How happy are you in your recovery? A novel predictor of positive treatment outcomes
Recovery is often defined as a multifaceted set of holistic outcomes and processes. Understanding which recovery aspects predict treatment and other outcomes can help refine recovery-related theories and inform best practice recommendations. This study examined how well recovery well-being indicators predicted other positive outcomes among adults in either residential or intensive outpatient treatment.
Recovery from substance use disorder is typically defined as positive shifts in substance use – low-risk use or abstinence – alongside improvements in overall health and well-being. There has been a broad convergence of perspectives among scientists, clinicians, and those with lived experience that recovery is multifaceted, dynamic, and reciprocal where reductions in substance use enhances well-being (i.e., recovery capital) which in turn helps maintain abstinence and remission, and so on. However, there remains much to learn about the well-being indicators as research has focused comparatively more on substance use. This study investigated which well-being domains were associated with abstinence during treatment and treatment retention. Identifying which factors are most strongly linked to better understood outcomes may help refine how treatment and recovery support services define, measure, and target recovery as an organizing construct for individuals with substance use and co-occurring disorders.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of data collected from a longitudinal, randomized control trial investigating the effect of a journaling intervention to support recovery from substance use disorder. Participants were recruited from one residential and two intensive outpatient programs that were branches of the same not-for-profit abstinence-based addiction treatment in the Midwestern US. A total of 81 adults, aged 18 or older, participated in original study. However, 78 were included in this study due to missing data. They all were enrolled in the respective program for at least 2 weeks, had about 2 weeks of abstinence, and had a scheduled discharge date after the study ended. Participants were not eligible if they reported significant co-morbid mental health symptoms in the past week. Following a participant’s discharge, the research team met with treatment administrators to extract outcomes from health records. The 2 outcomes were abstinence during treatment and treatment retention. Abstinence was dichotomous and determined by whether a participant’s treatment record showed no substance use between the study’s baseline assessment and the participant’s departure from the treatment setting. Treatment retention was also a dichotomous outcome, with either the participant graduating or leaving on good terms versus leaving for any other reason (e.g., against staff/medical advice).
