Can a breathing-based intervention enhance the benefits of cognitive-behavioral therapy for amphetamine use disorder?
Heart Rate Variability Biofeedback is unique in its focus specifically on physiological systems that support emotional and behavioral regulation for individuals with substance use disorder. This clinical trial tested the utility of a biofeedback intervention for the treatment of amphetamine use disorder.
Heart Rate Variability Biofeedback is a breathing-based intervention that involves breathing at special frequencies that elicit immediate and dramatic changes in the cardiovascular system, including increased heart rate variability, which is a biomarker of health (higher variability reflects greater adaptive capacity and health). This intervention has been shown to reduce symptoms associated with a number of disorders including anxiety and depressive disorders, and post-traumatic stress disorder (PTSD). Based on these results, substance use disorder researchers have begun to explore if Heart Rate Variability Biofeedback could complement existing substance use disorder treatments.
Several small clinical trials have suggested Heart Rate Variability Biofeedback can assist substance use disorder recovery, particularly by reducing craving (see here for a review). At the same time, only one clinical trial to date has actually examined substance use outcomes, with Penzlin and colleagues finding Heart Rate Variability Biofeedback to be associated with lower alcohol use among those with alcohol use disorder, versus controls. Additionally, although previous studies have included individuals with a range of primary substances, no study to date has tested the utility of Heart Rate Variability Biofeedback specifically for the treatment of amphetamine use disorder.
To examine if Heart Rate Variability Biofeedback could potentially improve treatment outcomes among people with amphetamine use disorder, the authors of this paper tested a concise, 4-week Heart Rate Variability Biofeedback treatment protocol with individuals receiving outpatient treatment for amphetamine use disorder in Taiwan.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial that included 64 individuals engaged in outpatient treatment for amphetamine use disorder in which participants received either 4 weeks of Heart Rate Variability Biofeedback in addition to outpatient treatment-as-usual (experimental group), or treatment-as-usual only (control group).
Study inclusion criteria were: 1) being 20+ years of age, 2) male, 3) having mild, moderate, or severe DSM 5 amphetamine use disorder, 4) no co-occurring use of other substances, 5) no comorbid schizophrenia, major depressive disorder, or bipolar disorder, 6) no cardiovascular, lung, and neurological illnesses, and 7) having completed elementary school or higher.
Participants were assessed at study baseline, at 4-week follow-up (i.e., the end of the intervention), and at 8-week follow-up (i.e., 4 weeks after intervention completion). Study outcomes included craving, severity of amphetamine use disorder (measured with the Severity of Dependence Scale), and urine drug screening for amphetamine use.
The Heart Rate Variability Biofeedback intervention was delivered through weekly, 60-minute Heart Rate Variability Biofeedback training sessions, in which participants in the experimental group met with study coordinators and were taught to pace their breathing at special frequencies known to produce major increases in heart rate variability. Participants viewed their changing heart rate via an electrocardiogram device linked to a computer, which showed how their heart rate responded in real time to their paced breathing (i.e., biofeedback). Experimental participants were also instructed to practice 2 x 20-minute sessions per day using a handheld Heart Rate Variability Biofeedback device.
Treatment-as-usual, which all participants received, included once-weekly sessions of addiction focused, group Cognitive Behavioral Therapy over the 4 weeks.
Of the 64 study participants, 3 discontinued after study enrollment (1 experimental and 2 controls). The sample was on average 37 years old with relatively late initiation of amphetamine use at 30 years of age. All participants were male. On average, at baseline, the sample had mild to moderate amphetamine use disorder characterized by Severity of Dependence Scale scores of 5.3 out of a total possible score of 15.
WHAT DID THIS STUDY FIND?
