How much does daily goal setting matter when quitting or reducing alcohol use? Quite a lot
Daily goal setting is an important aspect of cutting back or quitting alcohol use, and could change day-to-day, especially for people with less severe alcohol use problems that have goals other than abstinence. This study examined how day-to-day goal setting of abstinence or reduced drinking affects consumption over 3 weeks for individuals with alcohol use disorder in the community interested in reducing their alcohol use.
Treatment programs and other settings that offer brief interventions for alcohol use are increasingly providing individuals the opportunity to choose their drinking reduction goals as a way to increase engagement and reduce harm.
In research examining who may be more likely to choose an abstinence vs a moderation goal, and how the type of goal affects treatment outcomes over time, people who choose abstinence may be experiencing more alcohol problems at the time of entering treatment and worse mental and physical health symptoms overall. Whereas those who choose moderation may be experiencing fewer alcohol problems and more social support for drinking. Some nationally representative studies show that abstinence may be associated with greater quality of life, less psychological distress, and for those in remission, a lower likelihood that alcohol use disorder symptoms will return relative to a moderation goal.
However, this research cannot account entirely for changes to that goal throughout the course of treatment or in the person’s lifetime. In reality, and especially for individuals choosing moderation goals, individuals often set a daily alcohol use goal, and this can change day-to-day, or change over weeks or months. To learn more about how daily goal setting affects alcohol use on a day-to-day level, as part of a larger study of brief interventions for individuals with alcohol use disorder interested in reducing or quitting alcohol use, this study examined drinking goals and behaviors daily for 3 weeks after receiving personalized feedback and brief advice about their alcohol use.
HOW WAS THIS STUDY CONDUCTED?
In this study, 153 individuals seeking treatment for alcohol use disorder, after receiving personalized feedback and brief advice about their alcohol use, completed 21 days of daily surveys about their alcohol use the previous day and their drinking goal for the next 24 hours. The researchers examined changes in drinking goals over the 3-week period and how goal setting affected participants’ alcohol use day-to-day.
Participants were recruited for a larger trial testing brief interventions for alcohol use. For this study, the researchers analyzed the first 3-weeks of assessments before participants received further treatment. To be eligible for the study, participants must have been between ages 18-75, drinking heavily (NIAAA definition: for men, >4 drinks on any day or >14 drinks per week; for women, >3 drinks on any day or >7 drinks per week) and interested in reducing their drinking, did not have another substance use disorder (other than alcohol, cannabis, or nicotine) and were not using other drugs weekly, did not have a serious psychiatric disorder (e.g., Bipolar I, Schizophrenia), were not experiencing physical withdrawal symptoms from alcohol, had never received inpatient treatment for alcohol use (e.g., detox), and were not actively involved in another treatment for alcohol use in the past 90 days, including outpatient therapy or mutual-help groups (e.g., 12-step).
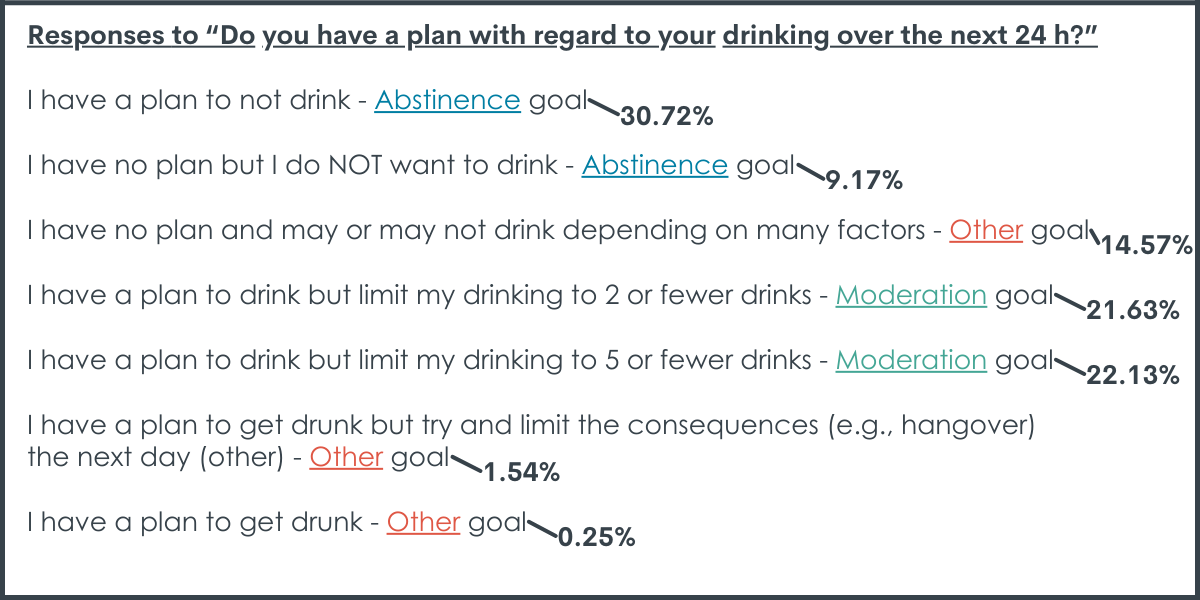
Upon enrollment into the study, participants received brief advice for alcohol use that included feedback on their risk for alcohol use disorder, determining their motivation to reduce drinking, setting drinking goals, and discussing strategies and potential challenges for reducing drinking. After receiving brief advice, participants received text messages for 21 days prompting them to complete a daily 5-7min survey asking about drinking in the last 24 hours and their goal for drinking in the next 24 hours. Participants were asked, “Do you have a plan with regard to your drinking over the next 24 h? (Plan here refers to having a specific strategy or number of drinks predetermined in your mind prior to starting drinking).” The options for drinking goals were:
For analysis, goals for drinking were categorized into: a) complete abstinence (e.g., I have a plan to not drink), b) moderation (e.g., I have a plan to drink but limit my drinking to 2 or fewer drinks), c) other (i.e., all other goals). Then the analysis tested how drinking goals at the daily level were related to: any alcohol consumption; exceeding 3 drinks; and total number of drinks on drinking days.