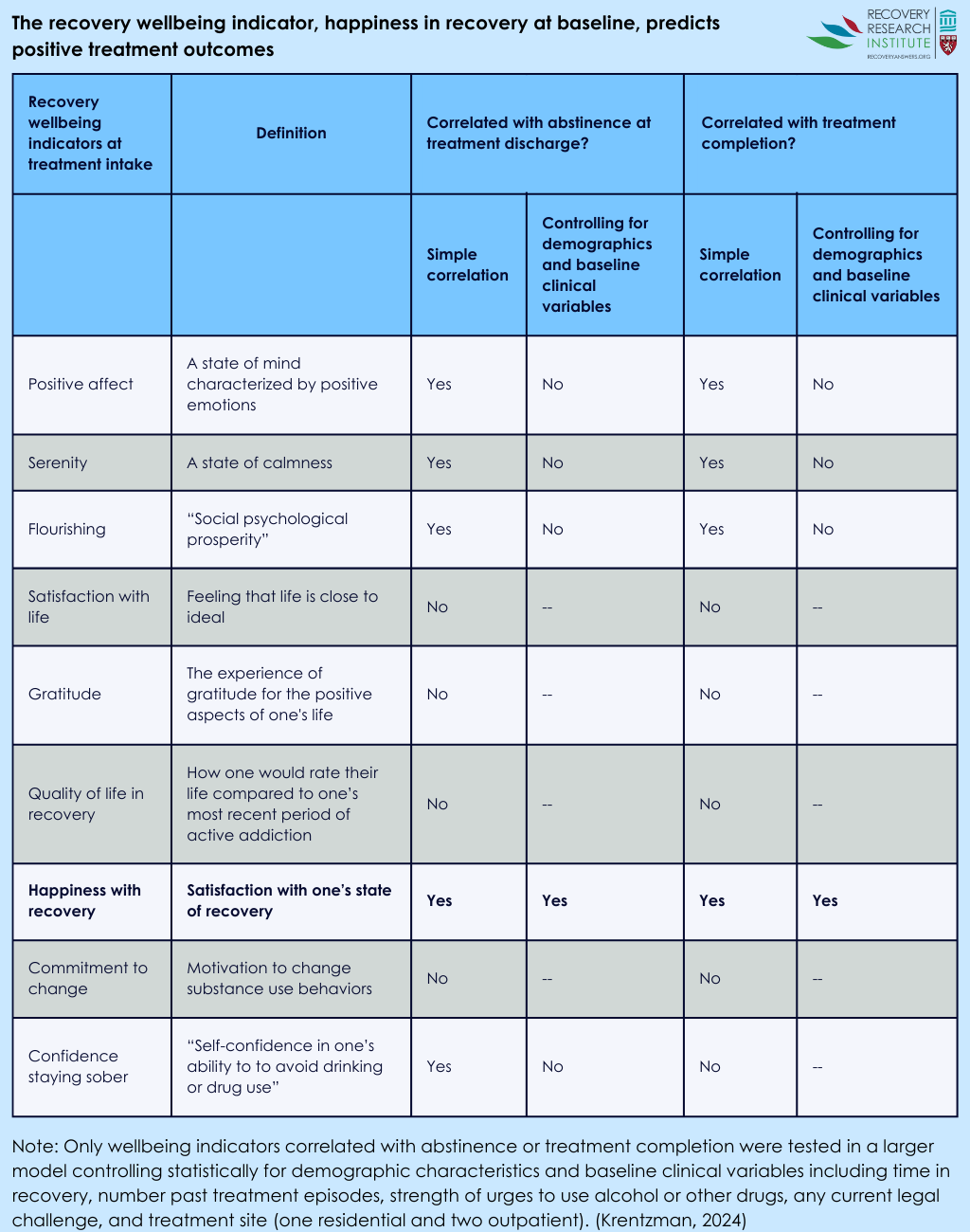
There were 9 unique well-being indicators included in the study: positive affect, serenity, flourishing, satisfaction with life, gratitude, quality of life in recovery, happiness with recovery, commitment to sobriety, and confidence staying sober. Happiness with recovery and confidence staying sober were measured with single items, and the other seven indicators were measured with existing or slightly adapted scales. Happiness with recovery (“In general, I am happy with my recovery”) ranged from 0 (strongly disagree) to 10 (strongly agree). Confidence staying sober ranged from 0 (not at all confident) to 10 (very confident). Initial analyses exploring the link between each individual demographic variable and the outcomes were conducted. Only those factors connected with an outcome were included as covariates in the full analyses. The included covariates were length of sobriety (in days), number of previous treatment episodes, having a current legal issue, urge to use drugs, and recruitment site.
Of the 81 participants in the original study, most were female (53%) and White (74%). There were also 63% of participants that reported a household income less than $15,000, and 47% were single or never married. The substances that participants reported that they were the most addicted to were alcohol (46%), opiates (26%), amphetamines (24%), cannabis (3%), and cocaine/crack (3%). The average days of sobriety was 140, and the average number of previous treatment episodes was 6. Four in 10 participants had a current, self-reported criminal-legal issue.
WHAT DID THIS STUDY FIND?
Only happiness with recovery was linked with abstinence during treatment
Several indicators were linked with abstinence when only considering the indicator itself and abstinence – meaning a simple correlation with no other variables were controlled statistically. This included positive affect, serenity, flourishing, confidence staying sober, and happiness with recovery. When the covariates were incorporated (e.g., previous treatment episodes, legal issue, craving) into the analysis, only happiness with recovery remained associated with abstinence during treatment (see Figure below). For every one unit increase in happiness with recovery (ranging from 0 to 10), participants were 83% more likely to be abstinent.
