Greater harms for different drinking patterns in younger versus older people may reflect the nature of alcohol use disorder over the life course
What constitutes harmful drinking for individuals not meeting alcohol use disorder criteria varies by life stage. Therefore, screenings to identify people that need treatment may be more accurate if they account for someone’s life stage. At the same time, an age-based approach could make these screenings overly complex, decreasing the likelihood that busy clinicians will use them. To examine the potential utility of an age-based screening approach, this study examined whether some drinking variables were better predictors of harms for younger versus older adults.
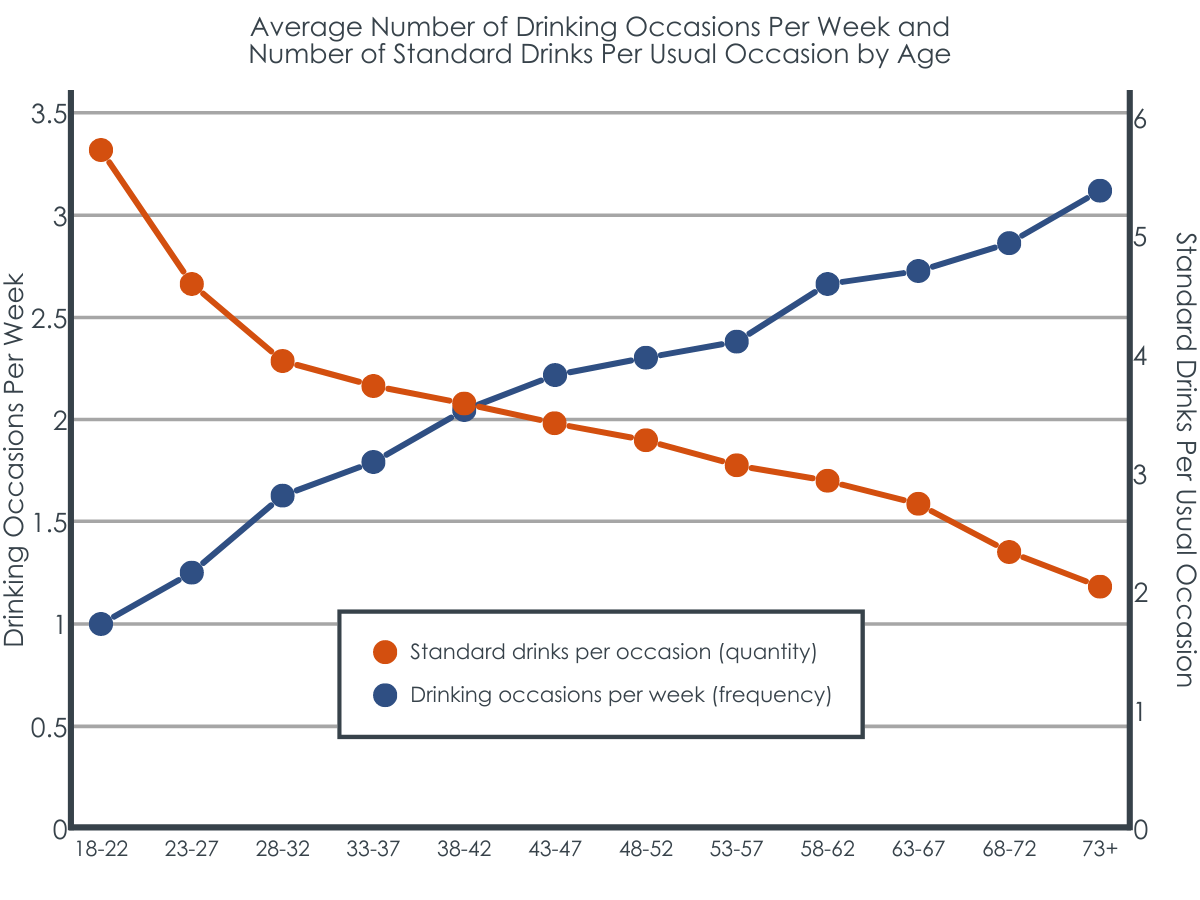
Alcohol use patterns can vary widely across the life span. That is, at a population level, as individuals age, they tend to drink alcohol more often (i.e., increasein their drinking frequency), but also tend to consume fewerdrinks per occasion (i.e., reduce their quantity of drinking at a single event). Although merely consuming alcohol can result in harmful health consequences, some individuals may be at particularly increased risk for developing an alcohol use disorder – that is continued drinking despite significant levels of alcohol-related functional impairment and distress, increasing the risk for disease, disability, and premature death.
