Whose voice counts? Treatment outcomes prioritized by people with substance use challenges and their families
In recent years, researchers have argued for moving away from prioritizing abstinence in treatment and recovery support service settings and moving toward more flexible goals driven by individuals receiving services and their families. In line with these efforts to promote person centered outcomes, this report highlights findings from a large survey and focus group interviews among individuals and families with current or former substance use challenges.
For the first several decades of treatment and recovery support service provision, abstinence has been the primary benchmark used by providers, researchers, and government agencies to evaluate successful recovery from a substance use disorder. This narrow focus on substance use versus non-use has come under increasing criticism from several perspectives. The growing field of recovery research has introduced the concept of multiple paths of recovery, including moderation and Harm Reduction-based paths. A nationally representative survey of people in recovery shows that many people resolve their problem despite continuing to use substances, return to moderate use in recovery, or combine abstinence from one substance with using others. Clinically, too, individuals may be using substances and still achieve substance use disorder remission (sustained remission is defined by meeting diagnostic criteria for at least 1 year and then reporting no symptoms for 1 year). For example, among individuals in remission from alcohol use disorder, 1/3 are abstinent, 1/3 are drinking but within NIAAA’s low-risk guidelines, and 1/3 are drinking beyond the low-risk drinking thresholds. This data has prompted calls to move away from use/non-use as the only metric to mark and measure recovery.
A new generation of research defines recovery as a dynamic, goal-directed process of change that may be best measured using multiple dimensions, such as, personal growth, quality of life, and fulfilling relationships, and other aspects of wellbeing. These arguments build on studies showing great diversity in how people who identify as being in recovery describe the core elements of their experience. Nevertheless, there is little consensus regarding what aspects of recovery to measure, how to measure them, and on what time scale. This confusion has made it difficult, if not impossible, for treatment providers and government agencies to adopt standardized metrics of success for individuals involved with treatment and recovery support services. Such metrics are key for judging the effectiveness of such services and supporting decision making for providers, policy makers, scientists, and individual stakeholders alike.
In health care more broadly, there has been a move toward promoting patient centered outcomes, which include the concerns of patients and family members in assessing treatment effectiveness, rather than relying solely on criteria defined by clinicians and scientists. Forms of patient centered care include a non-judgmental approach (“meeting people where they are at”), individualized treatment, including patients in crafting treatment plans or shared decision making, and holistic or integrated services. The successful integration of patient centered care in other domains has led to calls for developing a similar comprehensive and evidence-based framework for the treatment of substance use disorders.
Currently, only a minority of substance use disorder clinics invite patients into the clinical decision-making process in any form. There is wide-spread concern that clinically imposing or recommending treatment goals, especially abstinence, may discourage help-seeking and retention. This view is reinforced by, among others, a recent study showing that concerns about the effects of abstaining from use on craving and quality of life is an independent predictor of failing to complete treatment. It could be that support for a range of patient centered outcomes, including clinical support of moderation as a goal, would help to remove barriers to initiating and receiving care. Researchers also have suggested that patient centered frameworks may facilitate culturally competent and trauma informed approaches as well as greater attention to the social determinants of health that can impact individual recovery outcomes. More knowledge about such patient-centered preferences could inform and enhance the effectiveness of clinical care.
HOW WAS THIS STUDY CONDUCTED?
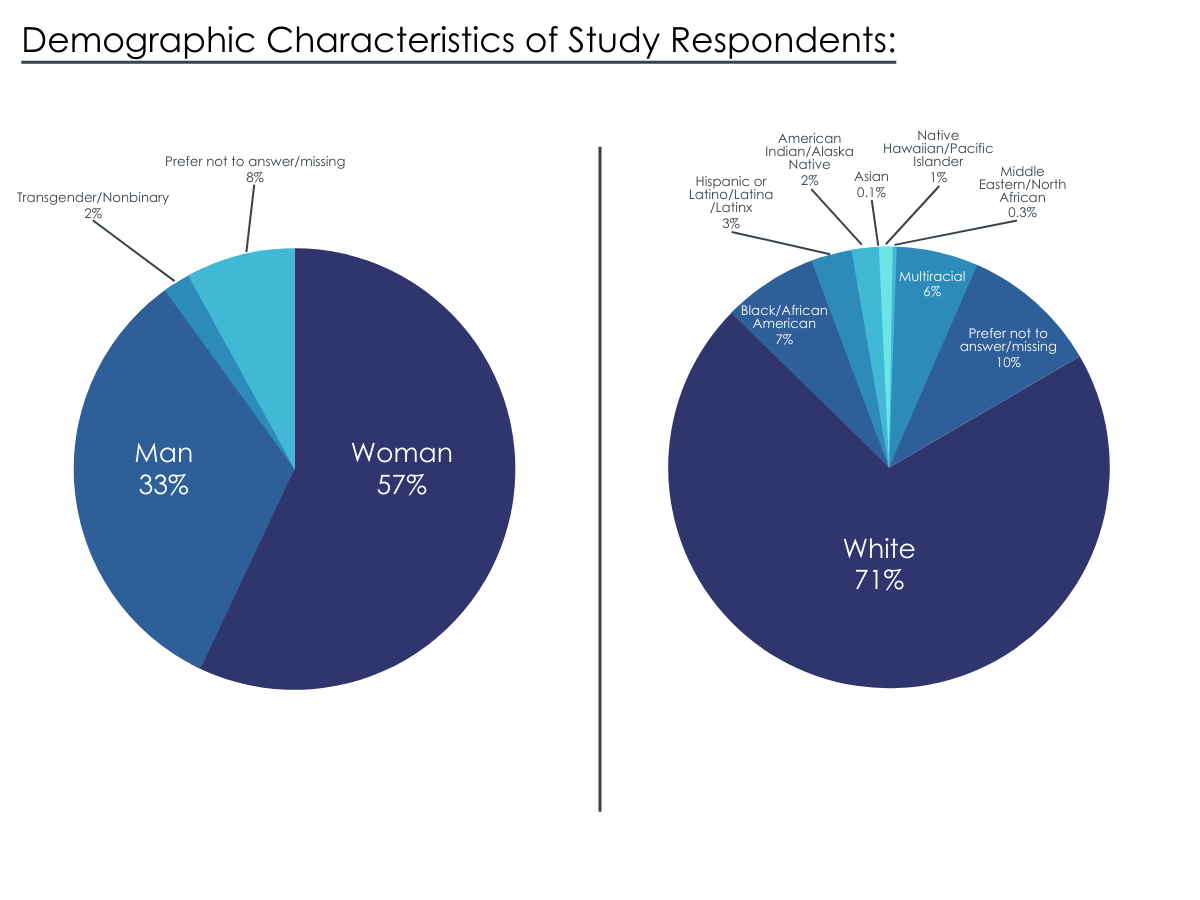
This innovative study, which was advised by a national council of people in recovery, surveyed 883 individuals with experiences of substance use challenges as well as family members to assess their priority outcomes for substance use disorder treatment. The initial data were collected through an online survey conducted between September and early November 2020. People were eligible to complete the survey if they were over 21 and had “lived experience of substance use challenges, including addiction.” The project also invited the participation of people with substance use disorders, people who are using substances, people who are in recovery (using their own definition of recovery), and family members of adults with substance use challenges, including those who had died of substance use. The survey was distributed online by email lists, conference calls, and direct outreach, yielding a convenience sample of 839 responses from 48 states.