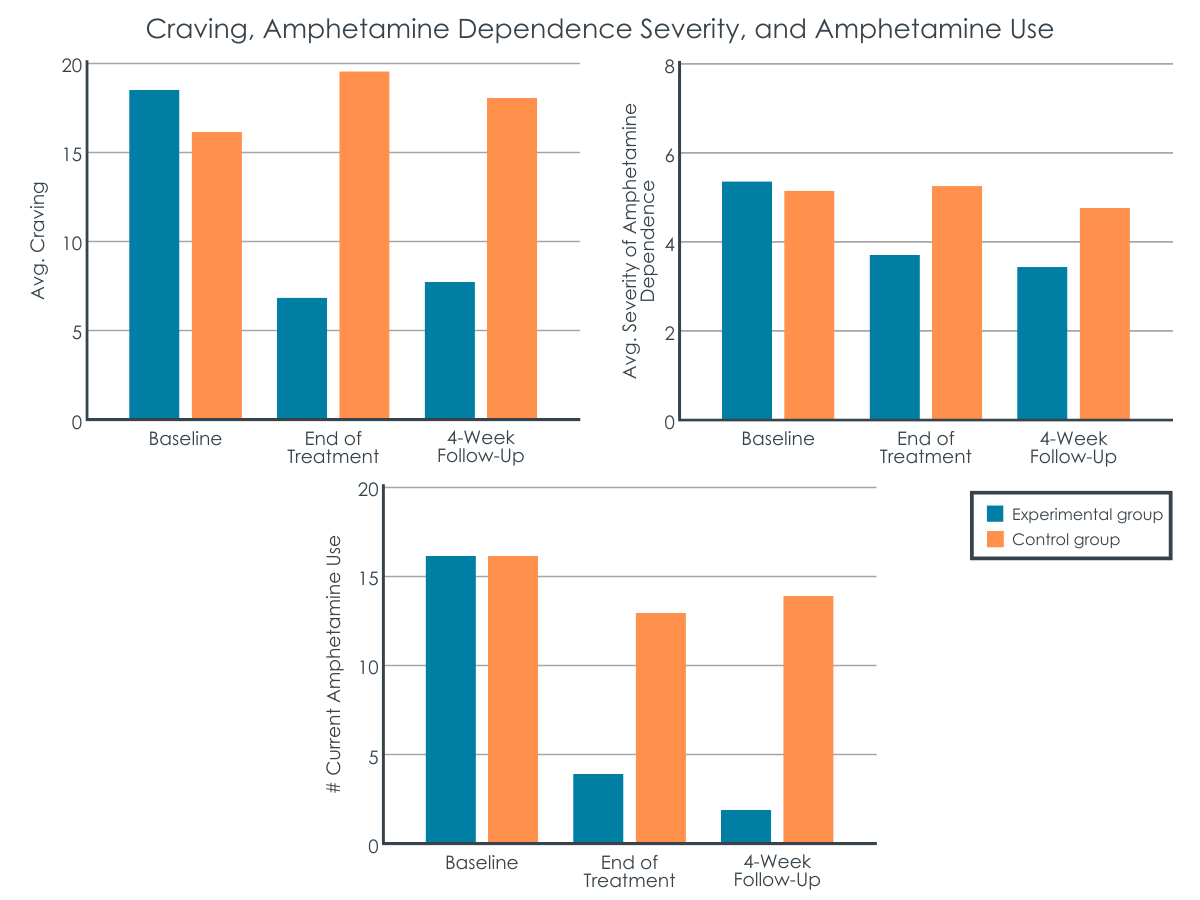
APatients receiving Heart Rate Variability Biofeedback experienced less craving.
At the 4-week follow-up, relative to controls, participants receiving Heart Rate Variability Biofeedback reported less craving (7 vs. 19 out of a total possible score of 100).
In terms of change in craving from study baseline, participants receiving Heart Rate Variability Biofeedback had, on average, an 11% reduction, versus control participants who did not meaningfully change in terms of craving through the four weeks of treatment.
At 8-week follow-up, groups were not meaningfully different in terms of craving, however, in terms of change in craving from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback maintained an average reduction of 11% reported at the 4-week follow-up, while control participant craving did not markedly change.
Patients receiving Heart Rate Variability Biofeedback endorsed less dependence severity.
At 4-week follow-up, participants receiving Heart Rate Variability Biofeedback had lower severity of amphetamine dependence compared to controls (3.8 vs. 5.3 out of a total possible score of 15).
