Screening, brief intervention, and referral to treatment (SBIRT) interventions implemented in primary care settings hold promise for early detection and treatment of substance use disorder. This study evaluated whether proven recovery management checkups that use assertive linkage as well as long-term monitoring and support add benefit to SBIRT for individuals with alcohol and other drugs use disorders in primary care.
Screening, brief intervention, and referral to treatment(SBIRT) interventions, often implemented in primary care and other traditional health care settings, are designed to identify individuals with substance use disorder, provide brief intervention where appropriate, and to facilitate referral to specialty treatment for those with more severe substance use disorder. For example, federally qualified health centers (federally qualified health centers), which offer care that can be covered by publicly funded health insurance (e.g., U.S. Medicare and Medicaid) and sliding scale fees, are specifically mandated to include SBIRT as part of standard care. However, a recent meta-analysis of SBIRT in primary care settings found the referral to treatment component of SBIRT may be less useful when when linking those with more severe substance use disorder to treatment. Other strategies added to SBIRT may help better meet patient needs and improve outcomes over the long term.
Recovery management checkups are proven, cost-effective interventions based on chronic disease management approaches to substance use disorder treatment. Consisting of quarterly check-ins over extended periods of time (e.g., 1 or more years) after an index episode of treatment that include assessment, motivational interviewing, and re-engagement with care if needed, they improve alcohol and other drug use outcomes compared to standard continuing care by getting people back into treatment sooner if needed.
This model is now being adapted and tested in clinical settings and situations beyond continuing care. In a version of recovery management checkups, training linkage managers remain connected with patients for 2 weeks after an initial referral, helping them access treatment, address participant concerns if they are resistant to enter treatment, and devise an alternative plan if participants refuse to attend treatment. Following this 2-week assertive linkage period, like other recovery management checkups, linkage managers outreach every 3 months to participants and help them re-engage in care if needed. Preliminary evidence in a quasi-experimental study where participants were not randomized to conditions shows primary care patients who received SBIRT plus recovery management checkups were more likely to initiate substance use disorder treatment and experienced greater reductions in past-month days of alcohol and drug use, compared to those who received SBIRT only. The number of days a patient received treatment partially explained these better alcohol and drug use outcomes. In a subsequent randomized controlled trial, primary care patients receiving recovery management checkups on top of SBIRT were more likely to initiate substance use disorder treatment and received more days of substance use disorder treatment, as well as reported more days of abstinence from all substances and fewer days of alcohol and cannabis use, compared to participants who received SBIRT only. The current study includes the 3-month data from the same trial, but examines whether these positive results extend across 12-month outcomes.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial at 4 federally qualified health center sites in Chicago. These federally qualified health centers already incorporated the SBIRT model into regular practice, and thus, staff screen patients annually for substance use disorder. Brief interventions and referrals were carried out by certified or licensed behavioral health staff. Patients who screened positively for substance use disorder (AUDIT 5+ or Drug Abuse Screening Test 3+) and who willingly provided contact information were contacted by research staff who explained study details and conducted additional screening of participants for study eligibility. Those meeting eligibility criteria were then asked to complete informed consent and baseline assessment.
Participants (N=266) were then randomized to either the control (SBIRT-only; n=132) or experimental arm (SBIRT+ recovery management checkups; n=134). In both conditions, SBIRT procedures were carried out by federally qualified health center staff. Recovery management checkup linkages to substance use disorder treatment was provided only in the experimental arm and included quarterly checkups over the 12-month study period (see further details below).
Follow up assessments occurred at 3-, 6-, 9-, and 12-months post-randomization. The primary outcome assessed was any use of alcohol or drug treatment (yes/no). Secondary outcomes summed over 12 months included the following: number of days of alcohol or drug treatment received and by level of care (i.e., residential, intensive outpatient, outpatient, substance use disorder medication, other); number of days of abstinence; number of days of any alcohol, cannabis, cocaine or other stimulant use, and heroin or other opioid use; average number of days of any alcohol or other drug use; and average number of self-reported problems caused by alcohol or other drugs. The researchers hypothesized that relative to patients in the comparison condition (i.e., SBIRT-only), patients in the intervention (i.e., SBIRT+ Recovery Management Checkups) would be more likely over the 12-month study period to have received any substance use disorder treatment, would report more days of treatment and more days of alcohol or other drug abstinence, and would experience greater reductions in substance use including alcohol, cannabis, cocaine or other stimulants, and heroin or other opioids. Finally, the authors hypothesized that the number of days of treatment would explain the effect of the intervention on number of days of abstinence (i.e., that more treatment would be a statistical mediator of improved outcomes).
Each participant assigned to the experimental arm was assigned a linkage manager from the research team, who could have any educational background but received extensive training and certification in motivational interviewing. Linkage managers utilized participants’ responses to research assessments to tailor feedback to participants during the initial linkage meeting and quarterly checkups. During the initial meeting, linkage managers provided participants feedback regarding their substance use and associated consequences and applied motivational interviewing (MI) strategies to help motivate participants to quit or cut down on their substance use and to promote engagement with treatment and recovery. Linkage managers helped to identify and address any barriers to treatment in order to enhance access to treatment and contacted participants 2-3 times per week during the first 2 weeks after the initial linkage meeting to further encourage treatment initiation and engagement. During check-in meetings every 3 months, linkage managers provided tailored feedback to align with participants’ past 30-day alcohol and drug use and treatment engagement. For example, for participants who experienced a recurrence of use and were not currently engaged with treatment, linkage managers focused on facilitating treatment reentry.
