for these differences in treatment response by gender.
Women had more clinical and life contexts which could affect treatment outcomes.
Women in this study were more likely to report having children to care for and of being single parents than men. In addition, women were more likely to report current/lifetime mental stress disorders and specific psychiatric disorders (e.g., posttraumatic stress disorder) known to be associated with poorer treatment outcomes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that on average women seeking treatment for methamphetamine use disorder face more psychiatric and social challenges than men. It is not possible to know from the findings reported in this specific study how these differences may have affected treatment efficacy as they were not reported. However, it is plausible that these factors may inform clinical needs when treating women for methamphetamine use disorder.
The researchers found that women were more likely to report non-addiction-related psychiatric comorbidities compared to men. Women also reported higher levels of psychological distress than men. These results generally align with past research demonstrating women who use methamphetamine suffer from high levels of psychological distress. These results may suggest that psychiatric comorbidities, which constitute substance use treatment barriers, are experienced more by women than men who use methamphetamine.
The researchers also found that women who used methamphetamine were more likely to report being a single parent relative to men. This suggests that women seeking methamphetamine use disorder treatment may face different social challenges and barriers to treatment than men. The fact that women were more likely to be the sole caregiver of children corroborates other research suggesting that childcare is a significant barrier to engaging in treatment for women. Offering childcare assistance for women with substance use disorder may therefore help increase women’s ability to engage in care. Other research suggests that women who use methamphetamine encounter high levels of social stigma, which may also lead to lower treatment utilization. Therefore, tailoring methamphetamine treatment to better accommodate the stigma faced by women (e.g., “failing” as a mother due to addiction) may improve the efficacy of treatment.
Of note, the study did not report findings related to post-treatment outcomes (e.g., relapse rates) so we cannot discern how women responded to the provided treatments compared to men. Furthermore, study attrition was very high (41%) – of the total baseline sample (n = 108) only 64 participants completed follow-up (59%). Although men and women had similar attrition rates, it is possible women having persistent elevated co-occurring disorders relative to men may have had different outcomes. For example, women’s co-occurring mental health issues may have affected behavioral change mechanisms through which substance use interventions operate. More research is needed to determine how treatment as usual can be modified to improve engagement and outcomes for women seeking methamphetamine use disorder treatment.
This study design does not allow for causal inferences about treatment effects specifically for women with methamphetamine use disorder. The authors measured psychiatric comorbidities at follow-up as a means of showing how well the inpatient rehabilitation program treated methamphetamine addiction. While psychological problems/symptoms are associated with methamphetamine use, there is no reason to assume that reductions in psychological problems/symptoms immediately following treatment necessarily would indicate recovery from substance use disorder.
The generalizability of this study’s findings is low due to several limitations. First, there was a high study dropout rate and the number of female participants in this study was very small. Only 22 women completed both the baseline and follow-up assessment, severely limiting the power of statistical analyses. Second, the researchers excluded patients with “severe disorders being able to influence (disrupt) measurements” (e.g., symptoms of depression, mania, psychosis, anxiety).” This is a problem as psychosis is a common consequence of methamphetamine use. Finally, the sample was comprised exclusively of those in treatment at an inpatient facility. Conclusions cannot be drawn at all about those with a methamphetamine use disorder not in treatment (e.g., due to incarceration).
BOTTOM LINE
Women with methamphetamine use disorders may have more psychiatric comorbidities and experience worse symptoms of psychological disorders than men. Furthermore, women with methamphetamine use disorders may face unique childcare needs. These factors together may affect women’s ability to receive substance use disorder treatment and achieve recovery. While this study does not directly inform how methamphetamine use treatment can be tailored to improve outcomes for women, it may suggest that addressing specific issues relevant to women who use methamphetamine (e.g., childcare assistance, and mental health problems) may help increase their ability to engage in care. In addition, this work contributes to the growing body of work on gender-specific health care needs of women with methamphetamine use disorder.
For individuals and families seeking recovery: The present study may indicate that women face more barriers to methamphetamine use treatment than men. Therefore, it is important for those seeking treatment for themselves or others to be aware of all available treatment options. For example, if a lack of childcare precludes visiting a substance use treatment center, telemedicine services could be an option. Such services are often covered by insurance including Medicaid.
For treatment professionals and treatment systems: Based on the present study, women who use methamphetamine may suffer from psychiatric problems more than men. As such, it is important for providers to be aware of such comorbidities and try to accommodate for them. This could entail considering how such issues may serve as barriers to treatment and/or impediments to successful recovery. Like past research, it may be important to consider how these issues affect the mechanisms of behavior change. For example, coping skills and self-efficacy related to mental health problems could affect substance use disorder treatment outcomes.
For scientists: The present study offers some clues that women face significant barriers to methamphetamine use disorder treatment and recovery. The inferences that can be drawn about how these factors play a role in treatment efficacy and how interventions can be changed to meet women’s needs are limited. Future research might investigate the ways in which psychiatric symptom severity predicts methamphetamine use disorder recovery among women. In addition, studies examining women’s beliefs about stigma, as well as treatment efficacy, and their associations with substance use and related treatment outcomes, would be useful.