Participants receiving Heart Rate Variability Biofeedback also demonstrated a greater reduction in dependence severity from study baseline to 4-week follow-up, with an average reduction in severity of amphetamine dependence of 11%, versus no meaningful change in dependence severity in controls.
At 8-week follow-up, groups were similar in terms of dependence severity scores. However, with regards to change from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback demonstrated an average severity of amphetamine dependence reduction of 13%, while control participants did not notably change on this measure.
Patients getting Heart Rate Variability Biofeedback had less substance use.
At 4-week follow-up, compared to controls, participants receiving Heart Rate Variability Biofeedback had less amphetamine use (4 vs. 13 tested positive at end of treatment).
In terms of change from baseline to 4-week follow-up, participants receiving Heart Rate Variability Biofeedback were less likely to test positive for amphetamine use (4 tested positive at end of treatment versus 16 at baseline), while control participants did not meaningfully change on this outcome during treatment (13 tested positive at end of treatment versus 16 at baseline).
At 8-week follow-up, participants who received Heart Rate Variability Biofeedback were less likely to have used amphetamines relative to controls (2 vs. 16 participants tested positive at 8-week follow-up). Regarding change from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback were less likely to test positive for amphetamine use (2 tested positive at 8-week follow-up versus 16 at baseline), while control participants did not markedly change in terms of this measure (14 tested positive at 8-week follow-up versus 16 at baseline).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Results from this study suggest Heart Rate Variability Biofeedback might enhance first-line treatments for mild-moderate amphetamine use disorder. As with other preliminary controlled trials on Heart Rate Variability Biofeedback for substance use disorder, the study authors observed meaningful reductions in craving, substance use disorder severity, and substance use.
Though Heart Rate Variability Biofeedback is generally thought of as a complementary intervention (rather than a first-line treatment), it will be interesting to see if future clinical trials suggest this intervention could serve as a stand-alone treatment. Also, because participants in this study had, on average, fairly low craving and mild-moderate substance use disorder severity at baseline, it is not clear from these findings whether these results would generalize to individuals with more severe amphetamine use disorder who more typically present to specialty SUD treatment services as well as to patients who are also using other substances – which is common (e.g., alcohol, cannabis, opioids).
Large-scale, gold-standard randomized controlled trials are needed before we can conclude Heart Rate Variability Biofeedback is efficacious for the treatment of substance use disorder, both as an adjunct to existing empirically supported treatments and as a stand-alone intervention. Also, this treatment may be particularly well-suited to some patients and not to others, and additional research will be needed to discover who may or may not be a good candidate for it.
The study only recruited males. Though previous Heart Rate Variability Biofeedback studies have not shown sex differences in treatment outcomes, future studies on Heart Rate Variability Biofeedback for substance use disorder should include women.
Amphetamine use disorder severity, and craving, were not especially severe in the study sample, and around half the sample appeared to not be using amphetamines at study baseline. Future studies will need to test this intervention in samples with greater problem severity to determine if it can benefit the spectrum of individuals with amphetamine use disorder.
Individuals using substances other than amphetamines and with common cooccurring mental disorders were excluded from the study. This limits the generalizability of the findings to the general population of individuals with amphetamine use disorder who commonly also use other substances and have cooccurring psychological conditions.
Urine testing for amphetamine use at 8-week follow-up would have only identified amphetamine use within the past 4-5 days. It is possible some participants who tested negative for amphetamine use at follow-up had used amphetamines over the follow-up period.
The follow-up period was 8 weeks. Future studies will need to assess the longer-term effects of Heart Rate Variability Biofeedback.
BOTTOM LINE
Though large, gold-standard randomized controlled trials are needed before we can know for certain if Heart Rate Variability Biofeedback benefits individuals seeking substance use disorder recovery, this small clinical trial among male outpatients with mild-moderate amphetamine use disorder suggests there may be benefits associated with this intervention. Given Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, is low cost, has no contraindications and is generally experienced as relaxing, there is little risk to adding this intervention in substance use disorder treatment programs. Future studies should explore if Heart Rate Variability Biofeedback can serve as a stand-alone treatment for substance use disorder as well as an addition to existing treatments.
