No protection against mortality with low or moderate alcohol use, mortality risk increases at higher levels
Research has suggested cardio-protective effects of low or moderate alcohol use, yet such results may be accounted for not by alcohol itself but by factors associated with alcohol use. Given the health care, criminal justice, and financial burden of alcohol in society, researchers in this study sought to conduct a scientifically rigorous and more fine grained review of the evidence.
Because systematic reviews and meta-analyses summarize a large amount of information, they often are considered the “best evidence” for answering a particular research question and are at the top of the evidence hierarchy. However, if the studies that are included have design features that call into question whether the primary variable of interest (e.g., alcohol use) is actually causing the outcome – sometimes referred to as a study “bias” – then their results will also be biased. There is a growing amount of research suggesting that many of the studies included in the systematic reviews and meta-analyses suggesting that moderate alcohol use is associated with decreased mortality risk contain biases. In other words, the presumed positive health effect of alcohol may not actually be real (i.e., a “spurious” effect).
Some of these biases involve the finding that people who drink lightly or moderately tend to be healthier overall (e.g., due to factors other than drinking like exercise, social involvement, consistent health care engagement, etc.) than people who are currently abstaining from alcohol and that people who have abstained throughout their lives may have poorer health than those who have not. Also, some studies have not removed people who may have quit drinking due to the negative health effects from alcohol, which would classify them as abstaining but not account for the health problems from their prior alcohol use that increases mortality risk. By examining cohorts of individuals from younger ages, researchers are able to include individuals who later became abstainers due to health difficulties (thereby skewing the data in favor of those who drink lightly) in their appropriate former drinker category rather than classifying them as abstainers. Finally, many studies have used samples that overrepresent White men. When adjusted to be more representative of the general population, the results showing protective associations from moderate alcohol use no longer are present. All of these biases may influence the studies’ results and call into question whether moderate drinking can really decrease mortality risk.
The current study updates these prior reviews. It also examines whether the effects of alcohol use on mortality differs by sex, and whether studies that followed initially younger cohorts over longer periods of time did not find an association between moderate drinking and mortality as they hypothesized.
HOW WAS THIS STUDY CONDUCTED?
The research team updated a previously conducted systematic review and meta-analysis by adding an additional 20 studies, resulting in a total of 107 studies. These studies examined the relationship between mortality from any cause (i.e., all-cause mortality) and alcohol use and were published between January 1980 and July 2021.
Studies were identified by searching the electronic databases PUBMED and Web of Science. To be included in the analysis, studies must: (1) be published in English; (2) be an original research manuscript that was published in a peer-reviewed journal and examine the relationship between all-cause mortality and at least 3 categories of alcohol use in humans; (3) be a retrospective or prospective cohort study (i.e., a study that follows a group of people who share a common characteristic over time); and (4) include people who drank alcohol. Studies could include people of all genders, ages, races, ethnicities, and religions from any location. Studies were excluded if the design was anything other than original research (e.g., editorials, dissertations, book chapters, etc. were excluded), if participants were selected due to having an illness or an alcohol use disorder, or if participants were from the general population but included those who had coronary heart disease or other related conditions.
After identification of the studies that met these criteria, three members of the research team extracted and coded relevant data from them. These data included risk statistics of all-cause mortality from alcohol use, measures of alcohol use (converted into grams of alcohol per day based on country-specific definitions of a standard drink; e.g., a standard drink in the US contains 14 grams of pure alcohol whereas in the UK a standard drink contains 10 grams of alcohol), study characteristics (e.g., age and sex of participants), types of errors involving misclassification of people who drink alcohol or abstain (e.g., categorizing people who drink occasionally or formerly drank alcohol as people who abstain), and variables that were statistically controlled to isolate the association of alcohol use and mortality.