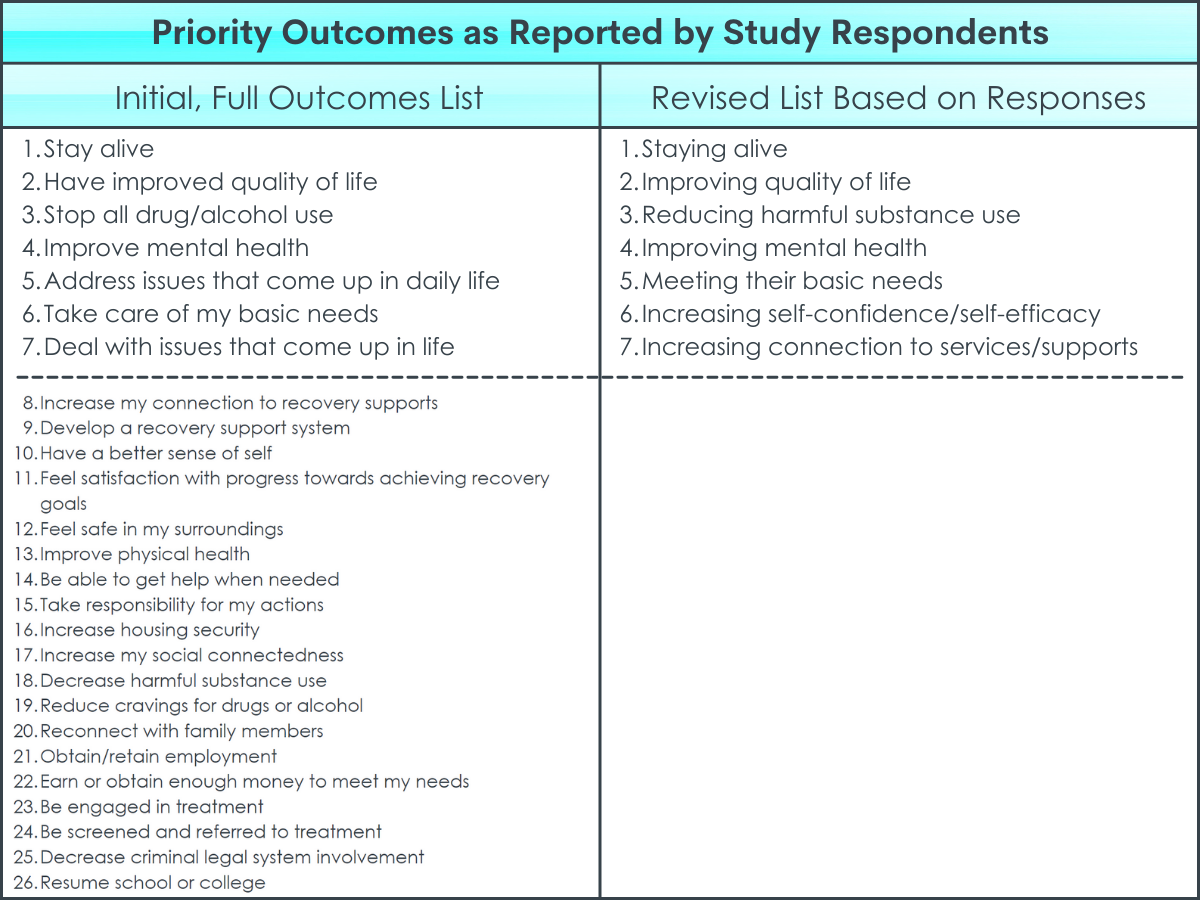
The survey asked individuals to select all outcomes they felt were important from a list of options given to them, and then to provide their top three outcomes in any order. In order to include in depth perspectives and better represent racially and ethnically diverse voices of people in recovery, the project team also hosted 9 virtual focus groups of 53 people in recovery. The results were described using descriptive statistics. Based on this analysis, the project team created an initial list of seven priority outcomes. The project team then revised this list drawing on the feedback of a peer advisory board and focus group discussions. This revised list is presented as the project’s findings in the executive summary.
One innovative aspect of this project was that it established a National Peer Council composed of a diverse group of people in recovery. This council guided the survey design, focus group recruitment, and interpretation of the survey’s findings. It is important to recognize that the final report and its recommendations, including the perspectives of expert consultants, were not independently peer-reviewed and published in a scientific journal, as is the case for most published scientific investigations.
WHAT DID THIS STUDY FIND?
Respondents prioritized treatment outcomes of “stay alive, “have improved quality of life,” and “stop all alcohol and drug use”.
Survey respondents prioritized five outcomes: 1) “stay alive” (32 percent); 2) “have improved quality of life” (29 percent); 3) “stop all alcohol and drug use” (23 percent); 4) “improve mental health” (22 percent); and 5) “address issues that come up in daily life” (20 percent).
There were similarities, but also some differences, by race/ethnicity.
The survey found both commonalities and differences in priority outcomes among racial and ethnic groups. “Stay alive” was ranked in top 5 outcomes by White, African American, Hispanic, and Multiracial respondents. “Stop all alcohol and drug use” was ranked in the top 5 outcomes by White, African American, and Hispanic respondents. “Improve mental health” was ranked in the top 5 outcomes by White, Hispanic, and Multiracial respondents. In contrast, “take care of basic needs” was ranked in the top 5 outcomes by African American and Hispanic respondents only. Despite these differences in preferred treatment outcomes by race/ethnicity, the survey did not find differences among outcomes by socio-economic status.
Men and women had similar priorities, while Transgender/Nonbinary priorities differed.
The priority outcomes selected most frequently by men and women were identical in four of five cases: 1) “Have improved quality of life”; 2) “stay alive”; 3) “stop alcohol and drug use”; and 4) “address issues that come up in daily life.” The women’s list included “improve mental health.”
In contrast, the list of outcomes selected by men included “take care of my basic needs.” Differences were greater between both groups and the small number (17) of Transgender/Nonbinary respondents. The list of outcomes most frequently selected by Transgender/Non-binary respondents included “develop a recovery support system” and “increase housing stability.” Transgender respondents selected “stay alive” (59 percent) more often than any other group.
COVID-19 shifts priorities for some.
The survey asked respondents whether different results become more important during a pandemic like COVID-19. Eighty percent of respondents said that their priority outcomes do not change. For the 20 percent who stated their results would change, they identified the following priority outcomes: 1) “Feel safe in surroundings”; 2) “stay alive”; 3) “improve mental health”; 4) “increase connection to recovery supports”; and 5) “take care of basic needs.”