Screening tools can help identify individuals most in need of intervention, but given the differences between subgroups of the population,screening tools have some limitations. That is, screening tools may be too sensitive (i.e., result in a false positive, indicatingsomeone may have a severe problem and need a clinical intervention when they may not) or not sensitive enough (i.e., result in a false negative, failing to identify those in need of clinical intervention). One screening tool for alcohol use that is commonly used by clinicians and interventionists worldwide is the Alcohol Use Disorders Identification Test (AUDIT).The AUDIT includes questions on frequency and quantity of drinking as well as drinking-related consequences, and has been used for youth and adults alike.
This study examined whether the amount and frequency of drinking were better at predicting drinking-related harms and consequences for each of these age groups.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis from a national sample of adults ages 14 and older who completed the 2016 Australian National Drug Strategy Household Survey.The survey is a national, cross-sectional survey that is conducted in Australia every 3 years. Respondents are asked a variety of questions about alcohol and drug use behaviors and attitudes. In 2016, the survey was administered to 23,772 Australian individuals; the sample of 22,642 participants used for this study were those who indicated that they were at least 18 years old and reported drinking at least some alcohol at some point in their life. In contrast to the US, where the legal drinking age is 21 years old, the legal drinking age in Australia is 18 years old.
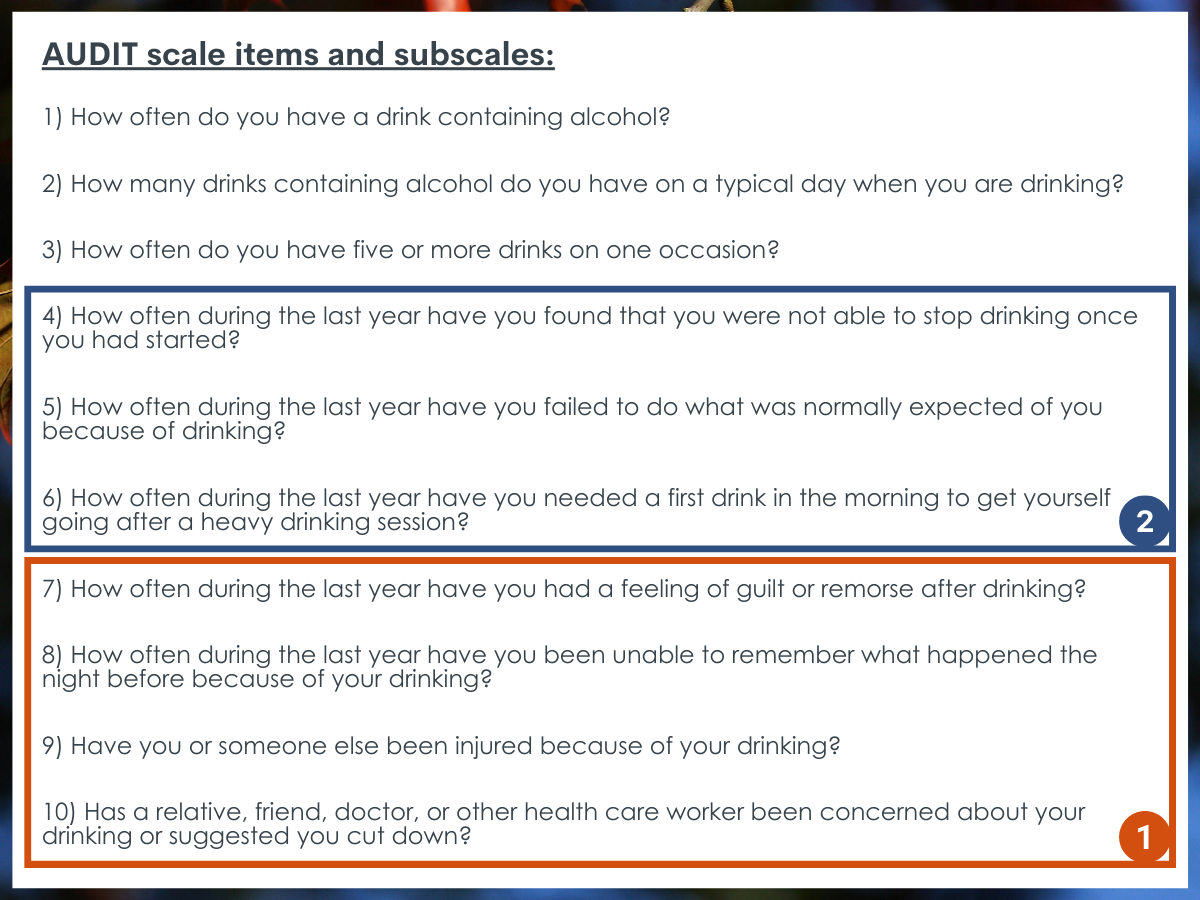
The survey included some questions either taken directly from the AUDIT or used some very similar questions, to assess alcohol use patterns. The AUDIT is a standardized scale, used worldwide. It has 10 questions and results in a score from 0-40, where higher scores indicate greater alcohol use. It has two subscales that can be calculated in addition to the total score: harmful alcohol use (AUDIT questions 7-10 for a score of 0-12) and alcohol dependence (AUDIT questions 4-6 for a score of 0-12).