Only happiness with recovery was independently associated with treatment retention
Similar to the abstinence outcome, positive affect, serenity, flourishing, and happiness with recovery were associated with treatment retention in simple correlations. Yet, when the covariates were included, only happiness with recovery remained associated with treatment retention (see Figure below). For a 1 unit increase in happiness with recovery, a participant was 54% more likely to complete treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined which indicators of well-being were associated with abstinence during treatment and treatment retention among 78 adults in either intensive outpatient or residential treatment. Results showed that across 9 unique indicators, only self-reported happiness with recovery was associated with the outcomes after accounting for demographic and clinical factors also associated with these outcomes (e.g., previous treatment, urge to use, legal issues). The findings highlight the complexity of defining and measuring recovery. There is not a single, agreed upon definition of recovery. However, there is a growing consensus among scientists, service providers, and people with lived experience that recovery as an organizing construct includes, but is not limited to, substance use (e.g., frequency of use, abstinence). These compelling findings highlighted that a single-item measure of happiness with recovery may be an important treatment target and component of recovery. The big remaining question here, of course, is what factors predict happiness in recovery? This remains a valuable research question given the findings in this study.
The lack of significant findings does not signify that the other well-being indicators are not valuable components of recovery. For one, the lack of association between the outcomes and indicators that were not correlated, such as flourishing, may be explained by the study’s small sample. The larger a study sample, the better able it is to detect an effect – in this case a correlation between the recovery indicator and treatment outcome – if one is present. A larger participant sample may find subtle connections between abstinence, treatment retention, and well-being that were not possible to observe in this secondary analysis not designed specifically to answer the research questions examined here. It is important to mention, though, that neither quality of life in recovery nor commitment to sobriety were correlated at all with abstinence or treatment retention.
If in fact these null findings are real – and suggest only happiness in recovery independently predicts positive treatment outcomes – this may mean they are distinct, perhaps offering unique information about one’s well-being not captured by substance use. Overall, continuing to explore how well-being indicators are linked to recovery outcomes and pathways is likely to benefit individuals in or seeking recovery. Furthermore, incorporating single item measures, such as happiness with recovery journey may be useful and efficient.
Participants were informed that the intervention was a journaling task prior to enrollment. Thus, individuals self-selecting into the project may have been predisposed to benefit from a journaling task and to interventions in general compared to those that did not participate in the study.
The small sample size limits the generalizability of the study. However, statistically significant effects found here – e.g., for happiness in recovery – may indicate that there are larger effects in the population.
The participants were from facilities all linked to a single non-profit organization. Thus, they may be unique compared to adults attending other treatment programs.
Although the study was longitudinal, there may not have been enough variation during treatment to find meaningful relationships between well-being indicators and the outcomes of interest.
Abstinence was evaluated solely by patient chart review. Thus, this study may overestimate abstinence rates among participants for whom staff were unaware of substance use.
BOTTOM LINE
Recovery is a complex and multifaceted outcome and process that is experienced and defined in many ways. Perspectives from scientists, service providers, and individuals with lived experience converge on recovery as an organizing construct that includes efforts to improve both substance use and well-being with reductions or elimination of substance giving rise to better functioning and well-being which can then reinforce and perpetuate ongoing remission. However, comparatively less is known scientifically about well-being indicators relative to substance use. This study suggests that happiness with recovery is an important indicator of abstinence during treatment and treatment retention over and above either other unique well-being indicators, including positive affect, serenity, flourishing, satisfaction with life, gratitude, quality of life in recovery, commitment to sobriety, and confidence staying sober. However, the small sample size limits generalizability. Future study is needed, but incorporating measures or an item focused on happiness with recovery is likely to benefit treatment planning and unlikely to hurt. Importantly, a question for future research is what predicts happiness in recovery, so that these factors might be leveraged to improve recovery happiness and other outcomes.
For individuals and families seeking recovery: This study found that happiness with recovery is related to abstinence during treatment and treatment retention among adults while several other well-being indicators were not. The positive experience with the recovery journey may be a simple way to evaluate how the recovery process is going. More work is needed with more people to fully understand the connection between well-being indicators, abstinence, and treatment retention. If you or a loved one is in or seeking recovery, it may be helpful to reflect on happiness with the recovery journey.
