Does it work if you work out? Exercise-based interventions promote exercise but not drinking changes among individuals with alcohol use disorder
The majority of individuals with alcohol use disorder do not seek treatment. Efforts to engage non-treatment seeking individuals in care – including screening, brief intervention, and referral to treatment (SBIRT) – have produced mixed results. Given the high need for alternative approaches, these researchers developed and tested exercise interventions aimed to increase physical activity and reduce drinking among non-treatment seeking individuals with alcohol use disorder.
Alcohol use disorder is by far the most prevalent type of substance use disorder and similar to other types of other substance use disorders the vast majority (95%) of individuals with alcohol use disorder do not seek specialty treatment. Efforts to engage these individuals in treatment through non-alcohol use disorder treatment specific, but nevertheless clinical, settings where they individuals find themselves as a consequence of their alcohol use (e.g., emergency rooms) – including screening, brief intervention, and referral to treatment (SBIRT) – have produced mixed results. Primary barriers to treatment include lack of interest or awareness that alcohol use might be a problem, stigma around alcohol use disorder, and individuals’ desire to manage their drinking on their own. As a result, novel alternative approaches that are easy to implement and individuals find engaging and acceptable are needed.
Exercise-based interventions provide a non-stigmatizing option and could promote positive and general health behavior changes, and indirectly target drinking reduction by providing a health behavior that competes with the unhealthy alcohol use behavior. These interventions have not been found to positively impact drinking overall, but can promote wellbeing and increased confidence in making positive changes. The authors of this study evaluated two such stand-alone interventions for alcohol use disorder – one in which they provided non-treatment seeking individuals with paid gym memberships, and another in which they provided motivational interviewing paired with financial incentives for engaging in physical exercise.
HOW WAS THIS STUDY CONDUCTED?
This was a two-site (Hartford, CT; St. Louis, MO) randomized clinical trial of 66 individuals with alcohol use disorder who were also classified as sedentary (exercising less than two days per week over the last two months) and were not currently seeking treatment for alcohol use. Participants were randomized into one of two conditions. The first included receiving a paid 4-month YMCA gym membership – referred to as “comparison” below – and the second included the same 4-month gym membership plus 16 weeks of integrated motivational interviewing (two sessions) for exercise and contingency management (16 weekly, 10-15-minute sessions) – referred to as “intervention” below. Participants completed evaluations at baseline, 2 month, and 4 months post-baseline. Participants completed self-report measures to assess demographic, alcohol use and alcohol use related consequences, readiness to change alcohol use, depression symptoms, treatment engagement, and client satisfaction. The researchers also gathered body mass index (BMI) and blood pressure (BP) data from participants. The primary outcomes included exercise outcomes, and alcohol consumption and alcohol-related negative consequence outcomes secondarily. The study took place between 2010 and 2013.
Every participant received a paid 4-month gym membership but only the intervention group received motivational interviewing and exercise-based contingency management. The focus of motivational interviewing in this study was to promote exercise. Weekly 10- to 15-minute contingency management sessions, held over 16 consecutive weeks, included collaborative behavioral contracting to agree on three exercise activities to be completed over the next week. Verified completion of exercises earned one draw each from the prize bowl, and an extra draw if they completed all three assigned exercises that week. Bonus draws escalated over time such that participants could earn up to 10 bonus draws per week over time. Prizes included slips of paper with written praise, small prizes worth $1, large prizes worth $20, and jumbo prizes worth $100.
Eligible participants included sedentary individuals with alcohol use disorder (based on DSM-IV diagnostic criteria) between the ages of 21 and 65. Participants were also required to report at least four heavy drinking episodes (five or more for men, four or more for women in 1 day) in the past 2 months. Participants were excluded if they were currently engaged in treatment for alcohol use disorder, had acute psychiatric concerns, a body mass index above 35, high blood pressure, pregnant/hoping to become pregnant, met criteria for an opioid or cocaine use disorder, or currently in recovery from gambling disorder (to protect against any risk that might be introduced from the contingency management prize draw). Participants also had to be medically cleared for moderate intensity exercise.