Figure 1. As mentioned in the above paragraph, the AUDIT scale contains two subscales that can be calculated in addition to the total score: Questions 7-10 for a subscale of harmful alcohol use; Questions 4-6 for a subscale of alcohol dependence.
In this analysis, the researchers used the frequency of alcohol consumption (drinking occasions per week) and amount of drinking (quantity) per typical drinking occasion to predict the AUDIT dependence score (from the AUDIT dependence subscale) and the AUDIT harmful drinking score (from the AUDIT harms subscale).Alcohol quantity was measured using a drink size of 10g of ethanol, which is a standard drink size in Australia (in the US, a standard drink size is 14g). Age was included as a categorical variable in incremental 5-year blocks so that gradual comparisons by age groupings could be examined.
Of the sample of 17,399 adults included in this analysis, just over half were female (53%) and the average age was 50 (SD = 17). Approximately 24% of the sample had a total AUDIT score of 8 or higher and so were indicated as needing intervention according to the AUDIT guidelines.
WHAT DID THIS STUDY FIND?
The ability of drinking frequency and quantity to predict alcohol-related harms differed by participant age.
For those aged 18-27, how often they drank alcohol (i.e., their frequency of alcohol consumption) was about twice as good a predictor of both dependence and harmful drinking AUDIT scores than the amount (i.e., quantity) consumed per drinking occasion. That is, although both the frequency and quantity items contributed to these overall scores, younger adults who indicated high frequency were more likely to be identified as needing intervention than younger adults who indicated high quantity of drinking per occasion.
In contrast, for participants aged 43 and older, the quantity consumed per drinking occasion was twice as good a predictor of dependence AUDIT scores than frequency of alcohol consumption. That is, although both the frequency and quantity items contribute to these overall scores, older adults who indicated a higher quantity of drinking per occasion were more likely to be identified as needing intervention than older adults who indicated higher frequency of drinking. This pattern was also similar among adults aged 43 or older for harmful drinking AUDIT scores, although not for those between 53-57 years old.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 17,399 adults found that, overall, younger adults typically drink less often, but more per occasion, than older adults. As such, it is actually the frequency with which young adults drink that more strongly predicts alcohol-related harms as measured by the AUDIT. In contrast, older adults showed the opposite pattern; they typically drink more often, but fewer drinks per drinking occasion. As such, it is the number of drinking per drinking occasion (i.e., “intensity”) that is the strongly predicts alcohol-related harms for this group.
While some individuals will develop chronic forms of alcohol use disorder, many who show heavy alcohol use patterns during emerging adulthood will “age out” as they assume greater responsibilities and meaningful activities that take up more of their free time. The researchers conducting this study suggest that in a limited time setting such as a clinic, focusing on screening for more frequent drinking may be very useful when working with younger adults for identifying a treatment need.It is possible that drinking frequency can more readily identify young people with drinking-related consequences who may need help to change their drinking. Alternatively, the authors suggest that the results for older adults indicate that screening for more heavy drinking may be more useful for this population when seeking to identify individuals who would benefit most from alcohol use disorder treatment.
That said, while this study helps to identify differences between the nature of alcohol use disorder in younger versus older adults, itis important to always assess for both quantity and frequency across all developmental life stages for two key reasons. One, screeners are intended to be brief and easy to administer. Adding more complex rules for interpretation depending on age range may make the AUDIT and other screeners like it unduly burdensome for healthcare professionals. Second, alcohol screeners are useful beyond their ability to identify individuals who meet the clinical threshold of alcohol use disorder. Specifically, alcohol-related hazards (i.e., injuries) and harms (i.e., toxicity effects such as cancer and liver disease) result simply from alcohol consumption, both in terms of how often someone drinks and how much they consume on each drinking occasion.
Another aspect of what the researchers may be capturing here is the development of alcohol use disorder across the lifespan. That is, as alcohol use disorder/dependency develops, the frequency of alcohol use is paramount; once alcohol dependency is developed, maintaining it requires more intensive use (e.g., as tolerance develops and neuroadaptation occurs). In other words, on average, in the development of alcohol use disorder, early adulthood is the time when the habitual patterns of the behavior often become ingrained that begins the process of dependence; then once acquired, the brain needs more alcohol to get the same effect over time as one ages.
In sum, brief and accurate screening tools are highly scalable resources with the potential for public health impact, yet their use might possibly be enhanced by tailoring them to specific patient characteristics, such as developmental stage as this study suggests. It should be remembered that given their broad and general approach to identifying drinking harms, screening tools like the AUDIT are best viewed as opportunities to begin a conversation about risky health behaviors, consequences, and readiness for change.
