High potential, blunted outcomes: Promising digital intervention did not reduce cannabis use compared to educational materials
Most individuals with cannabis-related problems do not receive evidence-based treatment. Reasons include a lack of perceived need for professional treatment, financial costs, and fear of stigma. This study evaluated a digital intervention delivered by smartphone to individuals who were interested in quitting or reducing their cannabis use.
Digital technology-based interventions, such as those delivered through mobile health applications, may serve to cut through some of these barriers. In fact, studies show digital self-management interventions for reducing cannabis use can be somewhat helpful, though producing small effect sizes and leaving much room for improvement. Additionally, many cannabis users at higher risk levels who choose to use digital interventions may require professional treatment services to help with their efforts to reduce or quit cannabis use. Thus, digital interventions designed not only to aid individuals in quitting or reducing cannabis use on their own, but also serving to educate and change attitudes concerning treatment-seeking behaviors are warranted.
Along these lines, this study developed and tested a digital cannabis reduction intervention (called “ICan”) designed to motivate and assist cannabis users to quit or cut down cannabis use on their own. The intervention also encouraged those with more severe cannabis use profiles to seek professional help to address their cannabis-related problems.
HOW WAS THIS STUDY CONDUCTED?
This was a single-blind randomized control trial comparing the ICan interactive digital cannabis reduction intervention to a non-interactive educational control, with participation occurring independently and entirely online in the Netherlands.
Social media advertisements on Instagram and Facebook were used to recruit 378 total participants (69% Male; Mean age = 27.5 years). To be deemed eligible to participate in the study, participants had to meet the following inclusion criteria: a) 18 years or older, b) used cannabis an average of at least 3 days/week over the previous 3 months, c) had a desire to quit or reduce cannabis use, d) had access to a smartphone, and e) were willing to participate in the full study. Participants were excluded from the study if they had received any formal substance use disorder treatment in the previous 3 months, were pregnant or lactating, had suicidal ideation, severe depression, or acute psychosis, or were not proficient in the Dutch language.