Most respondents perceived treatment benefit based on their experience.
Seventy-six percent of survey respondents said that some treatment they received helped them achieve their top three results. Most also said services need significant improvement.
Focus groups identified different priorities, including “increase their connection to community and recovery services”.
The focus groups composed of people in recovery identified these priority outcomes: 1) “increase their connection to community and recovery services”; 2) “increase their self-confidence and empowerment”; 3) “connect to a supportive network of community members”; 4) “meet their basic needs and increase life skills”; and 5) “reduce substance use and harmful behaviors, including through harm reduction.”
The report’s final results combine the survey findings and focus groups.
Based on the findings from the focus groups and surveys, the National Peer Council and staff from the sponsoring organizations created a revised priority outcomes list: 1) “staying alive”; 2) “improving quality of life”; 3) “reducing harmful substance use”; 4) improving mental health; 5) “meeting their basic needs”; 6) “increasing self-confidence/self-efficacy”; 7) “increasing connections to services and supports.” This list is described as capturing the outcomes of service that are “the most important to individuals with lived experiences”.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This project was a novel collaboration between Faces and Voices of Recovery, a leading recovery advocacy organization, and the American Society for Addiction Medicine. It represents an important step toward placing the voices of people directly impacted by substance use, including family members, at the center of discussions about what outcomes should be prioritized in treatment and recovery support services. Through the central role played by the National Peer Council, the project also validated the leadership and placed great value in the expertise of people with lived experiences of addiction. Critically, the project attempted to represent, primarily through the National Peer Council and focus groups, the perspectives of racially and ethnically diverse groups that are often marginalized or excluded. Their contributions underscore the need to promote the leadership of African American, Indigenous, and People of Color in the addiction and recovery fields.
Notable among the project’s overall findings are 1) the diversity of outcomes that the respondents endorsed and 2) the fact that no single outcome was prioritized by more than a third of respondents. While these results are informative rather than representative, they support arguments for a combination of standardized recovery metrics and self-defined recovery goals in assessing treatment success.
One of the more important findings of this report is that only a minority of participants identified either abstinence or decreasing harmful use as one of their priority goals. Consistent with general consensus among treatment and recovery scientists, this finding supports the use of additional measures beyond substance use in the evaluation of treatment and recovery support service outcomes. Although additional metrics would represent a departure from current practices for some programs, it would also build on existing understandings within the addiction treatment field and recovery groups. The history of addiction treatment and recovery support shows that emotional, social, and other areas of functioning have been priorities even in services with explicit goals of abstinence, such as 12-step mutual-help groups. Indeed, there is a long-standing view in 12-step literature that substance use is a “symptom” of a deeper problem and not the primary cause of addiction and only the first step in AA’s 12-steps actually mentions alcohol.
Of note, too, is that the report’s survey data showed abstinence (i.e., “stop all alcohol and drug use”) was the third most commonly selected outcome while “decrease harmful substance use” was the 18th. Abstinence was also in the top five preferred outcomes among most sub-groups, including white, African American, Hispanic, male, female, and family member respondents. In contrast, the report’s focus group interviews highlight a preference for the reduction of harmful use. Research shows individuals with abstinence goals may have better substance use outcomes and those with abstinent recovery may have better quality of life than those in non-abstinent recovery. However, for those who recognize a need for substance use treatment but do not receive it, the most commonly cited reason is that they were “not ready to stop using”. Moreover, people’s goals can change over time, even during a single treatment episode. Thus, in order to maximize individual and public health benefits of services for individuals with substance use disorder, stakeholders could institute a flexible approach to goal setting while also recommending – but not requiring – a primary abstinence goal.
Finally, improving evaluation of treatment and recovery support services to include a range of outcomes will require standardized measures with strong scientific underpinnings (also known as psychometric properties). These measures should include both objective (e.g., employment, education, community involvement) and subjective elements (e.g., quality of life, happiness, and psychological distress). Even measures with strong scientific underpinnings, such as the brief assessment of recovery capital (BARC-10), may not be sensitive to how the goals of individuals seeking treatment and recovery supports change over time. Overall, there is much work to be done on the most optimal ways to measure treatment and recovery support service effectiveness beyond substance use.
Findings from this survey should be considered in the context of some important limitations. One important limitation is that the report does not include a breakdown of how many survey respondents were people in recovery, how many were people with active substance use disorders, and how many were people with “substance use challenges.” Complicating the issue further, the report’s final recommendations are described as representing different groups in different sections of the report: individuals with “substance use challenges,” “individuals seeking services,” “people with substance use disorders,” and “people with lived experience of substance use.” Future reports like this one would benefit from greater clarity about both the composition of the surveyed population and what groups are represented by the final recommendations.
As the authors explain, the survey was based on a convenience sample recruited through outreach on the internet and therefore may be shaped by different kinds of selection bias, such as volunteer bias. Further, as the authors note, the sample does not reflect the full racial, ethnic, age, and sexual diversity of those with substance use challenges It is therefore not possible to make inferences from the survey’s findings to populations other than the respondents.
The survey invited participation from people with “lived experience with substance use challenges” in addition to people with substance use disorders and people in recovery (using their own definition). These criteria raise the possibility that some respondents had substance use challenges less severe than substance use disorders. This concern is also strengthened by the fact that people’s diagnosis of substance use disorder was self-reported. Whether people in this study with less severe substance use challenges are candidates for substance use disorder treatment programs remains in question. Including this group within the sample may have influenced the generalizability of these results to the population of addiction treatment participants in the US.
BOTTOM LINE
In this non-peer reviewed report, researchers—advised by a council of people in recovery—surveyed and conducted focus groups with over 800 people with lived experience of substance use issues and their families. Based on this data, they synthesized a priority outcomes list for substance use disorder treatment and recovery supports.
The survey found tremendous diversity in the priority outcomes selected by participants, with no one outcome selected by a majority of respondents. The top outcomes identified by survey participants were 1) “stay alive” (32 percent); 2) “have improved quality of life” (29 percent); 3) “stop all alcohol and drug use” (23 percent); 4) “improve mental health” (22 percent); and 5) “address issues that come up in daily life” (20 percent).
Based on focus group discussions and their peer advisory council, both of which emphasized the importance of racially and ethnically diverse voices of people in recovery, the report’s authors amended the survey findings to produce a revised list of priority outcomes. These are: 1) “staying alive”; 2) “improving quality of life”; 3) “reducing harmful substance use”; 4) improving mental health; 5) “meeting their basic needs”; 6) “increasing self-confidence/self-efficacy”; 7) “increasing connections to services and supports.”
While these results are informative rather than representative, they support arguments for a combination of standardized recovery metrics and self-defined recovery goals in assessing treatment success. They also support the idea of a flexible approach to goal setting while recommending – but not requiring – a primary abstinence goal.