The study did not examine other characteristics that could influence how drinking behavior patterns might be more prone to harmful drinking/dependence (e.g., gender, sexual orientation, minoritized status, and mental health comorbidities). Further exploration of these characteristics and potential interactions between them would help to further understand the need to tailor screening tools for different populations.
This study only focused on a single screening tool, the AUDIT, and cannot speak to the ability of other screening tools to be specific and sensitive enough for the population of interest.
BOTTOM LINE
The researchers found that using the AUDIT screening tool, the frequency of alcohol consumption was a better predictor of alcohol-related consequences in younger adults but more drinks per occasion was a stronger predictor of consequences in older adults. While this finding may suggest greater utility of age-specific interpretations of this screener, clinical screening tools are more likely to be adopted and implemented when they are easy to use, score, and interpret. Adding complexity by introducing different scoring that caters to different subgroups may result in less actual real-world use. It is also may be that these findings reflect how alcohol use disorder changes over the lifespan. Given that the hazards (e.g., injuries) and harms (e.g., liver toxicity) of alcohol use generally result simply from alcohol consumption, keeping the threshold lower to identify as many cases of risky drinking as possible, at the expense of more false positives, will aid with detection of most/all of the actual harmful use cases of alcohol use, regardless of age, thereby more efficiently addressing the public health burden of alcohol.
For individuals and families seeking recovery: Drinking less alcohol and/or drinking less frequentlycan result in improved health and well-being. Although it can be difficult at times to understand whether someone’s drinking behaviors warrants treatment, it is important to have conversations with your loved ones if you are concerned and to support them to speak with a provider. This study demonstrates that especially for younger adults, noticing more frequent drinking could be a sign of alcohol use disorder, while for older adults, noticing heavy drinking during single occasions could be a sign for intervention.
For treatment professionals and treatment systems: The ability to screen and intervene on problematic alcohol use in primary care and other medical settings can help improve the health and well-being of individuals who exhibit these alcohol use patterns and also reduce alcohol’s broader public health burden. Although short screening tools such as the AUDIT are useful for identifying levels of alcohol use that may need intervention, it is important to carefully implement these tools in clinical practice. These tools can be a helpful starting point for discussion, but treatment professionals should also consider the target population of focus (i.e., patient-centered care) and whether certain drinking patterns may be more likely to indicate need for swift or more intensive intervention than what the current scoring algorithms of these tools currently suggest.
For scientists:This study highlights a potential need to closely examine how drinking behavior patterns in different population subgroups may drive certain screening tool scores, and whether the sensitivity of those tools to indicate care is compromised. Although much work has been done on the factorial invariance of screening tools like the AUDIT, more fine-grained analyses with larger samples might reveal nuances that have clinical significance. That said, increasing these tools’ universal sensitivity (e.g., lowering the overall screening threshold score that triggers further assessment) may be one approach to investigate to accurately detect the whole range and variety of different patterns of alcohol use that are associated with health harms irrespective of the different characteristics of individuals in the population who could benefit from care, unless differences are very large between sub-groups. Given simplicity in administration, scoring, and interpretation is key in tool adoption in clinical practice, a single change in scoring is likely to result higher adoption than having multiple scoring algorithms or different screening tools for different population subgroups.
For policy makers: Screening for problematic alcohol use in primary care and other medical settings can help to improve public health. Supporting research that addresses how to best tailor alcohol screening tools and providing funding for clinical initiatives to improve existing approaches so as not to miss important at-risk population subgroups could have potential to further enhance public health in more effective and cost-efficient ways.
Alcohol use patterns can vary widely across the life span. That is, at a population level, as individuals age, they tend to drink alcohol more often (i.e., increasein their drinking frequency), but also tend to consume fewerdrinks per occasion (i.e., reduce their quantity of drinking at a single event). Although merely consuming alcohol can result in harmful health consequences, some individuals may be at particularly increased risk for developing an alcohol use disorder – that is continued drinking despite significant levels of alcohol-related functional impairment and distress, increasing the risk for disease, disability, and premature death.
Screening tools can help identify individuals most in need of intervention, but given the differences between subgroups of the population,screening tools have some limitations. That is, screening tools may be too sensitive (i.e., result in a false positive, indicatingsomeone may have a severe problem and need a clinical intervention when they may not) or not sensitive enough (i.e., result in a false negative, failing to identify those in need of clinical intervention). One screening tool for alcohol use that is commonly used by clinicians and interventionists worldwide is the Alcohol Use Disorders Identification Test (AUDIT).The AUDIT includes questions on frequency and quantity of drinking as well as drinking-related consequences, and has been used for youth and adults alike.
