Screening and brief intervention delivered in the workplace can reduce alcohol consumption
Screening individuals for hazardous alcohol use and providing a brief intervention is shown to help reduce consumption, but the length and type of intervention, and the best settings for their delivery remain unclear. This study evaluated the effectiveness of two different intensities of an intervention for excessive alcohol consumption in a workplace setting.
Screening and brief intervention is one such strategy that involves asking individuals a set of questions about their current drinking habits. If they report drinking more than the recommended amounts, a staff person engages them in a short, but systematic discussion about ways to reduce their drinking. This low-intensity intervention produces small, but reliable drinking reductions in primary care and workplace settings across the world.
However, important aspects of implementing the intervention optimally are unclear. For example, there do not appear to be any additional benefits of a longer intervention or repeating the intervention above and beyond a shorter intervention that lasts approximately 20 minutes. It may therefore be that even shorter interventions (e.g., 5 minutes) have beneficial effects and would be more feasible to implement under time constraints. It is also unclear whether the intervention can be effective in workplace settings in Japan specifically. Given the “overwork” culture in Japan, it may be that people are attempting to relax with alcohol. However, this also means the workplace may be an ideal setting to reduce alcohol consumption because of the amount of time spent working. Finally, having nurses deliver the intervention can result in broader implementation than doctors because more nurses are employed in occupational healthcare settings than doctors. This study evaluated the effectiveness of two types of the intervention delivered by nurses in a workplace setting. Studies like these can shed light on the conditions and settings in which screening and brief intervention is likely to be effective and feasible.
HOW WAS THIS STUDY CONDUCTED?
The research team evaluated the effectiveness of two intensities of the same type of brief intervention delivered by nurses in 5 companies from 2 western Japanese regions. Nurses were trained to screen participants using the Alcohol Use Disorder Identification Test (hereafter referred to as “screener”) and provide the types of intervention. This consisted of e-learning and role-playing and included information about the stages of change model and motivational interviewing techniques. The stages of change model helps to identify participants’ readiness and motivation to change their drinking behavior, while motivational interviewing helps them to resolve any ambivalence they may have about change.
Participants were eligible for the study if they were 20 years old or older (i.e., of legal drinking age in Japan) and had a high score on the screener (i.e., greater than 8 points, which reflects hazardous alcohol use). Participants were not eligible if they were 75 years old or older; received treatment for their alcohol use in the past year; had symptoms of alcohol withdrawal in the past year; were advised by a doctor to change their drinking habits in the past 3 months; were pregnant; or reported suicidal thoughts or behaviors.
If eligible, participants were randomized into 1 of 3 groups: (1) the standard intervention, which consisted of a 15-minute advice and counseling session; (2) a shorter intervention, which consisted of a 5-minute brief advice session; or (3) a control group. In the standard intervention group, participants completed a baseline questionnaire and were provided with 15-minutes of the intervention during which they completed a worksheet with feedback on the results from their screener, a weighing of the advantages and disadvantages of drinking, goal setting, and a list of coping strategies when presented with binge drinking situations. In the short intervention group, participants completed a baseline questionnaire and were provided with 5 minutes of a simple, structured intervention during which they completed a shortened version of the worksheet with feedback on their screener results and goal setting. In the control group, participants completed the baseline questionnaire and were simply given their scores from the screener and an information leaflet.