The daily surveys in this study (commonly referred to as ecological momentary assessment or “EMA”) allows the researchers to examine both individual differences between people in the study, as well as day-to-day differences for the same person, in more of a “real-world” setting because participants are filling out surveys “in-the-moment” or closer to when the behavior of interest (in this case, drinking and goal-setting about drinking) actually occurred.
Participants were between 22 and 73 years old, with an average age of 51. Most participants were White (90.9%), did not identify as Hispanic or Latinx (93.5%), and about two-thirds identified as female (68.0%). Almost half had a graduate degree or some graduate school (47.1%), about one quarter a bachelor’s degree (26.8%), and roughly two-thirds were employed full time (61.2%) and married (60.5%). Participants drank an average of 30 standard drinks per week and had an average of 3.5 heavy drinking days (>4 drinks per day for men, >3 drinks per day for women) per week. All participants met criteria for DSM-5 Alcohol Use Disorder, with most (71%) meeting 6 or more criteria indicative of severe Alcohol Use Disorder. The majority of participants indicated moderation drinking goals at the initial, brief advice session (88.9%).
WHAT DID THIS STUDY FIND?
The most common drinking goal was abstinence, however most drinking goals changed.
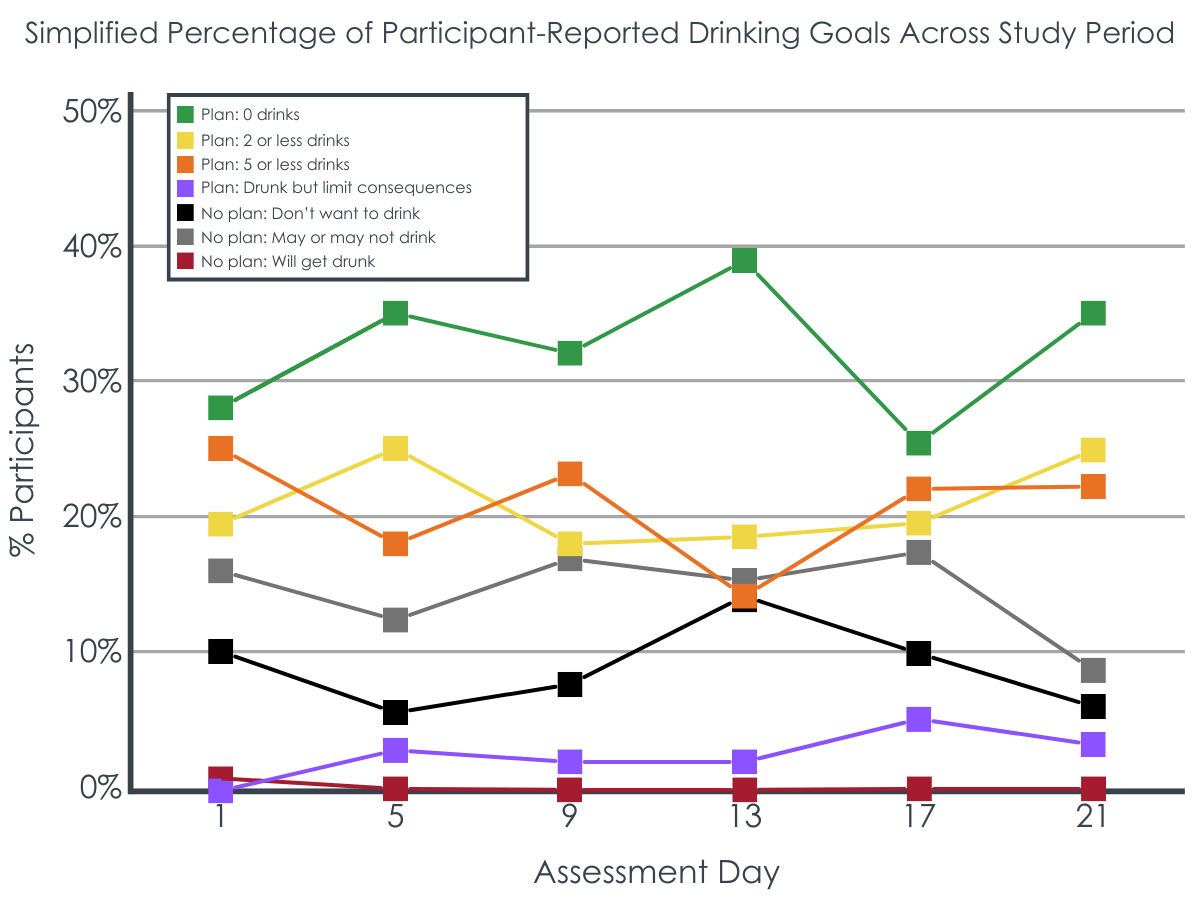
Across all daily surveys, abstinence was the most common goal (31% of morning reports), but there were only 3 participants (2%) whose daily goal started at, and never deviated from, complete abstinence. Goals to limit drinking to 2 or fewer (22%) or 5 or fewer (22%) were also common. Not having a drinking goal was less common (15%) and having a plan to get drunk was very infrequent (0.25%). About ¼ of participants (40 participants, 26%) never set an abstinence goal.
Setting a daily abstinence goal associated with best drinking outcomes in the next 24 hours.
When an abstinence goal was set, the odds of consuming 3+ drinks in the next 24 hours were reduced by 86% relative to when any other goal was set. On the other hand, for those setting abstinence goals, when a moderation goal was set, the odds of drinking 3+ drinks were increased by 3.28 times compared to when any other goal was set. For those who never set an abstinence goal, moderation goals were unrelated to (did not increase or decrease the odds of) drinking 3+ more drinks in the next 24 hours.