For individuals and families seeking recovery: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line substance use disorder treatments. More research is needed, however, to determine if this intervention can serve as a stand-alone intervention. Because Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, is low cost, and is generally experienced as relaxing, there is little to no down-side to adding this practice to recovery activities like psychotherapy and mutual-help group participation.
For treatment professionals and treatment systems: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line treatments. More research is needed, however, to determine if this intervention can add meaningfully to, or stand alone as a substance use disorder treatment. Because Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, has no contraindications, is low cost, and is generally experienced as relaxing, there is little to no down-side in offering this practice as an addendum to first-line treatments.
For scientists: Preliminary studies suggest Heart Rate Variability Biofeedback can support individuals’ substance use disorder recovery when added to existing first-line treatments. Larger randomized controlled trials are needed, however, to support preliminary studies. Future studies should also explore if this intervention can stand alone as a substance use disorder treatment. Additionally, more research is needed to determine Heart Rate Variability Biofeedback’s therapeutic mechanism/s.
For policy makers: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line treatments. If shown to be effective, it will be important insurers be required to reimburse for these interventions so programs can offer, and patients can access, these interventions.
Heart Rate Variability Biofeedback is a breathing-based intervention that involves breathing at special frequencies that elicit immediate and dramatic changes in the cardiovascular system, including increased heart rate variability, which is a biomarker of health (higher variability reflects greater adaptive capacity and health). This intervention has been shown to reduce symptoms associated with a number of disorders including anxiety and depressive disorders, and post-traumatic stress disorder (PTSD). Based on these results, substance use disorder researchers have begun to explore if Heart Rate Variability Biofeedback could complement existing substance use disorder treatments.
Several small clinical trials have suggested Heart Rate Variability Biofeedback can assist substance use disorder recovery, particularly by reducing craving (see here for a review). At the same time, only one clinical trial to date has actually examined substance use outcomes, with Penzlin and colleagues finding Heart Rate Variability Biofeedback to be associated with lower alcohol use among those with alcohol use disorder, versus controls. Additionally, although previous studies have included individuals with a range of primary substances, no study to date has tested the utility of Heart Rate Variability Biofeedback specifically for the treatment of amphetamine use disorder.
To examine if Heart Rate Variability Biofeedback could potentially improve treatment outcomes among people with amphetamine use disorder, the authors of this paper tested a concise, 4-week Heart Rate Variability Biofeedback treatment protocol with individuals receiving outpatient treatment for amphetamine use disorder in Taiwan.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial that included 64 individuals engaged in outpatient treatment for amphetamine use disorder in which participants received either 4 weeks of Heart Rate Variability Biofeedback in addition to outpatient treatment-as-usual (experimental group), or treatment-as-usual only (control group).
Study inclusion criteria were: 1) being 20+ years of age, 2) male, 3) having mild, moderate, or severe DSM 5 amphetamine use disorder, 4) no co-occurring use of other substances, 5) no comorbid schizophrenia, major depressive disorder, or bipolar disorder, 6) no cardiovascular, lung, and neurological illnesses, and 7) having completed elementary school or higher.
Participants were assessed at study baseline, at 4-week follow-up (i.e., the end of the intervention), and at 8-week follow-up (i.e., 4 weeks after intervention completion). Study outcomes included craving, severity of amphetamine use disorder (measured with the Severity of Dependence Scale), and urine drug screening for amphetamine use.
The Heart Rate Variability Biofeedback intervention was delivered through weekly, 60-minute Heart Rate Variability Biofeedback training sessions, in which participants in the experimental group met with study coordinators and were taught to pace their breathing at special frequencies known to produce major increases in heart rate variability. Participants viewed their changing heart rate via an electrocardiogram device linked to a computer, which showed how their heart rate responded in real time to their paced breathing (i.e., biofeedback). Experimental participants were also instructed to practice 2 x 20-minute sessions per day using a handheld Heart Rate Variability Biofeedback device.
Treatment-as-usual, which all participants received, included once-weekly sessions of addiction focused, group Cognitive Behavioral Therapy over the 4 weeks.