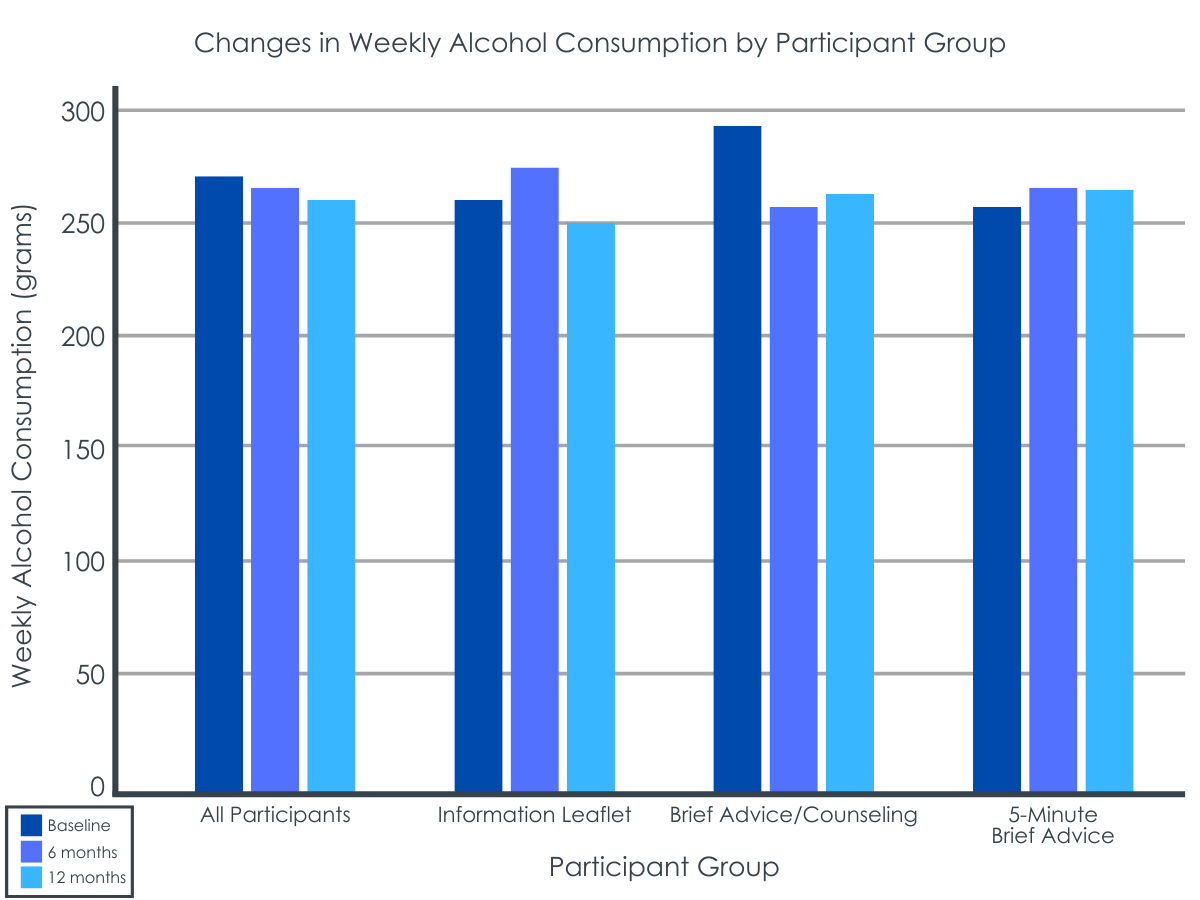
The researchers measured drinking in grams of pure alcohol per week, following the intervention. They assessed the frequency of alcohol use, binge drinking in the past 30 days (defined as 60 or more grams of pure alcohol per occasion), and amount of alcohol consumed at baseline, 6 months after the intervention, and 12 months after the intervention. Weekly alcohol use was calculated by using information about the frequency, type, and amount of alcohol consumed on a daily and monthly basis
They compared the 15-minute intervention, 5-minute intervention, and comparison group on changes in drinking from baseline to 6-month follow-up and baseline to 12-month follow-up on each of weekly drinking, frequency of drinking 5+ days in a week, binge drinking in the past 30 days, as well as on the screener (which was repeated at follow-ups).
In total, 2,276 employees completed the screener, which identified 505 employees as drinking in harmful ways (i.e., they screened “positive”). Of these, 380 employees were eligible for the study and were randomized, but 351 ultimately consented to the study. Follow up rates at 6 and 12 months did not differ between the 3 groups. Among the 351 participants who consented and whose data was analyzed, 98.3% were men, with a median age of 49 years old. The median score on the screener was 11 points and the median amount of alcohol consumed weekly was 238 grams per week (the equivalent of 17 standard drinks per week in the US). The percentage of participants who drank more than 3 days per week was 84.9%, while the percentage of those who binge drank was 73.5% and who smoked was 39.3%. There were no baseline differences between the groups in any of the variables of interest.
WHAT DID THIS STUDY FIND?
Participants in the 15-minute intervention group reduced their drinking more than those in the control group.
At 6 months following the intervention, those who received the standard 15-minute intervention of brief advice and counseling drank 38.1 grams less per week than they did at baseline (the equivalent of 2.72 fewer standard US drinks). This was a greater reduction than was observed in the control group who only received an information leaflet. No decreases in weekly alcohol use were observed in the short 5-minute intervention group at the 6-month follow-up.