For policy makers: Women in treatment for methamphetamine use disorder were more likely to have a diagnosis of psychiatric problems and to report severe mental health symptoms. Women who used methamphetamine were also more likely to report being the sole caregiver of a child. This suggests that women may face unique challenges to achieving methamphetamine use disorder recovery. As such, policymakers may want to consider strategies to improve women’s access to mental health and substance use disorder treatment (e.g., through Medicaid). This could include partnering with local foundations to channel funding where methamphetamine use is endemic.
Globally methamphetamine use disorder is a major public health issue. Methamphetamine use has multiple health consequences including elevated risk of HIV infection. Generally, men are more likely to use drugs than women, but the gender gap in methamphetamine use is narrower between women and men comparedto other substances. This is of concern given women may be more susceptible to methamphetamine addiction than men. It is unclear why these differences in addiction susceptibility occur, but it may be associated with greater risk for psychiatric comorbidity and other gender-specific life stress for women (e.g., childcare; cultural pressure and desire among women to be thin which stimulants can facilitate through suppressing appetite).
Furthermore, women who use methamphetamine face different barriers to recovery than men. For example, women who use methamphetamine are at elevated risk of intimate partner violence, and have more limited resources on average (e.g., low economic status). It is unclear, however, how methamphetamine use disorder treatment may need to be tailored to better serve women. To address this, the present study sought to identify gender differences in demographic and psychiatric comorbidity characteristics of a sample of treatment seeking methamphetamine use disorder patients.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary analysis using data from the Crystal Project. The Crystal Project was a comparative study of 2 inpatient treatment methods employed by 2 different clinics in Germany. One clinic offered treatment as usual for substance use disorder. The other clinic offered the same treatment with additional amphetamine focused therapy (e.g., psychoeducation about stimulant use). The goal of the original study was to compare the efficacy of a stimulant specific treatment program and usual substance use disorder treatment in a cohort of methamphetamine using patients. The study that these data were derived from was conducted between 2016-2020. For these analyses, patients from both clinics were pooled and measured at baseline and follow-up (24 weeks post-baseline).
Study participants (N=108) met these inclusion criteria: 1) provided informed consent, 2) had a diagnosis of methamphetamine use disorder (according to ICD-10 diagnosis F15.2, mental and behavioral disorders are due to use of stimulants), and 3) were at least 18 years old. Participants were excluded from the study if a) they had concurrent “severe symptoms and severe [mental health] disorders” that could disrupt study participation (e.g., mania, or psychosis), b) engaged in substance use of any kind during the study (verified via urine tests), or c) were unable to read or understand the study tests.
Most variables for the present study were derived via self-report measures. Data were collected at baseline (~2 weeks post clinic admission) and at a follow-up assessment (~24 weeks post-baseline). At baseline, demographic data were collected according to the Documentation Standards III for the Evaluation of the Treatment of Dependents. Mental illness diagnoses were measured in several ways. First study staff conducted clinical interviews with participants to assess current and previous mental illness diagnoses. Additionally psychiatric diagnosis data were culled from participants medical records. Psychiatric symptoms data were obtained at both the baseline and follow-up assessment via the Symptom Checklist-90-Revised. This measure includes 90 items assessing nine subscales of mental health issues (e.g., depression and anxiety. Severity of psychological distress is also captured with this measure via global scales (e.g., the Global Severity Index).
WHAT DID THIS STUDY FIND?
Women were more likely to be diagnosed with mental health disorders then men.
Female participants were more likely to report co-occurring mental health disorder diagnoses (e.g., PTSD) than men at both study assessments. In addition, when examining the number of symptoms for each disorder, women also reported higher severity of these symptoms than men (e.g., via the global severity index).
Significant gender differences in psychiatric symptom relief arose at the time of clinic discharge.
At the time they left either clinic, rates of psychiatric symptoms (e.g., depression) improved for men, on average. In contrast, women reported stable levels of psychiatric symptoms, on average, at discharge compared to baseline – their psychiatric symptoms did not improve during treatment. Men and women had similar attrition rates, so that differential dropout was unlikely to account for these differences in treatment response by gender.
Women had more clinical and life contexts which could affect treatment outcomes.
Women in this study were more likely to report having children to care for and of being single parents than men. In addition, women were more likely to report current/lifetime mental stress disorders and specific psychiatric disorders (e.g., posttraumatic stress disorder) known to be associated with poorer treatment outcomes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that on average women seeking treatment for methamphetamine use disorder face more psychiatric and social challenges than men. It is not possible to know from the findings reported in this specific study how these differences may have affected treatment efficacy as they were not reported. However, it is plausible that these factors may inform clinical needs when treating women for methamphetamine use disorder.