For treatment professionals and treatment systems: This study found that a single item assessing an individual’s happiness with their recovery journey was related to abstinence during treatment as well as treatment retention. The small sample size may limit the ability to extend these findings to other adults. However, it is unlikely to hurt and may help evaluate recovery if treatment professionals and systems measure a patient’s happiness with their recovery journey. Measuring happiness with recovery may also provide an avenue to collaboratively improve the recovery journey, improve substance use outcomes, and facilitate treatment completion.
For scientists: This study explored the relationship between 9 well-being indicators and two primary outcomes: abstinence during treatment and treatment retention. The study found that only happiness with recovery was associated with either outcome after adjusting for covariates (e.g., days abstinent at baseline), and happiness with recovery was associated with both primary outcomes. The small sample size limits both generalizability and the ability to detect subtle relationships – i.e., this secondary analysisnot designed to examine the research question examined in this study may have been underpowered. Future investigation should incorporate more individuals across a more diverse sampling pool and investigate what predicts happiness in recovery, so that these factors might be leveraged to improve recovery happiness and other subsequent other outcomes.
For policy makers: This study found that happiness with recovery was connected to both abstinence during treatment and treatment retention. These results reflect the importance of individual experiences during the recovery process. Funding to help understand and validate personal experiences of the treatment and recovery systems may help individuals thrive in recovery. Policies that address critical individual differences (e.g., employment, insurance) may help improve the ability treatment and recovery services have to meet individuals where they are at, which may help reduce the harms caused by substance use and improve happiness with recovery which may in turn bolster and perpetuate the chances of ongoing remission.
Recovery from substance use disorder is typically defined as positive shifts in substance use – low-risk use or abstinence – alongside improvements in overall health and well-being. There has been a broad convergence of perspectives among scientists, clinicians, and those with lived experience that recovery is multifaceted, dynamic, and reciprocal where reductions in substance use enhances well-being (i.e., recovery capital) which in turn helps maintain abstinence and remission, and so on. However, there remains much to learn about the well-being indicators as research has focused comparatively more on substance use. This study investigated which well-being domains were associated with abstinence during treatment and treatment retention. Identifying which factors are most strongly linked to better understood outcomes may help refine how treatment and recovery support services define, measure, and target recovery as an organizing construct for individuals with substance use and co-occurring disorders.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of data collected from a longitudinal, randomized control trial investigating the effect of a journaling intervention to support recovery from substance use disorder. Participants were recruited from one residential and two intensive outpatient programs that were branches of the same not-for-profit abstinence-based addiction treatment in the Midwestern US. A total of 81 adults, aged 18 or older, participated in original study. However, 78 were included in this study due to missing data. They all were enrolled in the respective program for at least 2 weeks, had about 2 weeks of abstinence, and had a scheduled discharge date after the study ended. Participants were not eligible if they reported significant co-morbid mental health symptoms in the past week. Following a participant’s discharge, the research team met with treatment administrators to extract outcomes from health records. The 2 outcomes were abstinence during treatment and treatment retention. Abstinence was dichotomous and determined by whether a participant’s treatment record showed no substance use between the study’s baseline assessment and the participant’s departure from the treatment setting. Treatment retention was also a dichotomous outcome, with either the participant graduating or leaving on good terms versus leaving for any other reason (e.g., against staff/medical advice).
There were 9 unique well-being indicators included in the study: positive affect, serenity, flourishing, satisfaction with life, gratitude, quality of life in recovery, happiness with recovery, commitment to sobriety, and confidence staying sober. Happiness with recovery and confidence staying sober were measured with single items, and the other seven indicators were measured with existing or slightly adapted scales. Happiness with recovery (“In general, I am happy with my recovery”) ranged from 0 (strongly disagree) to 10 (strongly agree). Confidence staying sober ranged from 0 (not at all confident) to 10 (very confident). Initial analyses exploring the link between each individual demographic variable and the outcomes were conducted. Only those factors connected with an outcome were included as covariates in the full analyses. The included covariates were length of sobriety (in days), number of previous treatment episodes, having a current legal issue, urge to use drugs, and recruitment site.