For individuals and families seeking recovery: Today, we understand recovery as a holistic process of change that can involve improving relationships, addressing mental health, developing a sense of community and purpose, and improving overall quality of life. While addressing problematic substance use is a critically important part of treatment, the broader construct of recovery is more than just abstinence or reduced substance use. When seeking out treatment for oneself or a family member, individuals might ask if the provider addresses areas in addition to substance use and if they provide more than one kind of recovery support option. Some individuals may do better in programs and services that develop individualized treatment plans with active input from the person seeking recovery and their families.
For treatment professionals and treatment systems: This report underlines the diversity of treatment outcomes prioritized by people with substance use problems and family members and speaks to the need to move beyond the binary of use versus abstinence in evaluating recovery success. This report also strengthens the case for incorporating patient centered outcomes into addiction treatment that have been employed in multiple other areas of health care. These might include shared decision making, the adoption of a non-judgmental approach (“meeting people where they are at”), individualized treatment, and holistic or integrated services. There is a good case for combining self-defined recovery goals and standardized metrics to evaluate both short- and longer-term recovery success. These findings add to the case for incorporating harm reduction as well as abstinence-based options into addiction treatment services and recovery supports.
For scientists:This project highlights the potential value of incorporating people with lived experience of substance use problems and their families into research on treatment and recovery. It gives further support to researchers who have argued for more holistic metrics to measure recovery as well as the need to evaluate treatment outcomes according to criteria in addition to use/not use or days abstinent. It points to the need for more studies of Black, Hispanic, and Indigenous perspectives on treatment and recovery as well as the specific obstacles faced by each of these groups in seeking and receiving care. The report lends additional weights to arguments for the further incorporation of patient centered outcomes in treatment and recovery support services. Future research might explore how best to integrate patient centered outcomes like shared decision making as well as which groups may benefit more from these practices and which groups might need a more structured approach to care.
For policy makers: Researchers now see recovery as a long-term, holistic process that involves multiple life domains, including mental health, relationships, a sense of purpose or community, and overall quality of life in addition to salubrious changes in substance use. This report lends further support to this view by conveying the large number and diversity of treatment outcomes prioritized by people with lived experience of substance use problems and their families. This result lends support to calls for new measures of treatment success and recovery in addition to substance use only metrics relating to use/non use or numbers of days abstinent from substances. However, there is much that we still do not know regarding how best to measure treatment outcomes and long-term recovery success. This is an area that needs significant research funding. Additionally, African American, Hispanic, and Indigenous people may face unique obstacles to accessing care and have different preferred recovery outcomes. This report underscores the need for the greater availability services that meet the Culturally and Linguistically Appropriate Services (CLAS) standards and research in this area.
For the first several decades of treatment and recovery support service provision, abstinence has been the primary benchmark used by providers, researchers, and government agencies to evaluate successful recovery from a substance use disorder. This narrow focus on substance use versus non-use has come under increasing criticism from several perspectives. The growing field of recovery research has introduced the concept of multiple paths of recovery, including moderation and Harm Reduction-based paths. A nationally representative survey of people in recovery shows that many people resolve their problem despite continuing to use substances, return to moderate use in recovery, or combine abstinence from one substance with using others. Clinically, too, individuals may be using substances and still achieve substance use disorder remission (sustained remission is defined by meeting diagnostic criteria for at least 1 year and then reporting no symptoms for 1 year). For example, among individuals in remission from alcohol use disorder, 1/3 are abstinent, 1/3 are drinking but within NIAAA’s low-risk guidelines, and 1/3 are drinking beyond the low-risk drinking thresholds. This data has prompted calls to move away from use/non-use as the only metric to mark and measure recovery.
A new generation of research defines recovery as a dynamic, goal-directed process of change that may be best measured using multiple dimensions, such as, personal growth, quality of life, and fulfilling relationships, and other aspects of wellbeing. These arguments build on studies showing great diversity in how people who identify as being in recovery describe the core elements of their experience. Nevertheless, there is little consensus regarding what aspects of recovery to measure, how to measure them, and on what time scale. This confusion has made it difficult, if not impossible, for treatment providers and government agencies to adopt standardized metrics of success for individuals involved with treatment and recovery support services. Such metrics are key for judging the effectiveness of such services and supporting decision making for providers, policy makers, scientists, and individual stakeholders alike.
In health care more broadly, there has been a move toward promoting patient centered outcomes, which include the concerns of patients and family members in assessing treatment effectiveness, rather than relying solely on criteria defined by clinicians and scientists. Forms of patient centered care include a non-judgmental approach (“meeting people where they are at”), individualized treatment, including patients in crafting treatment plans or shared decision making, and holistic or integrated services. The successful integration of patient centered care in other domains has led to calls for developing a similar comprehensive and evidence-based framework for the treatment of substance use disorders.
Currently, only a minority of substance use disorder clinics invite patients into the clinical decision-making process in any form. There is wide-spread concern that clinically imposing or recommending treatment goals, especially abstinence, may discourage help-seeking and retention. This view is reinforced by, among others, a recent study showing that concerns about the effects of abstaining from use on craving and quality of life is an independent predictor of failing to complete treatment. It could be that support for a range of patient centered outcomes, including clinical support of moderation as a goal, would help to remove barriers to initiating and receiving care. Researchers also have suggested that patient centered frameworks may facilitate culturally competent and trauma informed approaches as well as greater attention to the social determinants of health that can impact individual recovery outcomes. More knowledge about such patient-centered preferences could inform and enhance the effectiveness of clinical care.
HOW WAS THIS STUDY CONDUCTED?
This innovative study, which was advised by a national council of people in recovery, surveyed 883 individuals with experiences of substance use challenges as well as family members to assess their priority outcomes for substance use disorder treatment. The initial data were collected through an online survey conducted between September and early November 2020. People were eligible to complete the survey if they were over 21 and had “lived experience of substance use challenges, including addiction.” The project also invited the participation of people with substance use disorders, people who are using substances, people who are in recovery (using their own definition of recovery), and family members of adults with substance use challenges, including those who had died of substance use. The survey was distributed online by email lists, conference calls, and direct outreach, yielding a convenience sample of 839 responses from 48 states.
The survey asked individuals to select all outcomes they felt were important from a list of options given to them, and then to provide their top three outcomes in any order. In order to include in depth perspectives and better represent racially and ethnically diverse voices of people in recovery, the project team also hosted 9 virtual focus groups of 53 people in recovery. The results were described using descriptive statistics. Based on this analysis, the project team created an initial list of seven priority outcomes. The project team then revised this list drawing on the feedback of a peer advisory board and focus group discussions. This revised list is presented as the project’s findings in the executive summary.
One innovative aspect of this project was that it established a National Peer Council composed of a diverse group of people in recovery. This council guided the survey design, focus group recruitment, and interpretation of the survey’s findings. It is important to recognize that the final report and its recommendations, including the perspectives of expert consultants, were not independently peer-reviewed and published in a scientific journal, as is the case for most published scientific investigations.