Participants were 35 on average but ranged from 23 to 62. A total of 39% of the participants were men, 61% were women. Half of participants were White, a third were Black/African American, 8% reported multiple races/ethnicities, 5% were Hispanic, 3% were Asian, and nearly 2% were Native American. Participants reported completing an average of 15 years of education (e.g., some college/Associates degree level, on average) and reported a low average income of $25,000 per year. Participants’ body mass indexes ranged from 17-35 (“underweight” – “overweight”) and were 27 (“overweight”) on average.
WHAT DID THIS STUDY FIND?
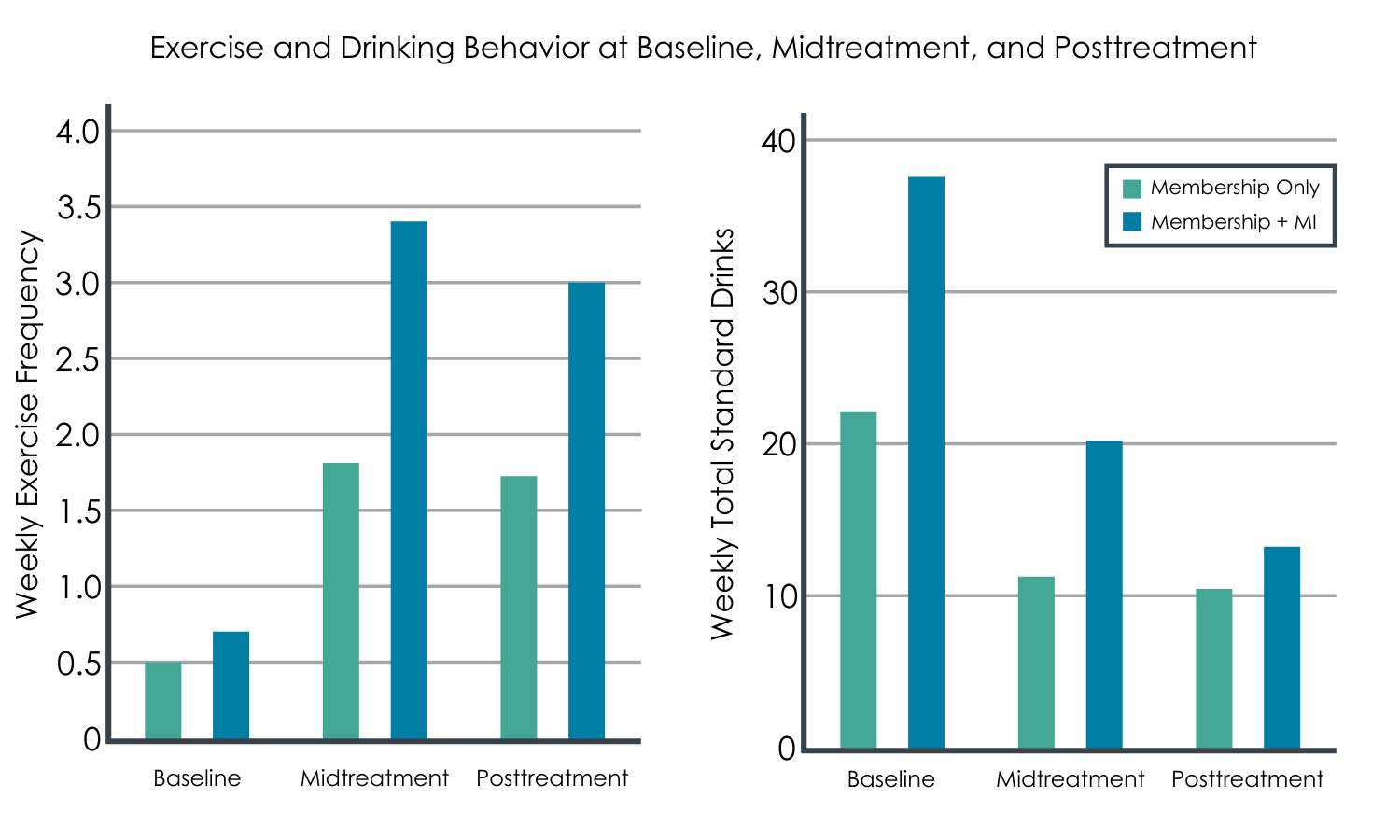
The intervention promoted increased exercise.