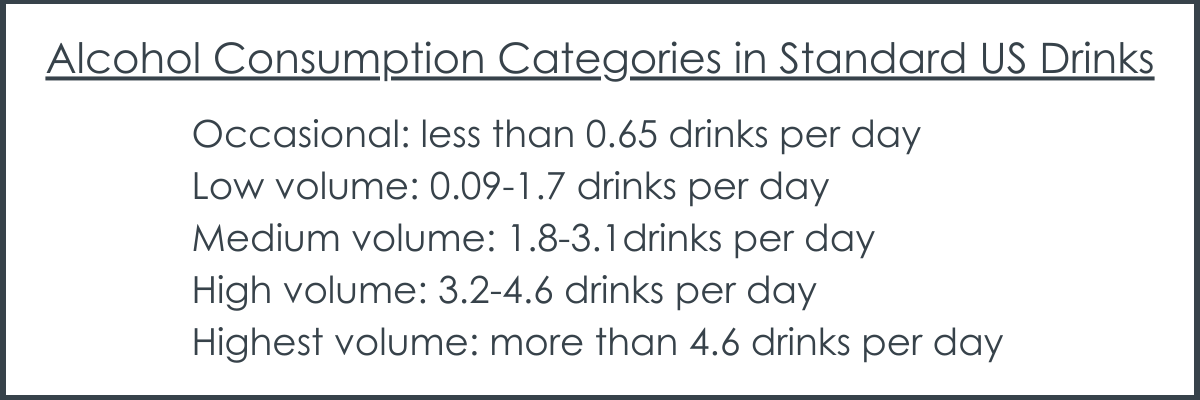
The main outcome of interest was “all-cause mortality” (death by any cause). The predictor variable was the mean daily alcohol intake (grams of alcohol per day), categorized into occasional (less than 9.1 grams per day), low volume (1.3-24.0 grams per day), medium volume (25.0-44.0 grams per day), high volume (45.0-64.0 grams per day), and highest volume (more than 65.0 grams per day) drinking, as well as former drinkers who are now completely abstaining. Publication bias, heterogeneity, and potential confounding variables such as smoking status, socioeconomic status, race, diet, exercise, and body-mass index were also assessed.
Analyses compared the alcohol categories to a category of people who have abstained from alcohol throughout their lives to estimate the risk of all-cause mortality from alcohol use. The researchers ran these analyses together and then stratified by the cohort’s median age (younger or older than age 56) and sex (men vs. women).
4.8 million people between the ages of 19 and 78 from across all studies that were included in the meta-analysis. Of the 107 studies, 67 included participants between the ages of 19 and 55 and 46 included participants between the ages of 56 and 78 (studies could cover both age ranges). Seventy-three studies included men only, 48 included women only, and 31 included men and women.
WHAT DID THIS STUDY FIND?
There were no protective effects of alcohol use at lower levels and increased mortality risk present at higher levels
In the fully adjusted models, there was no association of all-cause mortality among people who drank medium volume amounts (25 to 44 g per day) or less when compared to people who consumed alcohol occasionally or never drank alcohol throughout their lives (i.e., no protective effects were observed with moderate alcohol use or less). However, there was a significantly increased risk for people who drank at the high (45 to 64 grams per day) and highest (65 or more grams per day) amounts when compared with lifetime nondrinkers and occasional drinkers.
In models adjusting for potential confounding effects of other variables such as sampling variation, former drinker bias, and other study-level criteria, there was not a reduced risk of all-cause mortality among those who consumed alcohol occasionally or at low-volume amounts compared with lifetime nondrinkers.
Greater mortality risks for those who are younger and for women
In the models that did not adjust for other variables or only partially adjusted for them, older cohorts showed greater decreases in mortality risk with low-volume consumption than younger cohorts. However, in the models that were fully adjusted, there were no differences between the younger and older cohorts with low-volume use. Also in the fully adjusted models, younger cohorts showed greater increases in mortality risk than older cohorts with higher volume consumption.
In the fully adjusted models, there were significantly greater risks of mortality among women who drank alcohol compared with women who never drank alcohol. Increased risks for women were observed at lower levels of alcohol use than men. Among men, increased risks of mortality were observed with high volume (45-64 grams) and higher volume (more than 65 grams) consumption, while for women, increased risks were observed with medium volume (25-45 grams) and greater.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team updated a previously conducted systematic review and meta-analysis to examine the association between alcohol use and mortality risk and to understand how age, sex, and sources of bias may affect the results. In the full sample, the researchers did not find any evidence for protective effects from moderate or less alcohol use and there was an increased risk of mortality with high levels of alcohol use and more. Adjusting the analysis to control for different sources of bias did not influence these results, but the results did vary by age and sex, with greater mortality risks observed in those who are younger and for women.