WHAT DID THIS STUDY FIND?
Respondents prioritized treatment outcomes of “stay alive, “have improved quality of life,” and “stop all alcohol and drug use”.
Survey respondents prioritized five outcomes: 1) “stay alive” (32 percent); 2) “have improved quality of life” (29 percent); 3) “stop all alcohol and drug use” (23 percent); 4) “improve mental health” (22 percent); and 5) “address issues that come up in daily life” (20 percent).
There were similarities, but also some differences, by race/ethnicity.
The survey found both commonalities and differences in priority outcomes among racial and ethnic groups. “Stay alive” was ranked in top 5 outcomes by White, African American, Hispanic, and Multiracial respondents. “Stop all alcohol and drug use” was ranked in the top 5 outcomes by White, African American, and Hispanic respondents. “Improve mental health” was ranked in the top 5 outcomes by White, Hispanic, and Multiracial respondents. In contrast, “take care of basic needs” was ranked in the top 5 outcomes by African American and Hispanic respondents only. Despite these differences in preferred treatment outcomes by race/ethnicity, the survey did not find differences among outcomes by socio-economic status.
Men and women had similar priorities, while Transgender/Nonbinary priorities differed.
The priority outcomes selected most frequently by men and women were identical in four of five cases: 1) “Have improved quality of life”; 2) “stay alive”; 3) “stop alcohol and drug use”; and 4) “address issues that come up in daily life.” The women’s list included “improve mental health.”
In contrast, the list of outcomes selected by men included “take care of my basic needs.” Differences were greater between both groups and the small number (17) of Transgender/Nonbinary respondents. The list of outcomes most frequently selected by Transgender/Non-binary respondents included “develop a recovery support system” and “increase housing stability.” Transgender respondents selected “stay alive” (59 percent) more often than any other group.
COVID-19 shifts priorities for some.
The survey asked respondents whether different results become more important during a pandemic like COVID-19. Eighty percent of respondents said that their priority outcomes do not change. For the 20 percent who stated their results would change, they identified the following priority outcomes: 1) “Feel safe in surroundings”; 2) “stay alive”; 3) “improve mental health”; 4) “increase connection to recovery supports”; and 5) “take care of basic needs.”
Most respondents perceived treatment benefit based on their experience.
Seventy-six percent of survey respondents said that some treatment they received helped them achieve their top three results. Most also said services need significant improvement.
Focus groups identified different priorities, including “increase their connection to community and recovery services”.
The focus groups composed of people in recovery identified these priority outcomes: 1) “increase their connection to community and recovery services”; 2) “increase their self-confidence and empowerment”; 3) “connect to a supportive network of community members”; 4) “meet their basic needs and increase life skills”; and 5) “reduce substance use and harmful behaviors, including through harm reduction.”
The report’s final results combine the survey findings and focus groups.
Based on the findings from the focus groups and surveys, the National Peer Council and staff from the sponsoring organizations created a revised priority outcomes list: 1) “staying alive”; 2) “improving quality of life”; 3) “reducing harmful substance use”; 4) improving mental health; 5) “meeting their basic needs”; 6) “increasing self-confidence/self-efficacy”; 7) “increasing connections to services and supports.” This list is described as capturing the outcomes of service that are “the most important to individuals with lived experiences”.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This project was a novel collaboration between Faces and Voices of Recovery, a leading recovery advocacy organization, and the American Society for Addiction Medicine. It represents an important step toward placing the voices of people directly impacted by substance use, including family members, at the center of discussions about what outcomes should be prioritized in treatment and recovery support services. Through the central role played by the National Peer Council, the project also validated the leadership and placed great value in the expertise of people with lived experiences of addiction. Critically, the project attempted to represent, primarily through the National Peer Council and focus groups, the perspectives of racially and ethnically diverse groups that are often marginalized or excluded. Their contributions underscore the need to promote the leadership of African American, Indigenous, and People of Color in the addiction and recovery fields.
Notable among the project’s overall findings are 1) the diversity of outcomes that the respondents endorsed and 2) the fact that no single outcome was prioritized by more than a third of respondents. While these results are informative rather than representative, they support arguments for a combination of standardized recovery metrics and self-defined recovery goals in assessing treatment success.
One of the more important findings of this report is that only a minority of participants identified either abstinence or decreasing harmful use as one of their priority goals. Consistent with general consensus among treatment and recovery scientists, this finding supports the use of additional measures beyond substance use in the evaluation of treatment and recovery support service outcomes. Although additional metrics would represent a departure from current practices for some programs, it would also build on existing understandings within the addiction treatment field and recovery groups. The history of addiction treatment and recovery support shows that emotional, social, and other areas of functioning have been priorities even in services with explicit goals of abstinence, such as 12-step mutual-help groups. Indeed, there is a long-standing view in 12-step literature that substance use is a “symptom” of a deeper problem and not the primary cause of addiction and only the first step in AA’s 12-steps actually mentions alcohol.
Of note, too, is that the report’s survey data showed abstinence (i.e., “stop all alcohol and drug use”) was the third most commonly selected outcome while “decrease harmful substance use” was the 18th. Abstinence was also in the top five preferred outcomes among most sub-groups, including white, African American, Hispanic, male, female, and family member respondents. In contrast, the report’s focus group interviews highlight a preference for the reduction of harmful use. Research shows individuals with abstinence goals may have better substance use outcomes and those with abstinent recovery may have better quality of life than those in non-abstinent recovery. However, for those who recognize a need for substance use treatment but do not receive it, the most commonly cited reason is that they were “not ready to stop using”. Moreover, people’s goals can change over time, even during a single treatment episode. Thus, in order to maximize individual and public health benefits of services for individuals with substance use disorder, stakeholders could institute a flexible approach to goal setting while also recommending – but not requiring – a primary abstinence goal.
Finally, improving evaluation of treatment and recovery support services to include a range of outcomes will require standardized measures with strong scientific underpinnings (also known as psychometric properties). These measures should include both objective (e.g., employment, education, community involvement) and subjective elements (e.g., quality of life, happiness, and psychological distress). Even measures with strong scientific underpinnings, such as the brief assessment of recovery capital (BARC-10), may not be sensitive to how the goals of individuals seeking treatment and recovery supports change over time. Overall, there is much work to be done on the most optimal ways to measure treatment and recovery support service effectiveness beyond substance use.
Findings from this survey should be considered in the context of some important limitations. One important limitation is that the report does not include a breakdown of how many survey respondents were people in recovery, how many were people with active substance use disorders, and how many were people with “substance use challenges.” Complicating the issue further, the report’s final recommendations are described as representing different groups in different sections of the report: individuals with “substance use challenges,” “individuals seeking services,” “people with substance use disorders,” and “people with lived experience of substance use.” Future reports like this one would benefit from greater clarity about both the composition of the surveyed population and what groups are represented by the final recommendations.