While weekly alcohol use also decreased at the 12-month follow-up in the standard intervention group, the change was not different than what was observed in the control group.
Improvement in other drinking outcomes were observed in all 3 groups over time.
For frequency of drinking more than 5 days per week, there was not a decrease at 6-months for any of the groups, but at 12 months, a decrease was observed in all 3 groups, with no differences between them.
For binge drinking in the past 30 days, 16.8% fewer participants in the standard intervention group reported doing so at the 6-month follow-up. At 12 months, all 3 groups reported a decrease from baseline, with no differences between them.
For the screener score, scores for those in the standard intervention group decreased at the 6-month follow-up from baseline. At 12 months, all 3 groups reported a decrease from baseline, with no differences between them.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study evaluated the effectiveness of a standard intervention for reducing alcohol use compared to a shorter intervention and no intervention (i.e., control group) in a workplace setting in Japan. Results showed that the standard intervention was effective in reducing alcohol use at 6 months after the intervention, and it was a greater reduction than what was observed in the control group. As is often the case for brief interventions, effects were small, however, with an average reduction of almost 3 standard US drinks per week.
Improvements in other drinking outcomes, such as the frequency of drinking more than 5 days per week, binge drinking, and scores from the screener, were observed in all 3 groups. This suggests that, while the standard intervention is likely to be effective in the short-term, bringing attention to harmful drinking patterns may also be effective longer-term, given that all 3 groups received their scores from the screener and saw improvements at the 12-month follow-up. It may be that bringing people’s awareness to their drinking is sufficient to reduce alcohol use among people who drink in risky ways but do not have an alcohol use disorder. Another possible explanation for these findings, however, is that data for the 12-month follow-up was collected during the COVID-19 pandemic (June – December 2020), when people were prevented from socializing. Accordingly, people may have reduced their alcohol use as a result of less socializing, a finding that has been shown in other countries where alcohol may be a large part of social activities, such as the Netherlands.
In sum, the study’s findings suggest that screening and the standard 15-minute brief intervention can be effective in slightly reducing weekly alcohol use among people who may drink in potentially harmful ways 6 months following the intervention. Improvements were also seen in other alcohol outcomes among the shorter intervention group and no intervention group, suggesting a possible effect of either bringing awareness to one’s alcohol use or an effect of the COVID-19 pandemic. While the effect sizes were small, this intervention provides another avenue for screening for and addressing hazardous drinking that can be scaled up to achieve important public health benefits.
The study took place in a workplace setting, which may have affected the accuracy of the results. Specifically, while employers were not aware of who was participating or their results, employees still may have under-reported their alcohol use because of fear of their employer finding out.
Participants were mostly men. The study results may therefore not apply to women.
The screener used (i.e., the AUDIT) was developed using participants who were not from Japan. Specifically, it was developed using participants from Australia, Bulgaria, Kenya, Mexico, Norway, and the USA. While its use has since been tested with Japanese participants, and has shown to be reliable and valid with this population, these studies were conducted with fewer participants than the original development. Accordingly, the screener may have falsely captured participants who do not have alcohol problems, or conversely, may have missed some that do, due to cultural variations.
BOTTOM LINE
The study’s findings suggest that screening and the standard 15-minute brief intervention delivered by nurses within a workplace setting can be helpful in slightly reducing weekly alcohol use among people who may drink in potentially harmful ways 6 months following the intervention. While the impact was small, the study adds to other research demonstrating screening and brief intervention can be a helpful approach for reducing alcohol use that could be scaled upacross workplace settingsinternationally to achieve a broader public health benefit.
For individuals and families seeking recovery: The study findings show that individuals who received 15 minutes of an intervention delivered by nurses within a workplace settingreduced their weekly alcohol use more than a shorter version of the same intervention and to a greater extent than providing assessment scores and some alcohol information alone. These findings are similar to those found in primary care settings. Accordingly, people who drink in potentially harmful ways and want to reduce their use, but do not want to enter treatment long-term, are encouraged to speak with their primary care physician about options similar to the one tested in this study.