All participants, on average, increased their level of exercise over the study period, regardless of condition. However, participants in the intervention (i.e., motivational interviewing plus contingency management) exercised more frequently and for longer periods of time relative to the comparison (i.e., gym membership only). The intervention group experienced greater improvements in their systolic blood pressure over time relative to those in the comparison gym membership only group.
The intervention did not, however, promote reductions in drinking or other health outcomes.
Participants’ drinking levels across both groups decreased significantly over time, including weekly drinking totals, heavy drinking frequency, and alcohol-related negative consequences, but change did not differ between groups. However, intervention participants rated their experience more highly than comparison participants with respect to perceived positive impact of their intervention. While the groups were generally similar on other health outcomes in addition to drinking, the intervention group had moderately lower depression symptoms (i.e., a “medium” sized difference) though the benefit was quite varied among group members and did not quite meet for statistical significance.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The findings of this study suggest that motivational interviewing intervention plus contingency management can increase exercise frequency, duration, and improve blood pressure among sedentary individuals with alcohol use disorder who are given a free gym membership. These benefits were greater than those observed among individuals who only received the gym membership. Yet, this greater degree of exercise did not reduce alcohol use among individuals with alcohol use disorder any more than just receiving solely a gym membership.
The study used a four-month follow up period but this length of time might not have been long enough to observe between group differences on alcohol measures.
The exercise measures included self-report and would have benefitted from objective measures of physical exercise.
The study used a small sample and replication may benefit from larger samples.
BOTTOM LINE
For non-treatment-seeking individuals with alcohol use disorder who received a free gym membership, motivational interviewing plus contingency management interventions targeting increases in physical activity was found to be associated with more physical exercise and greater exercise duration compared to a gym membership only condition. Both groups were found to improve their drinking over time but there was no difference between the groups.
For treatment professionals and treatment systems: Helping clients to increase exercise can improve their mental health, physical health, and could also potentially promote reduction of alcohol use. The results of this study, however, do not support the notion that getting people to exercise more in the short-term is more likely to reduce alcohol use.
For scientists:This was a small randomized controlled trial of two exercise-based interventions. The first was a gym membership-only intervention and the other included Motivational Interviewing paired with contingency management to promote exercise. With respect to observing differential alcohol outcomes, future research may benefit from larger sample sizes, a longer follow up period, more intensive or different types of exercise, or pairing interventions with alcohol use-specific content to combine exercise with drinking reduction.
For policy makers: This study supports the efficacy of a Motivational Interviewing plus contingency management intervention over a gym membership-only condition in improving exercise frequency and duration among sedentary clients with alcohol use disorder. This study also demonstrated the potential to engage sedentary individuals with alcohol use disorder, who might not otherwise be engaged in other forms of intervention. Policy implications might be to help support more research into understanding the extent to which exercise interventions by themselves can promote reduced alcohol-related harms among individuals with alcohol use disorder.
Alcohol use disorder is by far the most prevalent type of substance use disorder and similar to other types of other substance use disorders the vast majority (95%) of individuals with alcohol use disorder do not seek specialty treatment. Efforts to engage these individuals in treatment through non-alcohol use disorder treatment specific, but nevertheless clinical, settings where they individuals find themselves as a consequence of their alcohol use (e.g., emergency rooms) – including screening, brief intervention, and referral to treatment (SBIRT) – have produced mixed results. Primary barriers to treatment include lack of interest or awareness that alcohol use might be a problem, stigma around alcohol use disorder, and individuals’ desire to manage their drinking on their own. As a result, novel alternative approaches that are easy to implement and individuals find engaging and acceptable are needed.
Exercise-based interventions provide a non-stigmatizing option and could promote positive and general health behavior changes, and indirectly target drinking reduction by providing a health behavior that competes with the unhealthy alcohol use behavior. These interventions have not been found to positively impact drinking overall, but can promote wellbeing and increased confidence in making positive changes. The authors of this study evaluated two such stand-alone interventions for alcohol use disorder – one in which they provided non-treatment seeking individuals with paid gym memberships, and another in which they provided motivational interviewing paired with financial incentives for engaging in physical exercise.
HOW WAS THIS STUDY CONDUCTED?