With regard to statistical analysis, the efficacy of the intervention on primary and secondary outcomes controlled for baseline values of substance use outcomes as well as time spent in a controlled environment (e.g., jail, prison, residential treatment program) in the 90 days prior to study admission.
Participants were 81% Black, 9% White, and 4% Latino. One third were female (no information regarding the other two-thirds were given though presumably many identified as male). Three-quarters were age 40 or older. Regarding clinical profiles, 68% met criteria for alcohol use disorder, 39% stimulant use disorder, 34% cannabis use disorder, and 24% opioid use disorder. Very few – e.g., 5% – were in treatment in the 90 days before receiving SBIRT in primary care.
WHAT DID THIS STUDY FIND?
Adding recovery management checkups to SBIRT improved treatment engagement
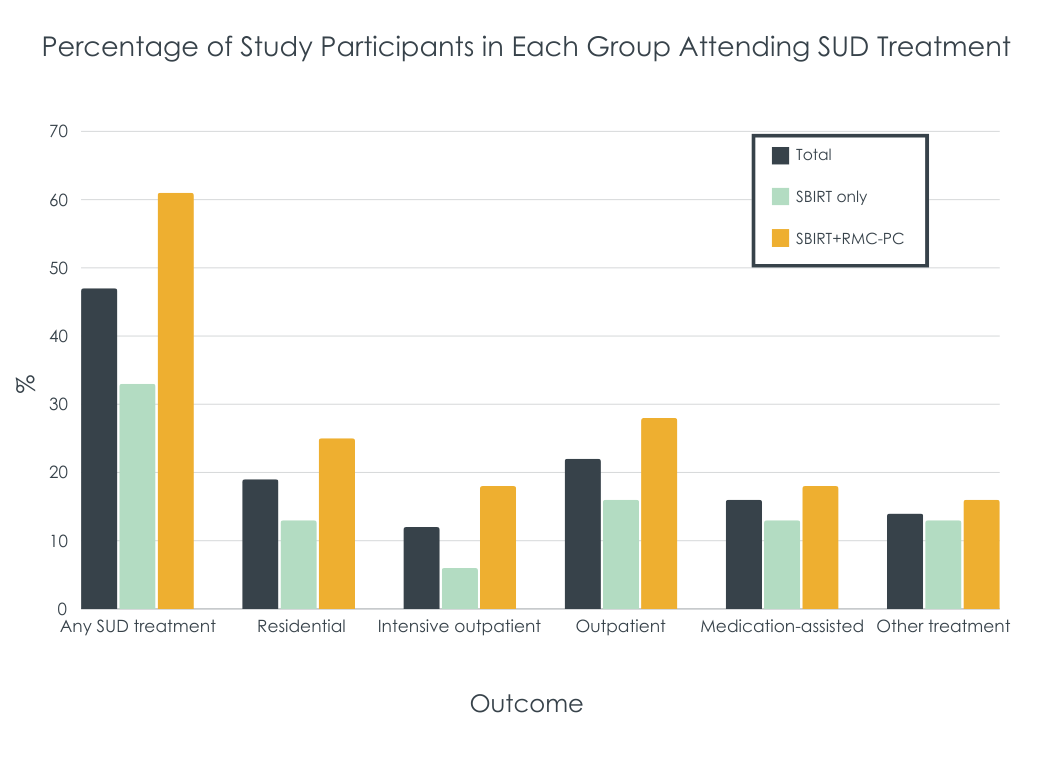
The intervention condition had 4 times greater odds of receiving any alcohol or drug treatment over the 12-month study period (61% vs. 33%). When breaking down results by specific type of treatment, similar effects of the intervention relative to the control were observed on residential (25% vs. 13%), intensive outpatient (18% vs. 6%), and outpatient treatment (28% vs. 16%). However, there were not differences between the experimental and control groups with regard to receiving substance use disorder medication although there was a trend that favored the experimental group (18% vs. 13%).
Relative to those in the SBIRT-only control (M=26.8 days), participants in the recovery management checkup group (M=53.9 days) attended twice as many days of alcohol or other drug treatment over 12 months.
Figure. % of participants in SBIRT-only (aqua bars) vs. SBIRT plus recovery management checkups (orange bars) who attended different types of treatment.