Any goal setting, whether abstinence or lower risk drinking, is associated with better outcomes than no goal setting.
Abstinence goals were associated with a 57% reduction in number of drinks compared to any other goal (including low risk drinking). Put another way, the predicted number of drinks consumed on a drinking day was 1.68 when an abstinence goal was set in the morning vs 3.92 drinks when any other goal was set in the morning. For those setting moderation goals, the number of drinks consumed in the next 24 hours was reduced by 10% compared to when any other goal was set (including abstinence). Put another way, the predicted number of drinks consumed on a drinking day was 2.44 when a moderation goal was set in the morning vs 2.70 drinks when any other goal was set in the morning.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Complete abstinence was the most common daily drinking goal and showed greater day-to-day stability than setting a moderation goal. In other words, once abstinence was chosen as a daily goal, the goal became more consistent over time. Alternatively, individuals who generally chose moderation-based goals fluctuated daily, perhaps being more influenced by external factors of the day. Setting an abstinence goal in the morning was also most successfully associated with abstinence as well as limiting alcohol consumption for the remainder of that day, relative to other goals.
The finding that individuals who set abstinence goals more often were also those who drank more per drinking occasion warrants special comment. Specifically, individuals who set abstinence goals may experience more problems related to alcohol use or may have had more attempts at moderation prior to starting treatment. For example, in a large alcohol treatment trial in the UK, participants choosing abstinence goals at the beginning of treatment also reported drinking more heavily but less frequently, were recently in detox, had more alcohol problems, less social support for drinking, and worse overall mental and physical health. Similarly, in the current study participants who set a larger proportion of abstinent days were more likely to drink more on the days they drank, —once they had any alcohol, they were likely to drink more heavily. Such individuals may have greater problem recognition given this severity and choose abstinence goals as a result. Those who set predominantly moderation goals on average did not demonstrate the same intensity of drinking on the days they drank. Individuals who have more difficulty with moderation may ultimately choose abstinence goals more often, compared to individuals who are able to set a moderation goal and achieve it.
There may be a therapeutic trade-off between daily abstinence and moderation goals, depending on the individual’s preferences and prior experiences. Although setting an abstinence goal was most successful in limiting alcohol consumption for the remainder of that day, setting any kind of specific goal, whether a daily abstinence goal or low-risk moderation goal, led to fewer drinks overall compared to the other goal categories. Prior research suggests that abstinence has the lowest risk of recurrence of alcohol use disorder symptoms, compared with non-abstinence-based goals; however, individuals may struggle with abstinence as a long-term choice, especially for those experiencing fewer consequences from drinking, and may reduce drinking and related-problems from moderation-based goals. In prior research, treatment success was related to the treatment goal: those with initial abstinence goals were more likely to obtain abstinence at the end of treatment, whereas those with initial moderation goals were more likely to reduce alcohol use and alcohol-related problems.
Taken together, it’s important for healthcare providers to engage as many individuals with alcohol use disorder as possible, who are likely to present with a range of goals. They should also help patients understand the challenges of setting daily goals for moderate drinking. While setting a goal to completely stop alcohol intake is a surefire way to reduce overall drinking, people who choose to include some alcohol-free days in their plan should be ready for the days when they do drink to avoid exceeding safe limits. Whether it’s a general practitioner or a specialist in alcohol treatment, professionals may recommend including a few days without alcohol to increase the chances of drinking less overall and on any single day.
This study focused on daily goals prior to starting treatment among people seeking treatment. The researchers wanted to understand how these goals affect how people change on their own and/or what may be useful to focus on when entering treatment. However, the researchers did not look at how goals and drinking habits change during treatment itself, which is something other studies often focus on. Comparing the goals people had before treatment with the ones they set during treatment could provide important insights into the process of change, but the researchers didn’t do that in this study.
The survey response options covered goals related to drinking less or abstaining altogether. However, as noted by the researchers, it might have been better if they had allowed participants to specify exactly how many drinks, they planned to have on a given day. The way the responses were currently worded didn’t allow the researchers to capture success of specific moderation-based goals (e.g., setting a goal to have 3 drinks and achieving it). Also, the way some questions were worded might have made it seem like the researchers were asking about different things. For instance, some questions were asked about goals, while others asked about plans or the consequences of drinking. For instance, asking about a “plan” might be more about the strategy someone has for reaching their goal, rather than the goal itself. Similarly, wanting to reduce the negative effects of heavy drinking could be a different goal than simply drinking less in terms of quantity.
A majority of participants in the study met criteria for severe alcohol use disorder (i.e., 7.5% had mild alcohol use disorder, 21% moderate, and 71.2% severe). This may mean that the findings demonstrating abstinence as a favorable daily goal may be most relevant to individuals who drink at higher levels or experience more negative consequences for use. In a sample with less severe alcohol problems, moderation-based daily goals could have shown greater success in goal achievement. Also, participants in the study were mostly female, middle-aged (i.e., between 40 and 60 years old on average), White, educated, and employed, meaning that the current study findings may not be representative of the general population of individuals with alcohol use disorder.
BOTTOM LINE
Daily goal setting can be an important aspect of alcohol reduction. Individuals tend to set daily goals as they pursue change in alcohol use. This study of individuals with alcohol use disorder seeking professional help to reduce their drinking, after receiving brief advice for alcohol use but before receiving additional treatment, found that abstinence- and moderation-based goals were both common. An abstinence goal in the morning, however, was most successful in limiting alcohol consumption for the remainder of that day, relative to other goals. Moderation goals were also beneficial compared to not setting any goal at all.
For individuals and families seeking recovery: Individuals experiencing more consequences from drinking may benefit more from setting abstinence-based goals relative to moderation-based goals. However, individuals struggling with abstinence as a long-term choice, or who may be experiencing fewer consequences from drinking, may find moderation a more approachable goal to reduce alcohol use and problems. Both abstinence and moderation goals appear to be better than not setting any goal at all.