As the authors explain, the survey was based on a convenience sample recruited through outreach on the internet and therefore may be shaped by different kinds of selection bias, such as volunteer bias. Further, as the authors note, the sample does not reflect the full racial, ethnic, age, and sexual diversity of those with substance use challenges It is therefore not possible to make inferences from the survey’s findings to populations other than the respondents.
The survey invited participation from people with “lived experience with substance use challenges” in addition to people with substance use disorders and people in recovery (using their own definition). These criteria raise the possibility that some respondents had substance use challenges less severe than substance use disorders. This concern is also strengthened by the fact that people’s diagnosis of substance use disorder was self-reported. Whether people in this study with less severe substance use challenges are candidates for substance use disorder treatment programs remains in question. Including this group within the sample may have influenced the generalizability of these results to the population of addiction treatment participants in the US.
BOTTOM LINE
In this non-peer reviewed report, researchers—advised by a council of people in recovery—surveyed and conducted focus groups with over 800 people with lived experience of substance use issues and their families. Based on this data, they synthesized a priority outcomes list for substance use disorder treatment and recovery supports.
The survey found tremendous diversity in the priority outcomes selected by participants, with no one outcome selected by a majority of respondents. The top outcomes identified by survey participants were 1) “stay alive” (32 percent); 2) “have improved quality of life” (29 percent); 3) “stop all alcohol and drug use” (23 percent); 4) “improve mental health” (22 percent); and 5) “address issues that come up in daily life” (20 percent).
Based on focus group discussions and their peer advisory council, both of which emphasized the importance of racially and ethnically diverse voices of people in recovery, the report’s authors amended the survey findings to produce a revised list of priority outcomes. These are: 1) “staying alive”; 2) “improving quality of life”; 3) “reducing harmful substance use”; 4) improving mental health; 5) “meeting their basic needs”; 6) “increasing self-confidence/self-efficacy”; 7) “increasing connections to services and supports.”
While these results are informative rather than representative, they support arguments for a combination of standardized recovery metrics and self-defined recovery goals in assessing treatment success. They also support the idea of a flexible approach to goal setting while recommending – but not requiring – a primary abstinence goal.
For individuals and families seeking recovery: Today, we understand recovery as a holistic process of change that can involve improving relationships, addressing mental health, developing a sense of community and purpose, and improving overall quality of life. While addressing problematic substance use is a critically important part of treatment, the broader construct of recovery is more than just abstinence or reduced substance use. When seeking out treatment for oneself or a family member, individuals might ask if the provider addresses areas in addition to substance use and if they provide more than one kind of recovery support option. Some individuals may do better in programs and services that develop individualized treatment plans with active input from the person seeking recovery and their families.
For treatment professionals and treatment systems: This report underlines the diversity of treatment outcomes prioritized by people with substance use problems and family members and speaks to the need to move beyond the binary of use versus abstinence in evaluating recovery success. This report also strengthens the case for incorporating patient centered outcomes into addiction treatment that have been employed in multiple other areas of health care. These might include shared decision making, the adoption of a non-judgmental approach (“meeting people where they are at”), individualized treatment, and holistic or integrated services. There is a good case for combining self-defined recovery goals and standardized metrics to evaluate both short- and longer-term recovery success. These findings add to the case for incorporating harm reduction as well as abstinence-based options into addiction treatment services and recovery supports.
For scientists:This project highlights the potential value of incorporating people with lived experience of substance use problems and their families into research on treatment and recovery. It gives further support to researchers who have argued for more holistic metrics to measure recovery as well as the need to evaluate treatment outcomes according to criteria in addition to use/not use or days abstinent. It points to the need for more studies of Black, Hispanic, and Indigenous perspectives on treatment and recovery as well as the specific obstacles faced by each of these groups in seeking and receiving care. The report lends additional weights to arguments for the further incorporation of patient centered outcomes in treatment and recovery support services. Future research might explore how best to integrate patient centered outcomes like shared decision making as well as which groups may benefit more from these practices and which groups might need a more structured approach to care.
For policy makers: Researchers now see recovery as a long-term, holistic process that involves multiple life domains, including mental health, relationships, a sense of purpose or community, and overall quality of life in addition to salubrious changes in substance use. This report lends further support to this view by conveying the large number and diversity of treatment outcomes prioritized by people with lived experience of substance use problems and their families. This result lends support to calls for new measures of treatment success and recovery in addition to substance use only metrics relating to use/non use or numbers of days abstinent from substances. However, there is much that we still do not know regarding how best to measure treatment outcomes and long-term recovery success. This is an area that needs significant research funding. Additionally, African American, Hispanic, and Indigenous people may face unique obstacles to accessing care and have different preferred recovery outcomes. This report underscores the need for the greater availability services that meet the Culturally and Linguistically Appropriate Services (CLAS) standards and research in this area.
For the first several decades of treatment and recovery support service provision, abstinence has been the primary benchmark used by providers, researchers, and government agencies to evaluate successful recovery from a substance use disorder. This narrow focus on substance use versus non-use has come under increasing criticism from several perspectives. The growing field of recovery research has introduced the concept of multiple paths of recovery, including moderation and Harm Reduction-based paths. A nationally representative survey of people in recovery shows that many people resolve their problem despite continuing to use substances, return to moderate use in recovery, or combine abstinence from one substance with using others. Clinically, too, individuals may be using substances and still achieve substance use disorder remission (sustained remission is defined by meeting diagnostic criteria for at least 1 year and then reporting no symptoms for 1 year). For example, among individuals in remission from alcohol use disorder, 1/3 are abstinent, 1/3 are drinking but within NIAAA’s low-risk guidelines, and 1/3 are drinking beyond the low-risk drinking thresholds. This data has prompted calls to move away from use/non-use as the only metric to mark and measure recovery.
A new generation of research defines recovery as a dynamic, goal-directed process of change that may be best measured using multiple dimensions, such as, personal growth, quality of life, and fulfilling relationships, and other aspects of wellbeing. These arguments build on studies showing great diversity in how people who identify as being in recovery describe the core elements of their experience. Nevertheless, there is little consensus regarding what aspects of recovery to measure, how to measure them, and on what time scale. This confusion has made it difficult, if not impossible, for treatment providers and government agencies to adopt standardized metrics of success for individuals involved with treatment and recovery support services. Such metrics are key for judging the effectiveness of such services and supporting decision making for providers, policy makers, scientists, and individual stakeholders alike.
In health care more broadly, there has been a move toward promoting patient centered outcomes, which include the concerns of patients and family members in assessing treatment effectiveness, rather than relying solely on criteria defined by clinicians and scientists. Forms of patient centered care include a non-judgmental approach (“meeting people where they are at”), individualized treatment, including patients in crafting treatment plans or shared decision making, and holistic or integrated services. The successful integration of patient centered care in other domains has led to calls for developing a similar comprehensive and evidence-based framework for the treatment of substance use disorders.