For treatment professionals and treatment systems: Given that the study findings showed that individuals who received 15 minutes of an intervention reduced their weekly alcohol use, health care professionals who implement brief interventions are likely to be helpful in reducing clients’ alcohol use who drink in potentially harmful ways. Also, since the study demonstrated the feasibility of implementing the intervention in a workplace, treatment professionals embedded within workplaces or who consider traveling to workplaces may reach individuals who they may not have otherwise been helped. However, treatment professionals are cautioned that brief intervention is not likely to be helpful for those with alcohol use disorder, who may require more intensive treatment.
For scientists: Given the small and short-lived effects, more work on the screening and brief intervention approach in workplace settings in Japan would shed light on the best strategies for scaling it up and sustaining and enlarging the effects over time. Additionally, research that uses a screener developed specifically for Japanese populations may be more culturally sensitive, thereby helping to eliminate the risk of false positives and negatives. Finally, examining the effectiveness of the approach with Japanese women would demonstrate the extent to which the current findings generalize to them as well or perhaps benefit women more.
For policy makers: Given the potential benefits of implementing a low intensity screening and brief intervention for reducing alcohol use, supporting funding for additional research on its effectiveness and feasibility of implementing it in a workplace would help shed light on the extent to which it can be beneficial in this setting. Importantly, implementing the approach in workplace settings may result in reaching individuals who drink in harmful ways, but would have not been reached and helped otherwise.
Screening and brief intervention is one such strategy that involves asking individuals a set of questions about their current drinking habits. If they report drinking more than the recommended amounts, a staff person engages them in a short, but systematic discussion about ways to reduce their drinking. This low-intensity intervention produces small, but reliable drinking reductions in primary care and workplace settings across the world.
However, important aspects of implementing the intervention optimally are unclear. For example, there do not appear to be any additional benefits of a longer intervention or repeating the intervention above and beyond a shorter intervention that lasts approximately 20 minutes. It may therefore be that even shorter interventions (e.g., 5 minutes) have beneficial effects and would be more feasible to implement under time constraints. It is also unclear whether the intervention can be effective in workplace settings in Japan specifically. Given the “overwork” culture in Japan, it may be that people are attempting to relax with alcohol. However, this also means the workplace may be an ideal setting to reduce alcohol consumption because of the amount of time spent working. Finally, having nurses deliver the intervention can result in broader implementation than doctors because more nurses are employed in occupational healthcare settings than doctors. This study evaluated the effectiveness of two types of the intervention delivered by nurses in a workplace setting. Studies like these can shed light on the conditions and settings in which screening and brief intervention is likely to be effective and feasible.
HOW WAS THIS STUDY CONDUCTED?
The research team evaluated the effectiveness of two intensities of the same type of brief intervention delivered by nurses in 5 companies from 2 western Japanese regions. Nurses were trained to screen participants using the Alcohol Use Disorder Identification Test (hereafter referred to as “screener”) and provide the types of intervention. This consisted of e-learning and role-playing and included information about the stages of change model and motivational interviewing techniques. The stages of change model helps to identify participants’ readiness and motivation to change their drinking behavior, while motivational interviewing helps them to resolve any ambivalence they may have about change.
Participants were eligible for the study if they were 20 years old or older (i.e., of legal drinking age in Japan) and had a high score on the screener (i.e., greater than 8 points, which reflects hazardous alcohol use). Participants were not eligible if they were 75 years old or older; received treatment for their alcohol use in the past year; had symptoms of alcohol withdrawal in the past year; were advised by a doctor to change their drinking habits in the past 3 months; were pregnant; or reported suicidal thoughts or behaviors.
If eligible, participants were randomized into 1 of 3 groups: (1) the standard intervention, which consisted of a 15-minute advice and counseling session; (2) a shorter intervention, which consisted of a 5-minute brief advice session; or (3) a control group. In the standard intervention group, participants completed a baseline questionnaire and were provided with 15-minutes of the intervention during which they completed a worksheet with feedback on the results from their screener, a weighing of the advantages and disadvantages of drinking, goal setting, and a list of coping strategies when presented with binge drinking situations. In the short intervention group, participants completed a baseline questionnaire and were provided with 5 minutes of a simple, structured intervention during which they completed a shortened version of the worksheet with feedback on their screener results and goal setting. In the control group, participants completed the baseline questionnaire and were simply given their scores from the screener and an information leaflet.