For treatment professionals and treatment systems: Abstinence-based goals were the most stable relative to other goals and were the most successful in reducing overall drinking. However, individuals who set abstinence goals more often were also those who drank more per drinking occasion – such individuals may be more severe and have greater risk for hazardous drinking on days they drink. Healthcare providers may highlight the benefits of both abstinence and moderation-based goals, while helping patients understand the potential challenges of setting moderation goals and support patients to make specific plans for the days when they do drink to avoid exceeding recommended limits. Providers may recommend including a few days without alcohol to increase the chances of drinking less overall and on any single day and both abstinence and moderation goals are better than not setting any goal at all.
For scientists: This EMA study followed 153 individuals seeking treatment for alcohol use disorder, after receiving brief advice about alcohol use, for 21 days to measure changes in daily drinking goals and their effects on alcohol use. While both abstinence- and moderation-based goals were associated with reduced odds of drinking in the next 24 hours, abstinence was associated with the greatest reductions in alcohol use. Notably, individuals who set more abstinence goals, on average, were more likely to exceed 3+ drinks on drinking days when a moderation goal was set. In other words, once these participants had any alcohol, they were likely to drink more heavily. Such individuals may have greater problem recognition given this severity, have more difficulty limiting consumption once they start drinking, and thus choose abstinence goals as a result. Future research should utilize goal setting measures that allow for better goal specificity of moderation-based goals (i.e., a continuous capture of drinking) and separately capture different moderation constructs (i.e., reduction in drinking quantity versus negative consequences from heavy drinking). Lastly, to better guide the utility of goals for successful reduction in drinking, further research should be done comparing pre-treatment to in-treatment goals, as well as daily goals to overall goals for treatment. Such investigation would assist in establishing better treatment guidelines planning, skill building, and motivation.
For policy makers: Individuals experiencing more consequences from drinking may experience more overall reductions in alcohol use from setting abstinence-based goals relative to moderation-based goals. However, individuals struggling with abstinence as a long-term choice, or who may be experiencing fewer consequences from drinking, may find moderation a more approachable goal to reduce alcohol use and problems. Policies that recommend abstinence but are equally effective at engaging individuals with both abstinence and moderation goals may help bring more individuals into treatment while improving public health overall.
Treatment programs and other settings that offer brief interventions for alcohol use are increasingly providing individuals the opportunity to choose their drinking reduction goals as a way to increase engagement and reduce harm.
In research examining who may be more likely to choose an abstinence vs a moderation goal, and how the type of goal affects treatment outcomes over time, people who choose abstinence may be experiencing more alcohol problems at the time of entering treatment and worse mental and physical health symptoms overall. Whereas those who choose moderation may be experiencing fewer alcohol problems and more social support for drinking. Some nationally representative studies show that abstinence may be associated with greater quality of life, less psychological distress, and for those in remission, a lower likelihood that alcohol use disorder symptoms will return relative to a moderation goal.
However, this research cannot account entirely for changes to that goal throughout the course of treatment or in the person’s lifetime. In reality, and especially for individuals choosing moderation goals, individuals often set a daily alcohol use goal, and this can change day-to-day, or change over weeks or months. To learn more about how daily goal setting affects alcohol use on a day-to-day level, as part of a larger study of brief interventions for individuals with alcohol use disorder interested in reducing or quitting alcohol use, this study examined drinking goals and behaviors daily for 3 weeks after receiving personalized feedback and brief advice about their alcohol use.
HOW WAS THIS STUDY CONDUCTED?
In this study, 153 individuals seeking treatment for alcohol use disorder, after receiving personalized feedback and brief advice about their alcohol use, completed 21 days of daily surveys about their alcohol use the previous day and their drinking goal for the next 24 hours. The researchers examined changes in drinking goals over the 3-week period and how goal setting affected participants’ alcohol use day-to-day.
Participants were recruited for a larger trial testing brief interventions for alcohol use. For this study, the researchers analyzed the first 3-weeks of assessments before participants received further treatment. To be eligible for the study, participants must have been between ages 18-75, drinking heavily (NIAAA definition: for men, >4 drinks on any day or >14 drinks per week; for women, >3 drinks on any day or >7 drinks per week) and interested in reducing their drinking, did not have another substance use disorder (other than alcohol, cannabis, or nicotine) and were not using other drugs weekly, did not have a serious psychiatric disorder (e.g., Bipolar I, Schizophrenia), were not experiencing physical withdrawal symptoms from alcohol, had never received inpatient treatment for alcohol use (e.g., detox), and were not actively involved in another treatment for alcohol use in the past 90 days, including outpatient therapy or mutual-help groups (e.g., 12-step).
Upon enrollment into the study, participants received brief advice for alcohol use that included feedback on their risk for alcohol use disorder, determining their motivation to reduce drinking, setting drinking goals, and discussing strategies and potential challenges for reducing drinking. After receiving brief advice, participants received text messages for 21 days prompting them to complete a daily 5-7min survey asking about drinking in the last 24 hours and their goal for drinking in the next 24 hours. Participants were asked, “Do you have a plan with regard to your drinking over the next 24 h? (Plan here refers to having a specific strategy or number of drinks predetermined in your mind prior to starting drinking).” The options for drinking goals were:
For analysis, goals for drinking were categorized into: a) complete abstinence (e.g., I have a plan to not drink), b) moderation (e.g., I have a plan to drink but limit my drinking to 2 or fewer drinks), c) other (i.e., all other goals). Then the analysis tested how drinking goals at the daily level were related to: any alcohol consumption; exceeding 3 drinks; and total number of drinks on drinking days.
The daily surveys in this study (commonly referred to as ecological momentary assessment or “EMA”) allows the researchers to examine both individual differences between people in the study, as well as day-to-day differences for the same person, in more of a “real-world” setting because participants are filling out surveys “in-the-moment” or closer to when the behavior of interest (in this case, drinking and goal-setting about drinking) actually occurred.