This study examined whether the amount and frequency of drinking were better at predicting drinking-related harms and consequences for each of these age groups.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis from a national sample of adults ages 14 and older who completed the 2016 Australian National Drug Strategy Household Survey.The survey is a national, cross-sectional survey that is conducted in Australia every 3 years. Respondents are asked a variety of questions about alcohol and drug use behaviors and attitudes. In 2016, the survey was administered to 23,772 Australian individuals; the sample of 22,642 participants used for this study were those who indicated that they were at least 18 years old and reported drinking at least some alcohol at some point in their life. In contrast to the US, where the legal drinking age is 21 years old, the legal drinking age in Australia is 18 years old.
The survey included some questions either taken directly from the AUDIT or used some very similar questions, to assess alcohol use patterns. The AUDIT is a standardized scale, used worldwide. It has 10 questions and results in a score from 0-40, where higher scores indicate greater alcohol use. It has two subscales that can be calculated in addition to the total score: harmful alcohol use (AUDIT questions 7-10 for a score of 0-12) and alcohol dependence (AUDIT questions 4-6 for a score of 0-12).
Figure 1. As mentioned in the above paragraph, the AUDIT scale contains two subscales that can be calculated in addition to the total score: Questions 7-10 for a subscale of harmful alcohol use; Questions 4-6 for a subscale of alcohol dependence.
In this analysis, the researchers used the frequency of alcohol consumption (drinking occasions per week) and amount of drinking (quantity) per typical drinking occasion to predict the AUDIT dependence score (from the AUDIT dependence subscale) and the AUDIT harmful drinking score (from the AUDIT harms subscale).Alcohol quantity was measured using a drink size of 10g of ethanol, which is a standard drink size in Australia (in the US, a standard drink size is 14g). Age was included as a categorical variable in incremental 5-year blocks so that gradual comparisons by age groupings could be examined.
Of the sample of 17,399 adults included in this analysis, just over half were female (53%) and the average age was 50 (SD = 17). Approximately 24% of the sample had a total AUDIT score of 8 or higher and so were indicated as needing intervention according to the AUDIT guidelines.
WHAT DID THIS STUDY FIND?
The ability of drinking frequency and quantity to predict alcohol-related harms differed by participant age.
For those aged 18-27, how often they drank alcohol (i.e., their frequency of alcohol consumption) was about twice as good a predictor of both dependence and harmful drinking AUDIT scores than the amount (i.e., quantity) consumed per drinking occasion. That is, although both the frequency and quantity items contributed to these overall scores, younger adults who indicated high frequency were more likely to be identified as needing intervention than younger adults who indicated high quantity of drinking per occasion.
In contrast, for participants aged 43 and older, the quantity consumed per drinking occasion was twice as good a predictor of dependence AUDIT scores than frequency of alcohol consumption. That is, although both the frequency and quantity items contribute to these overall scores, older adults who indicated a higher quantity of drinking per occasion were more likely to be identified as needing intervention than older adults who indicated higher frequency of drinking. This pattern was also similar among adults aged 43 or older for harmful drinking AUDIT scores, although not for those between 53-57 years old.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 17,399 adults found that, overall, younger adults typically drink less often, but more per occasion, than older adults. As such, it is actually the frequency with which young adults drink that more strongly predicts alcohol-related harms as measured by the AUDIT. In contrast, older adults showed the opposite pattern; they typically drink more often, but fewer drinks per drinking occasion. As such, it is the number of drinking per drinking occasion (i.e., “intensity”) that is the strongly predicts alcohol-related harms for this group.
While some individuals will develop chronic forms of alcohol use disorder, many who show heavy alcohol use patterns during emerging adulthood will “age out” as they assume greater responsibilities and meaningful activities that take up more of their free time. The researchers conducting this study suggest that in a limited time setting such as a clinic, focusing on screening for more frequent drinking may be very useful when working with younger adults for identifying a treatment need.It is possible that drinking frequency can more readily identify young people with drinking-related consequences who may need help to change their drinking. Alternatively, the authors suggest that the results for older adults indicate that screening for more heavy drinking may be more useful for this population when seeking to identify individuals who would benefit most from alcohol use disorder treatment.
That said, while this study helps to identify differences between the nature of alcohol use disorder in younger versus older adults, itis important to always assess for both quantity and frequency across all developmental life stages for two key reasons. One, screeners are intended to be brief and easy to administer. Adding more complex rules for interpretation depending on age range may make the AUDIT and other screeners like it unduly burdensome for healthcare professionals. Second, alcohol screeners are useful beyond their ability to identify individuals who meet the clinical threshold of alcohol use disorder. Specifically, alcohol-related hazards (i.e., injuries) and harms (i.e., toxicity effects such as cancer and liver disease) result simply from alcohol consumption, both in terms of how often someone drinks and how much they consume on each drinking occasion.