This was a two-site (Hartford, CT; St. Louis, MO) randomized clinical trial of 66 individuals with alcohol use disorder who were also classified as sedentary (exercising less than two days per week over the last two months) and were not currently seeking treatment for alcohol use. Participants were randomized into one of two conditions. The first included receiving a paid 4-month YMCA gym membership – referred to as “comparison” below – and the second included the same 4-month gym membership plus 16 weeks of integrated motivational interviewing (two sessions) for exercise and contingency management (16 weekly, 10-15-minute sessions) – referred to as “intervention” below. Participants completed evaluations at baseline, 2 month, and 4 months post-baseline. Participants completed self-report measures to assess demographic, alcohol use and alcohol use related consequences, readiness to change alcohol use, depression symptoms, treatment engagement, and client satisfaction. The researchers also gathered body mass index (BMI) and blood pressure (BP) data from participants. The primary outcomes included exercise outcomes, and alcohol consumption and alcohol-related negative consequence outcomes secondarily. The study took place between 2010 and 2013.
Every participant received a paid 4-month gym membership but only the intervention group received motivational interviewing and exercise-based contingency management. The focus of motivational interviewing in this study was to promote exercise. Weekly 10- to 15-minute contingency management sessions, held over 16 consecutive weeks, included collaborative behavioral contracting to agree on three exercise activities to be completed over the next week. Verified completion of exercises earned one draw each from the prize bowl, and an extra draw if they completed all three assigned exercises that week. Bonus draws escalated over time such that participants could earn up to 10 bonus draws per week over time. Prizes included slips of paper with written praise, small prizes worth $1, large prizes worth $20, and jumbo prizes worth $100.
Eligible participants included sedentary individuals with alcohol use disorder (based on DSM-IV diagnostic criteria) between the ages of 21 and 65. Participants were also required to report at least four heavy drinking episodes (five or more for men, four or more for women in 1 day) in the past 2 months. Participants were excluded if they were currently engaged in treatment for alcohol use disorder, had acute psychiatric concerns, a body mass index above 35, high blood pressure, pregnant/hoping to become pregnant, met criteria for an opioid or cocaine use disorder, or currently in recovery from gambling disorder (to protect against any risk that might be introduced from the contingency management prize draw). Participants also had to be medically cleared for moderate intensity exercise.
Participants were 35 on average but ranged from 23 to 62. A total of 39% of the participants were men, 61% were women. Half of participants were White, a third were Black/African American, 8% reported multiple races/ethnicities, 5% were Hispanic, 3% were Asian, and nearly 2% were Native American. Participants reported completing an average of 15 years of education (e.g., some college/Associates degree level, on average) and reported a low average income of $25,000 per year. Participants’ body mass indexes ranged from 17-35 (“underweight” – “overweight”) and were 27 (“overweight”) on average.
WHAT DID THIS STUDY FIND?
The intervention promoted increased exercise.
All participants, on average, increased their level of exercise over the study period, regardless of condition. However, participants in the intervention (i.e., motivational interviewing plus contingency management) exercised more frequently and for longer periods of time relative to the comparison (i.e., gym membership only). The intervention group experienced greater improvements in their systolic blood pressure over time relative to those in the comparison gym membership only group.
The intervention did not, however, promote reductions in drinking or other health outcomes.
Participants’ drinking levels across both groups decreased significantly over time, including weekly drinking totals, heavy drinking frequency, and alcohol-related negative consequences, but change did not differ between groups. However, intervention participants rated their experience more highly than comparison participants with respect to perceived positive impact of their intervention. While the groups were generally similar on other health outcomes in addition to drinking, the intervention group had moderately lower depression symptoms (i.e., a “medium” sized difference) though the benefit was quite varied among group members and did not quite meet for statistical significance.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The findings of this study suggest that motivational interviewing intervention plus contingency management can increase exercise frequency, duration, and improve blood pressure among sedentary individuals with alcohol use disorder who are given a free gym membership. These benefits were greater than those observed among individuals who only received the gym membership. Yet, this greater degree of exercise did not reduce alcohol use among individuals with alcohol use disorder any more than just receiving solely a gym membership.
The study used a four-month follow up period but this length of time might not have been long enough to observe between group differences on alcohol measures.
The exercise measures included self-report and would have benefitted from objective measures of physical exercise.
The study used a small sample and replication may benefit from larger samples.