Of the 81 participants in the original study, most were female (53%) and White (74%). There were also 63% of participants that reported a household income less than $15,000, and 47% were single or never married. The substances that participants reported that they were the most addicted to were alcohol (46%), opiates (26%), amphetamines (24%), cannabis (3%), and cocaine/crack (3%). The average days of sobriety was 140, and the average number of previous treatment episodes was 6. Four in 10 participants had a current, self-reported criminal-legal issue.
WHAT DID THIS STUDY FIND?
Only happiness with recovery was linked with abstinence during treatment
Several indicators were linked with abstinence when only considering the indicator itself and abstinence – meaning a simple correlation with no other variables were controlled statistically. This included positive affect, serenity, flourishing, confidence staying sober, and happiness with recovery. When the covariates were incorporated (e.g., previous treatment episodes, legal issue, craving) into the analysis, only happiness with recovery remained associated with abstinence during treatment (see Figure below). For every one unit increase in happiness with recovery (ranging from 0 to 10), participants were 83% more likely to be abstinent.
Only happiness with recovery was independently associated with treatment retention
Similar to the abstinence outcome, positive affect, serenity, flourishing, and happiness with recovery were associated with treatment retention in simple correlations. Yet, when the covariates were included, only happiness with recovery remained associated with treatment retention (see Figure below). For a 1 unit increase in happiness with recovery, a participant was 54% more likely to complete treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined which indicators of well-being were associated with abstinence during treatment and treatment retention among 78 adults in either intensive outpatient or residential treatment. Results showed that across 9 unique indicators, only self-reported happiness with recovery was associated with the outcomes after accounting for demographic and clinical factors also associated with these outcomes (e.g., previous treatment, urge to use, legal issues). The findings highlight the complexity of defining and measuring recovery. There is not a single, agreed upon definition of recovery. However, there is a growing consensus among scientists, service providers, and people with lived experience that recovery as an organizing construct includes, but is not limited to, substance use (e.g., frequency of use, abstinence). These compelling findings highlighted that a single-item measure of happiness with recovery may be an important treatment target and component of recovery. The big remaining question here, of course, is what factors predict happiness in recovery? This remains a valuable research question given the findings in this study.
The lack of significant findings does not signify that the other well-being indicators are not valuable components of recovery. For one, the lack of association between the outcomes and indicators that were not correlated, such as flourishing, may be explained by the study’s small sample. The larger a study sample, the better able it is to detect an effect – in this case a correlation between the recovery indicator and treatment outcome – if one is present. A larger participant sample may find subtle connections between abstinence, treatment retention, and well-being that were not possible to observe in this secondary analysis not designed specifically to answer the research questions examined here. It is important to mention, though, that neither quality of life in recovery nor commitment to sobriety were correlated at all with abstinence or treatment retention.
If in fact these null findings are real – and suggest only happiness in recovery independently predicts positive treatment outcomes – this may mean they are distinct, perhaps offering unique information about one’s well-being not captured by substance use. Overall, continuing to explore how well-being indicators are linked to recovery outcomes and pathways is likely to benefit individuals in or seeking recovery. Furthermore, incorporating single item measures, such as happiness with recovery journey may be useful and efficient.
Participants were informed that the intervention was a journaling task prior to enrollment. Thus, individuals self-selecting into the project may have been predisposed to benefit from a journaling task and to interventions in general compared to those that did not participate in the study.
The small sample size limits the generalizability of the study. However, statistically significant effects found here – e.g., for happiness in recovery – may indicate that there are larger effects in the population.
The participants were from facilities all linked to a single non-profit organization. Thus, they may be unique compared to adults attending other treatment programs.
Although the study was longitudinal, there may not have been enough variation during treatment to find meaningful relationships between well-being indicators and the outcomes of interest.
Abstinence was evaluated solely by patient chart review. Thus, this study may overestimate abstinence rates among participants for whom staff were unaware of substance use.
