Majority of heavy drinkers improve, but those who are abstinent and engaged with health care have more stable change
Research that goes beyond an initial resolution of harmful and hazardous drinking to how these changes are maintained over the long-term can enhance health-related recommendations and guidelines. In this study, researchers investigated factors associated with achieving both early and sustained cessation of heavy drinking in a large primary care sample.
Unhealthy alcohol use can range from risky drinking to alcohol use disorder including alcohol addiction. Such drinking can have a negative impact on health, including disruptions to brain, heart, liver, pancreas, and the immune functioning as well as cause social and familial consequences. In the United States, alcohol use is a leading cause of death and is estimated to cost the United States over $249 billion annually. Although many studies target individuals with alcohol use disorder in treatment and recovery support service settings, much of the disease burden from alcohol is caused by excessive drinking, rather than alcohol use disorder, per se, as this represents a much large number of people. Little is known, however, on how heavy drinkers change, such as reduce or abstain from drinking, in the 1st year after they screen positive for heavy drinking. Furthermore, evidence is lacking that explores what factors predict sustained cessation of heavy drinking or abstinence over time. This study sought to identify what characteristics (e.g., race/ethnicity) and experiences (e.g., addiction treatment) are associated with achieving cessation of heavy drinking over 5 years using a large sample of adults engaged in primary care.
HOW WAS THIS STUDY CONDUCTED?
In this retrospective study, researchers analyzed electronic health records of adults in the Kaiser Permanente Northern California (KPNC) health care network that screened positive for heavy drinking during a routine primary care visit that took place between June 1st, 2013, and May 31st, 2014. The KPNC network serves 4.3 million adults (~1/3 of the Northern Californian population) and has systematically screened for heavy drinking in adult primary care with approximately 80% of its members successfully screened. The main outcome of this study was the cessation of heavy drinking. Screening for heavy drinking consisted of a medical staff member asking three questions: (1) ‘How many times in the past 3 months have you had five/four or more drinks containing alcohol in a day?’ for men aged 18-65 and men aged ≥ 66 or women respectively; (2) ‘On average, how many days per week do you have an alcoholic drink?’, and (3) ‘On a typical drinking day, how many drinks do you have?’. Heavy drinking was positive if a person exceeded either daily (5+ drinks for men aged 18-66 or 4+ for men aged ≥66 and women) or weekly limits (14 drinks/week for men aged 18-66 or 7 drinks/week for men aged ≥66 and women), based on the National Institute of Alcohol Abuse and Alcoholism (NIAAA) guidelines at the time of the initial screening. Early cessation of heavy alcohol use was defined as reporting lower-risk drinking (no heavy drinking days or weeks in the past 3 months) or abstinence at all screenings up to 1-year after the first positive heavy drinking screening. Sustained cessation of heavy alcohol use was defined as obtaining early cessation and reporting lower drinking or abstinence at all screenings up to the 5-year follow-up screening. Possible predictors were also collected and included socio-demographic characteristics, smoking status, drinking level (e.g., exceeding daily, weekly, or both daily and weekly heavy drinking limits), psychiatric disorders, alcohol and other substance use disorders, psychiatric or addiction treatment, routine (i.e., annual) primary care visits, and the type of early cessation (low-risk drinking or abstinence).
All enrollees that screened positive for heavy drinking during the index period (June 1st, 2013, and May 31st, 2014) were eligible to be included. During the 1-year eligibility period, 200,458 adults screened positive for heavy drinking. For each adult, all alcohol screens for the following 63 months were collected. The screenings closest to 1-year and 5-year post index screening were used for early and sustained cessation markers respectively. Approximately 46% of these patients were lost to follow-up due to death, disenrollment from Kaiser Permanente, or not having a 1 year screening, which resulted in 85,434 adults with observed alcohol use data that were used in the final analyses. Among those adults, 53,916 achieved early cessation and were eligible for the sustained cessation analysis, resulting in 19,200 adults with complete outcome data 5 years after index screening. The study accounted statistically for differences in attrition (i.e., likelihood of dropping out of the care during the study window).
Of the 85,434 adults in the analytical sample: 34,761 (40.7%) were females and 28,853 (33.8%) identified as non-white. The average age was 50.3 and 11,914 (13.9%) reported current smoking. Most – 50,193 (58.8%) – exceeded only daily drinking limits, while 20,835 (24.4%) exceeded only weekly limits and 14,406 (16.9%) exceeded both daily and weekly limits. There were also 4,057 (4.7%) adults who met criteria for an alcohol use disorder.
WHAT DID THIS STUDY FIND?
Most that screened positive for heavy alcohol use achieved early cessation.