Eligible participants who completed the baseline measure were then randomized to either a smartphone app-based digital cannabis reduction intervention (n = 188) or a non-interactive online educational module control (n = 190). Participants completed follow-up measures 6 weeks, 3 months, and 6 months after they entered the study. The primary study outcome variable was number of days of cannabis use in the previous 7 days at the 6-month follow-up. Secondary outcomes included number of days of cannabis use in the previous 7 days at 3-month follow-up, number of grams of cannabis used in previous 7 days at 3- and 6-month follow ups, cannabis use-related problems, number of DSM-5 cannabis use disorder symptoms, number of self-reported serious quit attempts, treatment-seeking attitudes, use of professional help in 3 months prior to follow-up measurements, and satisfaction with the ICan digital intervention.
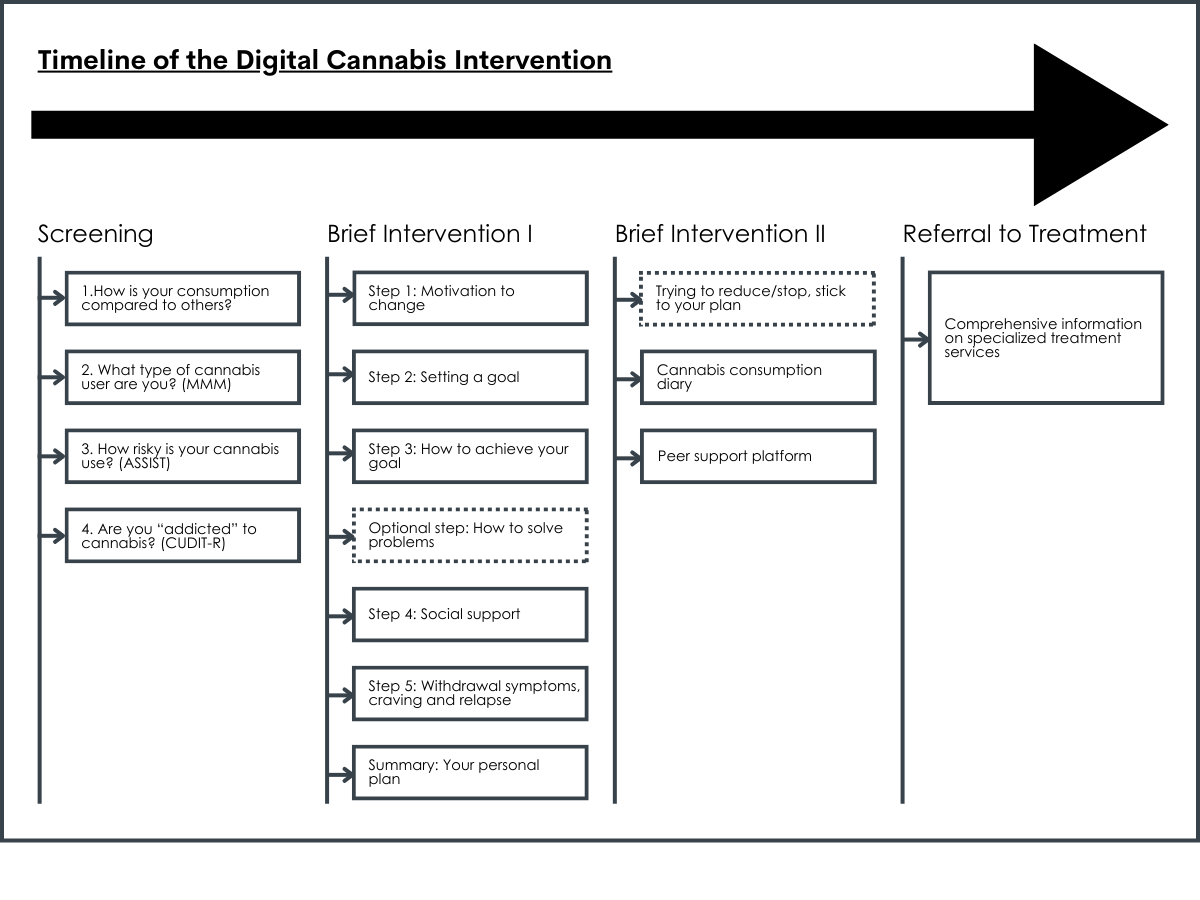
The ICan digital cannabis reduction intervention was based on CBT and MI principles and incorporated the screening, brief intervention, and referral to treatment framework. Four brief self-assessments (Marijuana Motives Measure, the ASSIST, Cannabis Use Disorders Identification Test-revised [CUDIT-R]) were used to screen cannabis use behaviors. Participant scores on screening items were used to inform feedback provided to the participant related to their cannabis-related risk profile. Those with elevated scores (ASSIST > 27, CUDIT-R > 13) on screening items indicative of increased risk for the development of cannabis use disorder were advised to use specialized treatment services in addition to using the ICan app. The ICan intervention itself consisted of 6 self-paced modules to help participants create a plan to quit or reduce their cannabis use, and upon completion of all six modules, encouraged them to follow their plan for at least 4 weeks. Those at elevated risk for developing cannabis use disorder as indicated by their scores on screening items were also given the referral to treatment component, which consisted of information on different evidence-based treatment options available and a tool to assist with finding treatment options in their local area. Participants assigned to the intervention condition received weekly personalized WhatsApp messages encouraging them to use the ICan app. Individuals assigned to the control condition in this study were given log-in access to a repository of 4 online modules of educational information pertaining to cannabis and general tips on how to reduce or quit cannabis use.
In this randomized trial, primary analyses tested whether participants assigned to the digital intervention had larger improvements over time (e.g., from baseline to 6-month follow-up) than the control group on cannabis use and related outcomes. Of note, all participants in the study were analyzed in the groups to which they were assigned, regardless of whether they completed the intervention as intended (i.e., an intent-to-treat analysis). Participants in this study were majority male (69.3%), mostly in their mid-to-late-20s (mean age = 27.5 years), and frequently used cannabis (6 out of the last 7 days on average). This study did not report racial and ethnic data for participants.
WHAT DID THIS STUDY FIND?