BOTTOM LINE
For non-treatment-seeking individuals with alcohol use disorder who received a free gym membership, motivational interviewing plus contingency management interventions targeting increases in physical activity was found to be associated with more physical exercise and greater exercise duration compared to a gym membership only condition. Both groups were found to improve their drinking over time but there was no difference between the groups.
For treatment professionals and treatment systems: Helping clients to increase exercise can improve their mental health, physical health, and could also potentially promote reduction of alcohol use. The results of this study, however, do not support the notion that getting people to exercise more in the short-term is more likely to reduce alcohol use.
For scientists:This was a small randomized controlled trial of two exercise-based interventions. The first was a gym membership-only intervention and the other included Motivational Interviewing paired with contingency management to promote exercise. With respect to observing differential alcohol outcomes, future research may benefit from larger sample sizes, a longer follow up period, more intensive or different types of exercise, or pairing interventions with alcohol use-specific content to combine exercise with drinking reduction.
For policy makers: This study supports the efficacy of a Motivational Interviewing plus contingency management intervention over a gym membership-only condition in improving exercise frequency and duration among sedentary clients with alcohol use disorder. This study also demonstrated the potential to engage sedentary individuals with alcohol use disorder, who might not otherwise be engaged in other forms of intervention. Policy implications might be to help support more research into understanding the extent to which exercise interventions by themselves can promote reduced alcohol-related harms among individuals with alcohol use disorder.
Alcohol use disorder is by far the most prevalent type of substance use disorder and similar to other types of other substance use disorders the vast majority (95%) of individuals with alcohol use disorder do not seek specialty treatment. Efforts to engage these individuals in treatment through non-alcohol use disorder treatment specific, but nevertheless clinical, settings where they individuals find themselves as a consequence of their alcohol use (e.g., emergency rooms) – including screening, brief intervention, and referral to treatment (SBIRT) – have produced mixed results. Primary barriers to treatment include lack of interest or awareness that alcohol use might be a problem, stigma around alcohol use disorder, and individuals’ desire to manage their drinking on their own. As a result, novel alternative approaches that are easy to implement and individuals find engaging and acceptable are needed.
Exercise-based interventions provide a non-stigmatizing option and could promote positive and general health behavior changes, and indirectly target drinking reduction by providing a health behavior that competes with the unhealthy alcohol use behavior. These interventions have not been found to positively impact drinking overall, but can promote wellbeing and increased confidence in making positive changes. The authors of this study evaluated two such stand-alone interventions for alcohol use disorder – one in which they provided non-treatment seeking individuals with paid gym memberships, and another in which they provided motivational interviewing paired with financial incentives for engaging in physical exercise.
HOW WAS THIS STUDY CONDUCTED?
This was a two-site (Hartford, CT; St. Louis, MO) randomized clinical trial of 66 individuals with alcohol use disorder who were also classified as sedentary (exercising less than two days per week over the last two months) and were not currently seeking treatment for alcohol use. Participants were randomized into one of two conditions. The first included receiving a paid 4-month YMCA gym membership – referred to as “comparison” below – and the second included the same 4-month gym membership plus 16 weeks of integrated motivational interviewing (two sessions) for exercise and contingency management (16 weekly, 10-15-minute sessions) – referred to as “intervention” below. Participants completed evaluations at baseline, 2 month, and 4 months post-baseline. Participants completed self-report measures to assess demographic, alcohol use and alcohol use related consequences, readiness to change alcohol use, depression symptoms, treatment engagement, and client satisfaction. The researchers also gathered body mass index (BMI) and blood pressure (BP) data from participants. The primary outcomes included exercise outcomes, and alcohol consumption and alcohol-related negative consequence outcomes secondarily. The study took place between 2010 and 2013.
Every participant received a paid 4-month gym membership but only the intervention group received motivational interviewing and exercise-based contingency management. The focus of motivational interviewing in this study was to promote exercise. Weekly 10- to 15-minute contingency management sessions, held over 16 consecutive weeks, included collaborative behavioral contracting to agree on three exercise activities to be completed over the next week. Verified completion of exercises earned one draw each from the prize bowl, and an extra draw if they completed all three assigned exercises that week. Bonus draws escalated over time such that participants could earn up to 10 bonus draws per week over time. Prizes included slips of paper with written praise, small prizes worth $1, large prizes worth $20, and jumbo prizes worth $100.