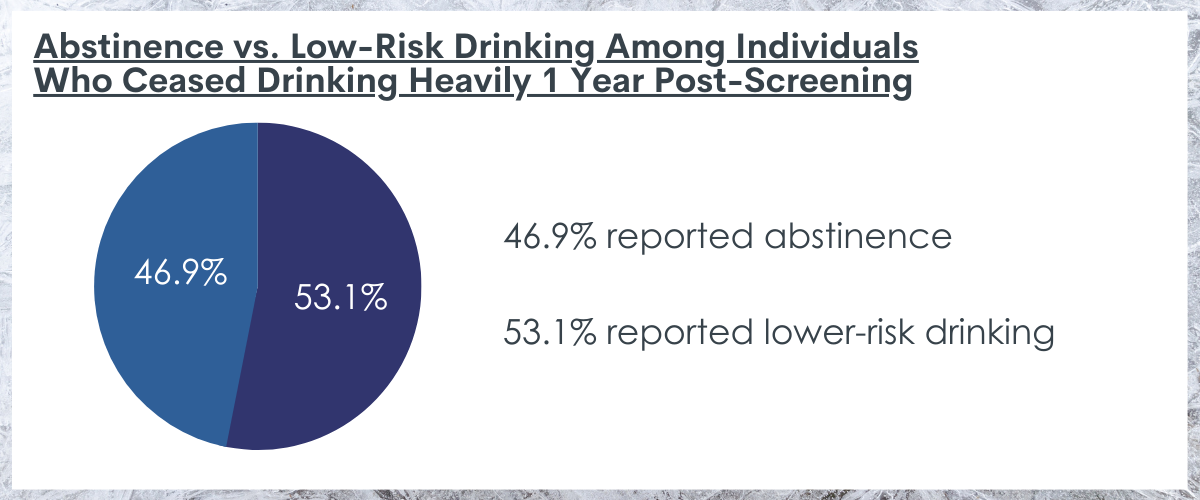
A total of 53,916 (63.1%) adults that screened positive for heavy drinking achieved early cessation. Among those that achieved early cessation, 25,289 (46.9%) reported abstinence and 28,627 (53.1%) reported lower-risk drinking. Similarly, close to 2/3 (60.0%, 11,539) of the 19,200 that achieved early cessation and had outcome data reported sustained heavy drinking cessation.
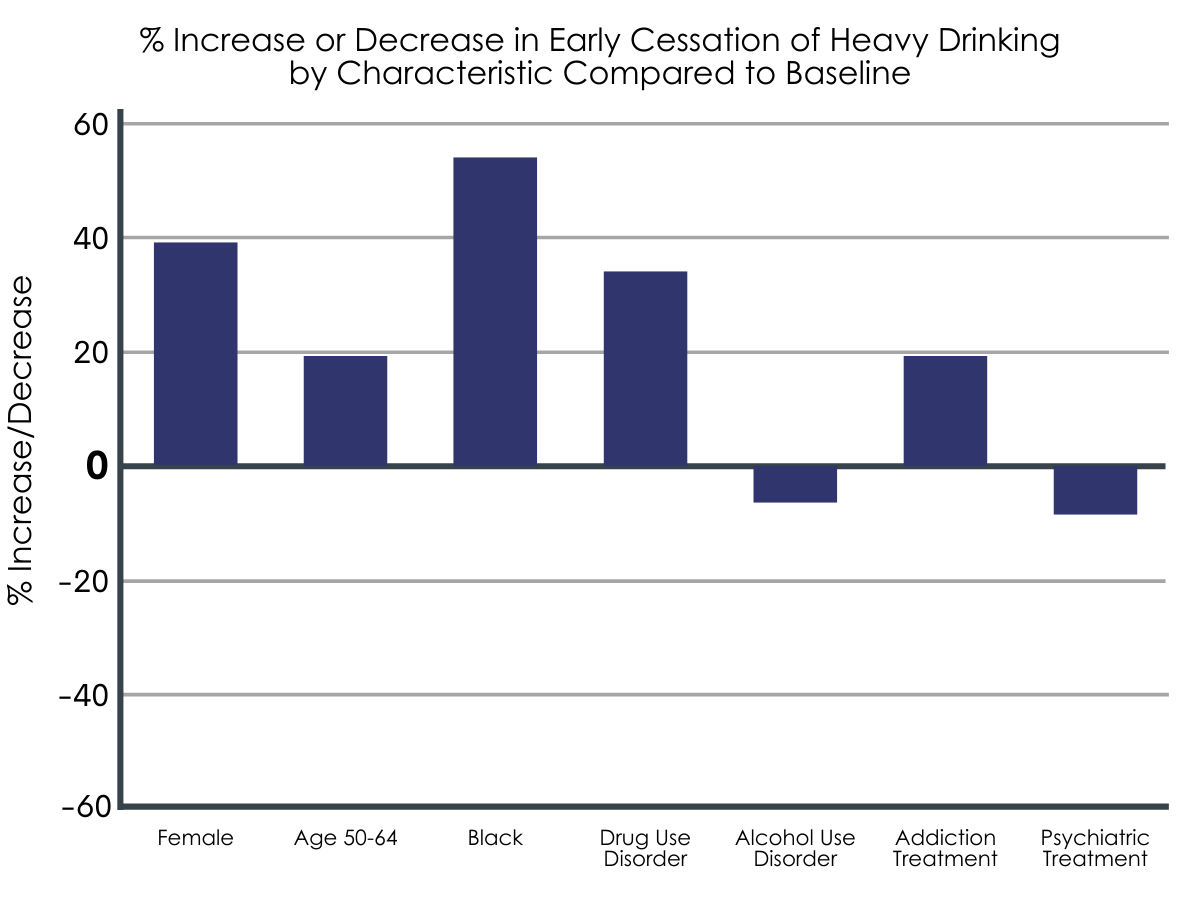
Early cessation was more likely among females compared to males and those that did not identify as White.
The researchers found that several demographic characteristics and experiences were linked with higher odds of achieving early cessation. However, those identifying as female compared to male and/or Asian, Native Hawaiian, or Pacific Islander, Black, Latinx/Hispanic, or Native American compared to white were the strongest predictors.
Engagement in services (primary care and addiction treatment) was associated with sustained (5-year) cessation.
Among the 19,200 adults that achieved early (1-year) heavy drinking cessation, those that participated in routine (i.e., annual) primary care had a 57% increase in odds of achieving sustained (5-year) cessation compared to those that did not have routine primary care.
Surprisingly, individuals that attended psychiatric treatment within the first year after being identified with heavy drinking had lower odds of early cessation compared to those that did not. Moreover, adults that attended psychiatric treatment within the first year after positive heavy drinking screening did not differ in odds of achieving sustained cessation compared to those that did not attend psychiatric treatment. Attending addiction treatment, however, was associated with a 19% and 41% increase in odds of achieving early and sustained cessation respectively. Addiction treatment was one of the stronger predictors of sustained heavy drinking cessation.