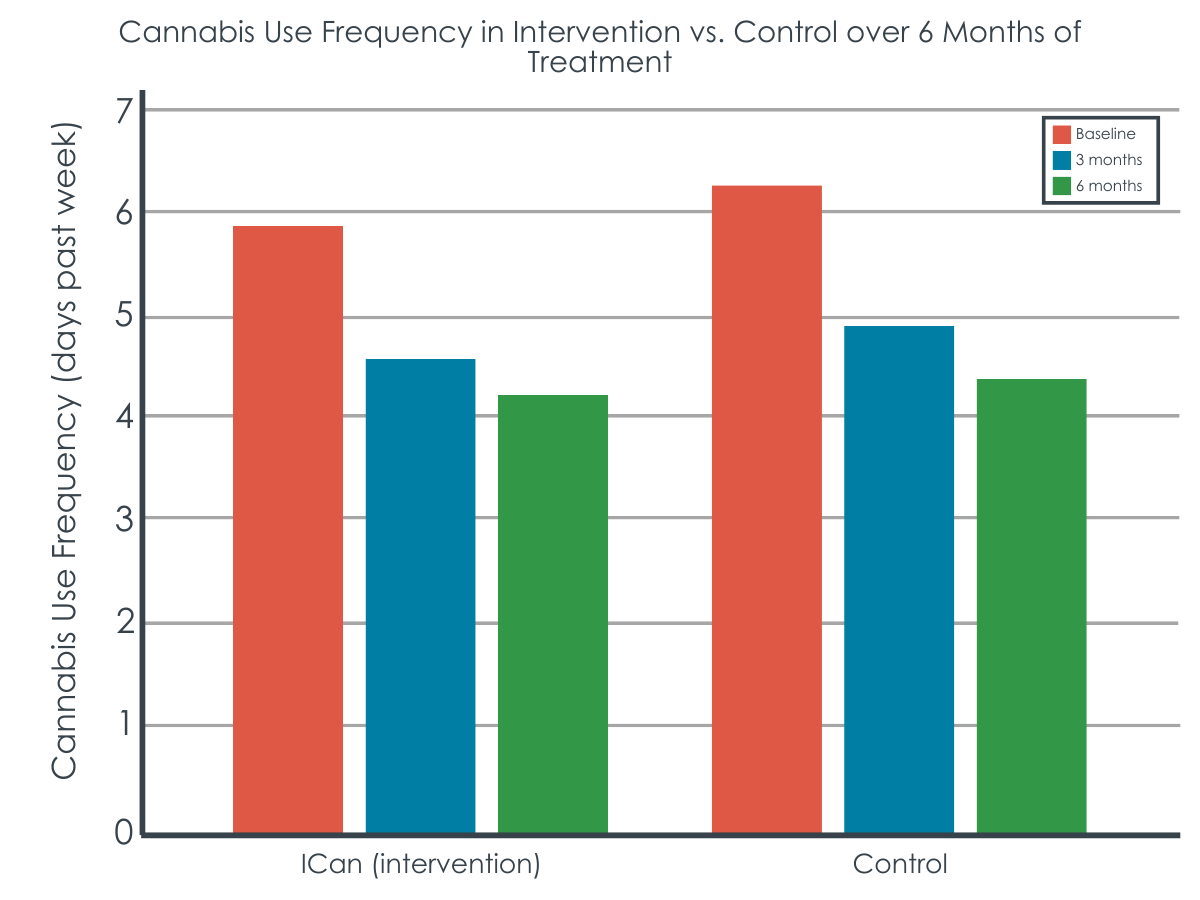
The interactive digital intervention and non-interactive online educational modules had similar outcomes.
At 3-month follow-up both the intervention and control groups had similar reductions on average number of days of cannabis, a pattern which lasted out to 6-month follow-up. The intervention condition had greater reductions in grams of cannabis use than the control group, however these differences between conditions were no longer there at 6-month follow-up. Participants in both conditions also increased their average number of serious attempts to quit or reduce cannabis use at 3-month follow-up with no differences between the groups.
Attitudes toward seeking formal help did not change throughout the study in either condition. Descriptively, slightly more participants in the ICan condition (16% at 3-month follow-up; 16% at 6-month follow-up) sought formal help compared to the educational control (11% at 3-month follow-up; 9% at 6-month follow-up).
Adherence to, and satisfaction with, the digital intervention.
In the ICan condition, 67% completed at least the 4 screening measures and first module. Only 25% of participants completed all six modules and participants completed 3 modules, on average. In the control, 78% completed at least 1 educational module and about 35% completed all 4 modules. Participants were more satisfied with the ICan digital intervention than the online educational modules although this greater satisfaction did not translate into greater reductions in cannabis use.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that a smartphone app adapted version of standard CBT/MI treatment did not outperform non-interactive online educational modules in assisting participants to reduce or quit their cannabis use over time. Additionally, the ICan mobile app-based intervention did not enhance attitudes concerning formal treatment-seeking.