Participants were between 22 and 73 years old, with an average age of 51. Most participants were White (90.9%), did not identify as Hispanic or Latinx (93.5%), and about two-thirds identified as female (68.0%). Almost half had a graduate degree or some graduate school (47.1%), about one quarter a bachelor’s degree (26.8%), and roughly two-thirds were employed full time (61.2%) and married (60.5%). Participants drank an average of 30 standard drinks per week and had an average of 3.5 heavy drinking days (>4 drinks per day for men, >3 drinks per day for women) per week. All participants met criteria for DSM-5 Alcohol Use Disorder, with most (71%) meeting 6 or more criteria indicative of severe Alcohol Use Disorder. The majority of participants indicated moderation drinking goals at the initial, brief advice session (88.9%).
WHAT DID THIS STUDY FIND?
The most common drinking goal was abstinence, however most drinking goals changed.
Across all daily surveys, abstinence was the most common goal (31% of morning reports), but there were only 3 participants (2%) whose daily goal started at, and never deviated from, complete abstinence. Goals to limit drinking to 2 or fewer (22%) or 5 or fewer (22%) were also common. Not having a drinking goal was less common (15%) and having a plan to get drunk was very infrequent (0.25%). About ¼ of participants (40 participants, 26%) never set an abstinence goal.
Setting a daily abstinence goal associated with best drinking outcomes in the next 24 hours.
When an abstinence goal was set, the odds of consuming 3+ drinks in the next 24 hours were reduced by 86% relative to when any other goal was set. On the other hand, for those setting abstinence goals, when a moderation goal was set, the odds of drinking 3+ drinks were increased by 3.28 times compared to when any other goal was set. For those who never set an abstinence goal, moderation goals were unrelated to (did not increase or decrease the odds of) drinking 3+ more drinks in the next 24 hours.
Any goal setting, whether abstinence or lower risk drinking, is associated with better outcomes than no goal setting.
Abstinence goals were associated with a 57% reduction in number of drinks compared to any other goal (including low risk drinking). Put another way, the predicted number of drinks consumed on a drinking day was 1.68 when an abstinence goal was set in the morning vs 3.92 drinks when any other goal was set in the morning. For those setting moderation goals, the number of drinks consumed in the next 24 hours was reduced by 10% compared to when any other goal was set (including abstinence). Put another way, the predicted number of drinks consumed on a drinking day was 2.44 when a moderation goal was set in the morning vs 2.70 drinks when any other goal was set in the morning.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Complete abstinence was the most common daily drinking goal and showed greater day-to-day stability than setting a moderation goal. In other words, once abstinence was chosen as a daily goal, the goal became more consistent over time. Alternatively, individuals who generally chose moderation-based goals fluctuated daily, perhaps being more influenced by external factors of the day. Setting an abstinence goal in the morning was also most successfully associated with abstinence as well as limiting alcohol consumption for the remainder of that day, relative to other goals.
The finding that individuals who set abstinence goals more often were also those who drank more per drinking occasion warrants special comment. Specifically, individuals who set abstinence goals may experience more problems related to alcohol use or may have had more attempts at moderation prior to starting treatment. For example, in a large alcohol treatment trial in the UK, participants choosing abstinence goals at the beginning of treatment also reported drinking more heavily but less frequently, were recently in detox, had more alcohol problems, less social support for drinking, and worse overall mental and physical health. Similarly, in the current study participants who set a larger proportion of abstinent days were more likely to drink more on the days they drank, —once they had any alcohol, they were likely to drink more heavily. Such individuals may have greater problem recognition given this severity and choose abstinence goals as a result. Those who set predominantly moderation goals on average did not demonstrate the same intensity of drinking on the days they drank. Individuals who have more difficulty with moderation may ultimately choose abstinence goals more often, compared to individuals who are able to set a moderation goal and achieve it.
There may be a therapeutic trade-off between daily abstinence and moderation goals, depending on the individual’s preferences and prior experiences. Although setting an abstinence goal was most successful in limiting alcohol consumption for the remainder of that day, setting any kind of specific goal, whether a daily abstinence goal or low-risk moderation goal, led to fewer drinks overall compared to the other goal categories. Prior research suggests that abstinence has the lowest risk of recurrence of alcohol use disorder symptoms, compared with non-abstinence-based goals; however, individuals may struggle with abstinence as a long-term choice, especially for those experiencing fewer consequences from drinking, and may reduce drinking and related-problems from moderation-based goals. In prior research, treatment success was related to the treatment goal: those with initial abstinence goals were more likely to obtain abstinence at the end of treatment, whereas those with initial moderation goals were more likely to reduce alcohol use and alcohol-related problems.
Taken together, it’s important for healthcare providers to engage as many individuals with alcohol use disorder as possible, who are likely to present with a range of goals. They should also help patients understand the challenges of setting daily goals for moderate drinking. While setting a goal to completely stop alcohol intake is a surefire way to reduce overall drinking, people who choose to include some alcohol-free days in their plan should be ready for the days when they do drink to avoid exceeding safe limits. Whether it’s a general practitioner or a specialist in alcohol treatment, professionals may recommend including a few days without alcohol to increase the chances of drinking less overall and on any single day.
This study focused on daily goals prior to starting treatment among people seeking treatment. The researchers wanted to understand how these goals affect how people change on their own and/or what may be useful to focus on when entering treatment. However, the researchers did not look at how goals and drinking habits change during treatment itself, which is something other studies often focus on. Comparing the goals people had before treatment with the ones they set during treatment could provide important insights into the process of change, but the researchers didn’t do that in this study.