Another aspect of what the researchers may be capturing here is the development of alcohol use disorder across the lifespan. That is, as alcohol use disorder/dependency develops, the frequency of alcohol use is paramount; once alcohol dependency is developed, maintaining it requires more intensive use (e.g., as tolerance develops and neuroadaptation occurs). In other words, on average, in the development of alcohol use disorder, early adulthood is the time when the habitual patterns of the behavior often become ingrained that begins the process of dependence; then once acquired, the brain needs more alcohol to get the same effect over time as one ages.
In sum, brief and accurate screening tools are highly scalable resources with the potential for public health impact, yet their use might possibly be enhanced by tailoring them to specific patient characteristics, such as developmental stage as this study suggests. It should be remembered that given their broad and general approach to identifying drinking harms, screening tools like the AUDIT are best viewed as opportunities to begin a conversation about risky health behaviors, consequences, and readiness for change.
The study did not examine other characteristics that could influence how drinking behavior patterns might be more prone to harmful drinking/dependence (e.g., gender, sexual orientation, minoritized status, and mental health comorbidities). Further exploration of these characteristics and potential interactions between them would help to further understand the need to tailor screening tools for different populations.
This study only focused on a single screening tool, the AUDIT, and cannot speak to the ability of other screening tools to be specific and sensitive enough for the population of interest.
BOTTOM LINE
The researchers found that using the AUDIT screening tool, the frequency of alcohol consumption was a better predictor of alcohol-related consequences in younger adults but more drinks per occasion was a stronger predictor of consequences in older adults. While this finding may suggest greater utility of age-specific interpretations of this screener, clinical screening tools are more likely to be adopted and implemented when they are easy to use, score, and interpret. Adding complexity by introducing different scoring that caters to different subgroups may result in less actual real-world use. It is also may be that these findings reflect how alcohol use disorder changes over the lifespan. Given that the hazards (e.g., injuries) and harms (e.g., liver toxicity) of alcohol use generally result simply from alcohol consumption, keeping the threshold lower to identify as many cases of risky drinking as possible, at the expense of more false positives, will aid with detection of most/all of the actual harmful use cases of alcohol use, regardless of age, thereby more efficiently addressing the public health burden of alcohol.
For individuals and families seeking recovery: Drinking less alcohol and/or drinking less frequentlycan result in improved health and well-being. Although it can be difficult at times to understand whether someone’s drinking behaviors warrants treatment, it is important to have conversations with your loved ones if you are concerned and to support them to speak with a provider. This study demonstrates that especially for younger adults, noticing more frequent drinking could be a sign of alcohol use disorder, while for older adults, noticing heavy drinking during single occasions could be a sign for intervention.
For treatment professionals and treatment systems: The ability to screen and intervene on problematic alcohol use in primary care and other medical settings can help improve the health and well-being of individuals who exhibit these alcohol use patterns and also reduce alcohol’s broader public health burden. Although short screening tools such as the AUDIT are useful for identifying levels of alcohol use that may need intervention, it is important to carefully implement these tools in clinical practice. These tools can be a helpful starting point for discussion, but treatment professionals should also consider the target population of focus (i.e., patient-centered care) and whether certain drinking patterns may be more likely to indicate need for swift or more intensive intervention than what the current scoring algorithms of these tools currently suggest.
For scientists:This study highlights a potential need to closely examine how drinking behavior patterns in different population subgroups may drive certain screening tool scores, and whether the sensitivity of those tools to indicate care is compromised. Although much work has been done on the factorial invariance of screening tools like the AUDIT, more fine-grained analyses with larger samples might reveal nuances that have clinical significance. That said, increasing these tools’ universal sensitivity (e.g., lowering the overall screening threshold score that triggers further assessment) may be one approach to investigate to accurately detect the whole range and variety of different patterns of alcohol use that are associated with health harms irrespective of the different characteristics of individuals in the population who could benefit from care, unless differences are very large between sub-groups. Given simplicity in administration, scoring, and interpretation is key in tool adoption in clinical practice, a single change in scoring is likely to result higher adoption than having multiple scoring algorithms or different screening tools for different population subgroups.
For policy makers: Screening for problematic alcohol use in primary care and other medical settings can help to improve public health. Supporting research that addresses how to best tailor alcohol screening tools and providing funding for clinical initiatives to improve existing approaches so as not to miss important at-risk population subgroups could have potential to further enhance public health in more effective and cost-efficient ways.
Alcohol use patterns can vary widely across the life span. That is, at a population level, as individuals age, they tend to drink alcohol more often (i.e., increasein their drinking frequency), but also tend to consume fewerdrinks per occasion (i.e., reduce their quantity of drinking at a single event). Although merely consuming alcohol can result in harmful health consequences, some individuals may be at particularly increased risk for developing an alcohol use disorder – that is continued drinking despite significant levels of alcohol-related functional impairment and distress, increasing the risk for disease, disability, and premature death.