Of the 64 study participants, 3 discontinued after study enrollment (1 experimental and 2 controls). The sample was on average 37 years old with relatively late initiation of amphetamine use at 30 years of age. All participants were male. On average, at baseline, the sample had mild to moderate amphetamine use disorder characterized by Severity of Dependence Scale scores of 5.3 out of a total possible score of 15.
WHAT DID THIS STUDY FIND?
APatients receiving Heart Rate Variability Biofeedback experienced less craving.
At the 4-week follow-up, relative to controls, participants receiving Heart Rate Variability Biofeedback reported less craving (7 vs. 19 out of a total possible score of 100).
In terms of change in craving from study baseline, participants receiving Heart Rate Variability Biofeedback had, on average, an 11% reduction, versus control participants who did not meaningfully change in terms of craving through the four weeks of treatment.
At 8-week follow-up, groups were not meaningfully different in terms of craving, however, in terms of change in craving from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback maintained an average reduction of 11% reported at the 4-week follow-up, while control participant craving did not markedly change.
Patients receiving Heart Rate Variability Biofeedback endorsed less dependence severity.
At 4-week follow-up, participants receiving Heart Rate Variability Biofeedback had lower severity of amphetamine dependence compared to controls (3.8 vs. 5.3 out of a total possible score of 15).
Participants receiving Heart Rate Variability Biofeedback also demonstrated a greater reduction in dependence severity from study baseline to 4-week follow-up, with an average reduction in severity of amphetamine dependence of 11%, versus no meaningful change in dependence severity in controls.
At 8-week follow-up, groups were similar in terms of dependence severity scores. However, with regards to change from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback demonstrated an average severity of amphetamine dependence reduction of 13%, while control participants did not notably change on this measure.
Patients getting Heart Rate Variability Biofeedback had less substance use.
At 4-week follow-up, compared to controls, participants receiving Heart Rate Variability Biofeedback had less amphetamine use (4 vs. 13 tested positive at end of treatment).
In terms of change from baseline to 4-week follow-up, participants receiving Heart Rate Variability Biofeedback were less likely to test positive for amphetamine use (4 tested positive at end of treatment versus 16 at baseline), while control participants did not meaningfully change on this outcome during treatment (13 tested positive at end of treatment versus 16 at baseline).
At 8-week follow-up, participants who received Heart Rate Variability Biofeedback were less likely to have used amphetamines relative to controls (2 vs. 16 participants tested positive at 8-week follow-up). Regarding change from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback were less likely to test positive for amphetamine use (2 tested positive at 8-week follow-up versus 16 at baseline), while control participants did not markedly change in terms of this measure (14 tested positive at 8-week follow-up versus 16 at baseline).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Results from this study suggest Heart Rate Variability Biofeedback might enhance first-line treatments for mild-moderate amphetamine use disorder. As with other preliminary controlled trials on Heart Rate Variability Biofeedback for substance use disorder, the study authors observed meaningful reductions in craving, substance use disorder severity, and substance use.
Though Heart Rate Variability Biofeedback is generally thought of as a complementary intervention (rather than a first-line treatment), it will be interesting to see if future clinical trials suggest this intervention could serve as a stand-alone treatment. Also, because participants in this study had, on average, fairly low craving and mild-moderate substance use disorder severity at baseline, it is not clear from these findings whether these results would generalize to individuals with more severe amphetamine use disorder who more typically present to specialty SUD treatment services as well as to patients who are also using other substances – which is common (e.g., alcohol, cannabis, opioids).
Large-scale, gold-standard randomized controlled trials are needed before we can conclude Heart Rate Variability Biofeedback is efficacious for the treatment of substance use disorder, both as an adjunct to existing empirically supported treatments and as a stand-alone intervention. Also, this treatment may be particularly well-suited to some patients and not to others, and additional research will be needed to discover who may or may not be a good candidate for it.
The study only recruited males. Though previous Heart Rate Variability Biofeedback studies have not shown sex differences in treatment outcomes, future studies on Heart Rate Variability Biofeedback for substance use disorder should include women.