BOTTOM LINE
Recovery is a complex and multifaceted outcome and process that is experienced and defined in many ways. Perspectives from scientists, service providers, and individuals with lived experience converge on recovery as an organizing construct that includes efforts to improve both substance use and well-being with reductions or elimination of substance giving rise to better functioning and well-being which can then reinforce and perpetuate ongoing remission. However, comparatively less is known scientifically about well-being indicators relative to substance use. This study suggests that happiness with recovery is an important indicator of abstinence during treatment and treatment retention over and above either other unique well-being indicators, including positive affect, serenity, flourishing, satisfaction with life, gratitude, quality of life in recovery, commitment to sobriety, and confidence staying sober. However, the small sample size limits generalizability. Future study is needed, but incorporating measures or an item focused on happiness with recovery is likely to benefit treatment planning and unlikely to hurt. Importantly, a question for future research is what predicts happiness in recovery, so that these factors might be leveraged to improve recovery happiness and other outcomes.
For individuals and families seeking recovery: This study found that happiness with recovery is related to abstinence during treatment and treatment retention among adults while several other well-being indicators were not. The positive experience with the recovery journey may be a simple way to evaluate how the recovery process is going. More work is needed with more people to fully understand the connection between well-being indicators, abstinence, and treatment retention. If you or a loved one is in or seeking recovery, it may be helpful to reflect on happiness with the recovery journey.
For treatment professionals and treatment systems: This study found that a single item assessing an individual’s happiness with their recovery journey was related to abstinence during treatment as well as treatment retention. The small sample size may limit the ability to extend these findings to other adults. However, it is unlikely to hurt and may help evaluate recovery if treatment professionals and systems measure a patient’s happiness with their recovery journey. Measuring happiness with recovery may also provide an avenue to collaboratively improve the recovery journey, improve substance use outcomes, and facilitate treatment completion.
For scientists: This study explored the relationship between 9 well-being indicators and two primary outcomes: abstinence during treatment and treatment retention. The study found that only happiness with recovery was associated with either outcome after adjusting for covariates (e.g., days abstinent at baseline), and happiness with recovery was associated with both primary outcomes. The small sample size limits both generalizability and the ability to detect subtle relationships – i.e., this secondary analysisnot designed to examine the research question examined in this study may have been underpowered. Future investigation should incorporate more individuals across a more diverse sampling pool and investigate what predicts happiness in recovery, so that these factors might be leveraged to improve recovery happiness and other subsequent other outcomes.
For policy makers: This study found that happiness with recovery was connected to both abstinence during treatment and treatment retention. These results reflect the importance of individual experiences during the recovery process. Funding to help understand and validate personal experiences of the treatment and recovery systems may help individuals thrive in recovery. Policies that address critical individual differences (e.g., employment, insurance) may help improve the ability treatment and recovery services have to meet individuals where they are at, which may help reduce the harms caused by substance use and improve happiness with recovery which may in turn bolster and perpetuate the chances of ongoing remission.
Recovery from substance use disorder is typically defined as positive shifts in substance use – low-risk use or abstinence – alongside improvements in overall health and well-being. There has been a broad convergence of perspectives among scientists, clinicians, and those with lived experience that recovery is multifaceted, dynamic, and reciprocal where reductions in substance use enhances well-being (i.e., recovery capital) which in turn helps maintain abstinence and remission, and so on. However, there remains much to learn about the well-being indicators as research has focused comparatively more on substance use. This study investigated which well-being domains were associated with abstinence during treatment and treatment retention. Identifying which factors are most strongly linked to better understood outcomes may help refine how treatment and recovery support services define, measure, and target recovery as an organizing construct for individuals with substance use and co-occurring disorders.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of data collected from a longitudinal, randomized control trial investigating the effect of a journaling intervention to support recovery from substance use disorder. Participants were recruited from one residential and two intensive outpatient programs that were branches of the same not-for-profit abstinence-based addiction treatment in the Midwestern US. A total of 81 adults, aged 18 or older, participated in original study. However, 78 were included in this study due to missing data. They all were enrolled in the respective program for at least 2 weeks, had about 2 weeks of abstinence, and had a scheduled discharge date after the study ended. Participants were not eligible if they reported significant co-morbid mental health symptoms in the past week. Following a participant’s discharge, the research team met with treatment administrators to extract outcomes from health records. The 2 outcomes were abstinence during treatment and treatment retention. Abstinence was dichotomous and determined by whether a participant’s treatment record showed no substance use between the study’s baseline assessment and the participant’s departure from the treatment setting. Treatment retention was also a dichotomous outcome, with either the participant graduating or leaving on good terms versus leaving for any other reason (e.g., against staff/medical advice).