These findings do not support the notion that drinking moderately or less may have health benefits and promote longevity, which is consistent with the results of their prior meta-analysis. This is important for medical professionals who may have begun mistakenly recommending to their patients that drinking 1-2 glasses of wine each night may promote good health. Instead, it seems that people who do not currently drink alcohol should not start doing so for health benefits.
In many of the studies, alcohol use was only assessed at one time point. This limits the extent to which the researchers can understand how changes in alcohol use over time affect mortality risk.
Participants self-reported their alcohol use, which is prone to under-reporting. Participants may have also inaccurately reported that they have abstained from alcohol throughout their lives, but actually formerly consumed alcohol.
There was a limited number of studies that controlled for how binge drinking episodes (e.g., a measure of alcohol consumption during a concrete period of time like 2 hours) affect mortality risk. Although participants’ mean daily alcohol use may have been low, their overall alcohol use was not.
BOTTOM LINE
This updated review and meta-analysis found that low to moderate alcohol use was not associated with a decreased risk of mortality, but that high amounts of alcohol use were associated with an increased risk of mortality.
For individuals and families seeking recovery: Because this study did not support the notion that moderate or less alcohol use was associated with a decreased risk of mortality, it is not recommended that individuals begin drinking for health benefits or longevity if they do not already do so. Among individuals who choose to drink alcohol, this study is consistent with the current guidelines that men should limit their alcohol use to 2 drinks per day or less, and women 1 drink per day (i.e., moderate drinking). Note however, that certain risks of alcohol use, like breast cancer in women, are present even at these lower levels and many countries now have already begun moving toward recommending no or very low levels of alcohol use in order to optimize your health.
For treatment professionals and treatment systems: This study did not support the notion that moderate alcohol use or less was associated with a decreased risk of mortality. Accordingly, health professionals are cautioned against recommending moderate drinking for health benefits. Further, health professionals who inform their patients of the health and mortality risks associated with high levels of alcohol use may reduce their mortality risks.
For scientists: Because many of the studies included in the meta-analysis assessed alcohol at one time point only, future research that includes additional time points would shed light on how changes in alcohol use over time influence mortality risk. Also, using methods other than self-report to assess alcohol use, such as new wearable technology or biosensors, may allow researchers to avoid the self-report bias often seen in these studies. Finally, future research that more closely examines how binge drinking affects mortality risk would provide an understanding of how different patterns of drinking influence health outcomes.
For policy makers: This study demonstrated that moderate alcohol use is not associated with decreased risk of mortality, but that drinking higher volumes of alcohol is associated with an increased mortality risk. Public health campaigns that promote the health risks of alcohol may help to inform the public and reduce their mortality risks from alcohol. Additionally, policies that limit access to alcohol (e.g., taxation, limits on the number of alcohol outlets in a given location, etc.) may further help to reduce how much alcohol people consume and improve overall public health.
Because systematic reviews and meta-analyses summarize a large amount of information, they often are considered the “best evidence” for answering a particular research question and are at the top of the evidence hierarchy. However, if the studies that are included have design features that call into question whether the primary variable of interest (e.g., alcohol use) is actually causing the outcome – sometimes referred to as a study “bias” – then their results will also be biased. There is a growing amount of research suggesting that many of the studies included in the systematic reviews and meta-analyses suggesting that moderate alcohol use is associated with decreased mortality risk contain biases. In other words, the presumed positive health effect of alcohol may not actually be real (i.e., a “spurious” effect).
Some of these biases involve the finding that people who drink lightly or moderately tend to be healthier overall (e.g., due to factors other than drinking like exercise, social involvement, consistent health care engagement, etc.) than people who are currently abstaining from alcohol and that people who have abstained throughout their lives may have poorer health than those who have not. Also, some studies have not removed people who may have quit drinking due to the negative health effects from alcohol, which would classify them as abstaining but not account for the health problems from their prior alcohol use that increases mortality risk. By examining cohorts of individuals from younger ages, researchers are able to include individuals who later became abstainers due to health difficulties (thereby skewing the data in favor of those who drink lightly) in their appropriate former drinker category rather than classifying them as abstainers. Finally, many studies have used samples that overrepresent White men. When adjusted to be more representative of the general population, the results showing protective associations from moderate alcohol use no longer are present. All of these biases may influence the studies’ results and call into question whether moderate drinking can really decrease mortality risk.