The researchers measured drinking in grams of pure alcohol per week, following the intervention. They assessed the frequency of alcohol use, binge drinking in the past 30 days (defined as 60 or more grams of pure alcohol per occasion), and amount of alcohol consumed at baseline, 6 months after the intervention, and 12 months after the intervention. Weekly alcohol use was calculated by using information about the frequency, type, and amount of alcohol consumed on a daily and monthly basis
They compared the 15-minute intervention, 5-minute intervention, and comparison group on changes in drinking from baseline to 6-month follow-up and baseline to 12-month follow-up on each of weekly drinking, frequency of drinking 5+ days in a week, binge drinking in the past 30 days, as well as on the screener (which was repeated at follow-ups).
In total, 2,276 employees completed the screener, which identified 505 employees as drinking in harmful ways (i.e., they screened “positive”). Of these, 380 employees were eligible for the study and were randomized, but 351 ultimately consented to the study. Follow up rates at 6 and 12 months did not differ between the 3 groups. Among the 351 participants who consented and whose data was analyzed, 98.3% were men, with a median age of 49 years old. The median score on the screener was 11 points and the median amount of alcohol consumed weekly was 238 grams per week (the equivalent of 17 standard drinks per week in the US). The percentage of participants who drank more than 3 days per week was 84.9%, while the percentage of those who binge drank was 73.5% and who smoked was 39.3%. There were no baseline differences between the groups in any of the variables of interest.
WHAT DID THIS STUDY FIND?
Participants in the 15-minute intervention group reduced their drinking more than those in the control group.
At 6 months following the intervention, those who received the standard 15-minute intervention of brief advice and counseling drank 38.1 grams less per week than they did at baseline (the equivalent of 2.72 fewer standard US drinks). This was a greater reduction than was observed in the control group who only received an information leaflet. No decreases in weekly alcohol use were observed in the short 5-minute intervention group at the 6-month follow-up.
While weekly alcohol use also decreased at the 12-month follow-up in the standard intervention group, the change was not different than what was observed in the control group.
Improvement in other drinking outcomes were observed in all 3 groups over time.
For frequency of drinking more than 5 days per week, there was not a decrease at 6-months for any of the groups, but at 12 months, a decrease was observed in all 3 groups, with no differences between them.
For binge drinking in the past 30 days, 16.8% fewer participants in the standard intervention group reported doing so at the 6-month follow-up. At 12 months, all 3 groups reported a decrease from baseline, with no differences between them.
For the screener score, scores for those in the standard intervention group decreased at the 6-month follow-up from baseline. At 12 months, all 3 groups reported a decrease from baseline, with no differences between them.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study evaluated the effectiveness of a standard intervention for reducing alcohol use compared to a shorter intervention and no intervention (i.e., control group) in a workplace setting in Japan. Results showed that the standard intervention was effective in reducing alcohol use at 6 months after the intervention, and it was a greater reduction than what was observed in the control group. As is often the case for brief interventions, effects were small, however, with an average reduction of almost 3 standard US drinks per week.
Improvements in other drinking outcomes, such as the frequency of drinking more than 5 days per week, binge drinking, and scores from the screener, were observed in all 3 groups. This suggests that, while the standard intervention is likely to be effective in the short-term, bringing attention to harmful drinking patterns may also be effective longer-term, given that all 3 groups received their scores from the screener and saw improvements at the 12-month follow-up. It may be that bringing people’s awareness to their drinking is sufficient to reduce alcohol use among people who drink in risky ways but do not have an alcohol use disorder. Another possible explanation for these findings, however, is that data for the 12-month follow-up was collected during the COVID-19 pandemic (June – December 2020), when people were prevented from socializing. Accordingly, people may have reduced their alcohol use as a result of less socializing, a finding that has been shown in other countries where alcohol may be a large part of social activities, such as the Netherlands.
In sum, the study’s findings suggest that screening and the standard 15-minute brief intervention can be effective in slightly reducing weekly alcohol use among people who may drink in potentially harmful ways 6 months following the intervention. Improvements were also seen in other alcohol outcomes among the shorter intervention group and no intervention group, suggesting a possible effect of either bringing awareness to one’s alcohol use or an effect of the COVID-19 pandemic. While the effect sizes were small, this intervention provides another avenue for screening for and addressing hazardous drinking that can be scaled up to achieve important public health benefits.
The study took place in a workplace setting, which may have affected the accuracy of the results. Specifically, while employers were not aware of who was participating or their results, employees still may have under-reported their alcohol use because of fear of their employer finding out.
Participants were mostly men. The study results may therefore not apply to women.