Screening tools can help identify individuals most in need of intervention, but given the differences between subgroups of the population,screening tools have some limitations. That is, screening tools may be too sensitive (i.e., result in a false positive, indicatingsomeone may have a severe problem and need a clinical intervention when they may not) or not sensitive enough (i.e., result in a false negative, failing to identify those in need of clinical intervention). One screening tool for alcohol use that is commonly used by clinicians and interventionists worldwide is the Alcohol Use Disorders Identification Test (AUDIT).The AUDIT includes questions on frequency and quantity of drinking as well as drinking-related consequences, and has been used for youth and adults alike.
This study examined whether the amount and frequency of drinking were better at predicting drinking-related harms and consequences for each of these age groups.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis from a national sample of adults ages 14 and older who completed the 2016 Australian National Drug Strategy Household Survey.The survey is a national, cross-sectional survey that is conducted in Australia every 3 years. Respondents are asked a variety of questions about alcohol and drug use behaviors and attitudes. In 2016, the survey was administered to 23,772 Australian individuals; the sample of 22,642 participants used for this study were those who indicated that they were at least 18 years old and reported drinking at least some alcohol at some point in their life. In contrast to the US, where the legal drinking age is 21 years old, the legal drinking age in Australia is 18 years old.
The survey included some questions either taken directly from the AUDIT or used some very similar questions, to assess alcohol use patterns. The AUDIT is a standardized scale, used worldwide. It has 10 questions and results in a score from 0-40, where higher scores indicate greater alcohol use. It has two subscales that can be calculated in addition to the total score: harmful alcohol use (AUDIT questions 7-10 for a score of 0-12) and alcohol dependence (AUDIT questions 4-6 for a score of 0-12).
Figure 1. As mentioned in the above paragraph, the AUDIT scale contains two subscales that can be calculated in addition to the total score: Questions 7-10 for a subscale of harmful alcohol use; Questions 4-6 for a subscale of alcohol dependence.
In this analysis, the researchers used the frequency of alcohol consumption (drinking occasions per week) and amount of drinking (quantity) per typical drinking occasion to predict the AUDIT dependence score (from the AUDIT dependence subscale) and the AUDIT harmful drinking score (from the AUDIT harms subscale).Alcohol quantity was measured using a drink size of 10g of ethanol, which is a standard drink size in Australia (in the US, a standard drink size is 14g). Age was included as a categorical variable in incremental 5-year blocks so that gradual comparisons by age groupings could be examined.
Of the sample of 17,399 adults included in this analysis, just over half were female (53%) and the average age was 50 (SD = 17). Approximately 24% of the sample had a total AUDIT score of 8 or higher and so were indicated as needing intervention according to the AUDIT guidelines.
WHAT DID THIS STUDY FIND?
The ability of drinking frequency and quantity to predict alcohol-related harms differed by participant age.
For those aged 18-27, how often they drank alcohol (i.e., their frequency of alcohol consumption) was about twice as good a predictor of both dependence and harmful drinking AUDIT scores than the amount (i.e., quantity) consumed per drinking occasion. That is, although both the frequency and quantity items contributed to these overall scores, younger adults who indicated high frequency were more likely to be identified as needing intervention than younger adults who indicated high quantity of drinking per occasion.
In contrast, for participants aged 43 and older, the quantity consumed per drinking occasion was twice as good a predictor of dependence AUDIT scores than frequency of alcohol consumption. That is, although both the frequency and quantity items contribute to these overall scores, older adults who indicated a higher quantity of drinking per occasion were more likely to be identified as needing intervention than older adults who indicated higher frequency of drinking. This pattern was also similar among adults aged 43 or older for harmful drinking AUDIT scores, although not for those between 53-57 years old.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 17,399 adults found that, overall, younger adults typically drink less often, but more per occasion, than older adults. As such, it is actually the frequency with which young adults drink that more strongly predicts alcohol-related harms as measured by the AUDIT. In contrast, older adults showed the opposite pattern; they typically drink more often, but fewer drinks per drinking occasion. As such, it is the number of drinking per drinking occasion (i.e., “intensity”) that is the strongly predicts alcohol-related harms for this group.
While some individuals will develop chronic forms of alcohol use disorder, many who show heavy alcohol use patterns during emerging adulthood will “age out” as they assume greater responsibilities and meaningful activities that take up more of their free time. The researchers conducting this study suggest that in a limited time setting such as a clinic, focusing on screening for more frequent drinking may be very useful when working with younger adults for identifying a treatment need.It is possible that drinking frequency can more readily identify young people with drinking-related consequences who may need help to change their drinking. Alternatively, the authors suggest that the results for older adults indicate that screening for more heavy drinking may be more useful for this population when seeking to identify individuals who would benefit most from alcohol use disorder treatment.