The current study updates these prior reviews. It also examines whether the effects of alcohol use on mortality differs by sex, and whether studies that followed initially younger cohorts over longer periods of time did not find an association between moderate drinking and mortality as they hypothesized.
HOW WAS THIS STUDY CONDUCTED?
The research team updated a previously conducted systematic review and meta-analysis by adding an additional 20 studies, resulting in a total of 107 studies. These studies examined the relationship between mortality from any cause (i.e., all-cause mortality) and alcohol use and were published between January 1980 and July 2021.
Studies were identified by searching the electronic databases PUBMED and Web of Science. To be included in the analysis, studies must: (1) be published in English; (2) be an original research manuscript that was published in a peer-reviewed journal and examine the relationship between all-cause mortality and at least 3 categories of alcohol use in humans; (3) be a retrospective or prospective cohort study (i.e., a study that follows a group of people who share a common characteristic over time); and (4) include people who drank alcohol. Studies could include people of all genders, ages, races, ethnicities, and religions from any location. Studies were excluded if the design was anything other than original research (e.g., editorials, dissertations, book chapters, etc. were excluded), if participants were selected due to having an illness or an alcohol use disorder, or if participants were from the general population but included those who had coronary heart disease or other related conditions.
After identification of the studies that met these criteria, three members of the research team extracted and coded relevant data from them. These data included risk statistics of all-cause mortality from alcohol use, measures of alcohol use (converted into grams of alcohol per day based on country-specific definitions of a standard drink; e.g., a standard drink in the US contains 14 grams of pure alcohol whereas in the UK a standard drink contains 10 grams of alcohol), study characteristics (e.g., age and sex of participants), types of errors involving misclassification of people who drink alcohol or abstain (e.g., categorizing people who drink occasionally or formerly drank alcohol as people who abstain), and variables that were statistically controlled to isolate the association of alcohol use and mortality.
The main outcome of interest was “all-cause mortality” (death by any cause). The predictor variable was the mean daily alcohol intake (grams of alcohol per day), categorized into occasional (less than 9.1 grams per day), low volume (1.3-24.0 grams per day), medium volume (25.0-44.0 grams per day), high volume (45.0-64.0 grams per day), and highest volume (more than 65.0 grams per day) drinking, as well as former drinkers who are now completely abstaining. Publication bias, heterogeneity, and potential confounding variables such as smoking status, socioeconomic status, race, diet, exercise, and body-mass index were also assessed.
Analyses compared the alcohol categories to a category of people who have abstained from alcohol throughout their lives to estimate the risk of all-cause mortality from alcohol use. The researchers ran these analyses together and then stratified by the cohort’s median age (younger or older than age 56) and sex (men vs. women).
4.8 million people between the ages of 19 and 78 from across all studies that were included in the meta-analysis. Of the 107 studies, 67 included participants between the ages of 19 and 55 and 46 included participants between the ages of 56 and 78 (studies could cover both age ranges). Seventy-three studies included men only, 48 included women only, and 31 included men and women.
WHAT DID THIS STUDY FIND?
There were no protective effects of alcohol use at lower levels and increased mortality risk present at higher levels
In the fully adjusted models, there was no association of all-cause mortality among people who drank medium volume amounts (25 to 44 g per day) or less when compared to people who consumed alcohol occasionally or never drank alcohol throughout their lives (i.e., no protective effects were observed with moderate alcohol use or less). However, there was a significantly increased risk for people who drank at the high (45 to 64 grams per day) and highest (65 or more grams per day) amounts when compared with lifetime nondrinkers and occasional drinkers.
In models adjusting for potential confounding effects of other variables such as sampling variation, former drinker bias, and other study-level criteria, there was not a reduced risk of all-cause mortality among those who consumed alcohol occasionally or at low-volume amounts compared with lifetime nondrinkers.
Greater mortality risks for those who are younger and for women
In the models that did not adjust for other variables or only partially adjusted for them, older cohorts showed greater decreases in mortality risk with low-volume consumption than younger cohorts. However, in the models that were fully adjusted, there were no differences between the younger and older cohorts with low-volume use. Also in the fully adjusted models, younger cohorts showed greater increases in mortality risk than older cohorts with higher volume consumption.