The screener used (i.e., the AUDIT) was developed using participants who were not from Japan. Specifically, it was developed using participants from Australia, Bulgaria, Kenya, Mexico, Norway, and the USA. While its use has since been tested with Japanese participants, and has shown to be reliable and valid with this population, these studies were conducted with fewer participants than the original development. Accordingly, the screener may have falsely captured participants who do not have alcohol problems, or conversely, may have missed some that do, due to cultural variations.
BOTTOM LINE
The study’s findings suggest that screening and the standard 15-minute brief intervention delivered by nurses within a workplace setting can be helpful in slightly reducing weekly alcohol use among people who may drink in potentially harmful ways 6 months following the intervention. While the impact was small, the study adds to other research demonstrating screening and brief intervention can be a helpful approach for reducing alcohol use that could be scaled upacross workplace settingsinternationally to achieve a broader public health benefit.
For individuals and families seeking recovery: The study findings show that individuals who received 15 minutes of an intervention delivered by nurses within a workplace settingreduced their weekly alcohol use more than a shorter version of the same intervention and to a greater extent than providing assessment scores and some alcohol information alone. These findings are similar to those found in primary care settings. Accordingly, people who drink in potentially harmful ways and want to reduce their use, but do not want to enter treatment long-term, are encouraged to speak with their primary care physician about options similar to the one tested in this study.
For treatment professionals and treatment systems: Given that the study findings showed that individuals who received 15 minutes of an intervention reduced their weekly alcohol use, health care professionals who implement brief interventions are likely to be helpful in reducing clients’ alcohol use who drink in potentially harmful ways. Also, since the study demonstrated the feasibility of implementing the intervention in a workplace, treatment professionals embedded within workplaces or who consider traveling to workplaces may reach individuals who they may not have otherwise been helped. However, treatment professionals are cautioned that brief intervention is not likely to be helpful for those with alcohol use disorder, who may require more intensive treatment.
For scientists: Given the small and short-lived effects, more work on the screening and brief intervention approach in workplace settings in Japan would shed light on the best strategies for scaling it up and sustaining and enlarging the effects over time. Additionally, research that uses a screener developed specifically for Japanese populations may be more culturally sensitive, thereby helping to eliminate the risk of false positives and negatives. Finally, examining the effectiveness of the approach with Japanese women would demonstrate the extent to which the current findings generalize to them as well or perhaps benefit women more.
For policy makers: Given the potential benefits of implementing a low intensity screening and brief intervention for reducing alcohol use, supporting funding for additional research on its effectiveness and feasibility of implementing it in a workplace would help shed light on the extent to which it can be beneficial in this setting. Importantly, implementing the approach in workplace settings may result in reaching individuals who drink in harmful ways, but would have not been reached and helped otherwise.
Screening and brief intervention is one such strategy that involves asking individuals a set of questions about their current drinking habits. If they report drinking more than the recommended amounts, a staff person engages them in a short, but systematic discussion about ways to reduce their drinking. This low-intensity intervention produces small, but reliable drinking reductions in primary care and workplace settings across the world.
However, important aspects of implementing the intervention optimally are unclear. For example, there do not appear to be any additional benefits of a longer intervention or repeating the intervention above and beyond a shorter intervention that lasts approximately 20 minutes. It may therefore be that even shorter interventions (e.g., 5 minutes) have beneficial effects and would be more feasible to implement under time constraints. It is also unclear whether the intervention can be effective in workplace settings in Japan specifically. Given the “overwork” culture in Japan, it may be that people are attempting to relax with alcohol. However, this also means the workplace may be an ideal setting to reduce alcohol consumption because of the amount of time spent working. Finally, having nurses deliver the intervention can result in broader implementation than doctors because more nurses are employed in occupational healthcare settings than doctors. This study evaluated the effectiveness of two types of the intervention delivered by nurses in a workplace setting. Studies like these can shed light on the conditions and settings in which screening and brief intervention is likely to be effective and feasible.
HOW WAS THIS STUDY CONDUCTED?
The research team evaluated the effectiveness of two intensities of the same type of brief intervention delivered by nurses in 5 companies from 2 western Japanese regions. Nurses were trained to screen participants using the Alcohol Use Disorder Identification Test (hereafter referred to as “screener”) and provide the types of intervention. This consisted of e-learning and role-playing and included information about the stages of change model and motivational interviewing techniques. The stages of change model helps to identify participants’ readiness and motivation to change their drinking behavior, while motivational interviewing helps them to resolve any ambivalence they may have about change.