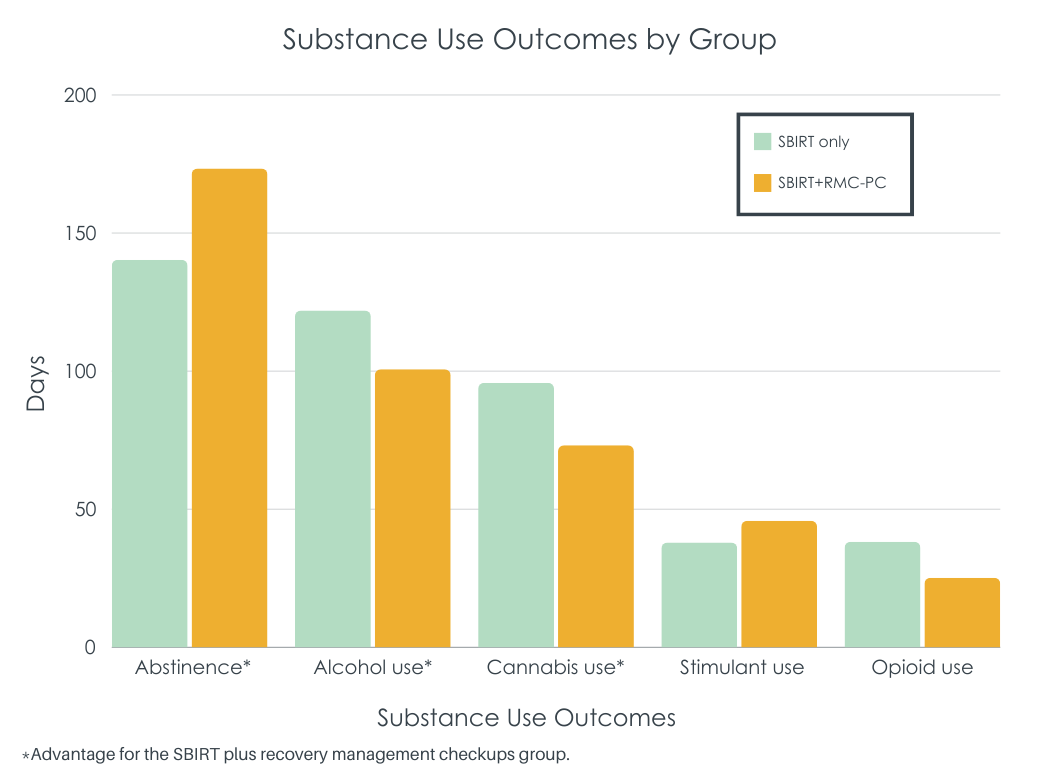
Recovery management checkup participants also had better alcohol and cannabis, but not stimulant and opioid, outcomes
The intervention group also reported increased number of days of abstinence (M=173.4 days) compared to the comparison group (M=140.3 days). While intervention participants had reduced days of alcohol (M=100.7 days vs. M=122.0 days) and cannabis use (M=73.2 days vs. M=95.8 days), differences were not observed between the two conditions for cocaine/stimulant use or heroin/opioid use. As hypothesized, the number of days of alcohol and drug treatment attended partially explained improved outcomes associated with assignment to the recovery management checkup condition.
Future research can help uncover why adding recovery management checkups was less helpful for reducing stimulant and opioid use. Other versions of recovery management checkups for individuals with opioid use disorder employed more assertive linkages to treatment, including direct assistance making appointments as well astransportation to these appointments. It may be that those with more severe substance use challenges – e.g., with severe stimulant and opioid use disorder (perhaps in addition to alcohol use disorder) – benefit from these adaptations of recovery management checkups with even more active linkage and support to attend treatment. In another possible adaptation, recovery management checkups might enhance outcomes for these patients if they are linked to treatments that more specifically cater to opioid or stimulant use disorder and that contain more patients with these disorders (most patients in standard treatment have primary alcohol use disorder and treatments are more aligned with alcohol specific effects). This study did not examine whether the intervention was less helpful for those with opioid and stimulant use disorder – so this idea should be tested in future work.
Of note in this study too was that 80% of participants identified as Black and receiving primary care in federally qualified health centers – 45% were homeless in the year before the study. The utility of recovery management checkups for patients who are likely facing a host of barriers and challenges is a major strength. In addition, linkage managers did not need to have prior high levels of education or specific clinical training, with the study taking anyone willing to be trained in some helpful clinical strategies, and doing so to good effect. Thus, the intervention may also prove to be cost-effective as well. Overall, this study builds on a strong evidence based regarding recovery management checkups to highlight the utility of an initial assertive treatment linkage and ongoing check-ins over time that help people re-enter treatment sooner when needed.
Recruitment for this study was paused in March 2020 due to the COVID-19 pandemic, which also resulted in changes to study protocols (e.g., halting urine testing; follow-up interviews over the phone instead of in-person) and how treatment was being delivered (i.e., more telehealth and virtual options).
Linkage managers assigned to monitor participants in the experimental arm were employed by the research team, received extensive training in motivational interviewing, and were not affiliated with the federally qualified health centers. Thus, findings cannot be generalized to settings where site clinicians deliver the recovery management checkups.
BOTTOM LINE
Recovery management checkups – including an initial, assertive linkage to treatment and regular check-ins with re-linkage to treatment if needed – improves treatment engagement as well as alcohol and cannabis use outcomes compared to standard SBIRT practices in primary care settings. Future studies should continue to examine why SBIRT – even with the addition of empirically-supported recovery management checkups – is more helpful for alcohol use than for opioid and stimulant use at the same levels of severity and impairment.