The survey response options covered goals related to drinking less or abstaining altogether. However, as noted by the researchers, it might have been better if they had allowed participants to specify exactly how many drinks, they planned to have on a given day. The way the responses were currently worded didn’t allow the researchers to capture success of specific moderation-based goals (e.g., setting a goal to have 3 drinks and achieving it). Also, the way some questions were worded might have made it seem like the researchers were asking about different things. For instance, some questions were asked about goals, while others asked about plans or the consequences of drinking. For instance, asking about a “plan” might be more about the strategy someone has for reaching their goal, rather than the goal itself. Similarly, wanting to reduce the negative effects of heavy drinking could be a different goal than simply drinking less in terms of quantity.
A majority of participants in the study met criteria for severe alcohol use disorder (i.e., 7.5% had mild alcohol use disorder, 21% moderate, and 71.2% severe). This may mean that the findings demonstrating abstinence as a favorable daily goal may be most relevant to individuals who drink at higher levels or experience more negative consequences for use. In a sample with less severe alcohol problems, moderation-based daily goals could have shown greater success in goal achievement. Also, participants in the study were mostly female, middle-aged (i.e., between 40 and 60 years old on average), White, educated, and employed, meaning that the current study findings may not be representative of the general population of individuals with alcohol use disorder.
BOTTOM LINE
Daily goal setting can be an important aspect of alcohol reduction. Individuals tend to set daily goals as they pursue change in alcohol use. This study of individuals with alcohol use disorder seeking professional help to reduce their drinking, after receiving brief advice for alcohol use but before receiving additional treatment, found that abstinence- and moderation-based goals were both common. An abstinence goal in the morning, however, was most successful in limiting alcohol consumption for the remainder of that day, relative to other goals. Moderation goals were also beneficial compared to not setting any goal at all.
For individuals and families seeking recovery: Individuals experiencing more consequences from drinking may benefit more from setting abstinence-based goals relative to moderation-based goals. However, individuals struggling with abstinence as a long-term choice, or who may be experiencing fewer consequences from drinking, may find moderation a more approachable goal to reduce alcohol use and problems. Both abstinence and moderation goals appear to be better than not setting any goal at all.
For treatment professionals and treatment systems: Abstinence-based goals were the most stable relative to other goals and were the most successful in reducing overall drinking. However, individuals who set abstinence goals more often were also those who drank more per drinking occasion – such individuals may be more severe and have greater risk for hazardous drinking on days they drink. Healthcare providers may highlight the benefits of both abstinence and moderation-based goals, while helping patients understand the potential challenges of setting moderation goals and support patients to make specific plans for the days when they do drink to avoid exceeding recommended limits. Providers may recommend including a few days without alcohol to increase the chances of drinking less overall and on any single day and both abstinence and moderation goals are better than not setting any goal at all.
For scientists: This EMA study followed 153 individuals seeking treatment for alcohol use disorder, after receiving brief advice about alcohol use, for 21 days to measure changes in daily drinking goals and their effects on alcohol use. While both abstinence- and moderation-based goals were associated with reduced odds of drinking in the next 24 hours, abstinence was associated with the greatest reductions in alcohol use. Notably, individuals who set more abstinence goals, on average, were more likely to exceed 3+ drinks on drinking days when a moderation goal was set. In other words, once these participants had any alcohol, they were likely to drink more heavily. Such individuals may have greater problem recognition given this severity, have more difficulty limiting consumption once they start drinking, and thus choose abstinence goals as a result. Future research should utilize goal setting measures that allow for better goal specificity of moderation-based goals (i.e., a continuous capture of drinking) and separately capture different moderation constructs (i.e., reduction in drinking quantity versus negative consequences from heavy drinking). Lastly, to better guide the utility of goals for successful reduction in drinking, further research should be done comparing pre-treatment to in-treatment goals, as well as daily goals to overall goals for treatment. Such investigation would assist in establishing better treatment guidelines planning, skill building, and motivation.
For policy makers: Individuals experiencing more consequences from drinking may experience more overall reductions in alcohol use from setting abstinence-based goals relative to moderation-based goals. However, individuals struggling with abstinence as a long-term choice, or who may be experiencing fewer consequences from drinking, may find moderation a more approachable goal to reduce alcohol use and problems. Policies that recommend abstinence but are equally effective at engaging individuals with both abstinence and moderation goals may help bring more individuals into treatment while improving public health overall.
Treatment programs and other settings that offer brief interventions for alcohol use are increasingly providing individuals the opportunity to choose their drinking reduction goals as a way to increase engagement and reduce harm.
In research examining who may be more likely to choose an abstinence vs a moderation goal, and how the type of goal affects treatment outcomes over time, people who choose abstinence may be experiencing more alcohol problems at the time of entering treatment and worse mental and physical health symptoms overall. Whereas those who choose moderation may be experiencing fewer alcohol problems and more social support for drinking. Some nationally representative studies show that abstinence may be associated with greater quality of life, less psychological distress, and for those in remission, a lower likelihood that alcohol use disorder symptoms will return relative to a moderation goal.
However, this research cannot account entirely for changes to that goal throughout the course of treatment or in the person’s lifetime. In reality, and especially for individuals choosing moderation goals, individuals often set a daily alcohol use goal, and this can change day-to-day, or change over weeks or months. To learn more about how daily goal setting affects alcohol use on a day-to-day level, as part of a larger study of brief interventions for individuals with alcohol use disorder interested in reducing or quitting alcohol use, this study examined drinking goals and behaviors daily for 3 weeks after receiving personalized feedback and brief advice about their alcohol use.
HOW WAS THIS STUDY CONDUCTED?
In this study, 153 individuals seeking treatment for alcohol use disorder, after receiving personalized feedback and brief advice about their alcohol use, completed 21 days of daily surveys about their alcohol use the previous day and their drinking goal for the next 24 hours. The researchers examined changes in drinking goals over the 3-week period and how goal setting affected participants’ alcohol use day-to-day.