Though there were at least moderate levels of engagement with the intervention (participants completed half of modules on average), findings highlight the multifaceted nature of behavioral change and potential need for incorporating advanced smartphone-based technological features that might serve to enhance efficacy and go beyond simple education (e.g., by using push notifications, providing personalized feedback, implementing geofencing, encouraging peer support). For example, empirically supported mobile apps like A-CHESS (Addiction-Comprehensive Health Enhancement Support System) leveraging advanced smartphone technology-based tools have been shown to support alcohol use disorder recovery efforts. Further exploration of smartphone technology-enhanced resources in digital cannabis reduction interventions is needed. Such digital interventions, if shown to be beneficial, could serve to offer several advantages and cut through barriers to change, including affordability and accessibility, and allow for broader implementation with fewer resources.
The trial was conducted only in the Netherlands and participants were required to have regular access to a smartphone and were recruited solely through social media advertisements. Thus, generalization of results to other populations, particularly to those outside of the Netherlands and with less access to technology are limited. This study also did not report on racial and ethnic data for participants.
Data collection for this study occurred from December 2019 to June 2020, which coincided with the COVID-19 pandemic and associated social distancing restrictions. As a result, it is plausible that participants’ substance use patterns changed during this time as a result (over a third of participants indicated that COVID-19 social distancing restrictions made it more difficult to reduce or stop their cannabis use), limiting generalizability of the findings beyond this time period.
BOTTOM LINE
Among young people already motivated to make a change to their cannabis use, simply having access to online educational content about cannabis use may be equally as helpful as the ICan digital intervention in supporting their efforts to quit or reduce their cannabis use.
For individuals and families seeking recovery: For those with more mild or moderate cannabis use problems, digital cannabis reduction interventions may be an easily accessible resource for aiding in self-guided attempts to quit or cut down on cannabis use that cut across barriers, such as cost and resistance to in-person treatment. This study showed that adapting an existing approach like CBT for cannabis use to the smartphone may not help any more than education and advice for individuals already interested in cutting back or quitting. Participation in digital cannabis reduction interventions may need to be coupled with more formal treatment services or additional support, especially for those with more severe cannabis use disorder.
For treatment professionals and treatment systems: This digital SBIRT intervention did not contribute to changes in treatment-seeking attitudes. Substance use disorder treatment systems may need to incorporate more effective strategies to help bridge the gap between individuals with cannabis use disorder and professional treatment. For example, actively linking patients from primary care settings with a desire to quit or reduce their cannabis use to specialized care may be a more effective approach. Treatment providers could devote further resources to help establish these linkages.
For scientists: Existing digital interventions to reduce cannabis use, while promising, leave much room for improvement. Efforts to increase the long-term effectiveness of these digital interventions, to better understand their active ingredients and the means through which participation in them confers benefits and for whom (demographic or clinical subgroups), as well as to increase ongoing engagement with them are needed. There is also a need to better understand how and to what extent it can be helpful to integrate digital substance use interventions in varying combinations with in-person treatment offerings. Additionally, the digital intervention in this study sought to add to existing efforts by attempting to change attitudes toward professional help-seeking behaviors but failed to do so. Future work to develop digital interventions capable of reducing perceived stigma among individuals struggling with cannabis-related problems may improve professional treatment seeking and ultimately improve substance use outcomes.
For policy makers: Increasing allocation of funding and resources to develop and test digital interventions to address cannabis use disorder and to implement these within treatment systems may prove to be a cost-effective means through which to provide support to many individuals who wish to quit or reduce their cannabis use and who may not be open to or able to access in-person or more formal treatment options. Increased funding can help researchers develop, test, and implement the best ways to engage individuals who would benefit from change but are not interested in seeking professional treatment.
Digital technology-based interventions, such as those delivered through mobile health applications, may serve to cut through some of these barriers. In fact, studies show digital self-management interventions for reducing cannabis use can be somewhat helpful, though producing small effect sizes and leaving much room for improvement. Additionally, many cannabis users at higher risk levels who choose to use digital interventions may require professional treatment services to help with their efforts to reduce or quit cannabis use. Thus, digital interventions designed not only to aid individuals in quitting or reducing cannabis use on their own, but also serving to educate and change attitudes concerning treatment-seeking behaviors are warranted.
Along these lines, this study developed and tested a digital cannabis reduction intervention (called “ICan”) designed to motivate and assist cannabis users to quit or cut down cannabis use on their own. The intervention also encouraged those with more severe cannabis use profiles to seek professional help to address their cannabis-related problems.
HOW WAS THIS STUDY CONDUCTED?