For individuals and families seeking recovery: Integrating recovery management checkups with standard screening, brief intervention, and referral to treatment (SBIRT) practices in Federally Qualified Health Centers can improve treatment engagement and alcohol and drug use outcomes over 12 months. Online tools like the Substance Abuse and Mental Health Service Administration’s treatment locator can be used to locate local health centers and clinics offering affordable evidence-based services. A quick follow-up with these locations can determine if they employ recovery management checkups to help with ongoing check-ins and support.
For treatment professionals and treatment systems: Substance use treatment systems may consider adding recovery management checkups into standard practice. Treatment systems could invest time and resources into training staff in motivational interviewing strategies and on how to conduct ongoing remission monitoring and check-ins for those who screen positive for severe substance use disorder. Simply adding this model to existing practices where SBIRT is already part of standard care may increase chances of successful treatment initiation, enhance engagement and retention, reduce alcohol and cannabis use outcomes, and lend to early re-intervention when a relapse occurs. For treatment settings where recovery management checkups are less feasible due to resource limitations, treatment professionals could consider implementing some of the components of the framework whereby staff are trained to incorporate some form of patient-centered, regular, structured check-ins (e.g., phone calls) with individuals who screen positive for substance use disorder and who receive a brief intervention and referral to treatment.
For scientists: This study adds to evidence supporting the integration of recovery management checkups as an extension of SBIRT in primary care settings. Recovery management checkups on top of SBIRT improved alcohol and drug treatment initiation and overall engagement over 12 months, as well as greater increases in abstinence and reductions in alcohol and cannabis use over the same time period compared to SBIRT-only. Future research with moderation analyses can help to understand why adding these interventions to SBIRT is not more effective than SBIRT alone for enhancing engagement with substance use disorder medication and for reducing stimulant and opioid use.
For policy makers: More funding devoted to the integration of recovery management checkups alongside SBIRT in primary care settings presents a significant opportunity to increase access to and engagement with alcohol and drug treatment among individuals with substance use disorder. Implementing recovery management checkups alongside SBIRT standard care in federally qualified health centers could support the wider dissemination of these services, particularly among those with limited access to resources. These recovery management frameworks that keep connections with patients active over the long-term and provide direct support that helps people get back into treatment sooner have been shown to improve outcomes and reduce costs.
Screening, brief intervention, and referral to treatment(SBIRT) interventions, often implemented in primary care and other traditional health care settings, are designed to identify individuals with substance use disorder, provide brief intervention where appropriate, and to facilitate referral to specialty treatment for those with more severe substance use disorder. For example, federally qualified health centers (federally qualified health centers), which offer care that can be covered by publicly funded health insurance (e.g., U.S. Medicare and Medicaid) and sliding scale fees, are specifically mandated to include SBIRT as part of standard care. However, a recent meta-analysis of SBIRT in primary care settings found the referral to treatment component of SBIRT may be less useful when when linking those with more severe substance use disorder to treatment. Other strategies added to SBIRT may help better meet patient needs and improve outcomes over the long term.
Recovery management checkups are proven, cost-effective interventions based on chronic disease management approaches to substance use disorder treatment. Consisting of quarterly check-ins over extended periods of time (e.g., 1 or more years) after an index episode of treatment that include assessment, motivational interviewing, and re-engagement with care if needed, they improve alcohol and other drug use outcomes compared to standard continuing care by getting people back into treatment sooner if needed.
This model is now being adapted and tested in clinical settings and situations beyond continuing care. In a version of recovery management checkups, training linkage managers remain connected with patients for 2 weeks after an initial referral, helping them access treatment, address participant concerns if they are resistant to enter treatment, and devise an alternative plan if participants refuse to attend treatment. Following this 2-week assertive linkage period, like other recovery management checkups, linkage managers outreach every 3 months to participants and help them re-engage in care if needed. Preliminary evidence in a quasi-experimental study where participants were not randomized to conditions shows primary care patients who received SBIRT plus recovery management checkups were more likely to initiate substance use disorder treatment and experienced greater reductions in past-month days of alcohol and drug use, compared to those who received SBIRT only. The number of days a patient received treatment partially explained these better alcohol and drug use outcomes. In a subsequent randomized controlled trial, primary care patients receiving recovery management checkups on top of SBIRT were more likely to initiate substance use disorder treatment and received more days of substance use disorder treatment, as well as reported more days of abstinence from all substances and fewer days of alcohol and cannabis use, compared to participants who received SBIRT only. The current study includes the 3-month data from the same trial, but examines whether these positive results extend across 12-month outcomes.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial at 4 federally qualified health center sites in Chicago. These federally qualified health centers already incorporated the SBIRT model into regular practice, and thus, staff screen patients annually for substance use disorder. Brief interventions and referrals were carried out by certified or licensed behavioral health staff. Patients who screened positively for substance use disorder (AUDIT 5+ or Drug Abuse Screening Test 3+) and who willingly provided contact information were contacted by research staff who explained study details and conducted additional screening of participants for study eligibility. Those meeting eligibility criteria were then asked to complete informed consent and baseline assessment.
Participants (N=266) were then randomized to either the control (SBIRT-only; n=132) or experimental arm (SBIRT+ recovery management checkups; n=134). In both conditions, SBIRT procedures were carried out by federally qualified health center staff. Recovery management checkup linkages to substance use disorder treatment was provided only in the experimental arm and included quarterly checkups over the 12-month study period (see further details below).