Abstinence but not Alcohol use disorder diagnosis linked to early or sustained cessation.
Among all adults that screened positive for heavy drinking, 4.7% (4,057) were also diagnosed with an alcohol use disorder. Those with an alcohol use disorder diagnosis were no more likely or less likely to achieve early or sustained cessation of heavy drinking.
Adults that reported abstinence at 1-year were more likely to achieve sustained cessation compared to those reporting low-risk drinking. This effect was even larger among those with alcohol use disorder. For those with alcohol use disorder, abstinence was associated with 2.27 greater odds of sustaining cessation. For those without alcohol use disorder the odds ratio was the same as for the overall sample.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Nationwide, there are tens of millions of individuals that have resolved a substance use problem, and over half of those identify alcohol as the primary problem substance. However, most individuals do not seek or receive help for mild to moderate problematic drinking, highlighting the need to understand how individuals might resolve heavy drinking including. The need includes both those who do and do not attend treatment, and more importantly as it has been studied less often, how these individuals sustain this change over time. The researchers in this study explored what characteristics and behavioral health service utilization predict early (1-year) and sustained (5-year) cessation of heavy drinking. They found that 2/3 of adults that were identified through screening achieved early cessation of heavy drinking. This is higher than previous studies and suggests that screening during primary care may help identify alcohol problems before severity increases and link to needed treatments. Furthermore, the researchers found that routine primary care visits, independent of other factors, was the strongest predictor of sustained cessation. The impact of primary care may be especially useful for those without high severity drinking issues or alcohol use disorder. Primary care may be uniquely situated to address overall medical needs impacting drinking behaviors, identify and treat heavy drinking relapse, promote healthy lifestyles, and link to targeted services. It is also possible that attending routine primary care reflects a larger commitment to healthy lifestyle and some factors that were not measured are responsible for individuals’ drinking change and ability to sustain that change over time.
The type of early drinking cessation mattered for sustaining cessation. Those who reported abstinence at 1-year were more likely to achieve sustained cessation compared to those who reported lower-risk drinking. Previous research has shown that some individuals are able to drink and function as well as those that are abstinent in some domains such as psychological functioning, employment, life satisfaction, and mental health, the greater health risks of their heavier drinking notwithstanding. So, for some, lower risk drinking or lifestyle changes may be most appropriate. In this study, however, it was found that adults who reported abstinence at 1-year were more likely to report sustained cessation of heavy drinking after 5 years compared adults engaging in low-risk drinking. The long-term benefits of abstinence found in this study mirrors findings from the National Epidemiologic Survey on Alcohol Related Conditions (NESARC), a nationally representative sample of U.S. adults. Researchers analyzing the NESCARC data found that abstinence represented the most stable form of remission from alcohol dependence compared to high- and low-risk drinkers after 3 years. Furthermore, researchers exploring a Dutch sample of adults also found that any alcohol use among those in alcohol use disorder remission was a significant risk factor for relapse to active alcohol use disorder. One contribution of the work done here is the inclusion of adults identified with heavy drinking behavior yet do not meet alcohol use disorder criteria; while showing that half of heavy drinkers stop drinking heavily through a low-risk drinking pathway, this study also highlights the greater stability of an abstinence approach to risk reduction and cessation of heavy drinking over time. This finding aligns with previous work highlighting the increased benefits of abstinence.
The electronic health record data obtained for this study was not collected for research purposes. Thus, the analysis presented here relies on both patients to have access to health care and medical staff to administer the alcohol screening and collect other key demographics.
The authors relied on retrospective recall of past 90-day alcohol use to calculate their outcome variable. Although such methods have been used extensively, it has limitations to the extent that individuals’ recall is imperfect. Additionally, there is possible response bias – the tendency to respond in ways that are perceived to be socially desirable.
The data from this study were gathered from adults Northern California members of Kaiser Permanente and replicating to the general US population may be of added value.
The data do not reflect the severity of nor consequences related to alcohol use. Those with higher severity (exclusive of those with alcohol use disorder) or specific consequences (i.e., legal repercussions) may reflect different characteristics related to early and sustained cessation of heavy drinking.
There was an extensive number of participants lost to follow up, which may have influenced findings as sicker patients are more likely to drop out of such care and studies. However, the researchers did employ a rigorous statistical technique to try to account for the differences between those retained for follow up and those lost to follow up. Future studies should replicate findings with a lower attrition rate.
Health and well-being outcomes were not assessed. Thus, the researchers are unable to examine whether early or sustained cessation of heavy drinking for this sample was linked to improvements in health or well-being. However, previous work has shown this to be the case.
BOTTOM LINE
Two-thirds of adults that were able to be followed up in this study that screened positive initially for heavy drinking in this retrospective cohort study of primary care patients achieved early (1-year) cessation of heavy drinking and of those that achieve early cessation, nearly 2/3 reported sustained (5-year) heavy drinking cessation. Routine primary care was the strongest predictor of sustained cessation. Addiction treatment was also one of the stronger predictors of both early and sustained cessation. Abstinence was linked to higher odds of sustained (5-year) heavy drinking cessation, and this effect was even bigger among those with alcohol use disorder. This study explored the types of factors that predict cessation of heavy drinking as well as what factors predict its stability over time in a primary care sample of adults.
For individuals and families seeking recovery: This study explored predictors of early (1-year) and sustained (5-year) heavy drinking cessation. They found that nearly 2/3 of adults that reported heavy drinking achieved early cessation. Two of the strongest predictors of sustained cessation were receiving addiction treatment within the first year after positive screening and continued routine primary care. Although many stop drinking heavily via low-risk drinking, abstinence tends to be more stable over the long term. If you or a loved one has access to primary care and addiction treatment, it is unlikely to harm and it will likely help achieve alcohol use, health, and wellness goals.