In the fully adjusted models, there were significantly greater risks of mortality among women who drank alcohol compared with women who never drank alcohol. Increased risks for women were observed at lower levels of alcohol use than men. Among men, increased risks of mortality were observed with high volume (45-64 grams) and higher volume (more than 65 grams) consumption, while for women, increased risks were observed with medium volume (25-45 grams) and greater.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team updated a previously conducted systematic review and meta-analysis to examine the association between alcohol use and mortality risk and to understand how age, sex, and sources of bias may affect the results. In the full sample, the researchers did not find any evidence for protective effects from moderate or less alcohol use and there was an increased risk of mortality with high levels of alcohol use and more. Adjusting the analysis to control for different sources of bias did not influence these results, but the results did vary by age and sex, with greater mortality risks observed in those who are younger and for women.
These findings do not support the notion that drinking moderately or less may have health benefits and promote longevity, which is consistent with the results of their prior meta-analysis. This is important for medical professionals who may have begun mistakenly recommending to their patients that drinking 1-2 glasses of wine each night may promote good health. Instead, it seems that people who do not currently drink alcohol should not start doing so for health benefits.
In many of the studies, alcohol use was only assessed at one time point. This limits the extent to which the researchers can understand how changes in alcohol use over time affect mortality risk.
Participants self-reported their alcohol use, which is prone to under-reporting. Participants may have also inaccurately reported that they have abstained from alcohol throughout their lives, but actually formerly consumed alcohol.
There was a limited number of studies that controlled for how binge drinking episodes (e.g., a measure of alcohol consumption during a concrete period of time like 2 hours) affect mortality risk. Although participants’ mean daily alcohol use may have been low, their overall alcohol use was not.
BOTTOM LINE
This updated review and meta-analysis found that low to moderate alcohol use was not associated with a decreased risk of mortality, but that high amounts of alcohol use were associated with an increased risk of mortality.
For individuals and families seeking recovery: Because this study did not support the notion that moderate or less alcohol use was associated with a decreased risk of mortality, it is not recommended that individuals begin drinking for health benefits or longevity if they do not already do so. Among individuals who choose to drink alcohol, this study is consistent with the current guidelines that men should limit their alcohol use to 2 drinks per day or less, and women 1 drink per day (i.e., moderate drinking). Note however, that certain risks of alcohol use, like breast cancer in women, are present even at these lower levels and many countries now have already begun moving toward recommending no or very low levels of alcohol use in order to optimize your health.
For treatment professionals and treatment systems: This study did not support the notion that moderate alcohol use or less was associated with a decreased risk of mortality. Accordingly, health professionals are cautioned against recommending moderate drinking for health benefits. Further, health professionals who inform their patients of the health and mortality risks associated with high levels of alcohol use may reduce their mortality risks.
For scientists: Because many of the studies included in the meta-analysis assessed alcohol at one time point only, future research that includes additional time points would shed light on how changes in alcohol use over time influence mortality risk. Also, using methods other than self-report to assess alcohol use, such as new wearable technology or biosensors, may allow researchers to avoid the self-report bias often seen in these studies. Finally, future research that more closely examines how binge drinking affects mortality risk would provide an understanding of how different patterns of drinking influence health outcomes.
For policy makers: This study demonstrated that moderate alcohol use is not associated with decreased risk of mortality, but that drinking higher volumes of alcohol is associated with an increased mortality risk. Public health campaigns that promote the health risks of alcohol may help to inform the public and reduce their mortality risks from alcohol. Additionally, policies that limit access to alcohol (e.g., taxation, limits on the number of alcohol outlets in a given location, etc.) may further help to reduce how much alcohol people consume and improve overall public health.
Because systematic reviews and meta-analyses summarize a large amount of information, they often are considered the “best evidence” for answering a particular research question and are at the top of the evidence hierarchy. However, if the studies that are included have design features that call into question whether the primary variable of interest (e.g., alcohol use) is actually causing the outcome – sometimes referred to as a study “bias” – then their results will also be biased. There is a growing amount of research suggesting that many of the studies included in the systematic reviews and meta-analyses suggesting that moderate alcohol use is associated with decreased mortality risk contain biases. In other words, the presumed positive health effect of alcohol may not actually be real (i.e., a “spurious” effect).