There were 9 unique well-being indicators included in the study: positive affect, serenity, flourishing, satisfaction with life, gratitude, quality of life in recovery, happiness with recovery, commitment to sobriety, and confidence staying sober. Happiness with recovery and confidence staying sober were measured with single items, and the other seven indicators were measured with existing or slightly adapted scales. Happiness with recovery (“In general, I am happy with my recovery”) ranged from 0 (strongly disagree) to 10 (strongly agree). Confidence staying sober ranged from 0 (not at all confident) to 10 (very confident). Initial analyses exploring the link between each individual demographic variable and the outcomes were conducted. Only those factors connected with an outcome were included as covariates in the full analyses. The included covariates were length of sobriety (in days), number of previous treatment episodes, having a current legal issue, urge to use drugs, and recruitment site.
Of the 81 participants in the original study, most were female (53%) and White (74%). There were also 63% of participants that reported a household income less than $15,000, and 47% were single or never married. The substances that participants reported that they were the most addicted to were alcohol (46%), opiates (26%), amphetamines (24%), cannabis (3%), and cocaine/crack (3%). The average days of sobriety was 140, and the average number of previous treatment episodes was 6. Four in 10 participants had a current, self-reported criminal-legal issue.
WHAT DID THIS STUDY FIND?
Only happiness with recovery was linked with abstinence during treatment
Several indicators were linked with abstinence when only considering the indicator itself and abstinence – meaning a simple correlation with no other variables were controlled statistically. This included positive affect, serenity, flourishing, confidence staying sober, and happiness with recovery. When the covariates were incorporated (e.g., previous treatment episodes, legal issue, craving) into the analysis, only happiness with recovery remained associated with abstinence during treatment (see Figure below). For every one unit increase in happiness with recovery (ranging from 0 to 10), participants were 83% more likely to be abstinent.
Only happiness with recovery was independently associated with treatment retention
Similar to the abstinence outcome, positive affect, serenity, flourishing, and happiness with recovery were associated with treatment retention in simple correlations. Yet, when the covariates were included, only happiness with recovery remained associated with treatment retention (see Figure below). For a 1 unit increase in happiness with recovery, a participant was 54% more likely to complete treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined which indicators of well-being were associated with abstinence during treatment and treatment retention among 78 adults in either intensive outpatient or residential treatment. Results showed that across 9 unique indicators, only self-reported happiness with recovery was associated with the outcomes after accounting for demographic and clinical factors also associated with these outcomes (e.g., previous treatment, urge to use, legal issues). The findings highlight the complexity of defining and measuring recovery. There is not a single, agreed upon definition of recovery. However, there is a growing consensus among scientists, service providers, and people with lived experience that recovery as an organizing construct includes, but is not limited to, substance use (e.g., frequency of use, abstinence). These compelling findings highlighted that a single-item measure of happiness with recovery may be an important treatment target and component of recovery. The big remaining question here, of course, is what factors predict happiness in recovery? This remains a valuable research question given the findings in this study.
The lack of significant findings does not signify that the other well-being indicators are not valuable components of recovery. For one, the lack of association between the outcomes and indicators that were not correlated, such as flourishing, may be explained by the study’s small sample. The larger a study sample, the better able it is to detect an effect – in this case a correlation between the recovery indicator and treatment outcome – if one is present. A larger participant sample may find subtle connections between abstinence, treatment retention, and well-being that were not possible to observe in this secondary analysis not designed specifically to answer the research questions examined here. It is important to mention, though, that neither quality of life in recovery nor commitment to sobriety were correlated at all with abstinence or treatment retention.