Eligible participants included sedentary individuals with alcohol use disorder (based on DSM-IV diagnostic criteria) between the ages of 21 and 65. Participants were also required to report at least four heavy drinking episodes (five or more for men, four or more for women in 1 day) in the past 2 months. Participants were excluded if they were currently engaged in treatment for alcohol use disorder, had acute psychiatric concerns, a body mass index above 35, high blood pressure, pregnant/hoping to become pregnant, met criteria for an opioid or cocaine use disorder, or currently in recovery from gambling disorder (to protect against any risk that might be introduced from the contingency management prize draw). Participants also had to be medically cleared for moderate intensity exercise.
Participants were 35 on average but ranged from 23 to 62. A total of 39% of the participants were men, 61% were women. Half of participants were White, a third were Black/African American, 8% reported multiple races/ethnicities, 5% were Hispanic, 3% were Asian, and nearly 2% were Native American. Participants reported completing an average of 15 years of education (e.g., some college/Associates degree level, on average) and reported a low average income of $25,000 per year. Participants’ body mass indexes ranged from 17-35 (“underweight” – “overweight”) and were 27 (“overweight”) on average.
WHAT DID THIS STUDY FIND?
The intervention promoted increased exercise.
All participants, on average, increased their level of exercise over the study period, regardless of condition. However, participants in the intervention (i.e., motivational interviewing plus contingency management) exercised more frequently and for longer periods of time relative to the comparison (i.e., gym membership only). The intervention group experienced greater improvements in their systolic blood pressure over time relative to those in the comparison gym membership only group.
The intervention did not, however, promote reductions in drinking or other health outcomes.
Participants’ drinking levels across both groups decreased significantly over time, including weekly drinking totals, heavy drinking frequency, and alcohol-related negative consequences, but change did not differ between groups. However, intervention participants rated their experience more highly than comparison participants with respect to perceived positive impact of their intervention. While the groups were generally similar on other health outcomes in addition to drinking, the intervention group had moderately lower depression symptoms (i.e., a “medium” sized difference) though the benefit was quite varied among group members and did not quite meet for statistical significance.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The findings of this study suggest that motivational interviewing intervention plus contingency management can increase exercise frequency, duration, and improve blood pressure among sedentary individuals with alcohol use disorder who are given a free gym membership. These benefits were greater than those observed among individuals who only received the gym membership. Yet, this greater degree of exercise did not reduce alcohol use among individuals with alcohol use disorder any more than just receiving solely a gym membership.
The study used a four-month follow up period but this length of time might not have been long enough to observe between group differences on alcohol measures.
The exercise measures included self-report and would have benefitted from objective measures of physical exercise.
The study used a small sample and replication may benefit from larger samples.
BOTTOM LINE
For non-treatment-seeking individuals with alcohol use disorder who received a free gym membership, motivational interviewing plus contingency management interventions targeting increases in physical activity was found to be associated with more physical exercise and greater exercise duration compared to a gym membership only condition. Both groups were found to improve their drinking over time but there was no difference between the groups.
For treatment professionals and treatment systems: Helping clients to increase exercise can improve their mental health, physical health, and could also potentially promote reduction of alcohol use. The results of this study, however, do not support the notion that getting people to exercise more in the short-term is more likely to reduce alcohol use.
For scientists:This was a small randomized controlled trial of two exercise-based interventions. The first was a gym membership-only intervention and the other included Motivational Interviewing paired with contingency management to promote exercise. With respect to observing differential alcohol outcomes, future research may benefit from larger sample sizes, a longer follow up period, more intensive or different types of exercise, or pairing interventions with alcohol use-specific content to combine exercise with drinking reduction.
For policy makers: This study supports the efficacy of a Motivational Interviewing plus contingency management intervention over a gym membership-only condition in improving exercise frequency and duration among sedentary clients with alcohol use disorder. This study also demonstrated the potential to engage sedentary individuals with alcohol use disorder, who might not otherwise be engaged in other forms of intervention. Policy implications might be to help support more research into understanding the extent to which exercise interventions by themselves can promote reduced alcohol-related harms among individuals with alcohol use disorder.