Participants were eligible for the study if they were 20 years old or older (i.e., of legal drinking age in Japan) and had a high score on the screener (i.e., greater than 8 points, which reflects hazardous alcohol use). Participants were not eligible if they were 75 years old or older; received treatment for their alcohol use in the past year; had symptoms of alcohol withdrawal in the past year; were advised by a doctor to change their drinking habits in the past 3 months; were pregnant; or reported suicidal thoughts or behaviors.
If eligible, participants were randomized into 1 of 3 groups: (1) the standard intervention, which consisted of a 15-minute advice and counseling session; (2) a shorter intervention, which consisted of a 5-minute brief advice session; or (3) a control group. In the standard intervention group, participants completed a baseline questionnaire and were provided with 15-minutes of the intervention during which they completed a worksheet with feedback on the results from their screener, a weighing of the advantages and disadvantages of drinking, goal setting, and a list of coping strategies when presented with binge drinking situations. In the short intervention group, participants completed a baseline questionnaire and were provided with 5 minutes of a simple, structured intervention during which they completed a shortened version of the worksheet with feedback on their screener results and goal setting. In the control group, participants completed the baseline questionnaire and were simply given their scores from the screener and an information leaflet.
The researchers measured drinking in grams of pure alcohol per week, following the intervention. They assessed the frequency of alcohol use, binge drinking in the past 30 days (defined as 60 or more grams of pure alcohol per occasion), and amount of alcohol consumed at baseline, 6 months after the intervention, and 12 months after the intervention. Weekly alcohol use was calculated by using information about the frequency, type, and amount of alcohol consumed on a daily and monthly basis
They compared the 15-minute intervention, 5-minute intervention, and comparison group on changes in drinking from baseline to 6-month follow-up and baseline to 12-month follow-up on each of weekly drinking, frequency of drinking 5+ days in a week, binge drinking in the past 30 days, as well as on the screener (which was repeated at follow-ups).
In total, 2,276 employees completed the screener, which identified 505 employees as drinking in harmful ways (i.e., they screened “positive”). Of these, 380 employees were eligible for the study and were randomized, but 351 ultimately consented to the study. Follow up rates at 6 and 12 months did not differ between the 3 groups. Among the 351 participants who consented and whose data was analyzed, 98.3% were men, with a median age of 49 years old. The median score on the screener was 11 points and the median amount of alcohol consumed weekly was 238 grams per week (the equivalent of 17 standard drinks per week in the US). The percentage of participants who drank more than 3 days per week was 84.9%, while the percentage of those who binge drank was 73.5% and who smoked was 39.3%. There were no baseline differences between the groups in any of the variables of interest.
WHAT DID THIS STUDY FIND?
Participants in the 15-minute intervention group reduced their drinking more than those in the control group.
At 6 months following the intervention, those who received the standard 15-minute intervention of brief advice and counseling drank 38.1 grams less per week than they did at baseline (the equivalent of 2.72 fewer standard US drinks). This was a greater reduction than was observed in the control group who only received an information leaflet. No decreases in weekly alcohol use were observed in the short 5-minute intervention group at the 6-month follow-up.
While weekly alcohol use also decreased at the 12-month follow-up in the standard intervention group, the change was not different than what was observed in the control group.
Improvement in other drinking outcomes were observed in all 3 groups over time.
For frequency of drinking more than 5 days per week, there was not a decrease at 6-months for any of the groups, but at 12 months, a decrease was observed in all 3 groups, with no differences between them.
For binge drinking in the past 30 days, 16.8% fewer participants in the standard intervention group reported doing so at the 6-month follow-up. At 12 months, all 3 groups reported a decrease from baseline, with no differences between them.
For the screener score, scores for those in the standard intervention group decreased at the 6-month follow-up from baseline. At 12 months, all 3 groups reported a decrease from baseline, with no differences between them.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study evaluated the effectiveness of a standard intervention for reducing alcohol use compared to a shorter intervention and no intervention (i.e., control group) in a workplace setting in Japan. Results showed that the standard intervention was effective in reducing alcohol use at 6 months after the intervention, and it was a greater reduction than what was observed in the control group. As is often the case for brief interventions, effects were small, however, with an average reduction of almost 3 standard US drinks per week.