Follow up assessments occurred at 3-, 6-, 9-, and 12-months post-randomization. The primary outcome assessed was any use of alcohol or drug treatment (yes/no). Secondary outcomes summed over 12 months included the following: number of days of alcohol or drug treatment received and by level of care (i.e., residential, intensive outpatient, outpatient, substance use disorder medication, other); number of days of abstinence; number of days of any alcohol, cannabis, cocaine or other stimulant use, and heroin or other opioid use; average number of days of any alcohol or other drug use; and average number of self-reported problems caused by alcohol or other drugs. The researchers hypothesized that relative to patients in the comparison condition (i.e., SBIRT-only), patients in the intervention (i.e., SBIRT+ Recovery Management Checkups) would be more likely over the 12-month study period to have received any substance use disorder treatment, would report more days of treatment and more days of alcohol or other drug abstinence, and would experience greater reductions in substance use including alcohol, cannabis, cocaine or other stimulants, and heroin or other opioids. Finally, the authors hypothesized that the number of days of treatment would explain the effect of the intervention on number of days of abstinence (i.e., that more treatment would be a statistical mediator of improved outcomes).
Each participant assigned to the experimental arm was assigned a linkage manager from the research team, who could have any educational background but received extensive training and certification in motivational interviewing. Linkage managers utilized participants’ responses to research assessments to tailor feedback to participants during the initial linkage meeting and quarterly checkups. During the initial meeting, linkage managers provided participants feedback regarding their substance use and associated consequences and applied motivational interviewing (MI) strategies to help motivate participants to quit or cut down on their substance use and to promote engagement with treatment and recovery. Linkage managers helped to identify and address any barriers to treatment in order to enhance access to treatment and contacted participants 2-3 times per week during the first 2 weeks after the initial linkage meeting to further encourage treatment initiation and engagement. During check-in meetings every 3 months, linkage managers provided tailored feedback to align with participants’ past 30-day alcohol and drug use and treatment engagement. For example, for participants who experienced a recurrence of use and were not currently engaged with treatment, linkage managers focused on facilitating treatment reentry.
With regard to statistical analysis, the efficacy of the intervention on primary and secondary outcomes controlled for baseline values of substance use outcomes as well as time spent in a controlled environment (e.g., jail, prison, residential treatment program) in the 90 days prior to study admission.
Participants were 81% Black, 9% White, and 4% Latino. One third were female (no information regarding the other two-thirds were given though presumably many identified as male). Three-quarters were age 40 or older. Regarding clinical profiles, 68% met criteria for alcohol use disorder, 39% stimulant use disorder, 34% cannabis use disorder, and 24% opioid use disorder. Very few – e.g., 5% – were in treatment in the 90 days before receiving SBIRT in primary care.
WHAT DID THIS STUDY FIND?
Adding recovery management checkups to SBIRT improved treatment engagement
The intervention condition had 4 times greater odds of receiving any alcohol or drug treatment over the 12-month study period (61% vs. 33%). When breaking down results by specific type of treatment, similar effects of the intervention relative to the control were observed on residential (25% vs. 13%), intensive outpatient (18% vs. 6%), and outpatient treatment (28% vs. 16%). However, there were not differences between the experimental and control groups with regard to receiving substance use disorder medication although there was a trend that favored the experimental group (18% vs. 13%).
Relative to those in the SBIRT-only control (M=26.8 days), participants in the recovery management checkup group (M=53.9 days) attended twice as many days of alcohol or other drug treatment over 12 months.
Figure. % of participants in SBIRT-only (aqua bars) vs. SBIRT plus recovery management checkups (orange bars) who attended different types of treatment.
Recovery management checkup participants also had better alcohol and cannabis, but not stimulant and opioid, outcomes
The intervention group also reported increased number of days of abstinence (M=173.4 days) compared to the comparison group (M=140.3 days). While intervention participants had reduced days of alcohol (M=100.7 days vs. M=122.0 days) and cannabis use (M=73.2 days vs. M=95.8 days), differences were not observed between the two conditions for cocaine/stimulant use or heroin/opioid use. As hypothesized, the number of days of alcohol and drug treatment attended partially explained improved outcomes associated with assignment to the recovery management checkup condition.
Future research can help uncover why adding recovery management checkups was less helpful for reducing stimulant and opioid use. Other versions of recovery management checkups for individuals with opioid use disorder employed more assertive linkages to treatment, including direct assistance making appointments as well astransportation to these appointments. It may be that those with more severe substance use challenges – e.g., with severe stimulant and opioid use disorder (perhaps in addition to alcohol use disorder) – benefit from these adaptations of recovery management checkups with even more active linkage and support to attend treatment. In another possible adaptation, recovery management checkups might enhance outcomes for these patients if they are linked to treatments that more specifically cater to opioid or stimulant use disorder and that contain more patients with these disorders (most patients in standard treatment have primary alcohol use disorder and treatments are more aligned with alcohol specific effects). This study did not examine whether the intervention was less helpful for those with opioid and stimulant use disorder – so this idea should be tested in future work.