This was a single-blind randomized control trial comparing the ICan interactive digital cannabis reduction intervention to a non-interactive educational control, with participation occurring independently and entirely online in the Netherlands.
Social media advertisements on Instagram and Facebook were used to recruit 378 total participants (69% Male; Mean age = 27.5 years). To be deemed eligible to participate in the study, participants had to meet the following inclusion criteria: a) 18 years or older, b) used cannabis an average of at least 3 days/week over the previous 3 months, c) had a desire to quit or reduce cannabis use, d) had access to a smartphone, and e) were willing to participate in the full study. Participants were excluded from the study if they had received any formal substance use disorder treatment in the previous 3 months, were pregnant or lactating, had suicidal ideation, severe depression, or acute psychosis, or were not proficient in the Dutch language.
Eligible participants who completed the baseline measure were then randomized to either a smartphone app-based digital cannabis reduction intervention (n = 188) or a non-interactive online educational module control (n = 190). Participants completed follow-up measures 6 weeks, 3 months, and 6 months after they entered the study. The primary study outcome variable was number of days of cannabis use in the previous 7 days at the 6-month follow-up. Secondary outcomes included number of days of cannabis use in the previous 7 days at 3-month follow-up, number of grams of cannabis used in previous 7 days at 3- and 6-month follow ups, cannabis use-related problems, number of DSM-5 cannabis use disorder symptoms, number of self-reported serious quit attempts, treatment-seeking attitudes, use of professional help in 3 months prior to follow-up measurements, and satisfaction with the ICan digital intervention.
The ICan digital cannabis reduction intervention was based on CBT and MI principles and incorporated the screening, brief intervention, and referral to treatment framework. Four brief self-assessments (Marijuana Motives Measure, the ASSIST, Cannabis Use Disorders Identification Test-revised [CUDIT-R]) were used to screen cannabis use behaviors. Participant scores on screening items were used to inform feedback provided to the participant related to their cannabis-related risk profile. Those with elevated scores (ASSIST > 27, CUDIT-R > 13) on screening items indicative of increased risk for the development of cannabis use disorder were advised to use specialized treatment services in addition to using the ICan app. The ICan intervention itself consisted of 6 self-paced modules to help participants create a plan to quit or reduce their cannabis use, and upon completion of all six modules, encouraged them to follow their plan for at least 4 weeks. Those at elevated risk for developing cannabis use disorder as indicated by their scores on screening items were also given the referral to treatment component, which consisted of information on different evidence-based treatment options available and a tool to assist with finding treatment options in their local area. Participants assigned to the intervention condition received weekly personalized WhatsApp messages encouraging them to use the ICan app. Individuals assigned to the control condition in this study were given log-in access to a repository of 4 online modules of educational information pertaining to cannabis and general tips on how to reduce or quit cannabis use.
In this randomized trial, primary analyses tested whether participants assigned to the digital intervention had larger improvements over time (e.g., from baseline to 6-month follow-up) than the control group on cannabis use and related outcomes. Of note, all participants in the study were analyzed in the groups to which they were assigned, regardless of whether they completed the intervention as intended (i.e., an intent-to-treat analysis). Participants in this study were majority male (69.3%), mostly in their mid-to-late-20s (mean age = 27.5 years), and frequently used cannabis (6 out of the last 7 days on average). This study did not report racial and ethnic data for participants.
WHAT DID THIS STUDY FIND?
The interactive digital intervention and non-interactive online educational modules had similar outcomes.
At 3-month follow-up both the intervention and control groups had similar reductions on average number of days of cannabis, a pattern which lasted out to 6-month follow-up. The intervention condition had greater reductions in grams of cannabis use than the control group, however these differences between conditions were no longer there at 6-month follow-up. Participants in both conditions also increased their average number of serious attempts to quit or reduce cannabis use at 3-month follow-up with no differences between the groups.
Attitudes toward seeking formal help did not change throughout the study in either condition. Descriptively, slightly more participants in the ICan condition (16% at 3-month follow-up; 16% at 6-month follow-up) sought formal help compared to the educational control (11% at 3-month follow-up; 9% at 6-month follow-up).
Adherence to, and satisfaction with, the digital intervention.
In the ICan condition, 67% completed at least the 4 screening measures and first module. Only 25% of participants completed all six modules and participants completed 3 modules, on average. In the control, 78% completed at least 1 educational module and about 35% completed all 4 modules. Participants were more satisfied with the ICan digital intervention than the online educational modules although this greater satisfaction did not translate into greater reductions in cannabis use.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that a smartphone app adapted version of standard CBT/MI treatment did not outperform non-interactive online educational modules in assisting participants to reduce or quit their cannabis use over time. Additionally, the ICan mobile app-based intervention did not enhance attitudes concerning formal treatment-seeking.