Currently, only a minority of substance use disorder clinics invite patients into the clinical decision-making process in any form. There is wide-spread concern that clinically imposing or recommending treatment goals, especially abstinence, may discourage help-seeking and retention. This view is reinforced by, among others, a recent study showing that concerns about the effects of abstaining from use on craving and quality of life is an independent predictor of failing to complete treatment. It could be that support for a range of patient centered outcomes, including clinical support of moderation as a goal, would help to remove barriers to initiating and receiving care. Researchers also have suggested that patient centered frameworks may facilitate culturally competent and trauma informed approaches as well as greater attention to the social determinants of health that can impact individual recovery outcomes. More knowledge about such patient-centered preferences could inform and enhance the effectiveness of clinical care.
HOW WAS THIS STUDY CONDUCTED?
This innovative study, which was advised by a national council of people in recovery, surveyed 883 individuals with experiences of substance use challenges as well as family members to assess their priority outcomes for substance use disorder treatment. The initial data were collected through an online survey conducted between September and early November 2020. People were eligible to complete the survey if they were over 21 and had “lived experience of substance use challenges, including addiction.” The project also invited the participation of people with substance use disorders, people who are using substances, people who are in recovery (using their own definition of recovery), and family members of adults with substance use challenges, including those who had died of substance use. The survey was distributed online by email lists, conference calls, and direct outreach, yielding a convenience sample of 839 responses from 48 states.
The survey asked individuals to select all outcomes they felt were important from a list of options given to them, and then to provide their top three outcomes in any order. In order to include in depth perspectives and better represent racially and ethnically diverse voices of people in recovery, the project team also hosted 9 virtual focus groups of 53 people in recovery. The results were described using descriptive statistics. Based on this analysis, the project team created an initial list of seven priority outcomes. The project team then revised this list drawing on the feedback of a peer advisory board and focus group discussions. This revised list is presented as the project’s findings in the executive summary.
One innovative aspect of this project was that it established a National Peer Council composed of a diverse group of people in recovery. This council guided the survey design, focus group recruitment, and interpretation of the survey’s findings. It is important to recognize that the final report and its recommendations, including the perspectives of expert consultants, were not independently peer-reviewed and published in a scientific journal, as is the case for most published scientific investigations.
WHAT DID THIS STUDY FIND?
Respondents prioritized treatment outcomes of “stay alive, “have improved quality of life,” and “stop all alcohol and drug use”.
Survey respondents prioritized five outcomes: 1) “stay alive” (32 percent); 2) “have improved quality of life” (29 percent); 3) “stop all alcohol and drug use” (23 percent); 4) “improve mental health” (22 percent); and 5) “address issues that come up in daily life” (20 percent).
There were similarities, but also some differences, by race/ethnicity.
The survey found both commonalities and differences in priority outcomes among racial and ethnic groups. “Stay alive” was ranked in top 5 outcomes by White, African American, Hispanic, and Multiracial respondents. “Stop all alcohol and drug use” was ranked in the top 5 outcomes by White, African American, and Hispanic respondents. “Improve mental health” was ranked in the top 5 outcomes by White, Hispanic, and Multiracial respondents. In contrast, “take care of basic needs” was ranked in the top 5 outcomes by African American and Hispanic respondents only. Despite these differences in preferred treatment outcomes by race/ethnicity, the survey did not find differences among outcomes by socio-economic status.
Men and women had similar priorities, while Transgender/Nonbinary priorities differed.
The priority outcomes selected most frequently by men and women were identical in four of five cases: 1) “Have improved quality of life”; 2) “stay alive”; 3) “stop alcohol and drug use”; and 4) “address issues that come up in daily life.” The women’s list included “improve mental health.”
In contrast, the list of outcomes selected by men included “take care of my basic needs.” Differences were greater between both groups and the small number (17) of Transgender/Nonbinary respondents. The list of outcomes most frequently selected by Transgender/Non-binary respondents included “develop a recovery support system” and “increase housing stability.” Transgender respondents selected “stay alive” (59 percent) more often than any other group.
COVID-19 shifts priorities for some.
The survey asked respondents whether different results become more important during a pandemic like COVID-19. Eighty percent of respondents said that their priority outcomes do not change. For the 20 percent who stated their results would change, they identified the following priority outcomes: 1) “Feel safe in surroundings”; 2) “stay alive”; 3) “improve mental health”; 4) “increase connection to recovery supports”; and 5) “take care of basic needs.”
Most respondents perceived treatment benefit based on their experience.
Seventy-six percent of survey respondents said that some treatment they received helped them achieve their top three results. Most also said services need significant improvement.
Focus groups identified different priorities, including “increase their connection to community and recovery services”.
The focus groups composed of people in recovery identified these priority outcomes: 1) “increase their connection to community and recovery services”; 2) “increase their self-confidence and empowerment”; 3) “connect to a supportive network of community members”; 4) “meet their basic needs and increase life skills”; and 5) “reduce substance use and harmful behaviors, including through harm reduction.”
The report’s final results combine the survey findings and focus groups.
Based on the findings from the focus groups and surveys, the National Peer Council and staff from the sponsoring organizations created a revised priority outcomes list: 1) “staying alive”; 2) “improving quality of life”; 3) “reducing harmful substance use”; 4) improving mental health; 5) “meeting their basic needs”; 6) “increasing self-confidence/self-efficacy”; 7) “increasing connections to services and supports.” This list is described as capturing the outcomes of service that are “the most important to individuals with lived experiences”.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This project was a novel collaboration between Faces and Voices of Recovery, a leading recovery advocacy organization, and the American Society for Addiction Medicine. It represents an important step toward placing the voices of people directly impacted by substance use, including family members, at the center of discussions about what outcomes should be prioritized in treatment and recovery support services. Through the central role played by the National Peer Council, the project also validated the leadership and placed great value in the expertise of people with lived experiences of addiction. Critically, the project attempted to represent, primarily through the National Peer Council and focus groups, the perspectives of racially and ethnically diverse groups that are often marginalized or excluded. Their contributions underscore the need to promote the leadership of African American, Indigenous, and People of Color in the addiction and recovery fields.
Notable among the project’s overall findings are 1) the diversity of outcomes that the respondents endorsed and 2) the fact that no single outcome was prioritized by more than a third of respondents. While these results are informative rather than representative, they support arguments for a combination of standardized recovery metrics and self-defined recovery goals in assessing treatment success.
One of the more important findings of this report is that only a minority of participants identified either abstinence or decreasing harmful use as one of their priority goals. Consistent with general consensus among treatment and recovery scientists, this finding supports the use of additional measures beyond substance use in the evaluation of treatment and recovery support service outcomes. Although additional metrics would represent a departure from current practices for some programs, it would also build on existing understandings within the addiction treatment field and recovery groups. The history of addiction treatment and recovery support shows that emotional, social, and other areas of functioning have been priorities even in services with explicit goals of abstinence, such as 12-step mutual-help groups. Indeed, there is a long-standing view in 12-step literature that substance use is a “symptom” of a deeper problem and not the primary cause of addiction and only the first step in AA’s 12-steps actually mentions alcohol.