Participants were recruited for a larger trial testing brief interventions for alcohol use. For this study, the researchers analyzed the first 3-weeks of assessments before participants received further treatment. To be eligible for the study, participants must have been between ages 18-75, drinking heavily (NIAAA definition: for men, >4 drinks on any day or >14 drinks per week; for women, >3 drinks on any day or >7 drinks per week) and interested in reducing their drinking, did not have another substance use disorder (other than alcohol, cannabis, or nicotine) and were not using other drugs weekly, did not have a serious psychiatric disorder (e.g., Bipolar I, Schizophrenia), were not experiencing physical withdrawal symptoms from alcohol, had never received inpatient treatment for alcohol use (e.g., detox), and were not actively involved in another treatment for alcohol use in the past 90 days, including outpatient therapy or mutual-help groups (e.g., 12-step).
Upon enrollment into the study, participants received brief advice for alcohol use that included feedback on their risk for alcohol use disorder, determining their motivation to reduce drinking, setting drinking goals, and discussing strategies and potential challenges for reducing drinking. After receiving brief advice, participants received text messages for 21 days prompting them to complete a daily 5-7min survey asking about drinking in the last 24 hours and their goal for drinking in the next 24 hours. Participants were asked, “Do you have a plan with regard to your drinking over the next 24 h? (Plan here refers to having a specific strategy or number of drinks predetermined in your mind prior to starting drinking).” The options for drinking goals were:
For analysis, goals for drinking were categorized into: a) complete abstinence (e.g., I have a plan to not drink), b) moderation (e.g., I have a plan to drink but limit my drinking to 2 or fewer drinks), c) other (i.e., all other goals). Then the analysis tested how drinking goals at the daily level were related to: any alcohol consumption; exceeding 3 drinks; and total number of drinks on drinking days.
The daily surveys in this study (commonly referred to as ecological momentary assessment or “EMA”) allows the researchers to examine both individual differences between people in the study, as well as day-to-day differences for the same person, in more of a “real-world” setting because participants are filling out surveys “in-the-moment” or closer to when the behavior of interest (in this case, drinking and goal-setting about drinking) actually occurred.
Participants were between 22 and 73 years old, with an average age of 51. Most participants were White (90.9%), did not identify as Hispanic or Latinx (93.5%), and about two-thirds identified as female (68.0%). Almost half had a graduate degree or some graduate school (47.1%), about one quarter a bachelor’s degree (26.8%), and roughly two-thirds were employed full time (61.2%) and married (60.5%). Participants drank an average of 30 standard drinks per week and had an average of 3.5 heavy drinking days (>4 drinks per day for men, >3 drinks per day for women) per week. All participants met criteria for DSM-5 Alcohol Use Disorder, with most (71%) meeting 6 or more criteria indicative of severe Alcohol Use Disorder. The majority of participants indicated moderation drinking goals at the initial, brief advice session (88.9%).
WHAT DID THIS STUDY FIND?
The most common drinking goal was abstinence, however most drinking goals changed.
Across all daily surveys, abstinence was the most common goal (31% of morning reports), but there were only 3 participants (2%) whose daily goal started at, and never deviated from, complete abstinence. Goals to limit drinking to 2 or fewer (22%) or 5 or fewer (22%) were also common. Not having a drinking goal was less common (15%) and having a plan to get drunk was very infrequent (0.25%). About ¼ of participants (40 participants, 26%) never set an abstinence goal.
Setting a daily abstinence goal associated with best drinking outcomes in the next 24 hours.
When an abstinence goal was set, the odds of consuming 3+ drinks in the next 24 hours were reduced by 86% relative to when any other goal was set. On the other hand, for those setting abstinence goals, when a moderation goal was set, the odds of drinking 3+ drinks were increased by 3.28 times compared to when any other goal was set. For those who never set an abstinence goal, moderation goals were unrelated to (did not increase or decrease the odds of) drinking 3+ more drinks in the next 24 hours.
Any goal setting, whether abstinence or lower risk drinking, is associated with better outcomes than no goal setting.
Abstinence goals were associated with a 57% reduction in number of drinks compared to any other goal (including low risk drinking). Put another way, the predicted number of drinks consumed on a drinking day was 1.68 when an abstinence goal was set in the morning vs 3.92 drinks when any other goal was set in the morning. For those setting moderation goals, the number of drinks consumed in the next 24 hours was reduced by 10% compared to when any other goal was set (including abstinence). Put another way, the predicted number of drinks consumed on a drinking day was 2.44 when a moderation goal was set in the morning vs 2.70 drinks when any other goal was set in the morning.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Complete abstinence was the most common daily drinking goal and showed greater day-to-day stability than setting a moderation goal. In other words, once abstinence was chosen as a daily goal, the goal became more consistent over time. Alternatively, individuals who generally chose moderation-based goals fluctuated daily, perhaps being more influenced by external factors of the day. Setting an abstinence goal in the morning was also most successfully associated with abstinence as well as limiting alcohol consumption for the remainder of that day, relative to other goals.
The finding that individuals who set abstinence goals more often were also those who drank more per drinking occasion warrants special comment. Specifically, individuals who set abstinence goals may experience more problems related to alcohol use or may have had more attempts at moderation prior to starting treatment. For example, in a large alcohol treatment trial in the UK, participants choosing abstinence goals at the beginning of treatment also reported drinking more heavily but less frequently, were recently in detox, had more alcohol problems, less social support for drinking, and worse overall mental and physical health. Similarly, in the current study participants who set a larger proportion of abstinent days were more likely to drink more on the days they drank, —once they had any alcohol, they were likely to drink more heavily. Such individuals may have greater problem recognition given this severity and choose abstinence goals as a result. Those who set predominantly moderation goals on average did not demonstrate the same intensity of drinking on the days they drank. Individuals who have more difficulty with moderation may ultimately choose abstinence goals more often, compared to individuals who are able to set a moderation goal and achieve it.