Amphetamine use disorder severity, and craving, were not especially severe in the study sample, and around half the sample appeared to not be using amphetamines at study baseline. Future studies will need to test this intervention in samples with greater problem severity to determine if it can benefit the spectrum of individuals with amphetamine use disorder.
Individuals using substances other than amphetamines and with common cooccurring mental disorders were excluded from the study. This limits the generalizability of the findings to the general population of individuals with amphetamine use disorder who commonly also use other substances and have cooccurring psychological conditions.
Urine testing for amphetamine use at 8-week follow-up would have only identified amphetamine use within the past 4-5 days. It is possible some participants who tested negative for amphetamine use at follow-up had used amphetamines over the follow-up period.
The follow-up period was 8 weeks. Future studies will need to assess the longer-term effects of Heart Rate Variability Biofeedback.
BOTTOM LINE
Though large, gold-standard randomized controlled trials are needed before we can know for certain if Heart Rate Variability Biofeedback benefits individuals seeking substance use disorder recovery, this small clinical trial among male outpatients with mild-moderate amphetamine use disorder suggests there may be benefits associated with this intervention. Given Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, is low cost, has no contraindications and is generally experienced as relaxing, there is little risk to adding this intervention in substance use disorder treatment programs. Future studies should explore if Heart Rate Variability Biofeedback can serve as a stand-alone treatment for substance use disorder as well as an addition to existing treatments.
For individuals and families seeking recovery: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line substance use disorder treatments. More research is needed, however, to determine if this intervention can serve as a stand-alone intervention. Because Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, is low cost, and is generally experienced as relaxing, there is little to no down-side to adding this practice to recovery activities like psychotherapy and mutual-help group participation.
For treatment professionals and treatment systems: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line treatments. More research is needed, however, to determine if this intervention can add meaningfully to, or stand alone as a substance use disorder treatment. Because Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, has no contraindications, is low cost, and is generally experienced as relaxing, there is little to no down-side in offering this practice as an addendum to first-line treatments.
For scientists: Preliminary studies suggest Heart Rate Variability Biofeedback can support individuals’ substance use disorder recovery when added to existing first-line treatments. Larger randomized controlled trials are needed, however, to support preliminary studies. Future studies should also explore if this intervention can stand alone as a substance use disorder treatment. Additionally, more research is needed to determine Heart Rate Variability Biofeedback’s therapeutic mechanism/s.
For policy makers: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line treatments. If shown to be effective, it will be important insurers be required to reimburse for these interventions so programs can offer, and patients can access, these interventions.
Heart Rate Variability Biofeedback is a breathing-based intervention that involves breathing at special frequencies that elicit immediate and dramatic changes in the cardiovascular system, including increased heart rate variability, which is a biomarker of health (higher variability reflects greater adaptive capacity and health). This intervention has been shown to reduce symptoms associated with a number of disorders including anxiety and depressive disorders, and post-traumatic stress disorder (PTSD). Based on these results, substance use disorder researchers have begun to explore if Heart Rate Variability Biofeedback could complement existing substance use disorder treatments.
Several small clinical trials have suggested Heart Rate Variability Biofeedback can assist substance use disorder recovery, particularly by reducing craving (see here for a review). At the same time, only one clinical trial to date has actually examined substance use outcomes, with Penzlin and colleagues finding Heart Rate Variability Biofeedback to be associated with lower alcohol use among those with alcohol use disorder, versus controls. Additionally, although previous studies have included individuals with a range of primary substances, no study to date has tested the utility of Heart Rate Variability Biofeedback specifically for the treatment of amphetamine use disorder.
To examine if Heart Rate Variability Biofeedback could potentially improve treatment outcomes among people with amphetamine use disorder, the authors of this paper tested a concise, 4-week Heart Rate Variability Biofeedback treatment protocol with individuals receiving outpatient treatment for amphetamine use disorder in Taiwan.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial that included 64 individuals engaged in outpatient treatment for amphetamine use disorder in which participants received either 4 weeks of Heart Rate Variability Biofeedback in addition to outpatient treatment-as-usual (experimental group), or treatment-as-usual only (control group).