For treatment professionals and treatment systems: The Screening, Brief Intervention, and Referral to Treatment initiative, commonly referred to as SBIRT, is a public health priority. Although previous findings refute the effectiveness of SBIRT linking to treatment, the researchers in this study present evidence of the role that screening for heavy alcohol use may have in real world clinical settings. Most of the adults that screened positive did achieve early cessation of heavy alcohol use, and those that did attend addiction treatment were more likely to reported sustained cessation 5 years after positive screening. Treatment professionals and treatment systems should consider further implementation and refinement of SBIRT in routine care. Furthermore, increasing access to addiction treatment (e.g., pharmacotherapy, flexible outpatient services) may empower primary care providers to meet adults where they are at and link them with the most appropriate care.
For scientists:Researchers in this retrospective cohort study assessed predictors of early (1-year) and sustained (5-year) heavy drinking cessation following a positive screen for engaging in heavy drinking. Routine primary care was the strongest predictor of sustained cessation, with addiction treatment one of the strongest predictors for both early and sustained cessation. Future research should consider exploring what types of addiction services (e.g., pharmacotherapy, outpatient) are most suited for adults with varying profiles engaging in heavy drinking. Additional research should investigate how drinking levels (high-risk, low-risk, abstinence) are linked to health outcomes including but not limited to alcohol among adults engaged in primary care.
For policy makers: Heavy alcohol use and associated problems beget significant cost in premature mortality, disability and lost economic productivity, criminal justice, and health care. This study found that not only is cessation of heavy alcohol use possible among adults engaged in primary care, but it is more likely among those that attend routine primary care and receive addiction treatment. Furthermore, this study explored what factors sustained this change over time. Policy makers may consider funding work that specifically targets this group and for fiscal allocations that may help individuals sustain change over time (e.g., resources to support long-term primary care engagement, such as Medicare, Medicaid, and reduced barriers to primary care visits).
Unhealthy alcohol use can range from risky drinking to alcohol use disorder including alcohol addiction. Such drinking can have a negative impact on health, including disruptions to brain, heart, liver, pancreas, and the immune functioning as well as cause social and familial consequences. In the United States, alcohol use is a leading cause of death and is estimated to cost the United States over $249 billion annually. Although many studies target individuals with alcohol use disorder in treatment and recovery support service settings, much of the disease burden from alcohol is caused by excessive drinking, rather than alcohol use disorder, per se, as this represents a much large number of people. Little is known, however, on how heavy drinkers change, such as reduce or abstain from drinking, in the 1st year after they screen positive for heavy drinking. Furthermore, evidence is lacking that explores what factors predict sustained cessation of heavy drinking or abstinence over time. This study sought to identify what characteristics (e.g., race/ethnicity) and experiences (e.g., addiction treatment) are associated with achieving cessation of heavy drinking over 5 years using a large sample of adults engaged in primary care.
HOW WAS THIS STUDY CONDUCTED?
In this retrospective study, researchers analyzed electronic health records of adults in the Kaiser Permanente Northern California (KPNC) health care network that screened positive for heavy drinking during a routine primary care visit that took place between June 1st, 2013, and May 31st, 2014. The KPNC network serves 4.3 million adults (~1/3 of the Northern Californian population) and has systematically screened for heavy drinking in adult primary care with approximately 80% of its members successfully screened. The main outcome of this study was the cessation of heavy drinking. Screening for heavy drinking consisted of a medical staff member asking three questions: (1) ‘How many times in the past 3 months have you had five/four or more drinks containing alcohol in a day?’ for men aged 18-65 and men aged ≥ 66 or women respectively; (2) ‘On average, how many days per week do you have an alcoholic drink?’, and (3) ‘On a typical drinking day, how many drinks do you have?’. Heavy drinking was positive if a person exceeded either daily (5+ drinks for men aged 18-66 or 4+ for men aged ≥66 and women) or weekly limits (14 drinks/week for men aged 18-66 or 7 drinks/week for men aged ≥66 and women), based on the National Institute of Alcohol Abuse and Alcoholism (NIAAA) guidelines at the time of the initial screening. Early cessation of heavy alcohol use was defined as reporting lower-risk drinking (no heavy drinking days or weeks in the past 3 months) or abstinence at all screenings up to 1-year after the first positive heavy drinking screening. Sustained cessation of heavy alcohol use was defined as obtaining early cessation and reporting lower drinking or abstinence at all screenings up to the 5-year follow-up screening. Possible predictors were also collected and included socio-demographic characteristics, smoking status, drinking level (e.g., exceeding daily, weekly, or both daily and weekly heavy drinking limits), psychiatric disorders, alcohol and other substance use disorders, psychiatric or addiction treatment, routine (i.e., annual) primary care visits, and the type of early cessation (low-risk drinking or abstinence).
All enrollees that screened positive for heavy drinking during the index period (June 1st, 2013, and May 31st, 2014) were eligible to be included. During the 1-year eligibility period, 200,458 adults screened positive for heavy drinking. For each adult, all alcohol screens for the following 63 months were collected. The screenings closest to 1-year and 5-year post index screening were used for early and sustained cessation markers respectively. Approximately 46% of these patients were lost to follow-up due to death, disenrollment from Kaiser Permanente, or not having a 1 year screening, which resulted in 85,434 adults with observed alcohol use data that were used in the final analyses. Among those adults, 53,916 achieved early cessation and were eligible for the sustained cessation analysis, resulting in 19,200 adults with complete outcome data 5 years after index screening. The study accounted statistically for differences in attrition (i.e., likelihood of dropping out of the care during the study window).