Some of these biases involve the finding that people who drink lightly or moderately tend to be healthier overall (e.g., due to factors other than drinking like exercise, social involvement, consistent health care engagement, etc.) than people who are currently abstaining from alcohol and that people who have abstained throughout their lives may have poorer health than those who have not. Also, some studies have not removed people who may have quit drinking due to the negative health effects from alcohol, which would classify them as abstaining but not account for the health problems from their prior alcohol use that increases mortality risk. By examining cohorts of individuals from younger ages, researchers are able to include individuals who later became abstainers due to health difficulties (thereby skewing the data in favor of those who drink lightly) in their appropriate former drinker category rather than classifying them as abstainers. Finally, many studies have used samples that overrepresent White men. When adjusted to be more representative of the general population, the results showing protective associations from moderate alcohol use no longer are present. All of these biases may influence the studies’ results and call into question whether moderate drinking can really decrease mortality risk.
The current study updates these prior reviews. It also examines whether the effects of alcohol use on mortality differs by sex, and whether studies that followed initially younger cohorts over longer periods of time did not find an association between moderate drinking and mortality as they hypothesized.
HOW WAS THIS STUDY CONDUCTED?
The research team updated a previously conducted systematic review and meta-analysis by adding an additional 20 studies, resulting in a total of 107 studies. These studies examined the relationship between mortality from any cause (i.e., all-cause mortality) and alcohol use and were published between January 1980 and July 2021.
Studies were identified by searching the electronic databases PUBMED and Web of Science. To be included in the analysis, studies must: (1) be published in English; (2) be an original research manuscript that was published in a peer-reviewed journal and examine the relationship between all-cause mortality and at least 3 categories of alcohol use in humans; (3) be a retrospective or prospective cohort study (i.e., a study that follows a group of people who share a common characteristic over time); and (4) include people who drank alcohol. Studies could include people of all genders, ages, races, ethnicities, and religions from any location. Studies were excluded if the design was anything other than original research (e.g., editorials, dissertations, book chapters, etc. were excluded), if participants were selected due to having an illness or an alcohol use disorder, or if participants were from the general population but included those who had coronary heart disease or other related conditions.
After identification of the studies that met these criteria, three members of the research team extracted and coded relevant data from them. These data included risk statistics of all-cause mortality from alcohol use, measures of alcohol use (converted into grams of alcohol per day based on country-specific definitions of a standard drink; e.g., a standard drink in the US contains 14 grams of pure alcohol whereas in the UK a standard drink contains 10 grams of alcohol), study characteristics (e.g., age and sex of participants), types of errors involving misclassification of people who drink alcohol or abstain (e.g., categorizing people who drink occasionally or formerly drank alcohol as people who abstain), and variables that were statistically controlled to isolate the association of alcohol use and mortality.
The main outcome of interest was “all-cause mortality” (death by any cause). The predictor variable was the mean daily alcohol intake (grams of alcohol per day), categorized into occasional (less than 9.1 grams per day), low volume (1.3-24.0 grams per day), medium volume (25.0-44.0 grams per day), high volume (45.0-64.0 grams per day), and highest volume (more than 65.0 grams per day) drinking, as well as former drinkers who are now completely abstaining. Publication bias, heterogeneity, and potential confounding variables such as smoking status, socioeconomic status, race, diet, exercise, and body-mass index were also assessed.
Analyses compared the alcohol categories to a category of people who have abstained from alcohol throughout their lives to estimate the risk of all-cause mortality from alcohol use. The researchers ran these analyses together and then stratified by the cohort’s median age (younger or older than age 56) and sex (men vs. women).
4.8 million people between the ages of 19 and 78 from across all studies that were included in the meta-analysis. Of the 107 studies, 67 included participants between the ages of 19 and 55 and 46 included participants between the ages of 56 and 78 (studies could cover both age ranges). Seventy-three studies included men only, 48 included women only, and 31 included men and women.
WHAT DID THIS STUDY FIND?
There were no protective effects of alcohol use at lower levels and increased mortality risk present at higher levels
In the fully adjusted models, there was no association of all-cause mortality among people who drank medium volume amounts (25 to 44 g per day) or less when compared to people who consumed alcohol occasionally or never drank alcohol throughout their lives (i.e., no protective effects were observed with moderate alcohol use or less). However, there was a significantly increased risk for people who drank at the high (45 to 64 grams per day) and highest (65 or more grams per day) amounts when compared with lifetime nondrinkers and occasional drinkers.