That said, while this study helps to identify differences between the nature of alcohol use disorder in younger versus older adults, itis important to always assess for both quantity and frequency across all developmental life stages for two key reasons. One, screeners are intended to be brief and easy to administer. Adding more complex rules for interpretation depending on age range may make the AUDIT and other screeners like it unduly burdensome for healthcare professionals. Second, alcohol screeners are useful beyond their ability to identify individuals who meet the clinical threshold of alcohol use disorder. Specifically, alcohol-related hazards (i.e., injuries) and harms (i.e., toxicity effects such as cancer and liver disease) result simply from alcohol consumption, both in terms of how often someone drinks and how much they consume on each drinking occasion.
Another aspect of what the researchers may be capturing here is the development of alcohol use disorder across the lifespan. That is, as alcohol use disorder/dependency develops, the frequency of alcohol use is paramount; once alcohol dependency is developed, maintaining it requires more intensive use (e.g., as tolerance develops and neuroadaptation occurs). In other words, on average, in the development of alcohol use disorder, early adulthood is the time when the habitual patterns of the behavior often become ingrained that begins the process of dependence; then once acquired, the brain needs more alcohol to get the same effect over time as one ages.
In sum, brief and accurate screening tools are highly scalable resources with the potential for public health impact, yet their use might possibly be enhanced by tailoring them to specific patient characteristics, such as developmental stage as this study suggests. It should be remembered that given their broad and general approach to identifying drinking harms, screening tools like the AUDIT are best viewed as opportunities to begin a conversation about risky health behaviors, consequences, and readiness for change.
The study did not examine other characteristics that could influence how drinking behavior patterns might be more prone to harmful drinking/dependence (e.g., gender, sexual orientation, minoritized status, and mental health comorbidities). Further exploration of these characteristics and potential interactions between them would help to further understand the need to tailor screening tools for different populations.
This study only focused on a single screening tool, the AUDIT, and cannot speak to the ability of other screening tools to be specific and sensitive enough for the population of interest.
BOTTOM LINE
The researchers found that using the AUDIT screening tool, the frequency of alcohol consumption was a better predictor of alcohol-related consequences in younger adults but more drinks per occasion was a stronger predictor of consequences in older adults. While this finding may suggest greater utility of age-specific interpretations of this screener, clinical screening tools are more likely to be adopted and implemented when they are easy to use, score, and interpret. Adding complexity by introducing different scoring that caters to different subgroups may result in less actual real-world use. It is also may be that these findings reflect how alcohol use disorder changes over the lifespan. Given that the hazards (e.g., injuries) and harms (e.g., liver toxicity) of alcohol use generally result simply from alcohol consumption, keeping the threshold lower to identify as many cases of risky drinking as possible, at the expense of more false positives, will aid with detection of most/all of the actual harmful use cases of alcohol use, regardless of age, thereby more efficiently addressing the public health burden of alcohol.
For individuals and families seeking recovery: Drinking less alcohol and/or drinking less frequentlycan result in improved health and well-being. Although it can be difficult at times to understand whether someone’s drinking behaviors warrants treatment, it is important to have conversations with your loved ones if you are concerned and to support them to speak with a provider. This study demonstrates that especially for younger adults, noticing more frequent drinking could be a sign of alcohol use disorder, while for older adults, noticing heavy drinking during single occasions could be a sign for intervention.
For treatment professionals and treatment systems: The ability to screen and intervene on problematic alcohol use in primary care and other medical settings can help improve the health and well-being of individuals who exhibit these alcohol use patterns and also reduce alcohol’s broader public health burden. Although short screening tools such as the AUDIT are useful for identifying levels of alcohol use that may need intervention, it is important to carefully implement these tools in clinical practice. These tools can be a helpful starting point for discussion, but treatment professionals should also consider the target population of focus (i.e., patient-centered care) and whether certain drinking patterns may be more likely to indicate need for swift or more intensive intervention than what the current scoring algorithms of these tools currently suggest.
For scientists:This study highlights a potential need to closely examine how drinking behavior patterns in different population subgroups may drive certain screening tool scores, and whether the sensitivity of those tools to indicate care is compromised. Although much work has been done on the factorial invariance of screening tools like the AUDIT, more fine-grained analyses with larger samples might reveal nuances that have clinical significance. That said, increasing these tools’ universal sensitivity (e.g., lowering the overall screening threshold score that triggers further assessment) may be one approach to investigate to accurately detect the whole range and variety of different patterns of alcohol use that are associated with health harms irrespective of the different characteristics of individuals in the population who could benefit from care, unless differences are very large between sub-groups. Given simplicity in administration, scoring, and interpretation is key in tool adoption in clinical practice, a single change in scoring is likely to result higher adoption than having multiple scoring algorithms or different screening tools for different population subgroups.
For policy makers: Screening for problematic alcohol use in primary care and other medical settings can help to improve public health. Supporting research that addresses how to best tailor alcohol screening tools and providing funding for clinical initiatives to improve existing approaches so as not to miss important at-risk population subgroups could have potential to further enhance public health in more effective and cost-efficient ways.