Of the 85,434 adults in the analytical sample: 34,761 (40.7%) were females and 28,853 (33.8%) identified as non-white. The average age was 50.3 and 11,914 (13.9%) reported current smoking. Most – 50,193 (58.8%) – exceeded only daily drinking limits, while 20,835 (24.4%) exceeded only weekly limits and 14,406 (16.9%) exceeded both daily and weekly limits. There were also 4,057 (4.7%) adults who met criteria for an alcohol use disorder.
WHAT DID THIS STUDY FIND?
Most that screened positive for heavy alcohol use achieved early cessation.
A total of 53,916 (63.1%) adults that screened positive for heavy drinking achieved early cessation. Among those that achieved early cessation, 25,289 (46.9%) reported abstinence and 28,627 (53.1%) reported lower-risk drinking. Similarly, close to 2/3 (60.0%, 11,539) of the 19,200 that achieved early cessation and had outcome data reported sustained heavy drinking cessation.
Early cessation was more likely among females compared to males and those that did not identify as White.
The researchers found that several demographic characteristics and experiences were linked with higher odds of achieving early cessation. However, those identifying as female compared to male and/or Asian, Native Hawaiian, or Pacific Islander, Black, Latinx/Hispanic, or Native American compared to white were the strongest predictors.
Engagement in services (primary care and addiction treatment) was associated with sustained (5-year) cessation.
Among the 19,200 adults that achieved early (1-year) heavy drinking cessation, those that participated in routine (i.e., annual) primary care had a 57% increase in odds of achieving sustained (5-year) cessation compared to those that did not have routine primary care.
Surprisingly, individuals that attended psychiatric treatment within the first year after being identified with heavy drinking had lower odds of early cessation compared to those that did not. Moreover, adults that attended psychiatric treatment within the first year after positive heavy drinking screening did not differ in odds of achieving sustained cessation compared to those that did not attend psychiatric treatment. Attending addiction treatment, however, was associated with a 19% and 41% increase in odds of achieving early and sustained cessation respectively. Addiction treatment was one of the stronger predictors of sustained heavy drinking cessation.
Abstinence but not Alcohol use disorder diagnosis linked to early or sustained cessation.
Among all adults that screened positive for heavy drinking, 4.7% (4,057) were also diagnosed with an alcohol use disorder. Those with an alcohol use disorder diagnosis were no more likely or less likely to achieve early or sustained cessation of heavy drinking.
Adults that reported abstinence at 1-year were more likely to achieve sustained cessation compared to those reporting low-risk drinking. This effect was even larger among those with alcohol use disorder. For those with alcohol use disorder, abstinence was associated with 2.27 greater odds of sustaining cessation. For those without alcohol use disorder the odds ratio was the same as for the overall sample.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Nationwide, there are tens of millions of individuals that have resolved a substance use problem, and over half of those identify alcohol as the primary problem substance. However, most individuals do not seek or receive help for mild to moderate problematic drinking, highlighting the need to understand how individuals might resolve heavy drinking including. The need includes both those who do and do not attend treatment, and more importantly as it has been studied less often, how these individuals sustain this change over time. The researchers in this study explored what characteristics and behavioral health service utilization predict early (1-year) and sustained (5-year) cessation of heavy drinking. They found that 2/3 of adults that were identified through screening achieved early cessation of heavy drinking. This is higher than previous studies and suggests that screening during primary care may help identify alcohol problems before severity increases and link to needed treatments. Furthermore, the researchers found that routine primary care visits, independent of other factors, was the strongest predictor of sustained cessation. The impact of primary care may be especially useful for those without high severity drinking issues or alcohol use disorder. Primary care may be uniquely situated to address overall medical needs impacting drinking behaviors, identify and treat heavy drinking relapse, promote healthy lifestyles, and link to targeted services. It is also possible that attending routine primary care reflects a larger commitment to healthy lifestyle and some factors that were not measured are responsible for individuals’ drinking change and ability to sustain that change over time.
The type of early drinking cessation mattered for sustaining cessation. Those who reported abstinence at 1-year were more likely to achieve sustained cessation compared to those who reported lower-risk drinking. Previous research has shown that some individuals are able to drink and function as well as those that are abstinent in some domains such as psychological functioning, employment, life satisfaction, and mental health, the greater health risks of their heavier drinking notwithstanding. So, for some, lower risk drinking or lifestyle changes may be most appropriate. In this study, however, it was found that adults who reported abstinence at 1-year were more likely to report sustained cessation of heavy drinking after 5 years compared adults engaging in low-risk drinking. The long-term benefits of abstinence found in this study mirrors findings from the National Epidemiologic Survey on Alcohol Related Conditions (NESARC), a nationally representative sample of U.S. adults. Researchers analyzing the NESCARC data found that abstinence represented the most stable form of remission from alcohol dependence compared to high- and low-risk drinkers after 3 years. Furthermore, researchers exploring a Dutch sample of adults also found that any alcohol use among those in alcohol use disorder remission was a significant risk factor for relapse to active alcohol use disorder. One contribution of the work done here is the inclusion of adults identified with heavy drinking behavior yet do not meet alcohol use disorder criteria; while showing that half of heavy drinkers stop drinking heavily through a low-risk drinking pathway, this study also highlights the greater stability of an abstinence approach to risk reduction and cessation of heavy drinking over time. This finding aligns with previous work highlighting the increased benefits of abstinence.
The electronic health record data obtained for this study was not collected for research purposes. Thus, the analysis presented here relies on both patients to have access to health care and medical staff to administer the alcohol screening and collect other key demographics.
The authors relied on retrospective recall of past 90-day alcohol use to calculate their outcome variable. Although such methods have been used extensively, it has limitations to the extent that individuals’ recall is imperfect. Additionally, there is possible response bias – the tendency to respond in ways that are perceived to be socially desirable.