Study inclusion criteria were: 1) being 20+ years of age, 2) male, 3) having mild, moderate, or severe DSM 5 amphetamine use disorder, 4) no co-occurring use of other substances, 5) no comorbid schizophrenia, major depressive disorder, or bipolar disorder, 6) no cardiovascular, lung, and neurological illnesses, and 7) having completed elementary school or higher.
Participants were assessed at study baseline, at 4-week follow-up (i.e., the end of the intervention), and at 8-week follow-up (i.e., 4 weeks after intervention completion). Study outcomes included craving, severity of amphetamine use disorder (measured with the Severity of Dependence Scale), and urine drug screening for amphetamine use.
The Heart Rate Variability Biofeedback intervention was delivered through weekly, 60-minute Heart Rate Variability Biofeedback training sessions, in which participants in the experimental group met with study coordinators and were taught to pace their breathing at special frequencies known to produce major increases in heart rate variability. Participants viewed their changing heart rate via an electrocardiogram device linked to a computer, which showed how their heart rate responded in real time to their paced breathing (i.e., biofeedback). Experimental participants were also instructed to practice 2 x 20-minute sessions per day using a handheld Heart Rate Variability Biofeedback device.
Treatment-as-usual, which all participants received, included once-weekly sessions of addiction focused, group Cognitive Behavioral Therapy over the 4 weeks.
Of the 64 study participants, 3 discontinued after study enrollment (1 experimental and 2 controls). The sample was on average 37 years old with relatively late initiation of amphetamine use at 30 years of age. All participants were male. On average, at baseline, the sample had mild to moderate amphetamine use disorder characterized by Severity of Dependence Scale scores of 5.3 out of a total possible score of 15.
WHAT DID THIS STUDY FIND?
APatients receiving Heart Rate Variability Biofeedback experienced less craving.
At the 4-week follow-up, relative to controls, participants receiving Heart Rate Variability Biofeedback reported less craving (7 vs. 19 out of a total possible score of 100).
In terms of change in craving from study baseline, participants receiving Heart Rate Variability Biofeedback had, on average, an 11% reduction, versus control participants who did not meaningfully change in terms of craving through the four weeks of treatment.
At 8-week follow-up, groups were not meaningfully different in terms of craving, however, in terms of change in craving from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback maintained an average reduction of 11% reported at the 4-week follow-up, while control participant craving did not markedly change.
Patients receiving Heart Rate Variability Biofeedback endorsed less dependence severity.
At 4-week follow-up, participants receiving Heart Rate Variability Biofeedback had lower severity of amphetamine dependence compared to controls (3.8 vs. 5.3 out of a total possible score of 15).
Participants receiving Heart Rate Variability Biofeedback also demonstrated a greater reduction in dependence severity from study baseline to 4-week follow-up, with an average reduction in severity of amphetamine dependence of 11%, versus no meaningful change in dependence severity in controls.
At 8-week follow-up, groups were similar in terms of dependence severity scores. However, with regards to change from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback demonstrated an average severity of amphetamine dependence reduction of 13%, while control participants did not notably change on this measure.
Patients getting Heart Rate Variability Biofeedback had less substance use.
At 4-week follow-up, compared to controls, participants receiving Heart Rate Variability Biofeedback had less amphetamine use (4 vs. 13 tested positive at end of treatment).
In terms of change from baseline to 4-week follow-up, participants receiving Heart Rate Variability Biofeedback were less likely to test positive for amphetamine use (4 tested positive at end of treatment versus 16 at baseline), while control participants did not meaningfully change on this outcome during treatment (13 tested positive at end of treatment versus 16 at baseline).
At 8-week follow-up, participants who received Heart Rate Variability Biofeedback were less likely to have used amphetamines relative to controls (2 vs. 16 participants tested positive at 8-week follow-up). Regarding change from baseline to 8-week follow-up, participants receiving Heart Rate Variability Biofeedback were less likely to test positive for amphetamine use (2 tested positive at 8-week follow-up versus 16 at baseline), while control participants did not markedly change in terms of this measure (14 tested positive at 8-week follow-up versus 16 at baseline).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Results from this study suggest Heart Rate Variability Biofeedback might enhance first-line treatments for mild-moderate amphetamine use disorder. As with other preliminary controlled trials on Heart Rate Variability Biofeedback for substance use disorder, the study authors observed meaningful reductions in craving, substance use disorder severity, and substance use.