Though there were at least moderate levels of engagement with the intervention (participants completed half of modules on average), findings highlight the multifaceted nature of behavioral change and potential need for incorporating advanced smartphone-based technological features that might serve to enhance efficacy and go beyond simple education (e.g., by using push notifications, providing personalized feedback, implementing geofencing, encouraging peer support). For example, empirically supported mobile apps like A-CHESS (Addiction-Comprehensive Health Enhancement Support System) leveraging advanced smartphone technology-based tools have been shown to support alcohol use disorder recovery efforts. Further exploration of smartphone technology-enhanced resources in digital cannabis reduction interventions is needed. Such digital interventions, if shown to be beneficial, could serve to offer several advantages and cut through barriers to change, including affordability and accessibility, and allow for broader implementation with fewer resources.
The trial was conducted only in the Netherlands and participants were required to have regular access to a smartphone and were recruited solely through social media advertisements. Thus, generalization of results to other populations, particularly to those outside of the Netherlands and with less access to technology are limited. This study also did not report on racial and ethnic data for participants.
Data collection for this study occurred from December 2019 to June 2020, which coincided with the COVID-19 pandemic and associated social distancing restrictions. As a result, it is plausible that participants’ substance use patterns changed during this time as a result (over a third of participants indicated that COVID-19 social distancing restrictions made it more difficult to reduce or stop their cannabis use), limiting generalizability of the findings beyond this time period.
BOTTOM LINE
Among young people already motivated to make a change to their cannabis use, simply having access to online educational content about cannabis use may be equally as helpful as the ICan digital intervention in supporting their efforts to quit or reduce their cannabis use.
For individuals and families seeking recovery: For those with more mild or moderate cannabis use problems, digital cannabis reduction interventions may be an easily accessible resource for aiding in self-guided attempts to quit or cut down on cannabis use that cut across barriers, such as cost and resistance to in-person treatment. This study showed that adapting an existing approach like CBT for cannabis use to the smartphone may not help any more than education and advice for individuals already interested in cutting back or quitting. Participation in digital cannabis reduction interventions may need to be coupled with more formal treatment services or additional support, especially for those with more severe cannabis use disorder.
For treatment professionals and treatment systems: This digital SBIRT intervention did not contribute to changes in treatment-seeking attitudes. Substance use disorder treatment systems may need to incorporate more effective strategies to help bridge the gap between individuals with cannabis use disorder and professional treatment. For example, actively linking patients from primary care settings with a desire to quit or reduce their cannabis use to specialized care may be a more effective approach. Treatment providers could devote further resources to help establish these linkages.
For scientists: Existing digital interventions to reduce cannabis use, while promising, leave much room for improvement. Efforts to increase the long-term effectiveness of these digital interventions, to better understand their active ingredients and the means through which participation in them confers benefits and for whom (demographic or clinical subgroups), as well as to increase ongoing engagement with them are needed. There is also a need to better understand how and to what extent it can be helpful to integrate digital substance use interventions in varying combinations with in-person treatment offerings. Additionally, the digital intervention in this study sought to add to existing efforts by attempting to change attitudes toward professional help-seeking behaviors but failed to do so. Future work to develop digital interventions capable of reducing perceived stigma among individuals struggling with cannabis-related problems may improve professional treatment seeking and ultimately improve substance use outcomes.
For policy makers: Increasing allocation of funding and resources to develop and test digital interventions to address cannabis use disorder and to implement these within treatment systems may prove to be a cost-effective means through which to provide support to many individuals who wish to quit or reduce their cannabis use and who may not be open to or able to access in-person or more formal treatment options. Increased funding can help researchers develop, test, and implement the best ways to engage individuals who would benefit from change but are not interested in seeking professional treatment.
Digital technology-based interventions, such as those delivered through mobile health applications, may serve to cut through some of these barriers. In fact, studies show digital self-management interventions for reducing cannabis use can be somewhat helpful, though producing small effect sizes and leaving much room for improvement. Additionally, many cannabis users at higher risk levels who choose to use digital interventions may require professional treatment services to help with their efforts to reduce or quit cannabis use. Thus, digital interventions designed not only to aid individuals in quitting or reducing cannabis use on their own, but also serving to educate and change attitudes concerning treatment-seeking behaviors are warranted.