The data from this study were gathered from adults Northern California members of Kaiser Permanente and replicating to the general US population may be of added value.
The data do not reflect the severity of nor consequences related to alcohol use. Those with higher severity (exclusive of those with alcohol use disorder) or specific consequences (i.e., legal repercussions) may reflect different characteristics related to early and sustained cessation of heavy drinking.
There was an extensive number of participants lost to follow up, which may have influenced findings as sicker patients are more likely to drop out of such care and studies. However, the researchers did employ a rigorous statistical technique to try to account for the differences between those retained for follow up and those lost to follow up. Future studies should replicate findings with a lower attrition rate.
Health and well-being outcomes were not assessed. Thus, the researchers are unable to examine whether early or sustained cessation of heavy drinking for this sample was linked to improvements in health or well-being. However, previous work has shown this to be the case.
BOTTOM LINE
Two-thirds of adults that were able to be followed up in this study that screened positive initially for heavy drinking in this retrospective cohort study of primary care patients achieved early (1-year) cessation of heavy drinking and of those that achieve early cessation, nearly 2/3 reported sustained (5-year) heavy drinking cessation. Routine primary care was the strongest predictor of sustained cessation. Addiction treatment was also one of the stronger predictors of both early and sustained cessation. Abstinence was linked to higher odds of sustained (5-year) heavy drinking cessation, and this effect was even bigger among those with alcohol use disorder. This study explored the types of factors that predict cessation of heavy drinking as well as what factors predict its stability over time in a primary care sample of adults.
For individuals and families seeking recovery: This study explored predictors of early (1-year) and sustained (5-year) heavy drinking cessation. They found that nearly 2/3 of adults that reported heavy drinking achieved early cessation. Two of the strongest predictors of sustained cessation were receiving addiction treatment within the first year after positive screening and continued routine primary care. Although many stop drinking heavily via low-risk drinking, abstinence tends to be more stable over the long term. If you or a loved one has access to primary care and addiction treatment, it is unlikely to harm and it will likely help achieve alcohol use, health, and wellness goals.
For treatment professionals and treatment systems: The Screening, Brief Intervention, and Referral to Treatment initiative, commonly referred to as SBIRT, is a public health priority. Although previous findings refute the effectiveness of SBIRT linking to treatment, the researchers in this study present evidence of the role that screening for heavy alcohol use may have in real world clinical settings. Most of the adults that screened positive did achieve early cessation of heavy alcohol use, and those that did attend addiction treatment were more likely to reported sustained cessation 5 years after positive screening. Treatment professionals and treatment systems should consider further implementation and refinement of SBIRT in routine care. Furthermore, increasing access to addiction treatment (e.g., pharmacotherapy, flexible outpatient services) may empower primary care providers to meet adults where they are at and link them with the most appropriate care.
For scientists:Researchers in this retrospective cohort study assessed predictors of early (1-year) and sustained (5-year) heavy drinking cessation following a positive screen for engaging in heavy drinking. Routine primary care was the strongest predictor of sustained cessation, with addiction treatment one of the strongest predictors for both early and sustained cessation. Future research should consider exploring what types of addiction services (e.g., pharmacotherapy, outpatient) are most suited for adults with varying profiles engaging in heavy drinking. Additional research should investigate how drinking levels (high-risk, low-risk, abstinence) are linked to health outcomes including but not limited to alcohol among adults engaged in primary care.
For policy makers: Heavy alcohol use and associated problems beget significant cost in premature mortality, disability and lost economic productivity, criminal justice, and health care. This study found that not only is cessation of heavy alcohol use possible among adults engaged in primary care, but it is more likely among those that attend routine primary care and receive addiction treatment. Furthermore, this study explored what factors sustained this change over time. Policy makers may consider funding work that specifically targets this group and for fiscal allocations that may help individuals sustain change over time (e.g., resources to support long-term primary care engagement, such as Medicare, Medicaid, and reduced barriers to primary care visits).
Unhealthy alcohol use can range from risky drinking to alcohol use disorder including alcohol addiction. Such drinking can have a negative impact on health, including disruptions to brain, heart, liver, pancreas, and the immune functioning as well as cause social and familial consequences. In the United States, alcohol use is a leading cause of death and is estimated to cost the United States over $249 billion annually. Although many studies target individuals with alcohol use disorder in treatment and recovery support service settings, much of the disease burden from alcohol is caused by excessive drinking, rather than alcohol use disorder, per se, as this represents a much large number of people. Little is known, however, on how heavy drinkers change, such as reduce or abstain from drinking, in the 1st year after they screen positive for heavy drinking. Furthermore, evidence is lacking that explores what factors predict sustained cessation of heavy drinking or abstinence over time. This study sought to identify what characteristics (e.g., race/ethnicity) and experiences (e.g., addiction treatment) are associated with achieving cessation of heavy drinking over 5 years using a large sample of adults engaged in primary care.
HOW WAS THIS STUDY CONDUCTED?