Of note in this study too was that 80% of participants identified as Black and receiving primary care in federally qualified health centers – 45% were homeless in the year before the study. The utility of recovery management checkups for patients who are likely facing a host of barriers and challenges is a major strength. In addition, linkage managers did not need to have prior high levels of education or specific clinical training, with the study taking anyone willing to be trained in some helpful clinical strategies, and doing so to good effect. Thus, the intervention may also prove to be cost-effective as well. Overall, this study builds on a strong evidence based regarding recovery management checkups to highlight the utility of an initial assertive treatment linkage and ongoing check-ins over time that help people re-enter treatment sooner when needed.
Recruitment for this study was paused in March 2020 due to the COVID-19 pandemic, which also resulted in changes to study protocols (e.g., halting urine testing; follow-up interviews over the phone instead of in-person) and how treatment was being delivered (i.e., more telehealth and virtual options).
Linkage managers assigned to monitor participants in the experimental arm were employed by the research team, received extensive training in motivational interviewing, and were not affiliated with the federally qualified health centers. Thus, findings cannot be generalized to settings where site clinicians deliver the recovery management checkups.
BOTTOM LINE
Recovery management checkups – including an initial, assertive linkage to treatment and regular check-ins with re-linkage to treatment if needed – improves treatment engagement as well as alcohol and cannabis use outcomes compared to standard SBIRT practices in primary care settings. Future studies should continue to examine why SBIRT – even with the addition of empirically-supported recovery management checkups – is more helpful for alcohol use than for opioid and stimulant use at the same levels of severity and impairment.
For individuals and families seeking recovery: Integrating recovery management checkups with standard screening, brief intervention, and referral to treatment (SBIRT) practices in Federally Qualified Health Centers can improve treatment engagement and alcohol and drug use outcomes over 12 months. Online tools like the Substance Abuse and Mental Health Service Administration’s treatment locator can be used to locate local health centers and clinics offering affordable evidence-based services. A quick follow-up with these locations can determine if they employ recovery management checkups to help with ongoing check-ins and support.
For treatment professionals and treatment systems: Substance use treatment systems may consider adding recovery management checkups into standard practice. Treatment systems could invest time and resources into training staff in motivational interviewing strategies and on how to conduct ongoing remission monitoring and check-ins for those who screen positive for severe substance use disorder. Simply adding this model to existing practices where SBIRT is already part of standard care may increase chances of successful treatment initiation, enhance engagement and retention, reduce alcohol and cannabis use outcomes, and lend to early re-intervention when a relapse occurs. For treatment settings where recovery management checkups are less feasible due to resource limitations, treatment professionals could consider implementing some of the components of the framework whereby staff are trained to incorporate some form of patient-centered, regular, structured check-ins (e.g., phone calls) with individuals who screen positive for substance use disorder and who receive a brief intervention and referral to treatment.
For scientists: This study adds to evidence supporting the integration of recovery management checkups as an extension of SBIRT in primary care settings. Recovery management checkups on top of SBIRT improved alcohol and drug treatment initiation and overall engagement over 12 months, as well as greater increases in abstinence and reductions in alcohol and cannabis use over the same time period compared to SBIRT-only. Future research with moderation analyses can help to understand why adding these interventions to SBIRT is not more effective than SBIRT alone for enhancing engagement with substance use disorder medication and for reducing stimulant and opioid use.
For policy makers: More funding devoted to the integration of recovery management checkups alongside SBIRT in primary care settings presents a significant opportunity to increase access to and engagement with alcohol and drug treatment among individuals with substance use disorder. Implementing recovery management checkups alongside SBIRT standard care in federally qualified health centers could support the wider dissemination of these services, particularly among those with limited access to resources. These recovery management frameworks that keep connections with patients active over the long-term and provide direct support that helps people get back into treatment sooner have been shown to improve outcomes and reduce costs.
Screening, brief intervention, and referral to treatment(SBIRT) interventions, often implemented in primary care and other traditional health care settings, are designed to identify individuals with substance use disorder, provide brief intervention where appropriate, and to facilitate referral to specialty treatment for those with more severe substance use disorder. For example, federally qualified health centers (federally qualified health centers), which offer care that can be covered by publicly funded health insurance (e.g., U.S. Medicare and Medicaid) and sliding scale fees, are specifically mandated to include SBIRT as part of standard care. However, a recent meta-analysis of SBIRT in primary care settings found the referral to treatment component of SBIRT may be less useful when when linking those with more severe substance use disorder to treatment. Other strategies added to SBIRT may help better meet patient needs and improve outcomes over the long term.
Recovery management checkups are proven, cost-effective interventions based on chronic disease management approaches to substance use disorder treatment. Consisting of quarterly check-ins over extended periods of time (e.g., 1 or more years) after an index episode of treatment that include assessment, motivational interviewing, and re-engagement with care if needed, they improve alcohol and other drug use outcomes compared to standard continuing care by getting people back into treatment sooner if needed.