In models adjusting for potential confounding effects of other variables such as sampling variation, former drinker bias, and other study-level criteria, there was not a reduced risk of all-cause mortality among those who consumed alcohol occasionally or at low-volume amounts compared with lifetime nondrinkers.
Greater mortality risks for those who are younger and for women
In the models that did not adjust for other variables or only partially adjusted for them, older cohorts showed greater decreases in mortality risk with low-volume consumption than younger cohorts. However, in the models that were fully adjusted, there were no differences between the younger and older cohorts with low-volume use. Also in the fully adjusted models, younger cohorts showed greater increases in mortality risk than older cohorts with higher volume consumption.
In the fully adjusted models, there were significantly greater risks of mortality among women who drank alcohol compared with women who never drank alcohol. Increased risks for women were observed at lower levels of alcohol use than men. Among men, increased risks of mortality were observed with high volume (45-64 grams) and higher volume (more than 65 grams) consumption, while for women, increased risks were observed with medium volume (25-45 grams) and greater.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team updated a previously conducted systematic review and meta-analysis to examine the association between alcohol use and mortality risk and to understand how age, sex, and sources of bias may affect the results. In the full sample, the researchers did not find any evidence for protective effects from moderate or less alcohol use and there was an increased risk of mortality with high levels of alcohol use and more. Adjusting the analysis to control for different sources of bias did not influence these results, but the results did vary by age and sex, with greater mortality risks observed in those who are younger and for women.
These findings do not support the notion that drinking moderately or less may have health benefits and promote longevity, which is consistent with the results of their prior meta-analysis. This is important for medical professionals who may have begun mistakenly recommending to their patients that drinking 1-2 glasses of wine each night may promote good health. Instead, it seems that people who do not currently drink alcohol should not start doing so for health benefits.
In many of the studies, alcohol use was only assessed at one time point. This limits the extent to which the researchers can understand how changes in alcohol use over time affect mortality risk.
Participants self-reported their alcohol use, which is prone to under-reporting. Participants may have also inaccurately reported that they have abstained from alcohol throughout their lives, but actually formerly consumed alcohol.
There was a limited number of studies that controlled for how binge drinking episodes (e.g., a measure of alcohol consumption during a concrete period of time like 2 hours) affect mortality risk. Although participants’ mean daily alcohol use may have been low, their overall alcohol use was not.
BOTTOM LINE
This updated review and meta-analysis found that low to moderate alcohol use was not associated with a decreased risk of mortality, but that high amounts of alcohol use were associated with an increased risk of mortality.
For individuals and families seeking recovery: Because this study did not support the notion that moderate or less alcohol use was associated with a decreased risk of mortality, it is not recommended that individuals begin drinking for health benefits or longevity if they do not already do so. Among individuals who choose to drink alcohol, this study is consistent with the current guidelines that men should limit their alcohol use to 2 drinks per day or less, and women 1 drink per day (i.e., moderate drinking). Note however, that certain risks of alcohol use, like breast cancer in women, are present even at these lower levels and many countries now have already begun moving toward recommending no or very low levels of alcohol use in order to optimize your health.
For treatment professionals and treatment systems: This study did not support the notion that moderate alcohol use or less was associated with a decreased risk of mortality. Accordingly, health professionals are cautioned against recommending moderate drinking for health benefits. Further, health professionals who inform their patients of the health and mortality risks associated with high levels of alcohol use may reduce their mortality risks.
For scientists: Because many of the studies included in the meta-analysis assessed alcohol at one time point only, future research that includes additional time points would shed light on how changes in alcohol use over time influence mortality risk. Also, using methods other than self-report to assess alcohol use, such as new wearable technology or biosensors, may allow researchers to avoid the self-report bias often seen in these studies. Finally, future research that more closely examines how binge drinking affects mortality risk would provide an understanding of how different patterns of drinking influence health outcomes.
For policy makers: This study demonstrated that moderate alcohol use is not associated with decreased risk of mortality, but that drinking higher volumes of alcohol is associated with an increased mortality risk. Public health campaigns that promote the health risks of alcohol may help to inform the public and reduce their mortality risks from alcohol. Additionally, policies that limit access to alcohol (e.g., taxation, limits on the number of alcohol outlets in a given location, etc.) may further help to reduce how much alcohol people consume and improve overall public health.