If in fact these null findings are real – and suggest only happiness in recovery independently predicts positive treatment outcomes – this may mean they are distinct, perhaps offering unique information about one’s well-being not captured by substance use. Overall, continuing to explore how well-being indicators are linked to recovery outcomes and pathways is likely to benefit individuals in or seeking recovery. Furthermore, incorporating single item measures, such as happiness with recovery journey may be useful and efficient.
Participants were informed that the intervention was a journaling task prior to enrollment. Thus, individuals self-selecting into the project may have been predisposed to benefit from a journaling task and to interventions in general compared to those that did not participate in the study.
The small sample size limits the generalizability of the study. However, statistically significant effects found here – e.g., for happiness in recovery – may indicate that there are larger effects in the population.
The participants were from facilities all linked to a single non-profit organization. Thus, they may be unique compared to adults attending other treatment programs.
Although the study was longitudinal, there may not have been enough variation during treatment to find meaningful relationships between well-being indicators and the outcomes of interest.
Abstinence was evaluated solely by patient chart review. Thus, this study may overestimate abstinence rates among participants for whom staff were unaware of substance use.
BOTTOM LINE
Recovery is a complex and multifaceted outcome and process that is experienced and defined in many ways. Perspectives from scientists, service providers, and individuals with lived experience converge on recovery as an organizing construct that includes efforts to improve both substance use and well-being with reductions or elimination of substance giving rise to better functioning and well-being which can then reinforce and perpetuate ongoing remission. However, comparatively less is known scientifically about well-being indicators relative to substance use. This study suggests that happiness with recovery is an important indicator of abstinence during treatment and treatment retention over and above either other unique well-being indicators, including positive affect, serenity, flourishing, satisfaction with life, gratitude, quality of life in recovery, commitment to sobriety, and confidence staying sober. However, the small sample size limits generalizability. Future study is needed, but incorporating measures or an item focused on happiness with recovery is likely to benefit treatment planning and unlikely to hurt. Importantly, a question for future research is what predicts happiness in recovery, so that these factors might be leveraged to improve recovery happiness and other outcomes.
For individuals and families seeking recovery: This study found that happiness with recovery is related to abstinence during treatment and treatment retention among adults while several other well-being indicators were not. The positive experience with the recovery journey may be a simple way to evaluate how the recovery process is going. More work is needed with more people to fully understand the connection between well-being indicators, abstinence, and treatment retention. If you or a loved one is in or seeking recovery, it may be helpful to reflect on happiness with the recovery journey.
For treatment professionals and treatment systems: This study found that a single item assessing an individual’s happiness with their recovery journey was related to abstinence during treatment as well as treatment retention. The small sample size may limit the ability to extend these findings to other adults. However, it is unlikely to hurt and may help evaluate recovery if treatment professionals and systems measure a patient’s happiness with their recovery journey. Measuring happiness with recovery may also provide an avenue to collaboratively improve the recovery journey, improve substance use outcomes, and facilitate treatment completion.
For scientists: This study explored the relationship between 9 well-being indicators and two primary outcomes: abstinence during treatment and treatment retention. The study found that only happiness with recovery was associated with either outcome after adjusting for covariates (e.g., days abstinent at baseline), and happiness with recovery was associated with both primary outcomes. The small sample size limits both generalizability and the ability to detect subtle relationships – i.e., this secondary analysisnot designed to examine the research question examined in this study may have been underpowered. Future investigation should incorporate more individuals across a more diverse sampling pool and investigate what predicts happiness in recovery, so that these factors might be leveraged to improve recovery happiness and other subsequent other outcomes.
For policy makers: This study found that happiness with recovery was connected to both abstinence during treatment and treatment retention. These results reflect the importance of individual experiences during the recovery process. Funding to help understand and validate personal experiences of the treatment and recovery systems may help individuals thrive in recovery. Policies that address critical individual differences (e.g., employment, insurance) may help improve the ability treatment and recovery services have to meet individuals where they are at, which may help reduce the harms caused by substance use and improve happiness with recovery which may in turn bolster and perpetuate the chances of ongoing remission.