This model is now being adapted and tested in clinical settings and situations beyond continuing care. In a version of recovery management checkups, training linkage managers remain connected with patients for 2 weeks after an initial referral, helping them access treatment, address participant concerns if they are resistant to enter treatment, and devise an alternative plan if participants refuse to attend treatment. Following this 2-week assertive linkage period, like other recovery management checkups, linkage managers outreach every 3 months to participants and help them re-engage in care if needed. Preliminary evidence in a quasi-experimental study where participants were not randomized to conditions shows primary care patients who received SBIRT plus recovery management checkups were more likely to initiate substance use disorder treatment and experienced greater reductions in past-month days of alcohol and drug use, compared to those who received SBIRT only. The number of days a patient received treatment partially explained these better alcohol and drug use outcomes. In a subsequent randomized controlled trial, primary care patients receiving recovery management checkups on top of SBIRT were more likely to initiate substance use disorder treatment and received more days of substance use disorder treatment, as well as reported more days of abstinence from all substances and fewer days of alcohol and cannabis use, compared to participants who received SBIRT only. The current study includes the 3-month data from the same trial, but examines whether these positive results extend across 12-month outcomes.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial at 4 federally qualified health center sites in Chicago. These federally qualified health centers already incorporated the SBIRT model into regular practice, and thus, staff screen patients annually for substance use disorder. Brief interventions and referrals were carried out by certified or licensed behavioral health staff. Patients who screened positively for substance use disorder (AUDIT 5+ or Drug Abuse Screening Test 3+) and who willingly provided contact information were contacted by research staff who explained study details and conducted additional screening of participants for study eligibility. Those meeting eligibility criteria were then asked to complete informed consent and baseline assessment.
Participants (N=266) were then randomized to either the control (SBIRT-only; n=132) or experimental arm (SBIRT+ recovery management checkups; n=134). In both conditions, SBIRT procedures were carried out by federally qualified health center staff. Recovery management checkup linkages to substance use disorder treatment was provided only in the experimental arm and included quarterly checkups over the 12-month study period (see further details below).
Follow up assessments occurred at 3-, 6-, 9-, and 12-months post-randomization. The primary outcome assessed was any use of alcohol or drug treatment (yes/no). Secondary outcomes summed over 12 months included the following: number of days of alcohol or drug treatment received and by level of care (i.e., residential, intensive outpatient, outpatient, substance use disorder medication, other); number of days of abstinence; number of days of any alcohol, cannabis, cocaine or other stimulant use, and heroin or other opioid use; average number of days of any alcohol or other drug use; and average number of self-reported problems caused by alcohol or other drugs. The researchers hypothesized that relative to patients in the comparison condition (i.e., SBIRT-only), patients in the intervention (i.e., SBIRT+ Recovery Management Checkups) would be more likely over the 12-month study period to have received any substance use disorder treatment, would report more days of treatment and more days of alcohol or other drug abstinence, and would experience greater reductions in substance use including alcohol, cannabis, cocaine or other stimulants, and heroin or other opioids. Finally, the authors hypothesized that the number of days of treatment would explain the effect of the intervention on number of days of abstinence (i.e., that more treatment would be a statistical mediator of improved outcomes).
Each participant assigned to the experimental arm was assigned a linkage manager from the research team, who could have any educational background but received extensive training and certification in motivational interviewing. Linkage managers utilized participants’ responses to research assessments to tailor feedback to participants during the initial linkage meeting and quarterly checkups. During the initial meeting, linkage managers provided participants feedback regarding their substance use and associated consequences and applied motivational interviewing (MI) strategies to help motivate participants to quit or cut down on their substance use and to promote engagement with treatment and recovery. Linkage managers helped to identify and address any barriers to treatment in order to enhance access to treatment and contacted participants 2-3 times per week during the first 2 weeks after the initial linkage meeting to further encourage treatment initiation and engagement. During check-in meetings every 3 months, linkage managers provided tailored feedback to align with participants’ past 30-day alcohol and drug use and treatment engagement. For example, for participants who experienced a recurrence of use and were not currently engaged with treatment, linkage managers focused on facilitating treatment reentry.
With regard to statistical analysis, the efficacy of the intervention on primary and secondary outcomes controlled for baseline values of substance use outcomes as well as time spent in a controlled environment (e.g., jail, prison, residential treatment program) in the 90 days prior to study admission.
Participants were 81% Black, 9% White, and 4% Latino. One third were female (no information regarding the other two-thirds were given though presumably many identified as male). Three-quarters were age 40 or older. Regarding clinical profiles, 68% met criteria for alcohol use disorder, 39% stimulant use disorder, 34% cannabis use disorder, and 24% opioid use disorder. Very few – e.g., 5% – were in treatment in the 90 days before receiving SBIRT in primary care.
WHAT DID THIS STUDY FIND?
Adding recovery management checkups to SBIRT improved treatment engagement
The intervention condition had 4 times greater odds of receiving any alcohol or drug treatment over the 12-month study period (61% vs. 33%). When breaking down results by specific type of treatment, similar effects of the intervention relative to the control were observed on residential (25% vs. 13%), intensive outpatient (18% vs. 6%), and outpatient treatment (28% vs. 16%). However, there were not differences between the experimental and control groups with regard to receiving substance use disorder medication although there was a trend that favored the experimental group (18% vs. 13%).
Relative to those in the SBIRT-only control (M=26.8 days), participants in the recovery management checkup group (M=53.9 days) attended twice as many days of alcohol or other drug treatment over 12 months.
Figure. % of participants in SBIRT-only (aqua bars) vs. SBIRT plus recovery management checkups (orange bars) who attended different types of treatment.