There may be a therapeutic trade-off between daily abstinence and moderation goals, depending on the individual’s preferences and prior experiences. Although setting an abstinence goal was most successful in limiting alcohol consumption for the remainder of that day, setting any kind of specific goal, whether a daily abstinence goal or low-risk moderation goal, led to fewer drinks overall compared to the other goal categories. Prior research suggests that abstinence has the lowest risk of recurrence of alcohol use disorder symptoms, compared with non-abstinence-based goals; however, individuals may struggle with abstinence as a long-term choice, especially for those experiencing fewer consequences from drinking, and may reduce drinking and related-problems from moderation-based goals. In prior research, treatment success was related to the treatment goal: those with initial abstinence goals were more likely to obtain abstinence at the end of treatment, whereas those with initial moderation goals were more likely to reduce alcohol use and alcohol-related problems.
Taken together, it’s important for healthcare providers to engage as many individuals with alcohol use disorder as possible, who are likely to present with a range of goals. They should also help patients understand the challenges of setting daily goals for moderate drinking. While setting a goal to completely stop alcohol intake is a surefire way to reduce overall drinking, people who choose to include some alcohol-free days in their plan should be ready for the days when they do drink to avoid exceeding safe limits. Whether it’s a general practitioner or a specialist in alcohol treatment, professionals may recommend including a few days without alcohol to increase the chances of drinking less overall and on any single day.
This study focused on daily goals prior to starting treatment among people seeking treatment. The researchers wanted to understand how these goals affect how people change on their own and/or what may be useful to focus on when entering treatment. However, the researchers did not look at how goals and drinking habits change during treatment itself, which is something other studies often focus on. Comparing the goals people had before treatment with the ones they set during treatment could provide important insights into the process of change, but the researchers didn’t do that in this study.
The survey response options covered goals related to drinking less or abstaining altogether. However, as noted by the researchers, it might have been better if they had allowed participants to specify exactly how many drinks, they planned to have on a given day. The way the responses were currently worded didn’t allow the researchers to capture success of specific moderation-based goals (e.g., setting a goal to have 3 drinks and achieving it). Also, the way some questions were worded might have made it seem like the researchers were asking about different things. For instance, some questions were asked about goals, while others asked about plans or the consequences of drinking. For instance, asking about a “plan” might be more about the strategy someone has for reaching their goal, rather than the goal itself. Similarly, wanting to reduce the negative effects of heavy drinking could be a different goal than simply drinking less in terms of quantity.
A majority of participants in the study met criteria for severe alcohol use disorder (i.e., 7.5% had mild alcohol use disorder, 21% moderate, and 71.2% severe). This may mean that the findings demonstrating abstinence as a favorable daily goal may be most relevant to individuals who drink at higher levels or experience more negative consequences for use. In a sample with less severe alcohol problems, moderation-based daily goals could have shown greater success in goal achievement. Also, participants in the study were mostly female, middle-aged (i.e., between 40 and 60 years old on average), White, educated, and employed, meaning that the current study findings may not be representative of the general population of individuals with alcohol use disorder.
BOTTOM LINE
Daily goal setting can be an important aspect of alcohol reduction. Individuals tend to set daily goals as they pursue change in alcohol use. This study of individuals with alcohol use disorder seeking professional help to reduce their drinking, after receiving brief advice for alcohol use but before receiving additional treatment, found that abstinence- and moderation-based goals were both common. An abstinence goal in the morning, however, was most successful in limiting alcohol consumption for the remainder of that day, relative to other goals. Moderation goals were also beneficial compared to not setting any goal at all.
For individuals and families seeking recovery: Individuals experiencing more consequences from drinking may benefit more from setting abstinence-based goals relative to moderation-based goals. However, individuals struggling with abstinence as a long-term choice, or who may be experiencing fewer consequences from drinking, may find moderation a more approachable goal to reduce alcohol use and problems. Both abstinence and moderation goals appear to be better than not setting any goal at all.
For treatment professionals and treatment systems: Abstinence-based goals were the most stable relative to other goals and were the most successful in reducing overall drinking. However, individuals who set abstinence goals more often were also those who drank more per drinking occasion – such individuals may be more severe and have greater risk for hazardous drinking on days they drink. Healthcare providers may highlight the benefits of both abstinence and moderation-based goals, while helping patients understand the potential challenges of setting moderation goals and support patients to make specific plans for the days when they do drink to avoid exceeding recommended limits. Providers may recommend including a few days without alcohol to increase the chances of drinking less overall and on any single day and both abstinence and moderation goals are better than not setting any goal at all.
For scientists: This EMA study followed 153 individuals seeking treatment for alcohol use disorder, after receiving brief advice about alcohol use, for 21 days to measure changes in daily drinking goals and their effects on alcohol use. While both abstinence- and moderation-based goals were associated with reduced odds of drinking in the next 24 hours, abstinence was associated with the greatest reductions in alcohol use. Notably, individuals who set more abstinence goals, on average, were more likely to exceed 3+ drinks on drinking days when a moderation goal was set. In other words, once these participants had any alcohol, they were likely to drink more heavily. Such individuals may have greater problem recognition given this severity, have more difficulty limiting consumption once they start drinking, and thus choose abstinence goals as a result. Future research should utilize goal setting measures that allow for better goal specificity of moderation-based goals (i.e., a continuous capture of drinking) and separately capture different moderation constructs (i.e., reduction in drinking quantity versus negative consequences from heavy drinking). Lastly, to better guide the utility of goals for successful reduction in drinking, further research should be done comparing pre-treatment to in-treatment goals, as well as daily goals to overall goals for treatment. Such investigation would assist in establishing better treatment guidelines planning, skill building, and motivation.
For policy makers: Individuals experiencing more consequences from drinking may experience more overall reductions in alcohol use from setting abstinence-based goals relative to moderation-based goals. However, individuals struggling with abstinence as a long-term choice, or who may be experiencing fewer consequences from drinking, may find moderation a more approachable goal to reduce alcohol use and problems. Policies that recommend abstinence but are equally effective at engaging individuals with both abstinence and moderation goals may help bring more individuals into treatment while improving public health overall.