In this retrospective study, researchers analyzed electronic health records of adults in the Kaiser Permanente Northern California (KPNC) health care network that screened positive for heavy drinking during a routine primary care visit that took place between June 1st, 2013, and May 31st, 2014. The KPNC network serves 4.3 million adults (~1/3 of the Northern Californian population) and has systematically screened for heavy drinking in adult primary care with approximately 80% of its members successfully screened. The main outcome of this study was the cessation of heavy drinking. Screening for heavy drinking consisted of a medical staff member asking three questions: (1) ‘How many times in the past 3 months have you had five/four or more drinks containing alcohol in a day?’ for men aged 18-65 and men aged ≥ 66 or women respectively; (2) ‘On average, how many days per week do you have an alcoholic drink?’, and (3) ‘On a typical drinking day, how many drinks do you have?’. Heavy drinking was positive if a person exceeded either daily (5+ drinks for men aged 18-66 or 4+ for men aged ≥66 and women) or weekly limits (14 drinks/week for men aged 18-66 or 7 drinks/week for men aged ≥66 and women), based on the National Institute of Alcohol Abuse and Alcoholism (NIAAA) guidelines at the time of the initial screening. Early cessation of heavy alcohol use was defined as reporting lower-risk drinking (no heavy drinking days or weeks in the past 3 months) or abstinence at all screenings up to 1-year after the first positive heavy drinking screening. Sustained cessation of heavy alcohol use was defined as obtaining early cessation and reporting lower drinking or abstinence at all screenings up to the 5-year follow-up screening. Possible predictors were also collected and included socio-demographic characteristics, smoking status, drinking level (e.g., exceeding daily, weekly, or both daily and weekly heavy drinking limits), psychiatric disorders, alcohol and other substance use disorders, psychiatric or addiction treatment, routine (i.e., annual) primary care visits, and the type of early cessation (low-risk drinking or abstinence).
All enrollees that screened positive for heavy drinking during the index period (June 1st, 2013, and May 31st, 2014) were eligible to be included. During the 1-year eligibility period, 200,458 adults screened positive for heavy drinking. For each adult, all alcohol screens for the following 63 months were collected. The screenings closest to 1-year and 5-year post index screening were used for early and sustained cessation markers respectively. Approximately 46% of these patients were lost to follow-up due to death, disenrollment from Kaiser Permanente, or not having a 1 year screening, which resulted in 85,434 adults with observed alcohol use data that were used in the final analyses. Among those adults, 53,916 achieved early cessation and were eligible for the sustained cessation analysis, resulting in 19,200 adults with complete outcome data 5 years after index screening. The study accounted statistically for differences in attrition (i.e., likelihood of dropping out of the care during the study window).
Of the 85,434 adults in the analytical sample: 34,761 (40.7%) were females and 28,853 (33.8%) identified as non-white. The average age was 50.3 and 11,914 (13.9%) reported current smoking. Most – 50,193 (58.8%) – exceeded only daily drinking limits, while 20,835 (24.4%) exceeded only weekly limits and 14,406 (16.9%) exceeded both daily and weekly limits. There were also 4,057 (4.7%) adults who met criteria for an alcohol use disorder.
WHAT DID THIS STUDY FIND?
Most that screened positive for heavy alcohol use achieved early cessation.
A total of 53,916 (63.1%) adults that screened positive for heavy drinking achieved early cessation. Among those that achieved early cessation, 25,289 (46.9%) reported abstinence and 28,627 (53.1%) reported lower-risk drinking. Similarly, close to 2/3 (60.0%, 11,539) of the 19,200 that achieved early cessation and had outcome data reported sustained heavy drinking cessation.
Early cessation was more likely among females compared to males and those that did not identify as White.
The researchers found that several demographic characteristics and experiences were linked with higher odds of achieving early cessation. However, those identifying as female compared to male and/or Asian, Native Hawaiian, or Pacific Islander, Black, Latinx/Hispanic, or Native American compared to white were the strongest predictors.
Engagement in services (primary care and addiction treatment) was associated with sustained (5-year) cessation.
Among the 19,200 adults that achieved early (1-year) heavy drinking cessation, those that participated in routine (i.e., annual) primary care had a 57% increase in odds of achieving sustained (5-year) cessation compared to those that did not have routine primary care.
Surprisingly, individuals that attended psychiatric treatment within the first year after being identified with heavy drinking had lower odds of early cessation compared to those that did not. Moreover, adults that attended psychiatric treatment within the first year after positive heavy drinking screening did not differ in odds of achieving sustained cessation compared to those that did not attend psychiatric treatment. Attending addiction treatment, however, was associated with a 19% and 41% increase in odds of achieving early and sustained cessation respectively. Addiction treatment was one of the stronger predictors of sustained heavy drinking cessation.
Abstinence but not Alcohol use disorder diagnosis linked to early or sustained cessation.
Among all adults that screened positive for heavy drinking, 4.7% (4,057) were also diagnosed with an alcohol use disorder. Those with an alcohol use disorder diagnosis were no more likely or less likely to achieve early or sustained cessation of heavy drinking.
Adults that reported abstinence at 1-year were more likely to achieve sustained cessation compared to those reporting low-risk drinking. This effect was even larger among those with alcohol use disorder. For those with alcohol use disorder, abstinence was associated with 2.27 greater odds of sustaining cessation. For those without alcohol use disorder the odds ratio was the same as for the overall sample.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Nationwide, there are tens of millions of individuals that have resolved a substance use problem, and over half of those identify alcohol as the primary problem substance. However, most individuals do not seek or receive help for mild to moderate problematic drinking, highlighting the need to understand how individuals might resolve heavy drinking including. The need includes both those who do and do not attend treatment, and more importantly as it has been studied less often, how these individuals sustain this change over time. The researchers in this study explored what characteristics and behavioral health service utilization predict early (1-year) and sustained (5-year) cessation of heavy drinking. They found that 2/3 of adults that were identified through screening achieved early cessation of heavy drinking. This is higher than previous studies and suggests that screening during primary care may help identify alcohol problems before severity increases and link to needed treatments. Furthermore, the researchers found that routine primary care visits, independent of other factors, was the strongest predictor of sustained cessation. The impact of primary care may be especially useful for those without high severity drinking issues or alcohol use disorder. Primary care may be uniquely situated to address overall medical needs impacting drinking behaviors, identify and treat heavy drinking relapse, promote healthy lifestyles, and link to targeted services. It is also possible that attending routine primary care reflects a larger commitment to healthy lifestyle and some factors that were not measured are responsible for individuals’ drinking change and ability to sustain that change over time.