Recovery management checkup participants also had better alcohol and cannabis, but not stimulant and opioid, outcomes
The intervention group also reported increased number of days of abstinence (M=173.4 days) compared to the comparison group (M=140.3 days). While intervention participants had reduced days of alcohol (M=100.7 days vs. M=122.0 days) and cannabis use (M=73.2 days vs. M=95.8 days), differences were not observed between the two conditions for cocaine/stimulant use or heroin/opioid use. As hypothesized, the number of days of alcohol and drug treatment attended partially explained improved outcomes associated with assignment to the recovery management checkup condition.
Future research can help uncover why adding recovery management checkups was less helpful for reducing stimulant and opioid use. Other versions of recovery management checkups for individuals with opioid use disorder employed more assertive linkages to treatment, including direct assistance making appointments as well astransportation to these appointments. It may be that those with more severe substance use challenges – e.g., with severe stimulant and opioid use disorder (perhaps in addition to alcohol use disorder) – benefit from these adaptations of recovery management checkups with even more active linkage and support to attend treatment. In another possible adaptation, recovery management checkups might enhance outcomes for these patients if they are linked to treatments that more specifically cater to opioid or stimulant use disorder and that contain more patients with these disorders (most patients in standard treatment have primary alcohol use disorder and treatments are more aligned with alcohol specific effects). This study did not examine whether the intervention was less helpful for those with opioid and stimulant use disorder – so this idea should be tested in future work.
Of note in this study too was that 80% of participants identified as Black and receiving primary care in federally qualified health centers – 45% were homeless in the year before the study. The utility of recovery management checkups for patients who are likely facing a host of barriers and challenges is a major strength. In addition, linkage managers did not need to have prior high levels of education or specific clinical training, with the study taking anyone willing to be trained in some helpful clinical strategies, and doing so to good effect. Thus, the intervention may also prove to be cost-effective as well. Overall, this study builds on a strong evidence based regarding recovery management checkups to highlight the utility of an initial assertive treatment linkage and ongoing check-ins over time that help people re-enter treatment sooner when needed.
Recruitment for this study was paused in March 2020 due to the COVID-19 pandemic, which also resulted in changes to study protocols (e.g., halting urine testing; follow-up interviews over the phone instead of in-person) and how treatment was being delivered (i.e., more telehealth and virtual options).
Linkage managers assigned to monitor participants in the experimental arm were employed by the research team, received extensive training in motivational interviewing, and were not affiliated with the federally qualified health centers. Thus, findings cannot be generalized to settings where site clinicians deliver the recovery management checkups.
BOTTOM LINE
Recovery management checkups – including an initial, assertive linkage to treatment and regular check-ins with re-linkage to treatment if needed – improves treatment engagement as well as alcohol and cannabis use outcomes compared to standard SBIRT practices in primary care settings. Future studies should continue to examine why SBIRT – even with the addition of empirically-supported recovery management checkups – is more helpful for alcohol use than for opioid and stimulant use at the same levels of severity and impairment.
For individuals and families seeking recovery: Integrating recovery management checkups with standard screening, brief intervention, and referral to treatment (SBIRT) practices in Federally Qualified Health Centers can improve treatment engagement and alcohol and drug use outcomes over 12 months. Online tools like the Substance Abuse and Mental Health Service Administration’s treatment locator can be used to locate local health centers and clinics offering affordable evidence-based services. A quick follow-up with these locations can determine if they employ recovery management checkups to help with ongoing check-ins and support.
For treatment professionals and treatment systems: Substance use treatment systems may consider adding recovery management checkups into standard practice. Treatment systems could invest time and resources into training staff in motivational interviewing strategies and on how to conduct ongoing remission monitoring and check-ins for those who screen positive for severe substance use disorder. Simply adding this model to existing practices where SBIRT is already part of standard care may increase chances of successful treatment initiation, enhance engagement and retention, reduce alcohol and cannabis use outcomes, and lend to early re-intervention when a relapse occurs. For treatment settings where recovery management checkups are less feasible due to resource limitations, treatment professionals could consider implementing some of the components of the framework whereby staff are trained to incorporate some form of patient-centered, regular, structured check-ins (e.g., phone calls) with individuals who screen positive for substance use disorder and who receive a brief intervention and referral to treatment.
For scientists: This study adds to evidence supporting the integration of recovery management checkups as an extension of SBIRT in primary care settings. Recovery management checkups on top of SBIRT improved alcohol and drug treatment initiation and overall engagement over 12 months, as well as greater increases in abstinence and reductions in alcohol and cannabis use over the same time period compared to SBIRT-only. Future research with moderation analyses can help to understand why adding these interventions to SBIRT is not more effective than SBIRT alone for enhancing engagement with substance use disorder medication and for reducing stimulant and opioid use.
For policy makers: More funding devoted to the integration of recovery management checkups alongside SBIRT in primary care settings presents a significant opportunity to increase access to and engagement with alcohol and drug treatment among individuals with substance use disorder. Implementing recovery management checkups alongside SBIRT standard care in federally qualified health centers could support the wider dissemination of these services, particularly among those with limited access to resources. These recovery management frameworks that keep connections with patients active over the long-term and provide direct support that helps people get back into treatment sooner have been shown to improve outcomes and reduce costs.