The researchers found that women were more likely to report non-addiction-related psychiatric comorbidities compared to men. Women also reported higher levels of psychological distress than men. These results generally align with past research demonstrating women who use methamphetamine suffer from high levels of psychological distress. These results may suggest that psychiatric comorbidities, which constitute substance use treatment barriers, are experienced more by women than men who use methamphetamine.
The researchers also found that women who used methamphetamine were more likely to report being a single parent relative to men. This suggests that women seeking methamphetamine use disorder treatment may face different social challenges and barriers to treatment than men. The fact that women were more likely to be the sole caregiver of children corroborates other research suggesting that childcare is a significant barrier to engaging in treatment for women. Offering childcare assistance for women with substance use disorder may therefore help increase women’s ability to engage in care. Other research suggests that women who use methamphetamine encounter high levels of social stigma, which may also lead to lower treatment utilization. Therefore, tailoring methamphetamine treatment to better accommodate the stigma faced by women (e.g., “failing” as a mother due to addiction) may improve the efficacy of treatment.
Of note, the study did not report findings related to post-treatment outcomes (e.g., relapse rates) so we cannot discern how women responded to the provided treatments compared to men. Furthermore, study attrition was very high (41%) – of the total baseline sample (n = 108) only 64 participants completed follow-up (59%). Although men and women had similar attrition rates, it is possible women having persistent elevated co-occurring disorders relative to men may have had different outcomes. For example, women’s co-occurring mental health issues may have affected behavioral change mechanisms through which substance use interventions operate. More research is needed to determine how treatment as usual can be modified to improve engagement and outcomes for women seeking methamphetamine use disorder treatment.
This study design does not allow for causal inferences about treatment effects specifically for women with methamphetamine use disorder. The authors measured psychiatric comorbidities at follow-up as a means of showing how well the inpatient rehabilitation program treated methamphetamine addiction. While psychological problems/symptoms are associated with methamphetamine use, there is no reason to assume that reductions in psychological problems/symptoms immediately following treatment necessarily would indicate recovery from substance use disorder.
The generalizability of this study’s findings is low due to several limitations. First, there was a high study dropout rate and the number of female participants in this study was very small. Only 22 women completed both the baseline and follow-up assessment, severely limiting the power of statistical analyses. Second, the researchers excluded patients with “severe disorders being able to influence (disrupt) measurements” (e.g., symptoms of depression, mania, psychosis, anxiety).” This is a problem as psychosis is a common consequence of methamphetamine use. Finally, the sample was comprised exclusively of those in treatment at an inpatient facility. Conclusions cannot be drawn at all about those with a methamphetamine use disorder not in treatment (e.g., due to incarceration).
BOTTOM LINE
Women with methamphetamine use disorders may have more psychiatric comorbidities and experience worse symptoms of psychological disorders than men. Furthermore, women with methamphetamine use disorders may face unique childcare needs. These factors together may affect women’s ability to receive substance use disorder treatment and achieve recovery. While this study does not directly inform how methamphetamine use treatment can be tailored to improve outcomes for women, it may suggest that addressing specific issues relevant to women who use methamphetamine (e.g., childcare assistance, and mental health problems) may help increase their ability to engage in care. In addition, this work contributes to the growing body of work on gender-specific health care needs of women with methamphetamine use disorder.
For individuals and families seeking recovery: The present study may indicate that women face more barriers to methamphetamine use treatment than men. Therefore, it is important for those seeking treatment for themselves or others to be aware of all available treatment options. For example, if a lack of childcare precludes visiting a substance use treatment center, telemedicine services could be an option. Such services are often covered by insurance including Medicaid.
For treatment professionals and treatment systems: Based on the present study, women who use methamphetamine may suffer from psychiatric problems more than men. As such, it is important for providers to be aware of such comorbidities and try to accommodate for them. This could entail considering how such issues may serve as barriers to treatment and/or impediments to successful recovery. Like past research, it may be important to consider how these issues affect the mechanisms of behavior change. For example, coping skills and self-efficacy related to mental health problems could affect substance use disorder treatment outcomes.
For scientists: The present study offers some clues that women face significant barriers to methamphetamine use disorder treatment and recovery. The inferences that can be drawn about how these factors play a role in treatment efficacy and how interventions can be changed to meet women’s needs are limited. Future research might investigate the ways in which psychiatric symptom severity predicts methamphetamine use disorder recovery among women. In addition, studies examining women’s beliefs about stigma, as well as treatment efficacy, and their associations with substance use and related treatment outcomes, would be useful.
For policy makers: Women in treatment for methamphetamine use disorder were more likely to have a diagnosis of psychiatric problems and to report severe mental health symptoms. Women who used methamphetamine were also more likely to report being the sole caregiver of a child. This suggests that women may face unique challenges to achieving methamphetamine use disorder recovery. As such, policymakers may want to consider strategies to improve women’s access to mental health and substance use disorder treatment (e.g., through Medicaid). This could include partnering with local foundations to channel funding where methamphetamine use is endemic.