Of note, too, is that the report’s survey data showed abstinence (i.e., “stop all alcohol and drug use”) was the third most commonly selected outcome while “decrease harmful substance use” was the 18th. Abstinence was also in the top five preferred outcomes among most sub-groups, including white, African American, Hispanic, male, female, and family member respondents. In contrast, the report’s focus group interviews highlight a preference for the reduction of harmful use. Research shows individuals with abstinence goals may have better substance use outcomes and those with abstinent recovery may have better quality of life than those in non-abstinent recovery. However, for those who recognize a need for substance use treatment but do not receive it, the most commonly cited reason is that they were “not ready to stop using”. Moreover, people’s goals can change over time, even during a single treatment episode. Thus, in order to maximize individual and public health benefits of services for individuals with substance use disorder, stakeholders could institute a flexible approach to goal setting while also recommending – but not requiring – a primary abstinence goal.
Finally, improving evaluation of treatment and recovery support services to include a range of outcomes will require standardized measures with strong scientific underpinnings (also known as psychometric properties). These measures should include both objective (e.g., employment, education, community involvement) and subjective elements (e.g., quality of life, happiness, and psychological distress). Even measures with strong scientific underpinnings, such as the brief assessment of recovery capital (BARC-10), may not be sensitive to how the goals of individuals seeking treatment and recovery supports change over time. Overall, there is much work to be done on the most optimal ways to measure treatment and recovery support service effectiveness beyond substance use.
Findings from this survey should be considered in the context of some important limitations. One important limitation is that the report does not include a breakdown of how many survey respondents were people in recovery, how many were people with active substance use disorders, and how many were people with “substance use challenges.” Complicating the issue further, the report’s final recommendations are described as representing different groups in different sections of the report: individuals with “substance use challenges,” “individuals seeking services,” “people with substance use disorders,” and “people with lived experience of substance use.” Future reports like this one would benefit from greater clarity about both the composition of the surveyed population and what groups are represented by the final recommendations.
As the authors explain, the survey was based on a convenience sample recruited through outreach on the internet and therefore may be shaped by different kinds of selection bias, such as volunteer bias. Further, as the authors note, the sample does not reflect the full racial, ethnic, age, and sexual diversity of those with substance use challenges It is therefore not possible to make inferences from the survey’s findings to populations other than the respondents.
The survey invited participation from people with “lived experience with substance use challenges” in addition to people with substance use disorders and people in recovery (using their own definition). These criteria raise the possibility that some respondents had substance use challenges less severe than substance use disorders. This concern is also strengthened by the fact that people’s diagnosis of substance use disorder was self-reported. Whether people in this study with less severe substance use challenges are candidates for substance use disorder treatment programs remains in question. Including this group within the sample may have influenced the generalizability of these results to the population of addiction treatment participants in the US.
BOTTOM LINE
In this non-peer reviewed report, researchers—advised by a council of people in recovery—surveyed and conducted focus groups with over 800 people with lived experience of substance use issues and their families. Based on this data, they synthesized a priority outcomes list for substance use disorder treatment and recovery supports.
The survey found tremendous diversity in the priority outcomes selected by participants, with no one outcome selected by a majority of respondents. The top outcomes identified by survey participants were 1) “stay alive” (32 percent); 2) “have improved quality of life” (29 percent); 3) “stop all alcohol and drug use” (23 percent); 4) “improve mental health” (22 percent); and 5) “address issues that come up in daily life” (20 percent).
Based on focus group discussions and their peer advisory council, both of which emphasized the importance of racially and ethnically diverse voices of people in recovery, the report’s authors amended the survey findings to produce a revised list of priority outcomes. These are: 1) “staying alive”; 2) “improving quality of life”; 3) “reducing harmful substance use”; 4) improving mental health; 5) “meeting their basic needs”; 6) “increasing self-confidence/self-efficacy”; 7) “increasing connections to services and supports.”
While these results are informative rather than representative, they support arguments for a combination of standardized recovery metrics and self-defined recovery goals in assessing treatment success. They also support the idea of a flexible approach to goal setting while recommending – but not requiring – a primary abstinence goal.
For individuals and families seeking recovery: Today, we understand recovery as a holistic process of change that can involve improving relationships, addressing mental health, developing a sense of community and purpose, and improving overall quality of life. While addressing problematic substance use is a critically important part of treatment, the broader construct of recovery is more than just abstinence or reduced substance use. When seeking out treatment for oneself or a family member, individuals might ask if the provider addresses areas in addition to substance use and if they provide more than one kind of recovery support option. Some individuals may do better in programs and services that develop individualized treatment plans with active input from the person seeking recovery and their families.
For treatment professionals and treatment systems: This report underlines the diversity of treatment outcomes prioritized by people with substance use problems and family members and speaks to the need to move beyond the binary of use versus abstinence in evaluating recovery success. This report also strengthens the case for incorporating patient centered outcomes into addiction treatment that have been employed in multiple other areas of health care. These might include shared decision making, the adoption of a non-judgmental approach (“meeting people where they are at”), individualized treatment, and holistic or integrated services. There is a good case for combining self-defined recovery goals and standardized metrics to evaluate both short- and longer-term recovery success. These findings add to the case for incorporating harm reduction as well as abstinence-based options into addiction treatment services and recovery supports.
For scientists:This project highlights the potential value of incorporating people with lived experience of substance use problems and their families into research on treatment and recovery. It gives further support to researchers who have argued for more holistic metrics to measure recovery as well as the need to evaluate treatment outcomes according to criteria in addition to use/not use or days abstinent. It points to the need for more studies of Black, Hispanic, and Indigenous perspectives on treatment and recovery as well as the specific obstacles faced by each of these groups in seeking and receiving care. The report lends additional weights to arguments for the further incorporation of patient centered outcomes in treatment and recovery support services. Future research might explore how best to integrate patient centered outcomes like shared decision making as well as which groups may benefit more from these practices and which groups might need a more structured approach to care.
For policy makers: Researchers now see recovery as a long-term, holistic process that involves multiple life domains, including mental health, relationships, a sense of purpose or community, and overall quality of life in addition to salubrious changes in substance use. This report lends further support to this view by conveying the large number and diversity of treatment outcomes prioritized by people with lived experience of substance use problems and their families. This result lends support to calls for new measures of treatment success and recovery in addition to substance use only metrics relating to use/non use or numbers of days abstinent from substances. However, there is much that we still do not know regarding how best to measure treatment outcomes and long-term recovery success. This is an area that needs significant research funding. Additionally, African American, Hispanic, and Indigenous people may face unique obstacles to accessing care and have different preferred recovery outcomes. This report underscores the need for the greater availability services that meet the Culturally and Linguistically Appropriate Services (CLAS) standards and research in this area.