The type of early drinking cessation mattered for sustaining cessation. Those who reported abstinence at 1-year were more likely to achieve sustained cessation compared to those who reported lower-risk drinking. Previous research has shown that some individuals are able to drink and function as well as those that are abstinent in some domains such as psychological functioning, employment, life satisfaction, and mental health, the greater health risks of their heavier drinking notwithstanding. So, for some, lower risk drinking or lifestyle changes may be most appropriate. In this study, however, it was found that adults who reported abstinence at 1-year were more likely to report sustained cessation of heavy drinking after 5 years compared adults engaging in low-risk drinking. The long-term benefits of abstinence found in this study mirrors findings from the National Epidemiologic Survey on Alcohol Related Conditions (NESARC), a nationally representative sample of U.S. adults. Researchers analyzing the NESCARC data found that abstinence represented the most stable form of remission from alcohol dependence compared to high- and low-risk drinkers after 3 years. Furthermore, researchers exploring a Dutch sample of adults also found that any alcohol use among those in alcohol use disorder remission was a significant risk factor for relapse to active alcohol use disorder. One contribution of the work done here is the inclusion of adults identified with heavy drinking behavior yet do not meet alcohol use disorder criteria; while showing that half of heavy drinkers stop drinking heavily through a low-risk drinking pathway, this study also highlights the greater stability of an abstinence approach to risk reduction and cessation of heavy drinking over time. This finding aligns with previous work highlighting the increased benefits of abstinence.
The electronic health record data obtained for this study was not collected for research purposes. Thus, the analysis presented here relies on both patients to have access to health care and medical staff to administer the alcohol screening and collect other key demographics.
The authors relied on retrospective recall of past 90-day alcohol use to calculate their outcome variable. Although such methods have been used extensively, it has limitations to the extent that individuals’ recall is imperfect. Additionally, there is possible response bias – the tendency to respond in ways that are perceived to be socially desirable.
The data from this study were gathered from adults Northern California members of Kaiser Permanente and replicating to the general US population may be of added value.
The data do not reflect the severity of nor consequences related to alcohol use. Those with higher severity (exclusive of those with alcohol use disorder) or specific consequences (i.e., legal repercussions) may reflect different characteristics related to early and sustained cessation of heavy drinking.
There was an extensive number of participants lost to follow up, which may have influenced findings as sicker patients are more likely to drop out of such care and studies. However, the researchers did employ a rigorous statistical technique to try to account for the differences between those retained for follow up and those lost to follow up. Future studies should replicate findings with a lower attrition rate.
Health and well-being outcomes were not assessed. Thus, the researchers are unable to examine whether early or sustained cessation of heavy drinking for this sample was linked to improvements in health or well-being. However, previous work has shown this to be the case.
BOTTOM LINE
Two-thirds of adults that were able to be followed up in this study that screened positive initially for heavy drinking in this retrospective cohort study of primary care patients achieved early (1-year) cessation of heavy drinking and of those that achieve early cessation, nearly 2/3 reported sustained (5-year) heavy drinking cessation. Routine primary care was the strongest predictor of sustained cessation. Addiction treatment was also one of the stronger predictors of both early and sustained cessation. Abstinence was linked to higher odds of sustained (5-year) heavy drinking cessation, and this effect was even bigger among those with alcohol use disorder. This study explored the types of factors that predict cessation of heavy drinking as well as what factors predict its stability over time in a primary care sample of adults.
For individuals and families seeking recovery: This study explored predictors of early (1-year) and sustained (5-year) heavy drinking cessation. They found that nearly 2/3 of adults that reported heavy drinking achieved early cessation. Two of the strongest predictors of sustained cessation were receiving addiction treatment within the first year after positive screening and continued routine primary care. Although many stop drinking heavily via low-risk drinking, abstinence tends to be more stable over the long term. If you or a loved one has access to primary care and addiction treatment, it is unlikely to harm and it will likely help achieve alcohol use, health, and wellness goals.
For treatment professionals and treatment systems: The Screening, Brief Intervention, and Referral to Treatment initiative, commonly referred to as SBIRT, is a public health priority. Although previous findings refute the effectiveness of SBIRT linking to treatment, the researchers in this study present evidence of the role that screening for heavy alcohol use may have in real world clinical settings. Most of the adults that screened positive did achieve early cessation of heavy alcohol use, and those that did attend addiction treatment were more likely to reported sustained cessation 5 years after positive screening. Treatment professionals and treatment systems should consider further implementation and refinement of SBIRT in routine care. Furthermore, increasing access to addiction treatment (e.g., pharmacotherapy, flexible outpatient services) may empower primary care providers to meet adults where they are at and link them with the most appropriate care.
For scientists:Researchers in this retrospective cohort study assessed predictors of early (1-year) and sustained (5-year) heavy drinking cessation following a positive screen for engaging in heavy drinking. Routine primary care was the strongest predictor of sustained cessation, with addiction treatment one of the strongest predictors for both early and sustained cessation. Future research should consider exploring what types of addiction services (e.g., pharmacotherapy, outpatient) are most suited for adults with varying profiles engaging in heavy drinking. Additional research should investigate how drinking levels (high-risk, low-risk, abstinence) are linked to health outcomes including but not limited to alcohol among adults engaged in primary care.
For policy makers: Heavy alcohol use and associated problems beget significant cost in premature mortality, disability and lost economic productivity, criminal justice, and health care. This study found that not only is cessation of heavy alcohol use possible among adults engaged in primary care, but it is more likely among those that attend routine primary care and receive addiction treatment. Furthermore, this study explored what factors sustained this change over time. Policy makers may consider funding work that specifically targets this group and for fiscal allocations that may help individuals sustain change over time (e.g., resources to support long-term primary care engagement, such as Medicare, Medicaid, and reduced barriers to primary care visits).