Along these lines, this study developed and tested a digital cannabis reduction intervention (called “ICan”) designed to motivate and assist cannabis users to quit or cut down cannabis use on their own. The intervention also encouraged those with more severe cannabis use profiles to seek professional help to address their cannabis-related problems.
HOW WAS THIS STUDY CONDUCTED?
This was a single-blind randomized control trial comparing the ICan interactive digital cannabis reduction intervention to a non-interactive educational control, with participation occurring independently and entirely online in the Netherlands.
Social media advertisements on Instagram and Facebook were used to recruit 378 total participants (69% Male; Mean age = 27.5 years). To be deemed eligible to participate in the study, participants had to meet the following inclusion criteria: a) 18 years or older, b) used cannabis an average of at least 3 days/week over the previous 3 months, c) had a desire to quit or reduce cannabis use, d) had access to a smartphone, and e) were willing to participate in the full study. Participants were excluded from the study if they had received any formal substance use disorder treatment in the previous 3 months, were pregnant or lactating, had suicidal ideation, severe depression, or acute psychosis, or were not proficient in the Dutch language.
Eligible participants who completed the baseline measure were then randomized to either a smartphone app-based digital cannabis reduction intervention (n = 188) or a non-interactive online educational module control (n = 190). Participants completed follow-up measures 6 weeks, 3 months, and 6 months after they entered the study. The primary study outcome variable was number of days of cannabis use in the previous 7 days at the 6-month follow-up. Secondary outcomes included number of days of cannabis use in the previous 7 days at 3-month follow-up, number of grams of cannabis used in previous 7 days at 3- and 6-month follow ups, cannabis use-related problems, number of DSM-5 cannabis use disorder symptoms, number of self-reported serious quit attempts, treatment-seeking attitudes, use of professional help in 3 months prior to follow-up measurements, and satisfaction with the ICan digital intervention.
The ICan digital cannabis reduction intervention was based on CBT and MI principles and incorporated the screening, brief intervention, and referral to treatment framework. Four brief self-assessments (Marijuana Motives Measure, the ASSIST, Cannabis Use Disorders Identification Test-revised [CUDIT-R]) were used to screen cannabis use behaviors. Participant scores on screening items were used to inform feedback provided to the participant related to their cannabis-related risk profile. Those with elevated scores (ASSIST > 27, CUDIT-R > 13) on screening items indicative of increased risk for the development of cannabis use disorder were advised to use specialized treatment services in addition to using the ICan app. The ICan intervention itself consisted of 6 self-paced modules to help participants create a plan to quit or reduce their cannabis use, and upon completion of all six modules, encouraged them to follow their plan for at least 4 weeks. Those at elevated risk for developing cannabis use disorder as indicated by their scores on screening items were also given the referral to treatment component, which consisted of information on different evidence-based treatment options available and a tool to assist with finding treatment options in their local area. Participants assigned to the intervention condition received weekly personalized WhatsApp messages encouraging them to use the ICan app. Individuals assigned to the control condition in this study were given log-in access to a repository of 4 online modules of educational information pertaining to cannabis and general tips on how to reduce or quit cannabis use.
In this randomized trial, primary analyses tested whether participants assigned to the digital intervention had larger improvements over time (e.g., from baseline to 6-month follow-up) than the control group on cannabis use and related outcomes. Of note, all participants in the study were analyzed in the groups to which they were assigned, regardless of whether they completed the intervention as intended (i.e., an intent-to-treat analysis). Participants in this study were majority male (69.3%), mostly in their mid-to-late-20s (mean age = 27.5 years), and frequently used cannabis (6 out of the last 7 days on average). This study did not report racial and ethnic data for participants.
WHAT DID THIS STUDY FIND?
The interactive digital intervention and non-interactive online educational modules had similar outcomes.
At 3-month follow-up both the intervention and control groups had similar reductions on average number of days of cannabis, a pattern which lasted out to 6-month follow-up. The intervention condition had greater reductions in grams of cannabis use than the control group, however these differences between conditions were no longer there at 6-month follow-up. Participants in both conditions also increased their average number of serious attempts to quit or reduce cannabis use at 3-month follow-up with no differences between the groups.
Attitudes toward seeking formal help did not change throughout the study in either condition. Descriptively, slightly more participants in the ICan condition (16% at 3-month follow-up; 16% at 6-month follow-up) sought formal help compared to the educational control (11% at 3-month follow-up; 9% at 6-month follow-up).