Though Heart Rate Variability Biofeedback is generally thought of as a complementary intervention (rather than a first-line treatment), it will be interesting to see if future clinical trials suggest this intervention could serve as a stand-alone treatment. Also, because participants in this study had, on average, fairly low craving and mild-moderate substance use disorder severity at baseline, it is not clear from these findings whether these results would generalize to individuals with more severe amphetamine use disorder who more typically present to specialty SUD treatment services as well as to patients who are also using other substances – which is common (e.g., alcohol, cannabis, opioids).
Large-scale, gold-standard randomized controlled trials are needed before we can conclude Heart Rate Variability Biofeedback is efficacious for the treatment of substance use disorder, both as an adjunct to existing empirically supported treatments and as a stand-alone intervention. Also, this treatment may be particularly well-suited to some patients and not to others, and additional research will be needed to discover who may or may not be a good candidate for it.
The study only recruited males. Though previous Heart Rate Variability Biofeedback studies have not shown sex differences in treatment outcomes, future studies on Heart Rate Variability Biofeedback for substance use disorder should include women.
Amphetamine use disorder severity, and craving, were not especially severe in the study sample, and around half the sample appeared to not be using amphetamines at study baseline. Future studies will need to test this intervention in samples with greater problem severity to determine if it can benefit the spectrum of individuals with amphetamine use disorder.
Individuals using substances other than amphetamines and with common cooccurring mental disorders were excluded from the study. This limits the generalizability of the findings to the general population of individuals with amphetamine use disorder who commonly also use other substances and have cooccurring psychological conditions.
Urine testing for amphetamine use at 8-week follow-up would have only identified amphetamine use within the past 4-5 days. It is possible some participants who tested negative for amphetamine use at follow-up had used amphetamines over the follow-up period.
The follow-up period was 8 weeks. Future studies will need to assess the longer-term effects of Heart Rate Variability Biofeedback.
BOTTOM LINE
Though large, gold-standard randomized controlled trials are needed before we can know for certain if Heart Rate Variability Biofeedback benefits individuals seeking substance use disorder recovery, this small clinical trial among male outpatients with mild-moderate amphetamine use disorder suggests there may be benefits associated with this intervention. Given Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, is low cost, has no contraindications and is generally experienced as relaxing, there is little risk to adding this intervention in substance use disorder treatment programs. Future studies should explore if Heart Rate Variability Biofeedback can serve as a stand-alone treatment for substance use disorder as well as an addition to existing treatments.
For individuals and families seeking recovery: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line substance use disorder treatments. More research is needed, however, to determine if this intervention can serve as a stand-alone intervention. Because Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, is low cost, and is generally experienced as relaxing, there is little to no down-side to adding this practice to recovery activities like psychotherapy and mutual-help group participation.
For treatment professionals and treatment systems: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line treatments. More research is needed, however, to determine if this intervention can add meaningfully to, or stand alone as a substance use disorder treatment. Because Heart Rate Variability Biofeedback has no adverse side effects, is safe to practice, has no contraindications, is low cost, and is generally experienced as relaxing, there is little to no down-side in offering this practice as an addendum to first-line treatments.
For scientists: Preliminary studies suggest Heart Rate Variability Biofeedback can support individuals’ substance use disorder recovery when added to existing first-line treatments. Larger randomized controlled trials are needed, however, to support preliminary studies. Future studies should also explore if this intervention can stand alone as a substance use disorder treatment. Additionally, more research is needed to determine Heart Rate Variability Biofeedback’s therapeutic mechanism/s.
For policy makers: Heart Rate Variability Biofeedback is a breathing-based intervention that might enhance the effects of existing first-line treatments. If shown to be effective, it will be important insurers be required to reimburse for these interventions so programs can offer, and patients can access, these interventions.