Improvements in other drinking outcomes, such as the frequency of drinking more than 5 days per week, binge drinking, and scores from the screener, were observed in all 3 groups. This suggests that, while the standard intervention is likely to be effective in the short-term, bringing attention to harmful drinking patterns may also be effective longer-term, given that all 3 groups received their scores from the screener and saw improvements at the 12-month follow-up. It may be that bringing people’s awareness to their drinking is sufficient to reduce alcohol use among people who drink in risky ways but do not have an alcohol use disorder. Another possible explanation for these findings, however, is that data for the 12-month follow-up was collected during the COVID-19 pandemic (June – December 2020), when people were prevented from socializing. Accordingly, people may have reduced their alcohol use as a result of less socializing, a finding that has been shown in other countries where alcohol may be a large part of social activities, such as the Netherlands.
In sum, the study’s findings suggest that screening and the standard 15-minute brief intervention can be effective in slightly reducing weekly alcohol use among people who may drink in potentially harmful ways 6 months following the intervention. Improvements were also seen in other alcohol outcomes among the shorter intervention group and no intervention group, suggesting a possible effect of either bringing awareness to one’s alcohol use or an effect of the COVID-19 pandemic. While the effect sizes were small, this intervention provides another avenue for screening for and addressing hazardous drinking that can be scaled up to achieve important public health benefits.
The study took place in a workplace setting, which may have affected the accuracy of the results. Specifically, while employers were not aware of who was participating or their results, employees still may have under-reported their alcohol use because of fear of their employer finding out.
Participants were mostly men. The study results may therefore not apply to women.
The screener used (i.e., the AUDIT) was developed using participants who were not from Japan. Specifically, it was developed using participants from Australia, Bulgaria, Kenya, Mexico, Norway, and the USA. While its use has since been tested with Japanese participants, and has shown to be reliable and valid with this population, these studies were conducted with fewer participants than the original development. Accordingly, the screener may have falsely captured participants who do not have alcohol problems, or conversely, may have missed some that do, due to cultural variations.
BOTTOM LINE
The study’s findings suggest that screening and the standard 15-minute brief intervention delivered by nurses within a workplace setting can be helpful in slightly reducing weekly alcohol use among people who may drink in potentially harmful ways 6 months following the intervention. While the impact was small, the study adds to other research demonstrating screening and brief intervention can be a helpful approach for reducing alcohol use that could be scaled upacross workplace settingsinternationally to achieve a broader public health benefit.
For individuals and families seeking recovery: The study findings show that individuals who received 15 minutes of an intervention delivered by nurses within a workplace settingreduced their weekly alcohol use more than a shorter version of the same intervention and to a greater extent than providing assessment scores and some alcohol information alone. These findings are similar to those found in primary care settings. Accordingly, people who drink in potentially harmful ways and want to reduce their use, but do not want to enter treatment long-term, are encouraged to speak with their primary care physician about options similar to the one tested in this study.
For treatment professionals and treatment systems: Given that the study findings showed that individuals who received 15 minutes of an intervention reduced their weekly alcohol use, health care professionals who implement brief interventions are likely to be helpful in reducing clients’ alcohol use who drink in potentially harmful ways. Also, since the study demonstrated the feasibility of implementing the intervention in a workplace, treatment professionals embedded within workplaces or who consider traveling to workplaces may reach individuals who they may not have otherwise been helped. However, treatment professionals are cautioned that brief intervention is not likely to be helpful for those with alcohol use disorder, who may require more intensive treatment.
For scientists: Given the small and short-lived effects, more work on the screening and brief intervention approach in workplace settings in Japan would shed light on the best strategies for scaling it up and sustaining and enlarging the effects over time. Additionally, research that uses a screener developed specifically for Japanese populations may be more culturally sensitive, thereby helping to eliminate the risk of false positives and negatives. Finally, examining the effectiveness of the approach with Japanese women would demonstrate the extent to which the current findings generalize to them as well or perhaps benefit women more.
For policy makers: Given the potential benefits of implementing a low intensity screening and brief intervention for reducing alcohol use, supporting funding for additional research on its effectiveness and feasibility of implementing it in a workplace would help shed light on the extent to which it can be beneficial in this setting. Importantly, implementing the approach in workplace settings may result in reaching individuals who drink in harmful ways, but would have not been reached and helped otherwise.