Adherence to, and satisfaction with, the digital intervention.
In the ICan condition, 67% completed at least the 4 screening measures and first module. Only 25% of participants completed all six modules and participants completed 3 modules, on average. In the control, 78% completed at least 1 educational module and about 35% completed all 4 modules. Participants were more satisfied with the ICan digital intervention than the online educational modules although this greater satisfaction did not translate into greater reductions in cannabis use.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that a smartphone app adapted version of standard CBT/MI treatment did not outperform non-interactive online educational modules in assisting participants to reduce or quit their cannabis use over time. Additionally, the ICan mobile app-based intervention did not enhance attitudes concerning formal treatment-seeking.
Though there were at least moderate levels of engagement with the intervention (participants completed half of modules on average), findings highlight the multifaceted nature of behavioral change and potential need for incorporating advanced smartphone-based technological features that might serve to enhance efficacy and go beyond simple education (e.g., by using push notifications, providing personalized feedback, implementing geofencing, encouraging peer support). For example, empirically supported mobile apps like A-CHESS (Addiction-Comprehensive Health Enhancement Support System) leveraging advanced smartphone technology-based tools have been shown to support alcohol use disorder recovery efforts. Further exploration of smartphone technology-enhanced resources in digital cannabis reduction interventions is needed. Such digital interventions, if shown to be beneficial, could serve to offer several advantages and cut through barriers to change, including affordability and accessibility, and allow for broader implementation with fewer resources.
The trial was conducted only in the Netherlands and participants were required to have regular access to a smartphone and were recruited solely through social media advertisements. Thus, generalization of results to other populations, particularly to those outside of the Netherlands and with less access to technology are limited. This study also did not report on racial and ethnic data for participants.
Data collection for this study occurred from December 2019 to June 2020, which coincided with the COVID-19 pandemic and associated social distancing restrictions. As a result, it is plausible that participants’ substance use patterns changed during this time as a result (over a third of participants indicated that COVID-19 social distancing restrictions made it more difficult to reduce or stop their cannabis use), limiting generalizability of the findings beyond this time period.
BOTTOM LINE
Among young people already motivated to make a change to their cannabis use, simply having access to online educational content about cannabis use may be equally as helpful as the ICan digital intervention in supporting their efforts to quit or reduce their cannabis use.
For individuals and families seeking recovery: For those with more mild or moderate cannabis use problems, digital cannabis reduction interventions may be an easily accessible resource for aiding in self-guided attempts to quit or cut down on cannabis use that cut across barriers, such as cost and resistance to in-person treatment. This study showed that adapting an existing approach like CBT for cannabis use to the smartphone may not help any more than education and advice for individuals already interested in cutting back or quitting. Participation in digital cannabis reduction interventions may need to be coupled with more formal treatment services or additional support, especially for those with more severe cannabis use disorder.
For treatment professionals and treatment systems: This digital SBIRT intervention did not contribute to changes in treatment-seeking attitudes. Substance use disorder treatment systems may need to incorporate more effective strategies to help bridge the gap between individuals with cannabis use disorder and professional treatment. For example, actively linking patients from primary care settings with a desire to quit or reduce their cannabis use to specialized care may be a more effective approach. Treatment providers could devote further resources to help establish these linkages.
For scientists: Existing digital interventions to reduce cannabis use, while promising, leave much room for improvement. Efforts to increase the long-term effectiveness of these digital interventions, to better understand their active ingredients and the means through which participation in them confers benefits and for whom (demographic or clinical subgroups), as well as to increase ongoing engagement with them are needed. There is also a need to better understand how and to what extent it can be helpful to integrate digital substance use interventions in varying combinations with in-person treatment offerings. Additionally, the digital intervention in this study sought to add to existing efforts by attempting to change attitudes toward professional help-seeking behaviors but failed to do so. Future work to develop digital interventions capable of reducing perceived stigma among individuals struggling with cannabis-related problems may improve professional treatment seeking and ultimately improve substance use outcomes.
For policy makers: Increasing allocation of funding and resources to develop and test digital interventions to address cannabis use disorder and to implement these within treatment systems may prove to be a cost-effective means through which to provide support to many individuals who wish to quit or reduce their cannabis use and who may not be open to or able to access in-person or more formal treatment options. Increased funding can help researchers develop, test, and implement the best ways to engage individuals who would benefit from change but are not interested in seeking professional treatment.